beyond health disparities: healthy … of first episode psychosis care 9. ... 6. promote personal...
TRANSCRIPT

BEYOND HEALTH
DISPARITIES: HEALTHY
OUTCOMES FOR ALLDefining a Culture of Health in Nebraska
Nebraska Action Coalition (NAC)-Future of Nursing,
Nebraska Nurse Association (NNA),
Nebraska Organization of Nurse Leaders (NONL), and
Nebraska Assembly of Nursing Deans and Directors (NANDD).
October 15, 2015
Sen. Sue Crawford (NE, LD45)

From Vision to Action: A Nebraska
Discussion• From Vision to Action Framework
• Measures of Nebraska Health
• Examples of Nebraska Action
• Special Attention to:
• Health Disparities (rural/urban)
• Mental Health
• Health Determinants
• Health Policy
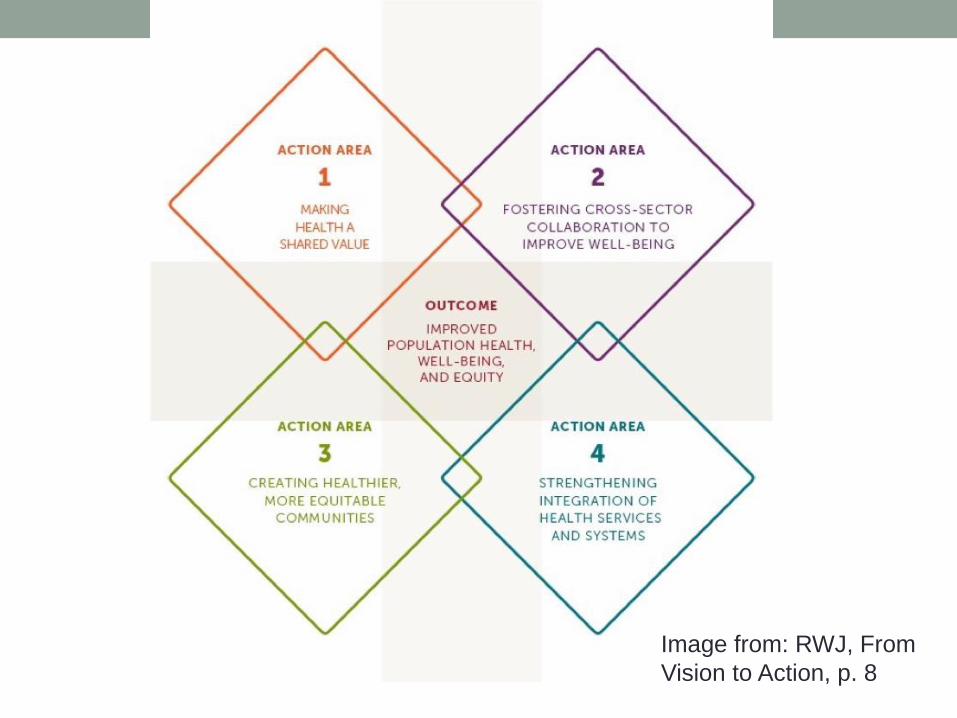
Image from: RWJ, From
Vision to Action, p. 8

Image from: https://icsihealthcareblog.wordpress.com/2014/03/28/social-determinants-helped-determine-my-
health-in-2013/ (Accessed September 22, 2015)
Public Policy and Health Outcomes
Health PolicyHealth
DeterminantsHealth
Outcomes



Making Health A Shared Value
Mindset and expectations
• Understand health interdependence
• Value well-being
• Discuss health promotion
Sense of Community
• Emotional connection
• Sense of belonging
• Social support
•
Civic Engagement
• Voter turnout
• Volunteer engagement




Nebraska Examples
• Service Learning
• Livewell Nebraska
• On-line voter registration

Fostering Cross-Sector Collaboration to
Improve Well-BeingQuality partnerships
• Local health department collaboration
• Opportunities to improve health for youth at schools
• Business support for workplace health promotion and Culture of Health
Investment in cross-sector collaboration
• U.S. corporate giving
• Federal allocations for health investments related to nutrition and indoor and outdoor physical activity
Policies that support collaboration
• Community relations and policing
• Youth exposure to advertising for healthy and unhealthy food and beverage products
• Climate resilience
• Health in all policies
Nebraska Examples
• VetSet
• School Based Health Clinics and Dental Partnerships
• Buffalo County Health Partners
• Whole Child Project (State-wide – Nebraska School
Board Association)
• Interim Discussion of State Paid Family Leave

Creating Healthier, More Equitable
CommunitiesBuilt/Physical Environment
• Housing affordability
• Access to healthy foods
• Youth safety
Social and Economic Environment• Residential segregation
• Early childhood education
• Public libraries
Policy and Governance• Complete Streets policies
• Air quality

Dr. Ali S. Khan, M.D. – Public Health
Measures in Nebraska• Nebraska Successes:
• Nebraska 10th in health
• Increases in high school graduation rates and child immunizations,
• Decreases in child poverty
• Nebraska Challenges:
• 20% consumed four or more (women) or five or more (men) alcoholic beverages on at least one occasion in the past month (44th)
• High incidence of infectious disease, including whooping cough and certain types of food poisoning and sexually transmitted infections.
• Obesity rates, with 29.6 percent of the adult population having a body mass index of 30.0 or higher (normal is 18.5 to 22).
• The most disturbing of these measures is that Nebraska is ranked 46th in health equity — only four states have more disparities in health among their populations.
Dr. Khan – Public Health Prescription for
Nebraska• Reduce Nebraska’s cancer deaths (and heart disease) by
increasing the cigarette tax by at least $1. Our current
excise tax on cigarettes of 64 cents per pack is lower than
74 percent of other states.
• Increase health care coverage in Nebraska so nobody
falls through the gap of our Medicaid programs and
federal health exchanges (Medicaid Expansion)
• Embrace more innovative public health strategies and
invest in public health research and prevention (Health
Enterprise Zones; Social Impact Bonds; Prevention
Funds)

Rural Social Determinants of Disparities
• Income, employment, and poverty
• Educational attainment and literacy
• Race/ethnicity
• Health literacy
• Adequate community infrastructure, which can ensure public safety, allow access to media, and promote wellness
• Environmental health, including water quality, air quality, and pollution
• Access to safe and healthy homes, including issues related to energy costs and weatherization needs, lead-based paint, and other safety issues
• Access to affordable transportation, which can impact both job access and healthcare access
• Access to healthy and affordable food
• Access to healthcare services
(Rural Assistance Center, accessed Sept. 5, 2015)

Nebraska Examples
• First Five Nebraska
• Complete Streets
• B-cycles
• Nebraska Futures
• Nebraska Community Foundation
• Farmer’s Markets
• Urban Farming (USDA)

STRENGTHENING INTEGRATION OF
HEALTH SERVICES AND SYSTEMS
Access• Access to public health
• Access to stable health insurance
• Access to mental health services
• Dental visit in past year
Consumer experience and quality• Consumer experience
• Population covered by an Accountable Care Organization
Balance and Integration• Electronic medical record linkages
• Hospital partnerships
• Practice laws for nurse practitioners
• Social spending relative to health expenditure

Nebraska Access & Poverty
• Percent of FPL
14% of Nebraskans live at < 100% of FPL for income
32% of Nebraskans live at < 200% of FPL for income
Uninsured
9% children uninsured (all state median 8.6%)
Best state = 3%
Out-of-pocket medical spending
• Nebraskans living at 200% of FPL or less spend 37% of their income
on medical spending
• As opposed to only 2% of their income spent on medical care for
those at or above 400% of the FPL
(LR 422 report, 2014; Dr. Zetterman)



Rural Health Systems and Professional
Incentive ActResults:
• 107 rural incentive recipients practicing under obligation in Nebraska
• The Nebraska Loan Repayment Program has 92% success rate of recipients completing their obligations
• The Nebraska Rural Health Student Loan Program buyout rate dropped from 50% in 1998 to 17%.
• Impacts care to approximately 800,000 people
Remaining Needs:• Comprehensive plan for recruitment and retention
• Integrated rural health system that includes critical access hospitals, primary care, and behavioral health
• Tele-health and electronic health records that integrate care
• Interdisciplinary training – primary & behavioral health
(Nebraska Rural Health Advisory Commission’s Annual Report, 2014)

Mental Health Gaps
1. Fragmentation and lack of comprehensive system collaboration
2. Insufficient access to care
3. Insufficient availability of integrated care for co-occuringdisorder services and services for people with complex needs
4. Insufficient availability of intensive community-based services
5. Insufficient availability of Supported Employment
6. Lack of comprehensive psychiatric emergency system
7. Insufficient resources and supports for housing
8. Unavailability of First Episode Psychosis Care
9. Workforce shortages
(TriWest Report, 2015)

Coverage Gap
• 50,000 – 70,000 Nebraskans uninsured who could be
covered
• Implications for Mental Health
• Implications for Health Care System
LR 422 Building Blocks
1. Assure healthcare is available for all Nebraskans
2. Support effective models of healthcare delivery, financing,
and payment.
3. Assume public transparency of health care quality and
patient safety for all providers and facilities.
4. Establish a state-wide database for the collection and
analysis of health and healthcare delivery data in Nebraska.
5. Use population health-based interventions.
6. Promote personal responsibility for wellness.
7. Address healthcare workforce shortages.
8. Coordination of state-wide health planning for Nebraska.

Nebraska Policy Examples
• Mental Health Partnership
• Nebraska Rural Health Advisory Commission
• LR 422 Study Group
• Nurse Practitioner Act
• Interim Discussions of Mental Health Workforce
• All-Payer Discussions of Medical Home Model
• Absence of Medicaid Expansion
• State Health Coordination?

Public Policy and Health Outcomes
Health PolicyHealth
DeterminantsHealth
Outcomes

Image from: RWJ, From
Vision to Action, p. 8