bartonella infection in children rabeen lutchman
TRANSCRIPT
Bartonella infection in children
Rabeen Lutchman
Why this talkO Think outside the box
StructureO Quick Revision of an Approach to lymphadenopathy
Bartonella: O Organism and different speciesO Etiology and PathogenesisO EpidemiologyO Clinical Picture of typical Cat Scratch DiseaseO Atypical PresentationO DiagnosisO Treatment
Case Presentation
LymphadenopathyO Infection, Inflammatory and
Malignant processesO Generalized – 2 or more non-
contagious lymph nodes groupsO Regional – 1 lymph node groupO Pathological is more than 10mm
(15mm inguinal)
Generalized Lymphadenopathy
O ViralEBV, CMV, HIV, Hepatitis(B,C), Varicella, Adenovirus, Rubella
O BacterialMycobacterium Tuberculosis, Treponema Pallidum (secondary syphilis), Brucella, Leptospira interrogans
O FungalHistoplasma capsulatum Coccidioides immitis
O ProtozoalToxoplasma gondi
Regional Lympadenopathy
O STDsNeisseria gonorrhoeseTreponema pallidumHerpes simples virusHaemophilus ducreyiChlamydia trochomatis
O Non Venereal OriginBacterialStaphylococcus aureusGroup A and B StreptococciMycobacterium tuberculosis
Bartonella henselaeYersinia pestisSporothrix schenckii
O ViralEBVO ProtozoalToxoplasma gondii
Non infectious lymphadenopathy
O CongenitalO Inflammatory conditions (JIA, SLE,
Kawasaki’s Disease)O Malignancy
(leukemia,lymphoma,neuroblastoma)O Adverse drug reactions (phenytoin,
INH, allopurinol)

Batonella Infection in Children
OrganismO gram-negative, intracellular,
oxidase-negative, fastidious aerobic rods.
O Warthin –Starry silver impregnation stain or Brown –Hopps tissue Gram-stain.
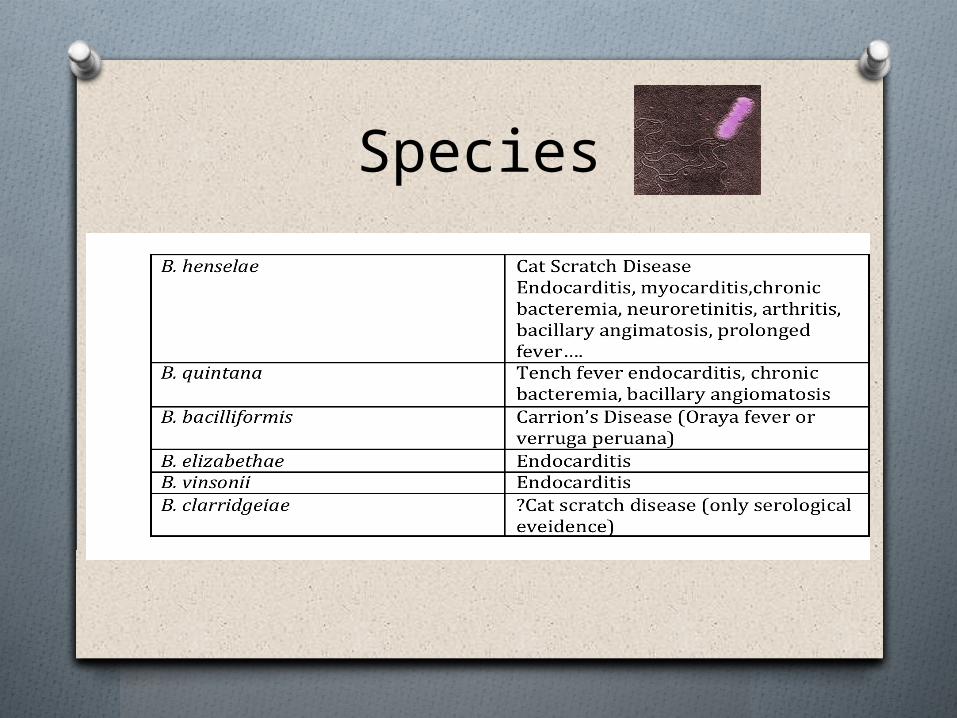
Species
Etiology and Pathogenesis
O Cats O Direct horizontal transmission ✗O Ctenocephalides felisO Evasion of the immune system -
intraerythrocytic parasitesO Humans cat saliva or scratch of a cat.O Invades CD34 hematopoietic progenitor
cells and not the erythrocytes directlyO Presence and Replication of these organisms
inside erythroid differentiated cells
Response Immune Competent Host:O Granulomatous and SuppurativeO Lymphoid hyperplasia and arteriolar
proliferationO Interferon- y- mediated T helper1 cell response
macrophage recruitment O Multinucleated giant cells with central areas of
necrosisO Microabsesses ± suppuration of the lymph nodeO Remains within the lymphatics O Symptomatic response lasting 2-4 months
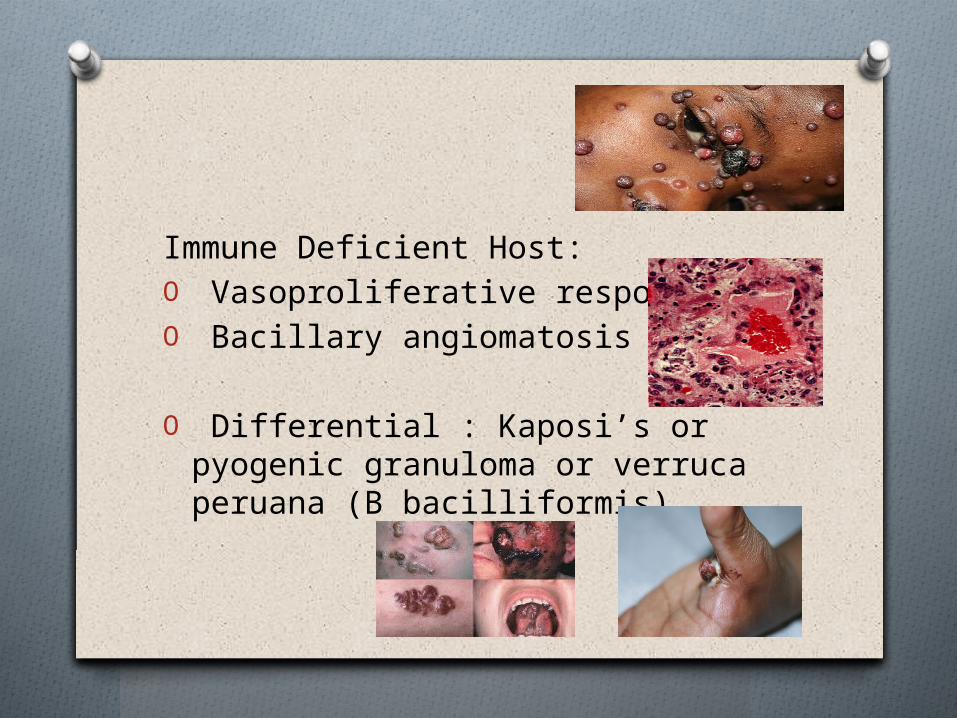
Immune Deficient Host:O Vasoproliferative responseO Bacillary angiomatosis
O Differential : Kaposi’s or pyogenic granuloma or verruca peruana (B bacilliformis)
Epidemiology
O Worldwide distribution (not confined to developing countries)
O Overall seroprevalence in cats in the US 28 -51%
O Disease of children 54- 87% of cases with CSD being under 18
O 0.6 per 100 000 children < 18 yearsO 0.86 per 100 000 children < 5 years
High Rate of Bartonella henselae infection in HIV-positive outpatients in Johannesburg, South Africa - Frean et al., Trans Royal Soc. Trop Med. Hyg., 2002;96:549-550O 188 pts – 19 (10.1%) were PCR positive for B
hensaelaeO 1 patient had suspected bacillary angimatosisO 13 of the 19 were tested serologically and 8/13
(62%) were seropositive (1:64 or higher)
Clinical Manifestations
Typical Cat Scratch:O Isolated lymphadenopathy with fever ( ⅓ may present
without fever and <10% have a fever > 39°C)O Erythematous papule - 3 to 10 days after inoculationO Erythematous, vesicular and papular crusted stagesO Regional lymphadenopathy 1-3 weeks after inoculationO Lymphadenopathy is seen in all with typical CSD and
85% have a single node involved – most commonly axillary and epitrochlear (46%) and the head and neck (26%) and inguinal (17.5%)
O Nodal distribution contact most commonly with the hands
O ± 10% of nodes will suppurate drainage
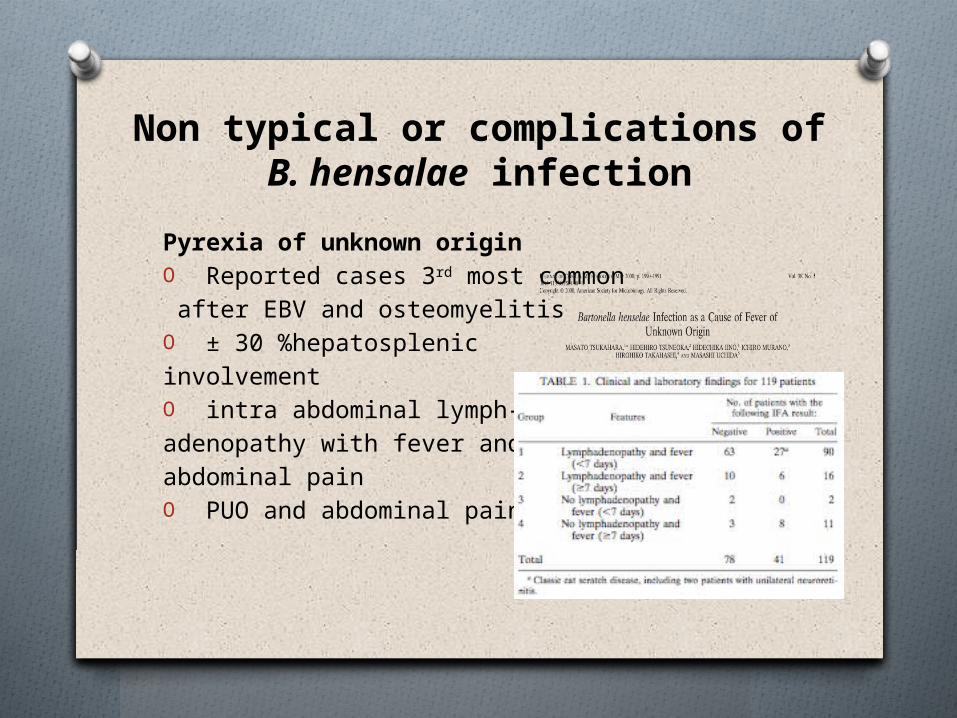
Non typical or complications of B. hensalae infection
Pyrexia of unknown originO Reported cases 3rd most common after EBV and osteomyelitis O ± 30 %hepatosplenic involvementO intra abdominal lymph-adenopathy with fever and abdominal painO PUO and abdominal pain
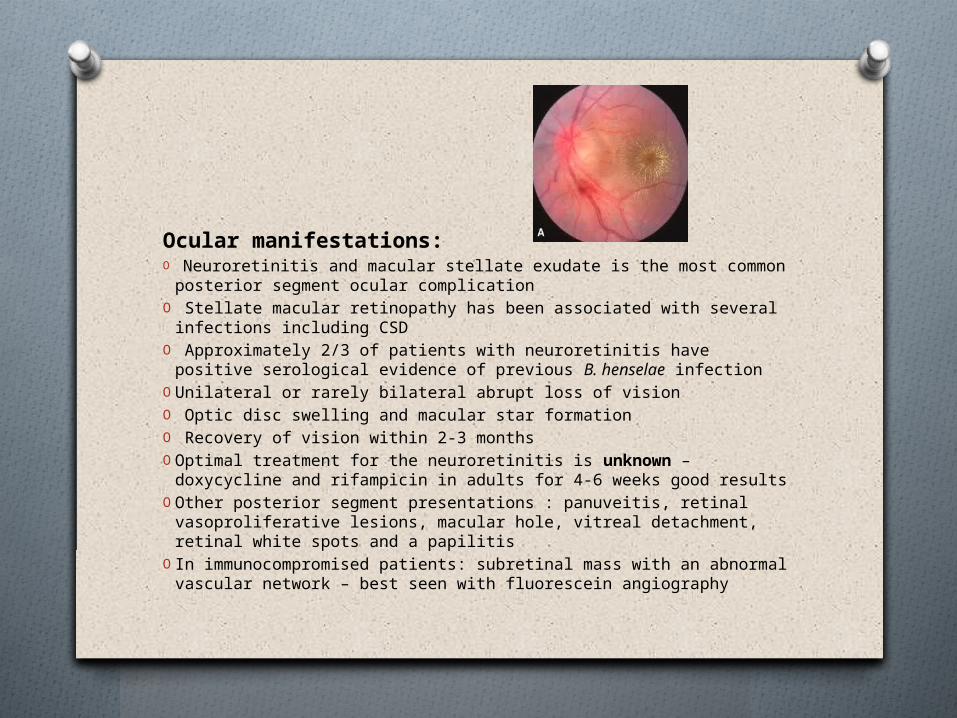
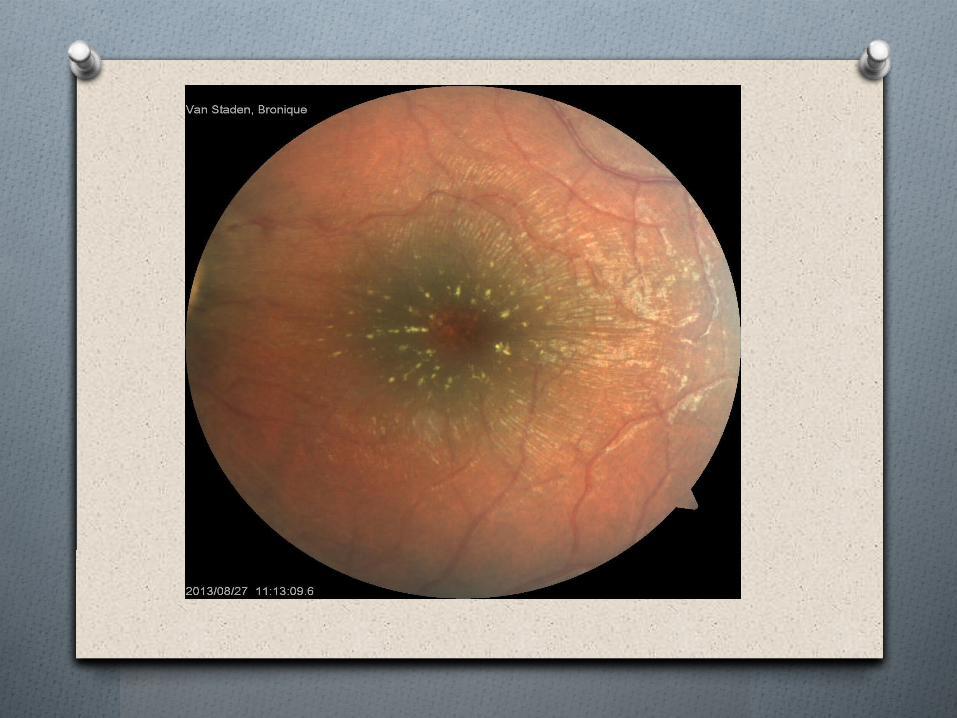
Ocular manifestations:O Neuroretinitis and macular stellate exudate is the most common
posterior segment ocular complicationO Stellate macular retinopathy has been associated with several
infections including CSDO Approximately 2/3 of patients with neuroretinitis have positive
serological evidence of previous B. henselae infectionO Unilateral or rarely bilateral abrupt loss of visionO Optic disc swelling and macular star formationO Recovery of vision within 2-3 monthsO Optimal treatment for the neuroretinitis is unknown – doxycycline
and rifampicin in adults for 4-6 weeks good resultsO Other posterior segment presentations : panuveitis, retinal
vasoproliferative lesions, macular hole, vitreal detachment, retinal white spots and a papilitis
O In immunocompromised patients: subretinal mass with an abnormal vascular network – best seen with fluorescein angiography
Other :O Encephalopathy O HaematologicalO Hepatosplenic – with abdominal lymphadenopathy and
microabscesses in the spleen (Not all TB!!)O Dermatological - Bacillary angiomatosisO Orthopedic – osteomyelitis/osteolytic lesions.O RF negative arthritis/ arthralgia
(female/adults/erythema nodosum) (mainly knees/wrist/ankle and elbow joints)
O Pulmonary – atypical pneumonia/ pleural thickening/ effusion
O Pseudomalignancy
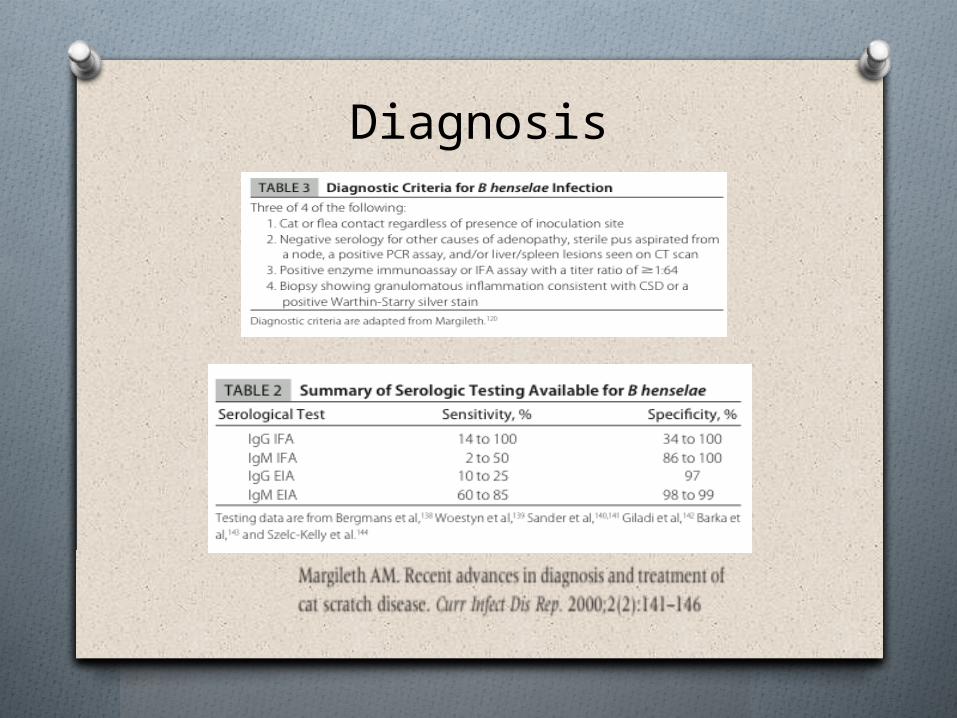
Diagnosis
Treatment
O Varies : clinical manifestation and immune status of the patient
O Paucity of data – most case series rather than RCA’s
O Divide between in vitro efficacy of antibiotics and the ability to successfully treat in clinical practice
O In vitro sensitive to macrolides/aminoglycosides/ trimethroprim-sulphamethoxazole /B lactams and extended spectrum cephalosporins/ rifampicin and ciprofloxacin
Single RCA : Prospective randomized double-blind placebo- controlled evaluation of azithromycin for the treatment of cat-scratch disease. Pediatr infect Dis J. 1998;17(6): 447-452 O 80% decrease in lymph node volume in 50% of
AZA treated patients compared to 7% of the placebo group in the first 30 days
O No difference in clinical outcome and no efficacy demonstrated for disseminated disease
O Aspiration if the suppurate or if chronic large painful lymphadenopathy
O I and D ✗ chronic sinus tract formation
O Complicated management is guided case studies rather than RCA’s
O For neuroretinitis doxycycline is considered a preferred drug because of the intraocular and CNS penetration . Children less than 8 ?
O ? antibiotic is necessary
Case StudyO 3 year old girl referred from the clinic
with non resolving conjunctivitis not responding to chloromycetin eye drops
O Seen in Ggr: 1 week history of red eyes, photophobia and poor vision – walking into objects
O On examination: lymph nodes palpated in the anterior chain of cervical region (small nodes) and (R) red eye
O Referred to opthalmology…
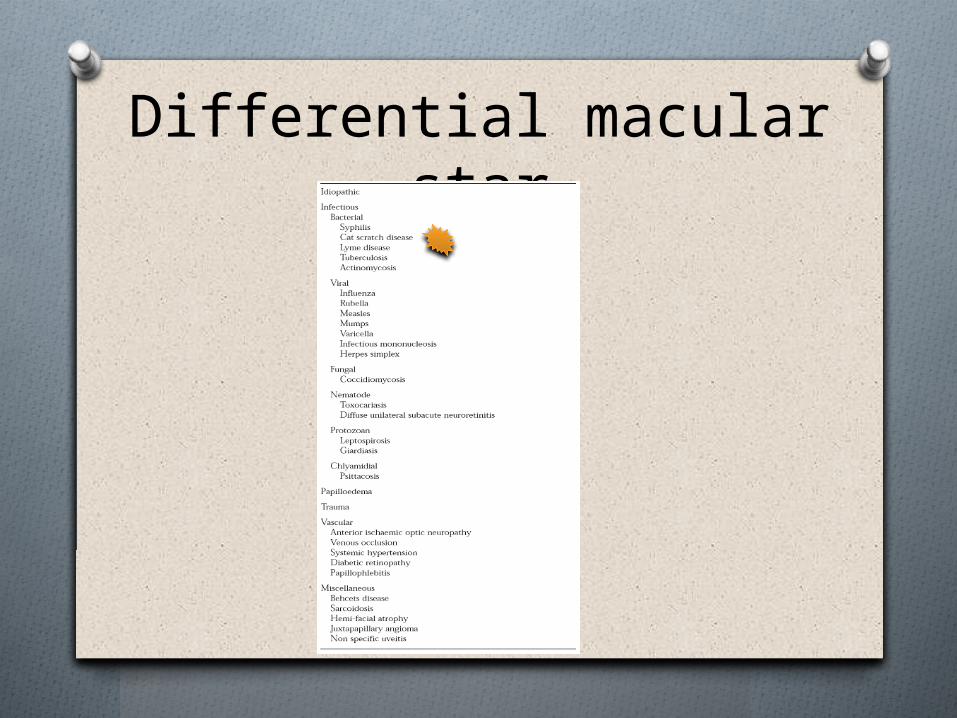
Differential macular star
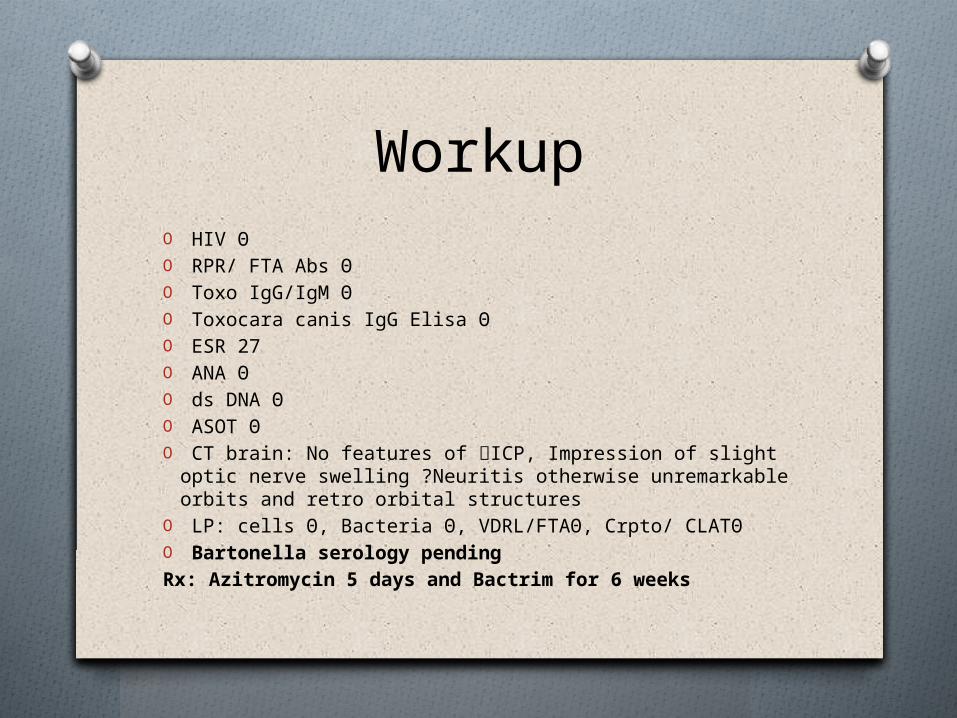
WorkupO HIV ΘO RPR/ FTA Abs ΘO Toxo IgG/IgM ΘO Toxocara canis IgG Elisa ΘO ESR 27O ANA ΘO ds DNA ΘO ASOT ΘO CT brain: No features of ICP, Impression of slight optic
nerve swelling ?Neuritis otherwise unremarkable orbits and retro orbital structures
O LP: cells Θ, Bacteria Θ, VDRL/FTAΘ, Crpto/ CLATΘO Bartonella serology pendingRx: Azitromycin 5 days and Bactrim for 6 weeks
References1. Todd et al. Beyond cat scratch disease: widening spectrum
of Bartonella henselae infection. Pediatrics May 2008; 121(5):e1413-1425
2. Tsukahara et al. Bartonella henselae infection as a cause of fever of unknown origin. Journal of Clinical Microbiology.2000,38(5):1990-1991
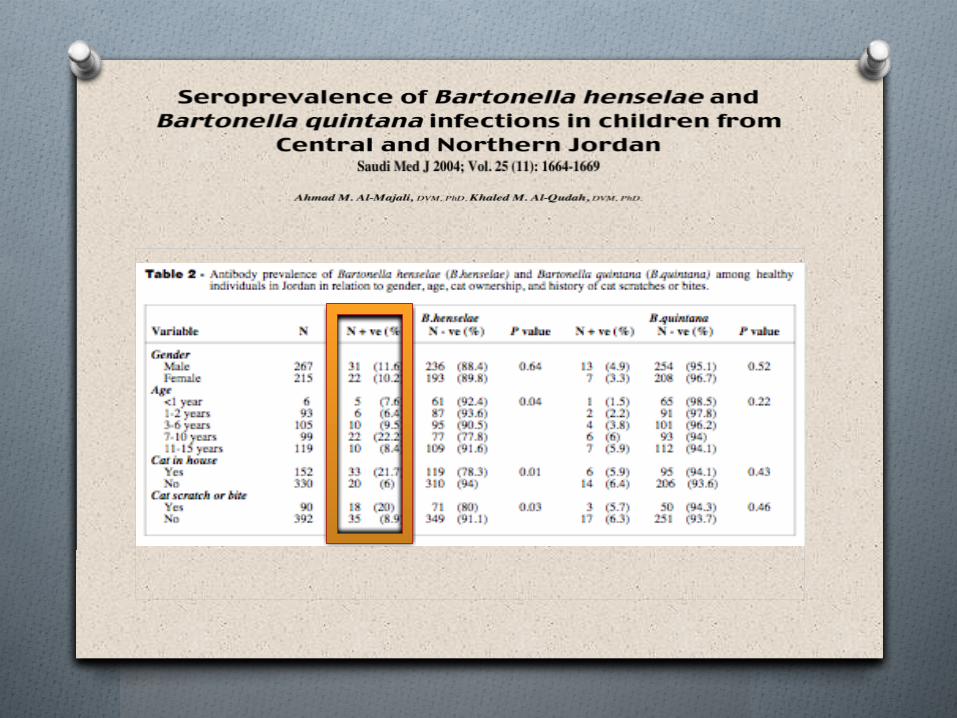
3. Ahmad M et al.Seroprevalence of Bartonella henselae and Bartonella quintana infections in children from Central and Northern Jordan Saudi Med J 2004; Vol.25(11): 1664-1669
4. Bass et al. Prospective randomized double-blind placebo- controlled evaluation of azithromycin for the treatment of cat-scratch disease. Pediatr infect Dis J. 1998;17(6): 447-452
5. Frean et al. High Rate of Bartonella henselae infection in HIV-positive outpatients in Johannesburg, South Africa. Trans Royal Soc. Trop Med. Hyg., 2002;96:549-550