bacterial overgrowth and ibs: causation, association, or neither? brennan spiegel, md, mshs
TRANSCRIPT

Bacterial Overgrowth and IBS: Causation, Association, or Neither?
Brennan Spiegel, MD, MSHS


The Brain-Gut Axis
Central nervoussystem (CNS)
Enteric nervoussystem (ENS)
Dysbiosis“Leaky” gutLow-grade inflammationVisceral hypersensitivityDysmotility
Brain-gut axis
Higher brain activation in response to stress
Thinner grey matter density
Altered amygdala reactivity
Mayer E. et al; Gastroenterol 2010;139:48
Mayer E. et al; Gastroenterol 2011;140:1943

Susceptible Host
Disease Expression
“Hit”Stress InfectionDietAllergy
Evolving IBS Disease Model
Underlying dysfunction in:• Intestinal dysbiosis • Mast cell number and function• Serotonin trafficking• HPA Axis• Cortical pain processing

Dietary factorsHigh sorbitol diet
High-fiber dietFODMAP Diet
Caffeine Alcohol
InflammationUlcerative colitisCrohn’s disease
Microscopic colitis
EndocrineHyperthyroidism
DiabetesCarcinoid
Gastrinoma
Psychological
AnxietySomatizationDepression
PTSD
InfectionSIBOC. diff
Giardiasis
MalabsorptionCeliac sprue
Carb intolerancePancreatic disease
Bile acid malabsorption
Existential Question: What Is IBS?
IBS

Is IBS an absence of other things?
Or is it some thing… unto itself?
IBS

InflammationAltered brain–
gut interactions
Visceral hypersensitivity
Geneticfactors
Psychosocialfactors
Bacterial-Host Interactions
IBSIBS
Proposed Pathophysiological Mechanisms Involved in IBS

IBS “Look-Alikes”
Bacterial overgrowth
Giardiasis
Hyperthyroidism
IBD
Lactose intolerance
Infectious colitis
Microscopic colitis
Celiac sprue
Diagnostic Battery is Extensive
Diagnostic Battery
Breath-testing
Stool Ova & Parasites
Thyroid function testing
ESR / CRP / Colonoscopy
Breath-testing
Stool leukocytes / C&S / C. diff
Colonoscopy / Flexsig
Sprue Serologies
Performing the wrong tests can lead to excessive
resource utilization and worsen patient outcomes
Performing the wrong tests can lead to excessive
resource utilization and worsen patient outcomes

IBS “Look-Alikes”
Bacterial overgrowth
Giardiasis
Hyperthyroidism
IBD
Lactose intolerance
Infectious colitis
Microscopic colitis
Celiac sprue
Diagnostic Battery is Extensive
Diagnostic Battery
Breath-testing
Stool Ova & Parasites
Thyroid function testing
ESR / CRP / Colonoscopy
Breath-testing
Stool leukocytes / C&S / C. diff
Colonoscopy / Flexsig
Sprue Serologies

“A revolutionary tool in the way irritable bowel syndrome is currently
being treated”
“A revolutionary tool in the way irritable bowel syndrome is currently
being treated”
“I am convinced that the primary cause of IBS is bacterial overgrowth –
‘The New Culprit’”
“I am convinced that the primary cause of IBS is bacterial overgrowth –
‘The New Culprit’”

duodenum jejunum ileum colon
100 103 106 1011
Normal Distribution Intestinal Flora
aerobes aerobesanaerobes

duodenum jejunum ileum colon
SIBO = >105 CFU/ml of “colonic type bacteria” in SI
e.g. gram negatives, anaerobes, enterococci
Aspirate
H2
breath tests
glucoselactulose
Normal Distribution Intestinal Flora

Lactulose Hydrogen Breath Test
H 2
H2
H2
PPM
Lactulose
min 900
cecum
colonic fermentation
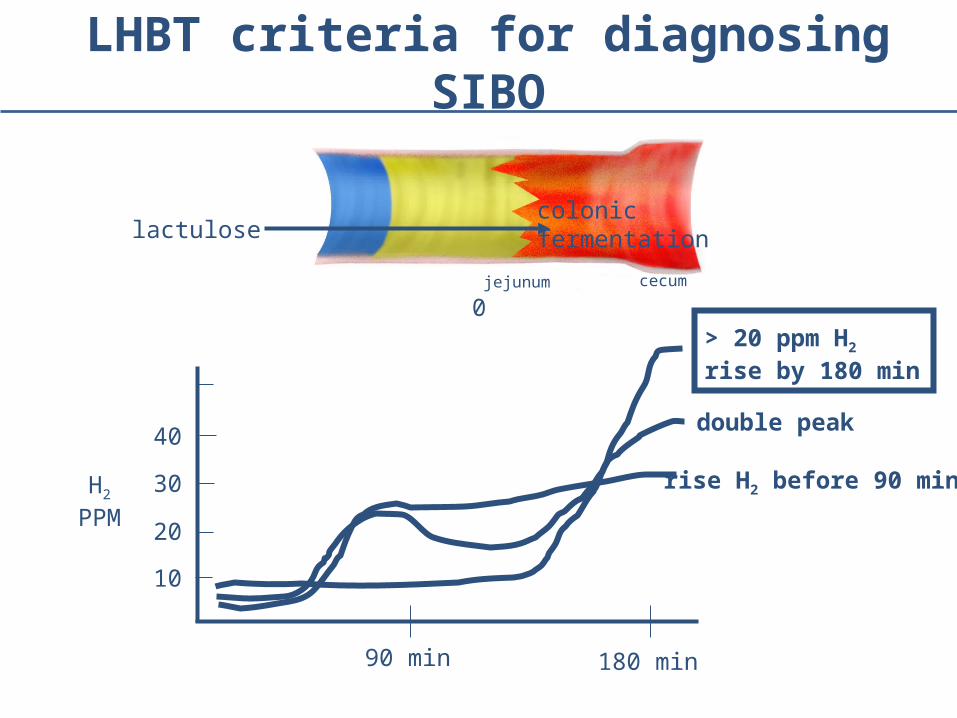
LHBT criteria for diagnosing SIBO
H2
PPM
90 min 180 min
0
colonic fermentationlactulose
10
20
30
40double peak
rise H2 before 90 min
> 20 ppm H2 rise by 180 min
jejunum cecum

Pimentel M et al. New Engl J Med 2011;364:22-32

Rifaximin in IBS
Pimentel M et al. New Engl J Med 2011;364:22-32

• It’s sensible that X could cause Y (biological plausibility)
• Competing mechanisms are less plausible (coherence)
• Most studies show X and Y are related (consistency)
• X comes before Y (temporal relationship)
• Removal of X removes or improves Y
• Therapies targeting X are most effective for Y (effect size)
• Nothing gets between X and Y (lack of confounding)
Does X Cause Y? Criteria for Causation
Hill, B. Proc R Soc Med 1965;58:295
The LHBT was used to promulgate the SIBO hypothesis of IBS. But how do we know it even tests for SIBO?
Question

Yu et al. Gut 2011 60:334

“These finding demonstrate that an abnormal rise in hydrogen
measured in the LHBT can be explained by variations in oro-
cecal transit time in patients with IBS and therefore do not
support the diagnosis of SIBO.”
“These finding demonstrate that an abnormal rise in hydrogen
measured in the LHBT can be explained by variations in oro-
cecal transit time in patients with IBS and therefore do not
support the diagnosis of SIBO.”
“It seems probable that antibiotics reduce bloating in IBS by
suppressing species of bacteria in the colon, not the small
intestine. Altering colonic flora using alternative strategies to
antibiotics, such as pre or probiotics, may prove advantageou
s.”
“It seems probable that antibiotics reduce bloating in IBS by
suppressing species of bacteria in the colon, not the small
intestine. Altering colonic flora using alternative strategies to
antibiotics, such as pre or probiotics, may prove advantageou
s.”

• The test used to promulgate the SIBO hypothesis may not have measured SIBO in the first place.
• LHBT is probably a measure of colonic bacteria that are not displaced from the colon itself.
• LHBT data may simply indicate that dysmotility underlies IBS – something long established.
SIBO and IBS: Biological Plausibility?
Camilleri et al. CGH 2008;6:772Pimentel et al. DDs 2002;47:2639
Yu et al. Gut 2011 60:334

• In order for a risk factor to be the predominant cause of a disease, we should expect that competing hypotheses are less plausible.
•A causal theory is strongest when it does not conflict with other facts and there are no plausible competing theories.
SIBO and IBS: Biological Plausibility?
Hill, B. Proc R Soc Med 1965;58:295

SIBO and IBS:
Consistency among studies?

Prevalence of Abnormal* Lactulose Breath Tests in Rome I IBS
IBS Controls
100
0
50
Pimentel et al. Am J Gastro 2003;98:412
84%
20%
N=111 N=15
OR=26.2 (95% CI=4.7, 104)
*Single peak >20 ppm rise of H2 by 90 min
0
10
20
30
40
50
60
70
80
90
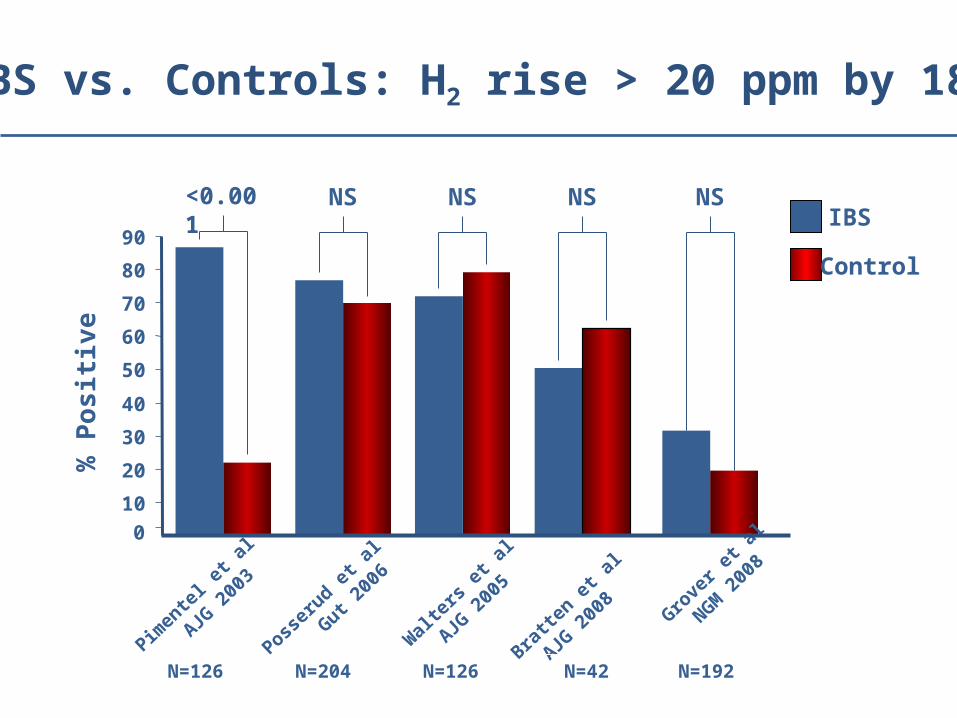
IBS vs. Controls: H2 rise > 20 ppm by 180%
Po
sit
ive
Pimen
tel e
t al
A
JG 2
003
<0.001IBS
Control
N=126
NS
Posser
ud et a
l
G
ut 200
6
N=204
NS
Wal
ters
et a
l
AJG 2
005
N=126
NS
Bratte
n et a
l
AJG
200
8
N=42
NS
Grove
r et a
l
NGM
200
8
N=192
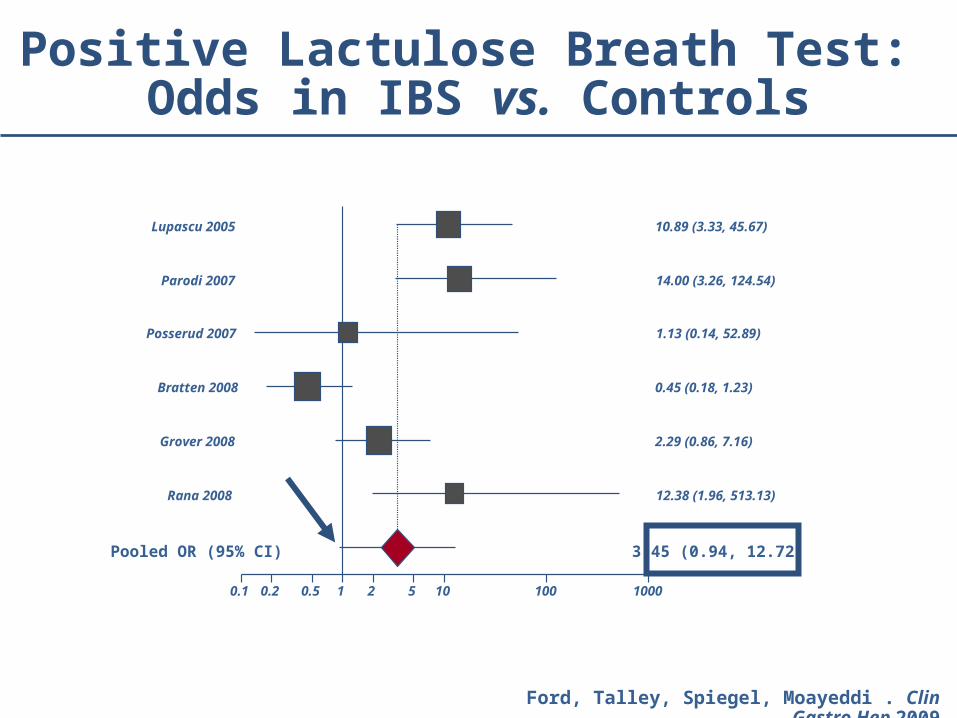
Positive Lactulose Breath Test: Odds in IBS vs. Controls
0.1 0.2 0.5 1 2 5 10 100 1000
Rana 2008 12.38 (1.96, 513.13)
Grover 2008 2.29 (0.86, 7.16)
Bratten 2008 0.45 (0.18, 1.23)
Posserud 2007 1.13 (0.14, 52.89)
Parodi 2007 14.00 (3.26, 124.54)
Lupascu 2005 10.89 (3.33, 45.67)
Pooled OR (95% CI) 3.45 (0.94, 12.72)
Ford, Talley, Spiegel, Moayeddi . Clin Gastro Hep 2009

SIBO and IBS:
Dose Response Relationship?

Clinical Relevance of Abnormal SI Bacterial Counts
Comparison Group Symptom Differences
>105 vs. <105 CFU/ml No difference in IBS symptoms
>103 vs. <103 CFU/ml No difference in IBS symptoms
LHBT double peak vs. no double peak No difference in IBS symptoms
Posserud et al. DDW 2009 AB#1052
“We found no clear association between symptoms and
culture verified SIBO, mildly increased small bowel
bacteria or abnormal LHBT. Thus, the clinical
importance of abnormal small bowel bacterial counts
in IBS patients is questionable.”
“We found no clear association between symptoms and
culture verified SIBO, mildly increased small bowel
bacteria or abnormal LHBT. Thus, the clinical
importance of abnormal small bowel bacterial counts
in IBS patients is questionable.”

SIBO and IBS:
Are treatments for SIBO more effective than treatments targeting other purported
mechanisms of IBS?

Rifaximin in IBS
Pimentel M et al. New Engl J Med 2011;364:22-32
NNT = 11NNT = 11

IBS Treatment NNT vs. PlaceboAntidepressants 4Antispasmodics 5Linaclotide* 5Alosetron* 8Rifaximin* 11Probiotics 11Fiber 11Lubiprostone* 13
Comparing NNTs of Available Pharmacotherapies for IBS
Spiegel B. Clinic Gastroenterol Hep. 2011;9:461
* Higher quality studies available to support NNT calculation

Even Peppermint Oil Looks Good in IBS
Ford A, Talley N, Spiegel B et al. Am J Gastroentrol 2008 Nov 13;337:a2313.
NNT = 2.5

NNT of “Placebo without Deception” in IBS?
4
Kaptchuk et al. PLoS One 2010;22:5

SIBO and IBS:
Lack of confounders?

I plan to use antibiotics regardless of the HBT or jejunal aspirate. In fact, I don’t
check the HBT anyway. Will clearing SIBO with rifaximin lead to a long-term cure?
Or will the SIBO just come back?
Question
50
40
30
20
10
0
% G
lc H
BT P
ositi
ve
3 Months
SIBO Recurrence Following Rifaximin
13%
6 Months 9 Months
28%
44%
Lauritano et al. Am J Gastroenterology 2008;103:2031
N=80
Predictors of SIBO Recurrence:
Older age (OR=1.09)
History of appendectomy (OR=5.9)
Use of proton pump inhibitors (OR=3.5)
Predictors of SIBO Recurrence:
Older age (OR=1.09)
History of appendectomy (OR=5.9)
Use of proton pump inhibitors (OR=3.5)

Relationship between PPI Use and Foregut Bacterial Counts
Thorens et al. Gut 1996; 35: 23-6.

Species Found in Foregut of Patients on PPIs
Fried et al. Gut 1994; 35;23-6.

PPIs as the Confounder: Could IBS Be Linked to SIBO Through PPIs?
Spiegel B, Chey W, Chang L. Am J Gastroenterol 2008;103

Causation?
1. Biological plausibility?
2. Consistency?
3. Lack of confounding?
4. Removing X provides cure or robust improvement in Y?
5. Removing X is most effective treatment for Y?
SIBO IBSCriteria for causation:
Yes No


Take-Away Messages
• Test used to promulgate SIBO hypothesis may not have measured SIBO in the first place
• A dose-response effect between intestinal microbiota and IBS symptoms is lacking
• The relationship between SIBO and IBS is inconsistent
• Therapies that do not address SIBO often outperform antibiotics – even “placebo without deception”
• PPIs confound the relationship between SIBO and IBS
• Bottom line: Bacteria may play a role in some symptoms in some patients, but are unlikely to be the predominant cause of IBS.