bacterial infections & acnecme.uthscsa.edu/presentations/peds2011/saturday/workshops/4_(2... ·...
TRANSCRIPT
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Bacterial Infections & Acne
Chad Hivnor, MD
Associate Program Director
Chief, Pediatric
Dermatology
San Antonio, Tx
Disclaimer
All authored materials and statements
constitute the personal statements of
Chad Hivnor, MD and are not intended to
constitute an endorsement by Wilford Hall
Medical Center, the US Air Force, or any
other Federal Government entity."
Perspective
Patients
Parents
Jrnl Am Acad Dermatol Apr 2007
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Epidemiology
Physiologic
85%
Familial
Only 20% visit dermatologist
Pro-active/OTC
Primary physicians
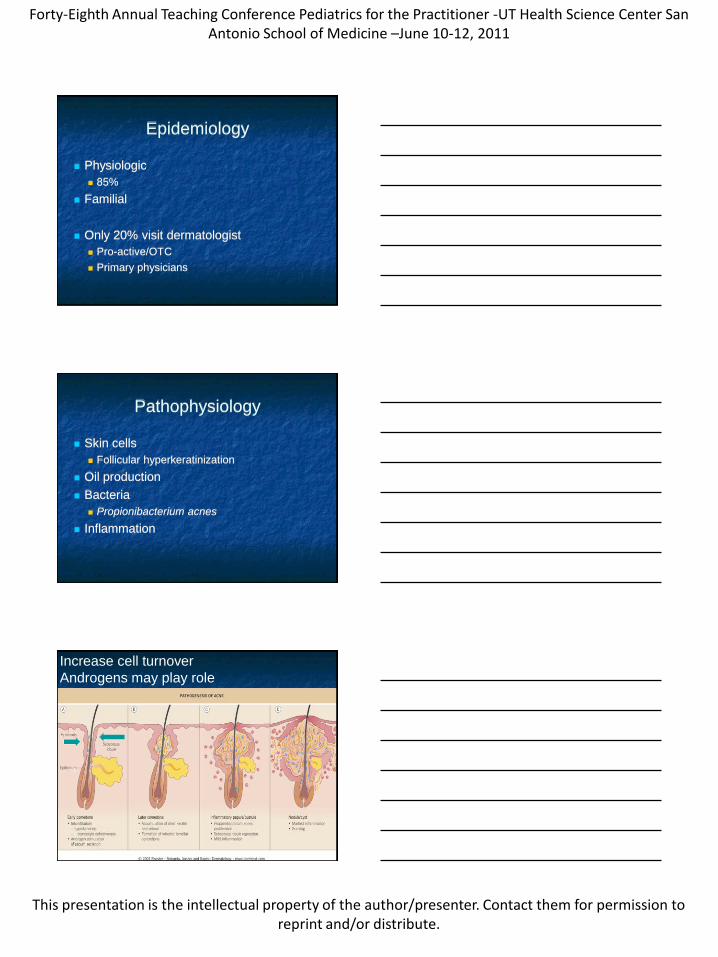
Pathophysiology
Skin cells
Follicular hyperkeratinization
Oil production
Bacteria
Propionibacterium acnes
Inflammation
Increase cell turnover
Androgens may play role
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
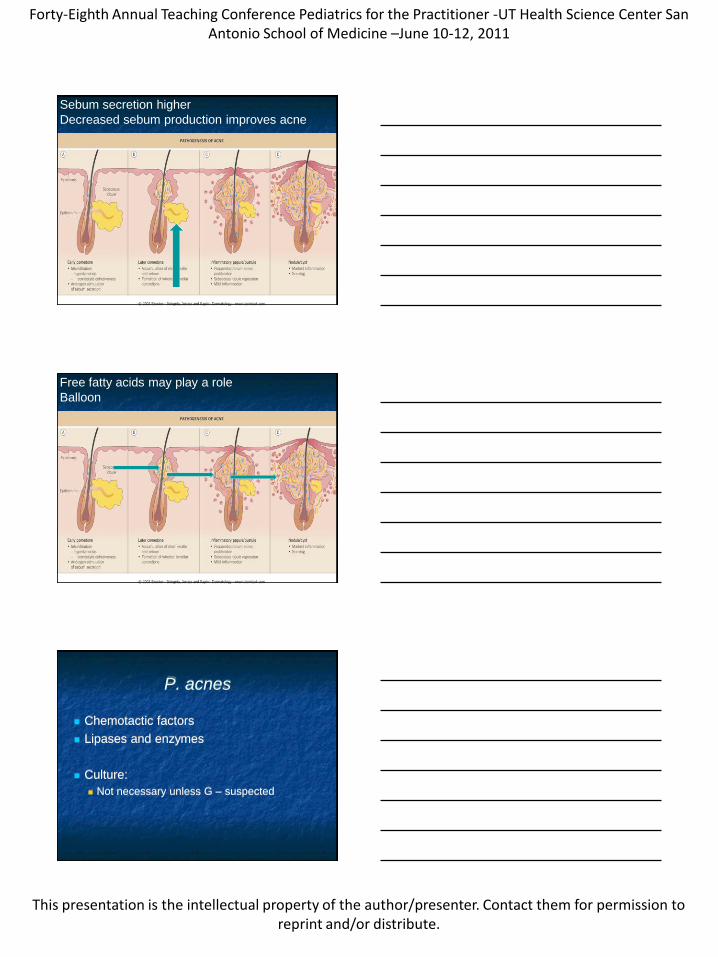
Sebum secretion higher
Decreased sebum production improves acne
Free fatty acids may play a role
Balloon
P. acnes
Chemotactic factors
Lipases and enzymes
Culture:
Not necessary unless G – suspected
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Aggrevating Factors
Popping
Occlusion
Friction/ Pressure
Medications
Stress
Other:
Drugs (steroids, lithium, INH)
Androgens (menses as example)
Aggrevating Factors
Endocrine Testing
Not indicated in most patients
Young child
Body odor, axillary/pubic hair, clitoromegaly
Adult women (PCOS)
Late-onset acne, menses, hirsutism, alopecia,
infertility, acanthosis nigricans
Acne Subtypes
Semantics
Recent Consensus Statement Most employ lesion counting & Global
5 point scale; mild mod severe
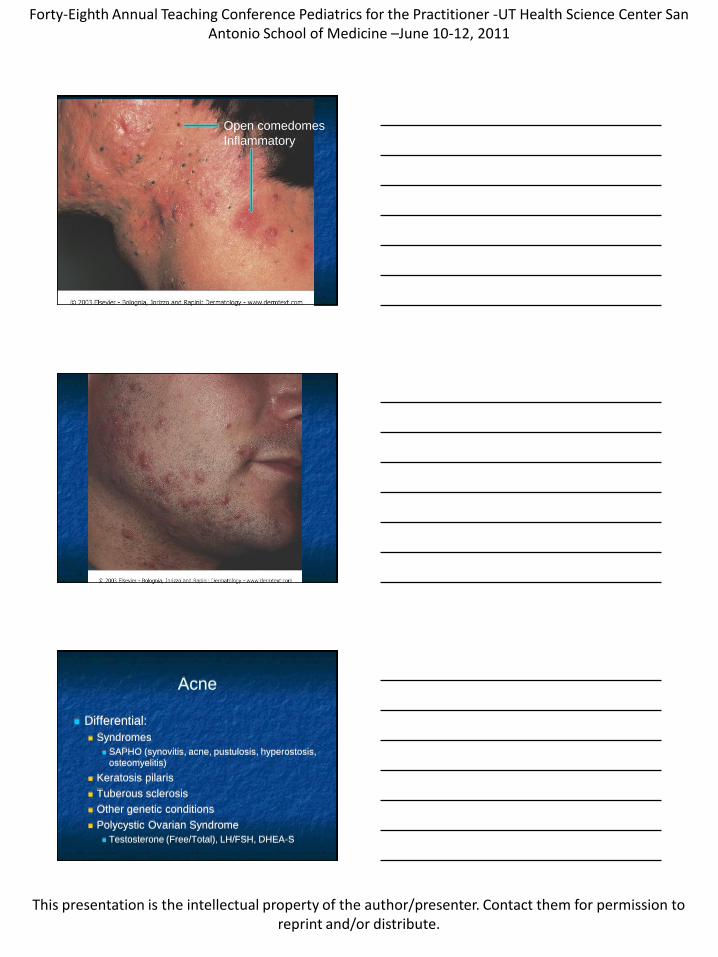
Non-inflammatory
Closed comedo
Open comedo
Inflammatory
Papules
Pustules
Nodules
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
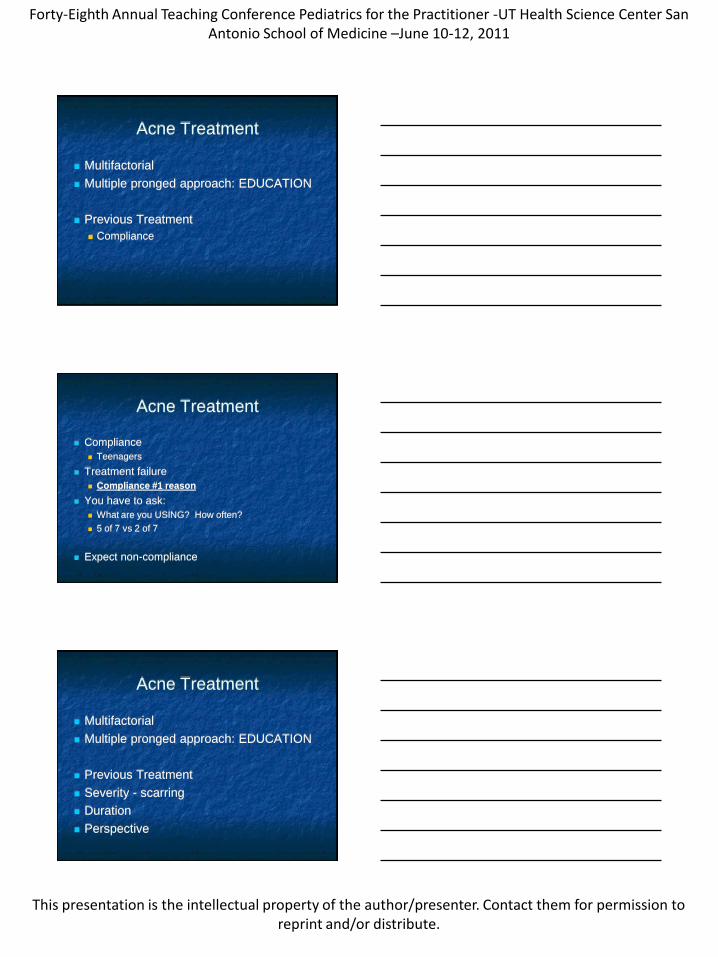
Open comedomes
Inflammatory
Acne
Differential:
Syndromes
SAPHO (synovitis, acne, pustulosis, hyperostosis,
osteomyelitis)
Keratosis pilaris
Tuberous sclerosis
Other genetic conditions
Polycystic Ovarian Syndrome
Testosterone (Free/Total), LH/FSH, DHEA-S
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Acne Treatment
Multifactorial
Multiple pronged approach: EDUCATION
Previous Treatment
Compliance
Acne Treatment
Compliance
Teenagers
Treatment failure
Compliance #1 reason
You have to ask:
What are you USING? How often?
5 of 7 vs 2 of 7
Expect non-compliance
Acne Treatment
Multifactorial
Multiple pronged approach: EDUCATION
Previous Treatment
Severity - scarring
Duration
Perspective
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Acne Treatment: Washing
Not a dirty problem: ―Fine china‖
Process:
Water
Salicylic acid wash – lather
Comedolytic
Lipophilic
Splash
Pat dry air dry
Acne Treatment
Retinoids
Benzoyl peroxide
Topical antibiotic
Combo of these 3
Work horse of acne
Combo is more effective than alone
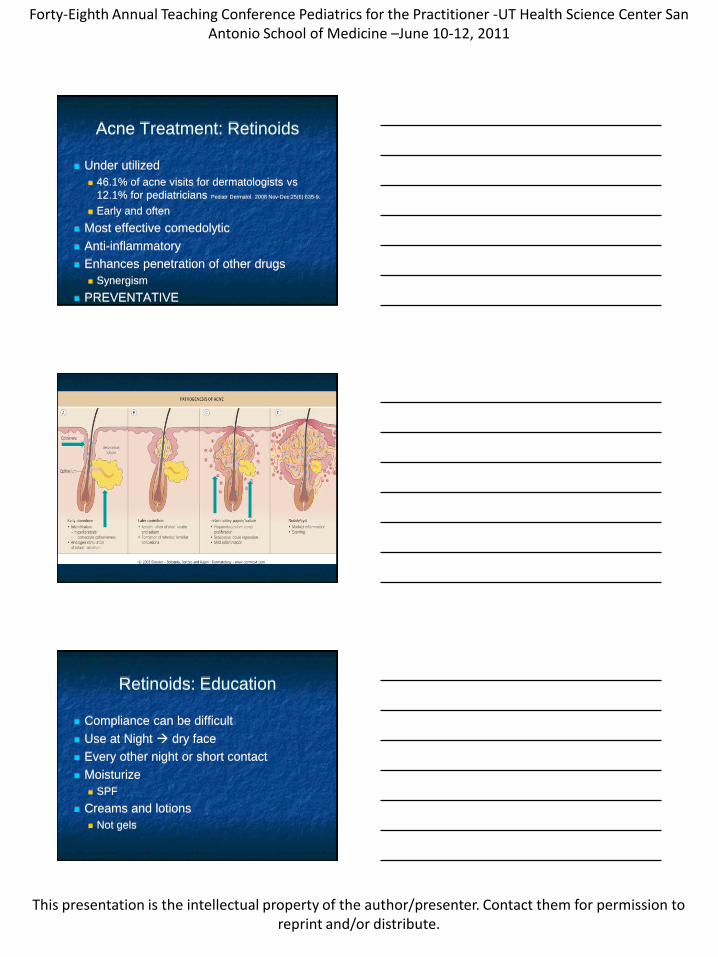
Pathophysiology
Follicular hyperkeratinization
Alter keratinization (Retinoid, Salicylic Acid, BP)
Oil production
Alter sebaceous gland (Retinoid, Salicylic Acid)
Bacteria
Decrease load (BP)
Inflammation
Anti-inflammatory (Retinoid)
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Acne Treatment: Retinoids
Under utilized
46.1% of acne visits for dermatologists vs
12.1% for pediatricians Pediatr Dermatol. 2008 Nov-Dec;25(6):635-9.
Early and often
Most effective comedolytic
Anti-inflammatory
Enhances penetration of other drugs
Synergism
PREVENTATIVE
Retinoids: Education
Compliance can be difficult
Use at Night dry face
Every other night or short contact
Moisturize
SPF
Creams and lotions
Not gels
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Acne Treatment:
Benzoyl peroxide
GREAT: anti-bacterial
Decrease bacterial population
Decrease hydrolysis of triglycerides
NO antibiotic resistance
Combo with oral and topicals essential
Consensus confirms
Treatment
Retinoids
Benzoyl peroxide
Topical antibiotic
Azelaic acid
Acne Treatment:
Azelaic Acid
Inflammatory > comedomal
Less irriation
Post inflammatory hyperpigmentation
Pregnancy Cat B
Consensus
Trial efficacy
Practice: not so much
Subset
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Treatment
Retinoids
Benzoyl peroxide
Topical antibiotic
Azelaic acid
Oral Antibiotic
Oral Antibiotic
Tetracycline
Doxycycline
Minocycline
Bactrim
Azithromycin
3-6 months
Use in combination
Oral Antibiotics
Erythromycin
Effective
High resistance rate
Pregnancy/ <8 yo
No ampicillin, amoxicillin or cephalexin
Should be avoided
Consensus
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Bacterial Resistance
Propionibacterium acnes
Clinically relevant
Cross resistance
S. aureus in nares
Streptococci in oral cavity
Enterobacteria in gut
―S. pyogenes colonization and resistance in the
oropharynx are associated with antibiotic therapy in
patients with acne.‖
Antibiotics
Two fold risk
URI/ UTI
Margolis DJ et al. Arch Dermatol 2005;141:1132-6
―Benzoyl-peroxide-based treatment is the
most evidence-based approach‖… to
prevent antibiotic resistance Expert Opin Pharmacother. 2011 Feb 29 (Epub)
Bacterial Resistance
Propionibacterium acnes
Clinically relevant
Cross resistance
S. aureus in nares
Streptococci in oral cavity
Enterobacteria in gut
Benzoyl peroxide use
Compliance
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Treatment
Retinoids
Benzoyl peroxide
Topical antibiotic
Azelaic acid
Oral Antibiotic
Others (Dermatologist)
Spironlactone
Accutane
Accutane
Dryness
May lead to S. aureus colonization
Depression
Some patients with challenge/ rechallenge
No causal relationship
Lipids
Arthralgias
Hyperostosis & epiphyseal closure
No screening
Acne Summary
Follicular hyperkeratosis
Bacterial proliferation
Excess sebum
Inflammation
Excess androgen stimulation
Decrease manipulation
Compliance with medications
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Acne - Mild
Comedomal
Retinoid
Salicylic Acid
Papular/ Pustular
Retinoid
Combination (benzoyl peroxide/clindamycin)
Salicylic Acid
Acne - Moderate
Oral antibiotic
Retinoid
Benzoyl peroxide (combination)
Salicylic acid
Women – spironlactone
OCP
Acne - Severe
Isotretinoin
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Gram Positive OrganismsStaphylococcal Infections
Staphylococcal Cutaneous
Manifestations
Impetigo—bullous and nonbullous
Folliculitis/Furunculosis
Pyodermas
Botromycosis
Paronychia
Pyomyositis
Staph Scalded Skin Syndrome
Toxic Shock Syndrome
Septic Emboli
Staphylococcal Infections S. aureus is a normal inhabitant of the anterior
nares in 20% -40% of adults
MRSA Suspected if:
Local resistance patterns,
Lack of response to initial Antibiotics
Predisposing Factors:
Age > 65
Exposure to MRSA+ infection
Recent hospitalization
Chronic illness – i.e. HIV, Atopic Dermatitis
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
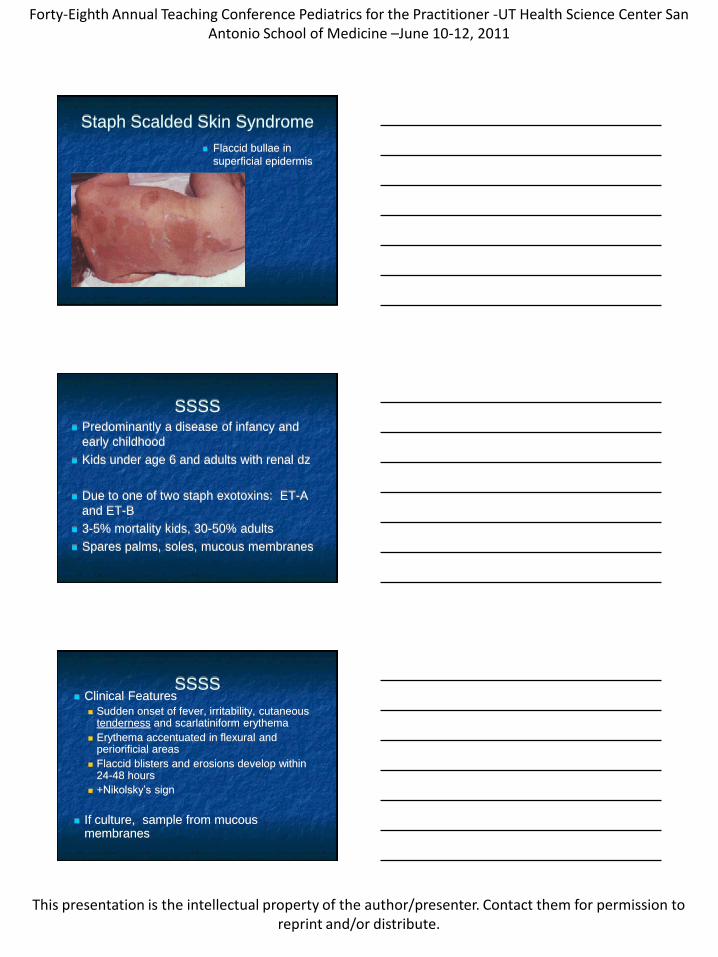
Staph Scalded Skin Syndrome
Flaccid bullae in
superficial epidermis
SSSS Predominantly a disease of infancy and
early childhood
Kids under age 6 and adults with renal dz
Due to one of two staph exotoxins: ET-A
and ET-B
3-5% mortality kids, 30-50% adults
Spares palms, soles, mucous membranes
SSSS Clinical Features
Sudden onset of fever, irritability, cutaneoustenderness and scarlatiniform erythema
Erythema accentuated in flexural and periorificial areas
Flaccid blisters and erosions develop within 24-48 hours
+Nikolsky’s sign
If culture, sample from mucous membranes
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
SSSS
Infections leading to SSSS typically
originate in the nasopharynx
Other foci of infection
Umbilicus
Urinary tract
Conjunctivae
Blood
Treatment
Beta-Lactamase resistant (Diclox,
Cephalexin) x 1 week
Supportive skin care
Isolation of newborns
Fluid and electrolyte management
Identify and treat S. aureus carriers
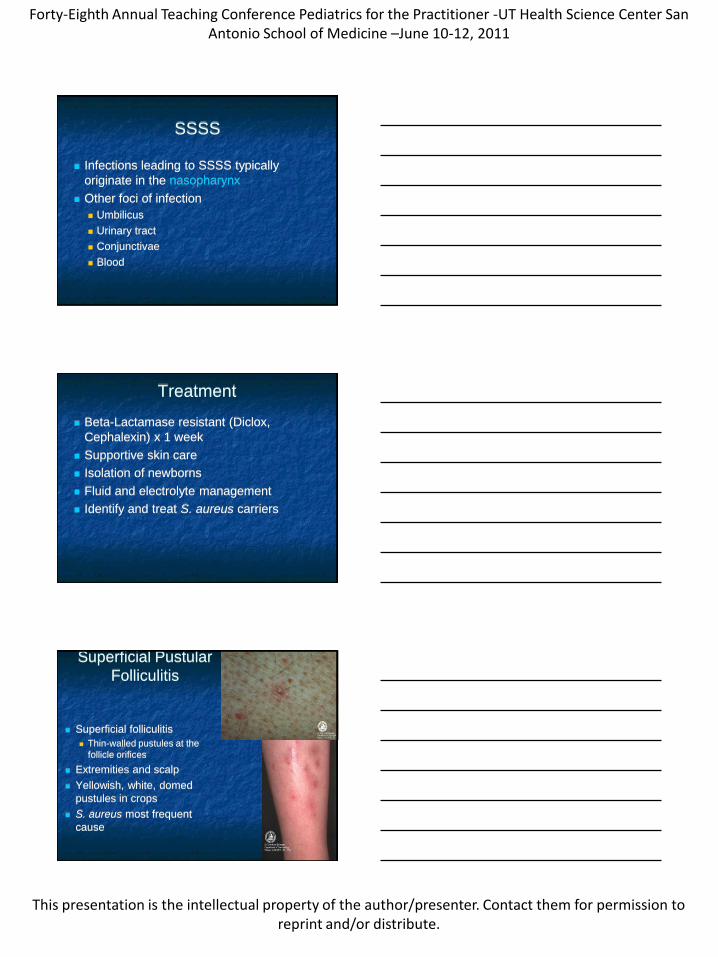
Superficial Pustular
Folliculitis
Superficial folliculitis
Thin-walled pustules at the
follicle orifices
Extremities and scalp
Yellowish, white, domed
pustules in crops
S. aureus most frequent
cause
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
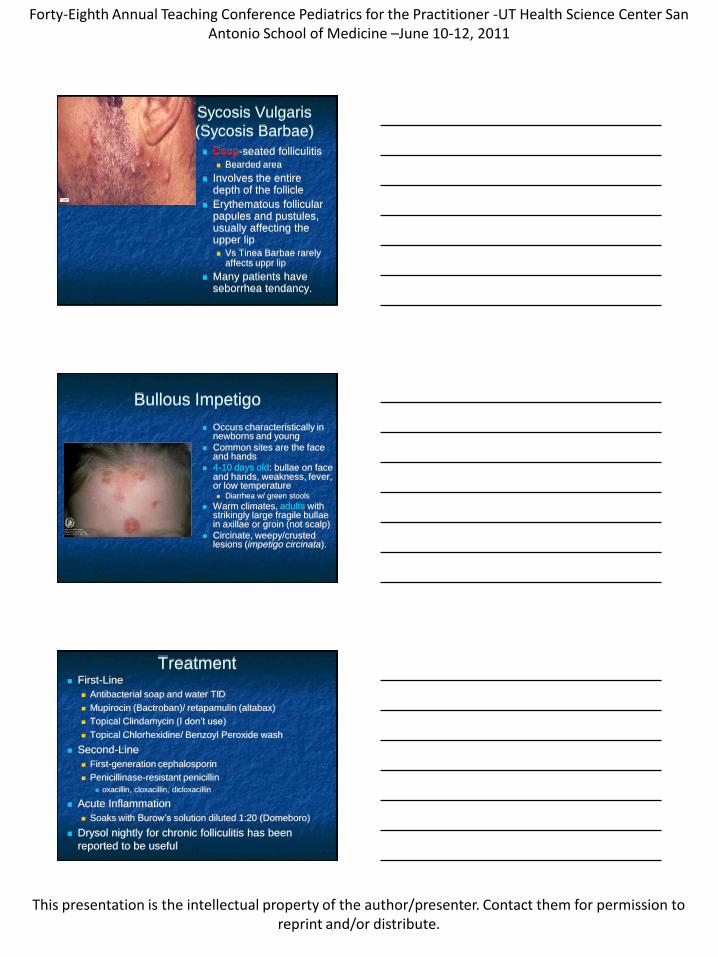
Sycosis Vulgaris
(Sycosis Barbae)
Deep-seated folliculitis
Bearded area
Involves the entire depth of the follicle
Erythematous follicular papules and pustules, usually affecting the upper lip
Vs Tinea Barbae rarely affects uppr lip
Many patients have seborrhea tendancy.
Bullous Impetigo
Occurs characteristically in newborns and young
Common sites are the face and hands
4-10 days old: bullae on face and hands, weakness, fever, or low temperature Diarrhea w/ green stools
Warm climates, adults with strikingly large fragile bullaein axillae or groin (not scalp)
Circinate, weepy/crusted lesions (impetigo circinata).
Treatment First-Line
Antibacterial soap and water TID
Mupirocin (Bactroban)/ retapamulin (altabax)
Topical Clindamycin (I don’t use)
Topical Chlorhexidine/ Benzoyl Peroxide wash
Second-Line
First-generation cephalosporin
Penicillinase-resistant penicillin
oxacillin, cloxacillin, dicloxacillin
Acute Inflammation
Soaks with Burow’s solution diluted 1:20 (Domeboro)
Drysol nightly for chronic folliculitis has been
reported to be useful
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
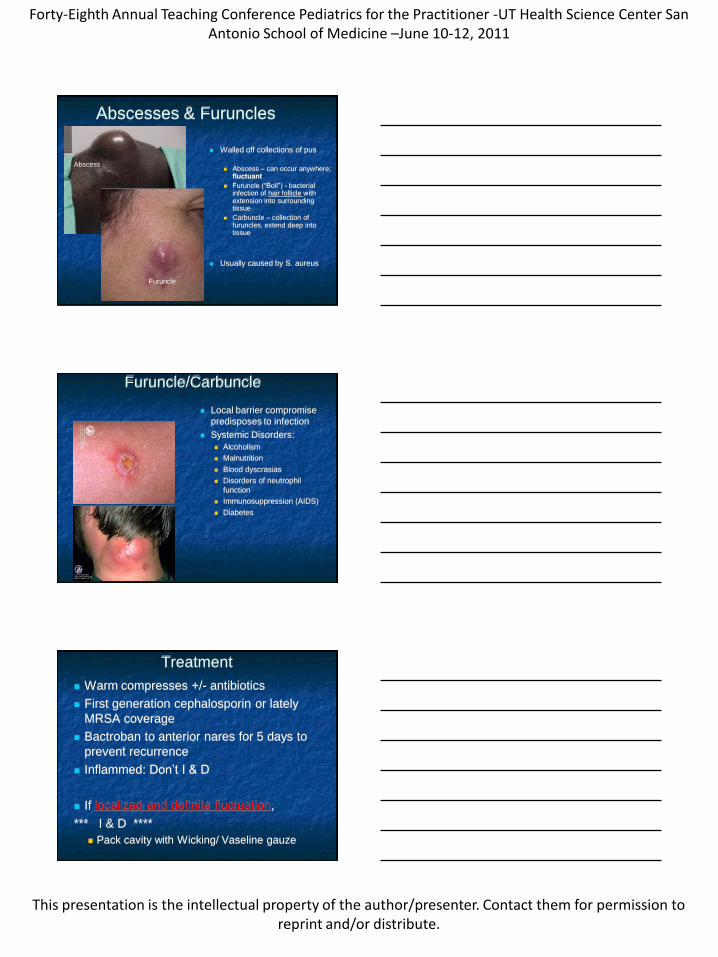
Abscesses & Furuncles
Walled off collections of pus
Abscess – can occur anywhere; fluctuant
Furuncle (―Boil‖) - bacterial infection of hair follicle with extension into surrounding tissue
Carbuncle – collection of furuncles, extend deep into tissue
Usually caused by S. aureus
Furuncle
Abscess
Furuncle/Carbuncle
Local barrier compromise
predisposes to infection
Systemic Disorders:
Alcoholism
Malnutrition
Blood dyscrasias
Disorders of neutrophil
function
Immunosuppression (AIDS)
Diabetes
Treatment
Warm compresses +/- antibiotics
First generation cephalosporin or lately
MRSA coverage
Bactroban to anterior nares for 5 days to
prevent recurrence
Inflammed: Don’t I & D
If localized and definite fluctuation,
*** I & D ****
Pack cavity with Wicking/ Vaseline gauze
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
Staph/MRSA
Options
Sensitivities: Key to culture
Doxycycline/ Minocycline
Bactrim
Prevention: Self- Contamination
Clorox baths
Benzoyl peroxide wash
Zinc pyrithione: prevents binding
Chlorhexidine: daily bath reduced incidence
MRSA
I&D
Know susceptibilities locally
Don’t forget rifampin;
Colonization
Creams, bar soap, towels, BP cuffs, Gym
lockers/ mats, Day care changing table,
Also follows Strep pharyngitis
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
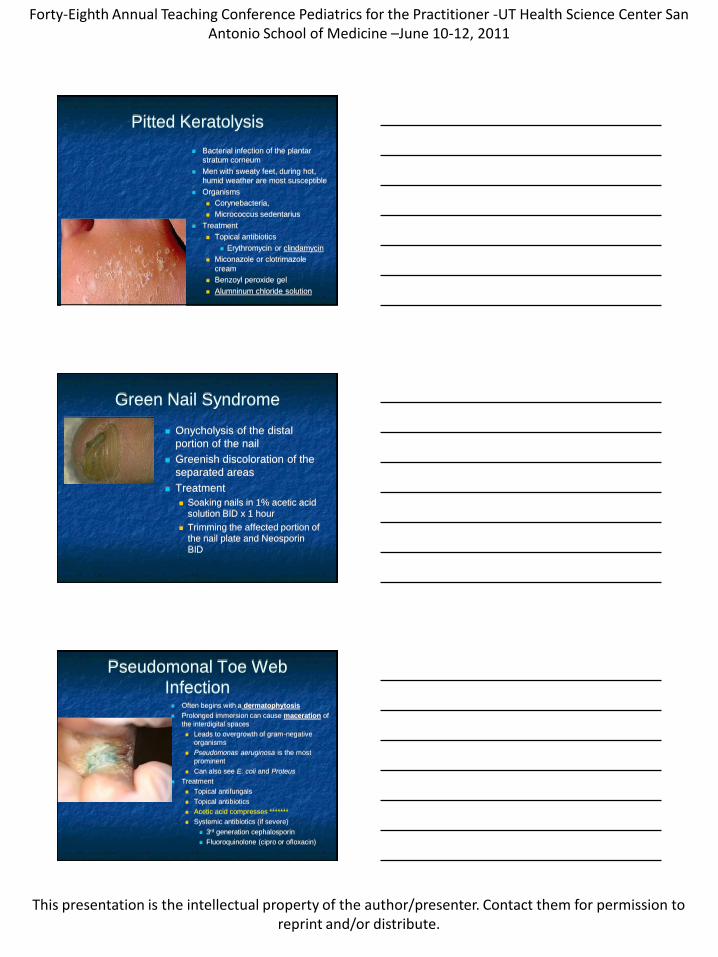
Pitted Keratolysis
Bacterial infection of the plantar
stratum corneum
Men with sweaty feet, during hot,
humid weather are most susceptible
Organisms
Corynebacteria,
Micrococcus sedentarius
Treatment
Topical antibiotics
Erythromycin or clindamycin
Miconazole or clotrimazole
cream
Benzoyl peroxide gel
Alumninum chloride solution
Green Nail Syndrome
Onycholysis of the distal
portion of the nail
Greenish discoloration of the
separated areas
Treatment
Soaking nails in 1% acetic acid
solution BID x 1 hour
Trimming the affected portion of
the nail plate and Neosporin
BID
Pseudomonal Toe Web
Infection Often begins with a dermatophytosis
Prolonged immersion can cause maceration of
the interdigital spaces
Leads to overgrowth of gram-negative
organisms
Pseudomonas aeruginosa is the most
prominent
Can also see E. coli and Proteus
Treatment
Topical antifungals
Topical antibiotics
Acetic acid compresses *******
Systemic antibiotics (if severe)
3rd generation cephalosporin
Fluoroquinolone (cipro or ofloxacin)
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine –June 10-12, 2011
This presentation is the intellectual property of the author/presenter. Contact them for permission to reprint and/or distribute.
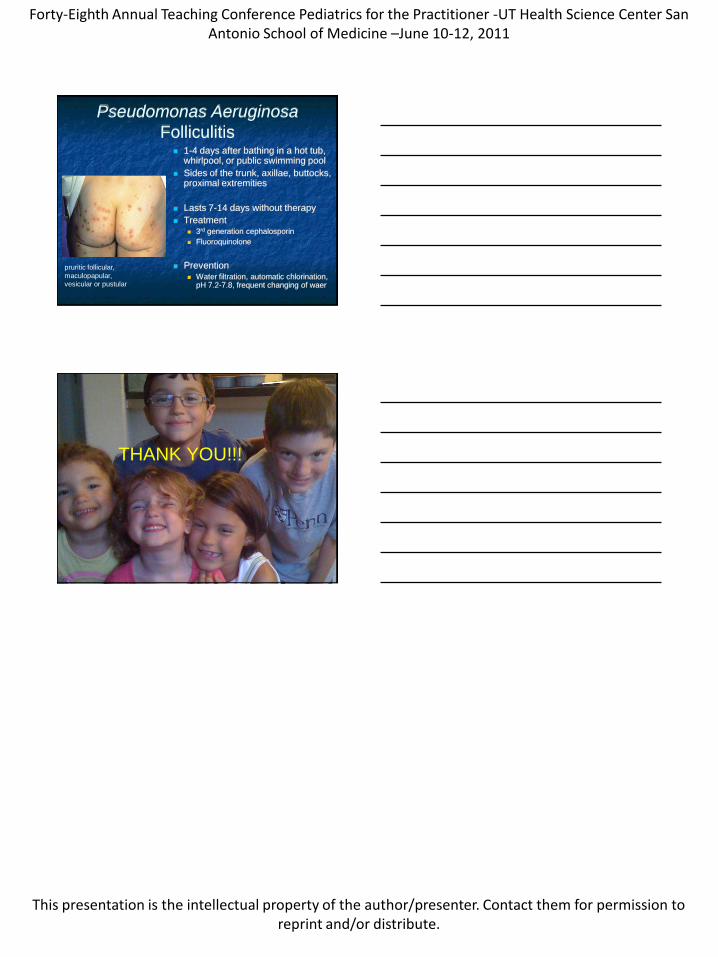
Pseudomonas Aeruginosa
Folliculitis 1-4 days after bathing in a hot tub,
whirlpool, or public swimming pool
Sides of the trunk, axillae, buttocks, proximal extremities
Lasts 7-14 days without therapy
Treatment 3rd generation cephalosporin
Fluoroquinolone
Prevention Water filtration, automatic chlorination,
pH 7.2-7.8, frequent changing of waer
pruritic follicular,
maculopapular,
vesicular or pustular
THANK YOU!!!