bachelor in science nursing · bachelor in science nursing (bsc)(cur) research proposal an...
TRANSCRIPT
Bachelor in Science Nursing
(Bsc)(Cur)
Research Proposal
An exploration of the knowledge and experiences of
Mental Health Nurses in the screening for metabolic syndrome among
people with Serious Mental Illness.
Research Proposal submitted to University of Dublin Trinity College,
in partial fulfillment of the requirements for the Bachelor in Science
(Nursing) (B.sc. (Cur.))
Wednesday 10th
March 2010
2
DECLARATION:
I hereby declare that this Research Proposal which I now submit for assessment is entirely
my own work and has not been submitted an exercise for assessment at this or any other
University.
Signed: _______________________
Print Name: _____________________________
Date: _____________________
3
ACKNOWLEDGEMENTS
I would like to extend my gratitude to my facilitator for her academic guidance and
understanding during this project. I would also like to thank the research module leader and
my personal tutor for their support and assistance. Finally I would also like to thank my
fellow classmates for being part of a great learning environment throughout this course and
my family for their understanding for the duration of this degree.
4
Table of Contents Declaration ...................................................................................................................................... 2
Acknowledements ........................................................................................................................... 3
Table of Contents ............................................................................................................................ 4
Abstract; .......................................................................................................................................... 6
Chapter One .................................................................................................................................. 7
1.1 Identifying the area of interest ............................................................................................... 7
1.2 Literature Review- Introduction ............................................................................................. 8
1.2.1 Metabolic Syndrome and SMI. .............................................................................................. 8
1.2.2 Screening Methods ................................................................................................................. 9
1.2.3 Current screening practice ................................................................................................... 11
1.2.4 MHN‟s knowledge and practices of MetS. .......................................................................... 12
1.2.5 Conclusion ........................................................................................................................... 13
1.3 Research Question: .............................................................................................................. 14
1.4 Aim: ..................................................................................................................................... 14
1.5 Objectives: ........................................................................................................................... 14
Chapter Two ................................................................................................................................ 15
2.1 Design/proposed methodology: ........................................................................................... 15
2.2 Population/Sample ............................................................................................................... 16
2.2.1 Sampling Criteria ................................................................................................................. 17
2.2.2 Access to research site and participant recruitment ............................................................. 17
2.3 Data Collection .................................................................................................................... 18
2.3.1 Semi-structured interviews. ................................................................................................. 18
2.3.2 The Interview ....................................................................................................................... 18
2.4 Rigor and Trustworthiness ................................................................................................... 19
2.4.1 Credibility ............................................................................................................................ 20
2.4.2 Dependability ....................................................................................................................... 20
2.4.3 Confirmability ...................................................................................................................... 20
2.4.4 Transferability ...................................................................................................................... 20
2.5 Data Analysis ....................................................................................................................... 21
2.6 Pilot study ............................................................................................................................ 22
2.7 Ethical considerations .......................................................................................................... 22
2.7.1 Informed consent.................................................................................................................. 22
2.7.2 Protection of participants ..................................................................................................... 23
5
2.7.3 Confidentiality and Anonymity ........................................................................................... 23
Chapter 3 ..................................................................................................................................... 24
3.1 Proposed Outcomes of Study. ............................................................................................... 24
3.1.2Limitations ............................................................................................................................ 24
3.1.3Research Dissemination ........................................................................................................ 25
3.2 Resources: ............................................................................................................................. 25
3.3 Gantt Chart ............................................................................................................................ 26
Appendix 1 World Health Organization (1999) Metabolic Syndrome definition....................... 27
Appendix 2. International Diabetes Federation(2005) Metabolic Syndrome definition .............. 28
Appendix 3 Inclusion and exclusion criteria ............................................................................... 29
Appendix 4 Letter to the Director of Nursing. ............................................................................ 30
Appendix 5 Letter to Gatekeeper/CNM III. ................................................................................ 32
Appendix 6 Information Leaflet ................................................................................................. 34
Appendix 7 Invitation to participate ........................................................................................... 37
Appendix 8 Letter to TCD research Ethics committee ............................................................... 38
Appendix 9 Letter to health service research ethics committee .................................................. 40
Appendix 10 Consent Form .......................................................................................................... 42
Appendix 11 Interview guide ........................................................................................................ 43
Appendix 12 Colaizzi‟s (1978) seven step framework. ................................................................ 44
References. ........................................................................................................................................
6
Abstract;
Historically people with serious mental illness(SMI) have suffered higher rates of physical
illness and premature mortality compared to the general population leading to some authors
describing it as a „life shortening disease‟ (Allebeck, 1989). Metabolic Syndrome (MetS)
comprises a cluster of metabolic abnormalities that increase the risk of cardiovascular disease
and has been identified as a significant pathological threat to people with SMI with prevalence
rates in these populations exceeding general population rates.
High rates of MetS in people with SMI have been attributed to unhealthy lifestyles; iatrogenic
effects of medication and genetic predisposition with international consensus groups calling for
comprehensive screening of these populations. Current practice does not reflect these
recommendations although specific screening tools have been developed ranging from simple
cost effective measures to more systematic tools. Mental health nurses (MHN‟s) have been
identified as a group that are in an ideal position to help tackle this emerging pathological threat.
The literature however suggests that MHN‟S may have a lack of knowledge and confidence in
the assessment and interpretation of MetS parameters and also a desire for further training in this
area. However there is little known about MHN‟s current practices in screening for MetS.
The purpose of this study is to explore the knowledge and experiences of MHN‟s working in an
acute unit in the screening for MetS among people with SMI. The method employed for this
study will be a qualitative descriptive approach utilising a purposive sample of 10 nurses
working in an acute in-patient unit. Data collection will be through semi-structured interview
supported by an interview schedule. Participants responses will be audio-taped, transcribed
verbatim and analysed using Collaizzi‟s (1978) framework. The final report will comprise
themes and sub-themes that have emerged from the data reflecting the totality of the participants
experiences.
It is envisaged that the findings of this study can provide insight into current practices of
screening for MetS. This can lead to recommendations for the development of local policies and
specific screening methods and the provision of further training if deemed necessary.
Dissemination of findings will be aimed at local, national and international forums with eventual
publication in peer reviewed nursing journals.
7
Chapter 1
1.1 Identifying the area of interest
The first broad definition of Metabolic Syndrome(MetS) was by the World Health Organisation
(1999)(Appendix 1), with the latest from the International Diabetes Federation (IDF)(2005)
(Appendix 2). Although these organisations differ in MetS diagnostic criteria Alberti et al,
(2005) states they are congruent on the core components of MetS: obesity, hypertension,
dyslipidemia and insulin resistance. This insulin resistance increases the risk of developing
cardiovascular disease(CVD) and type 2 Diabetes Mellitus(DM) both of which greatly
contribute to the premature mortality of people with serious mental illness(SMI) (Meyer and
Stahl, 2009).
As a result international consensus groups have developed guidelines for the screening of MetS
(Barnett et al,2004;Clark,2004;Lambert and Chapman,2004;Marder et al,2004 and
DeNayer,2005) among people with SMI. Minimum screening should then incorporate body mass
index(BMI), waist circumference at the level of the umbilicus, blood pressure(BP), fasting
plasma glucose(FPG), and a fasting lipid profile, results of which will indicate diagnostic criteria
for MetS(Cohn and Sernyak, 2006).
The rationale for this research proposal was borne out of the researchers interest in the scale of
premature mortality among people with SMI. This interest originates from 12 years of working
in a rehabilitative training centre in Dublin. Over this time the author noticed high levels of poor
physical health among clients attending the centre and also premature deaths particularly of a
cardiovascular nature. On commencing this proposal the author examined the area further and
discovered that a lot of the literature has noted stark excess mortality among people with SMI in
comparison to the general population (Brown, 1997;Harris and Barraclough, 1998;Saha et al,
2007). Furthermore while mortality rates decline among western populations they have remained
static among groups with SMI and in some categories increased thereby widening the differential
mortality gap (Saha et al, 2007).
8
This area of study was extremely broad and in aiming to focus clearly the concept of Metabolic
Syndrome (MetS) was identified as a contemporary physical health priority for Service Users
and Mental Health Nurses(MHN‟s). Therefore the researcher has chosen the Screening for MetS
as the topic for this research proposal.
1.2 Literature Review- Introduction
This literature review will critically and objectively analyse screening practices for MetS among
people with SMI within contemporary MH services. This author will attempt to briefly elucidate
the relationship between SMI and MetS and then fracture the review under themes of; Screening
methods; Current practice; and MHN‟s knowledge and practices of MetS.
The search strategy involved key words; Syndrome x, Metabolic Syndrome, insulin resistance
syndrome, mental health, psychiatric, weight gain, obesity, medication, antipsychotic, and
screening. Internurse, Cinahl, Web of knowledge and Proquest databases were searched from
1997 to 2010. Explicit arrangements of key words incorporating „screening‟ revealed few
definite studies however one article was identified and the ancestry approach uncovered further
articles. Grey literature was discovered following contact with an Irish author and manual
searching revealed further papers.
The literature is heavily influenced by consensus, review and commentary with this author
having difficulty sourcing actual research studies. Sources of literature stem primarily from
Australian, European and American authors and predominant research designs encapsulate
outcome/evaluative research utilising quantitative methodologies. Almost all the literature was
focused on prevalence, prevention and management of MetS with little discovered about nursing
practice, knowledge or roles. The studies found in relation to nurses input were often embedded
in larger studies of prevalence as illustrated in the last theme.
1.2.1 Metabolic Syndrome and SMI.
Serious mental illness although a term commonly used is one that has broad subjective meaning
depending on the context in which it is used. Cahill and Jackson (2008) define SMI as “any DSM
[diagnostic and statistical manual] mental disorder leading to substantial functional impairment”.
9
Throughout the literature however and in the context of physical co-morbidity SMI primarily
refers to schizophrenia, bipolar or schizo-affective disorder (Ohlsen et al, 2005; White et al,
2009).
The association between SMI and high prevalence rates of MetS have been attributable in the
literature primarily to lifestyle factors, genetic predisposition and iatrogenic effects of
Medication. Lifestyle factors have been identified as excessive smoking, lack of exercise and
poor diets of people with SMI (Brown et al 1999), (McCreadie 2003) with this latter McCreadie
study reporting 10 year risk of coronary heart disease over 40% greater than the general
population. The indirect iatrogenic effects of antipsychotic (AP) medication have also been
proposed as contributory factors in the exacerbation of MetS (Jones and Jones, 2008; Jarboe,
2007). The non industry funded Clinical Antipsychotic Trials of Intervention Effectiveness
(CATIE) identified a link between atypical antipsychotics and the development and exacerbation
of MetS(McEvoy et al, 2005). Finally genetic predisposition has also been proposed as a factor
hypothesising a link between the effects of stress on the hypothalamic–pituitary–adrenal axis and
the development of abnormal glucose metabolism and visceral obesity (Thakore, 2004).
The importance and consequence for mental health services is that rates of MetS in populations
with SMI surpass general population rates. An Irish study by O‟Brien et al (2007) found that
40.7% of people with SMI fulfilled criteria for MetS in comparison to 20.7% of the general
population while internationally Hausswolff-Juhlin et al, (2009) found rates of 27% in the
general population rising to approximately 40–60% in an overall SMI population. These high
rates of MetS have led to the development of specific screening methods.
1.2.2 Screening Methods
Tirupati and Chua (2007) in an Australian quantitative study proposed BMI as a simple
screening measure for MetS. This study applied IDF criteria for MetS with a convenience sample
of 202 people with schizophrenia with results indicating a high prevalence of MetS at 69.3%.
Similarly Straker et al, (2005) aimed to identify cost effective screening for MetS. A sample of
89 patients in an acute unit was assessed using a National Cholesterol Education Program
(NCEP) (2001) definition of MetS with rates of 29.2% identified. On examination of the five

10
NCEP defining criteria these authors identified elevated fasting glucose (EFG) as having the
greatest specificity. This is the ability of a screening tool to correctly recognise non cases(Polit
and Beck, 2008) of which in this study 60 of 63 non cases were correctly identified. They further
identified abdominal obesity as having the highest sensitivity correctly identifying 23 of 26 cases
of MetS. The authors conclude that combining EFG and abdominal obesity provides the highest
positive predictive value in detecting MetS.
Compared to the Tirupati and Chua(2007) study the Straker et al,(2005) study is limited in its
small sample size however employed equal gender distribution and used a multiracial sample
thus increasing its external validity. Conversely Tirupati and Chua selected a convenience
sample of primarily Caucasian males from a single rehabilitative centre. The Receiver Operating
Characteristic analysis utilised by Tirupati and Chua is described as an appropriate and valid test
instrument to develop and refine a screening instrument(Polit and Beck, 2008) thereby increasing
the strength of this study. Conversely the Straker study incorporated treatment and demographic
variables in their analyses however inclusion of these potentially confounding variables was not
apparent in the study by Tirupati and Chua. This perhaps challenges the weight these authors
place on BMI as a comprehensive screening tool.
A more systematic screening approach is proposed by Brunero and Lamont(2009) who devised a
Metabolic Syndrome Screening tool (MSST) incorporating IDF (2005) criteria for MetS. This
tool assessed the prevalence of MetS in a convenience sample of 73 people attending an
outpatient clozapine clinic and identified 61.6% as meeting criteria for MetS. The authors used
data from this study and controlled with results of an audit of screening for MetS in what they
term an opportunistic sample of 72 patients drawn from five clinical regions. The results of the
clinical audit revealed no records of waist circumference or BMI and no records of MetS
diagnosis under any defining criteria. The authors conclude that the use of the MSST is a
systematic and effective means of detecting MetS in consumers with SMI.
There is little evidence that the aforementioned MSST was tested for validity or reliability while
its time or cost effectiveness is also not apparent whereby Polit and Beck (2008) state this is a
critical constituent in the design of evaluative research. While the authors aim was to generalise
their findings to consumers with SMI not all people with SMI are prescribed clozapine therefore
findings solely from a clozapine clinic cannot be entirely representative of broad SMI
populations. Furthermore the MSST was not controlled against alternative screening methods but
11
simply to existing practices which as the next theme illustrates is virtually non-existent thereby
of little comparative value.
1.2.3 Current screening practice
Despite influential recommendations for screening the reality in practice is that screening rates
are suboptimal(Barnes et al, 2007). An audit standard based on a review of seven leading
consensus statements on MetS was developed by Barnes et al, (2007). A self selected sample of
1966 participants within 48 multidisciplinary assertive outreach teams (AOT) was studied. This
large sample strengthens the representativeness of this study however Parahoo (1997) states the
self selected strategy is a weak form of sampling. Data was collected from case notes and
revealed recorded measurements of Obesity in 17%, BP in 26% of people, plasma lipids in 22%
and FPG in 28%. Case notes indicated a diagnosis of hypertension in 6%, diabetes in 6 %, and
also dyslipidemia in 6% of cases. The authors then compared results of these case note findings
against specific studies into these conditions in similar populations. Results indicated that for
every case of diabetes recorded, another went undiagnosed, for every case of hypertension, four
went undiagnosed and for each case of dyslipidemia seven may not have been detected.
In conjunction with the aforementioned audit Barnes et al, (2007) used a questionnaire to
ascertain the views of each AOT regarding obstacles to screening and one factor that emerged
was of conflicting responsibility between primary and secondary care. Cahill and Jackson (2008)
state the primary responsibility for monitoring the physical health of people with SMI lies with
primary care however as Phelan et al,(2001) state GP practice is often reactive and incongruent
with people who are reluctant or unable to seek help.
A study by Roberts et al, (2007) examined the prevalence of routine health checks in primary
care of people with schizophrenia in comparison to a control group of asthma patients. Method
was by case matched case notes review. Results indicated that people with a diagnosis of
schizophrenia were less likely to have blood pressure checks, 55.9% compared to Asthma 71%,
weight recorded, 39.5% compared to Asthma 46.4%, and cholesterol, 12.3% compared to
Asthma 21.8%. People with schizophrenia were also less likely to have these standard health
checks in comparison to the general population albeit to a lesser extent. The study was limited as
only 17% of targeted practices responded which the authors state may be indicative of potentially
12
poorer practices among the non responding General Practitioners. These results increase the
hypothesis that people with SMI have less routine health checks than control groups and the
general population
1.2.4 MHN‟s knowledge and practices of MetS.
A lack of confidence in assessing physical health needs was highlighted in a training needs
analysis (TNA) of 168 Community Mental Health nurses by Nash (2005). This study found that
despite 71% of this sample stating they were currently providing physical health care over 96%
expressed a need for training in physical health care skills. In a further TNA this time of 138 in-
patient and CommunityMHN‟s diabetes care skills 86% reported a need for further training in
Diabetes care (Nash, 2009). Interestingly when asked if this care should be given by General
Nurses in mental health settings 71% indicated they did not wish to abdicate this responsibility
outside of their discipline but instead would prefer to receive further training to provide this care
themselves. As physical assessment skills are essential in order to screen for MetS this study has
highlighted an important area of training for MHN‟s in order to detect MetS.
This area of training need is again highlighted by a lack of knowledge of MetS shown in a study
by Ludwick and Oosthuizen (2009) in which only 18% of healthcare workers were aware that
clients with SMI were at increased risk of metabolic illness and only 9% knew that the same
population group had increased risk for CVD. Surprisingly76% of healthcare workers believed
that patients with SMI were monitored for metabolic disorders as often as the rest of the
population. The aforementioned survey of healthcare workers can be viewed tentatively as it was
a small sample (n=22) size with a vague description of the type of healthcare worker identified.
The sample was drawn from a single clinic with practices and services potentially very different
in other settings. These limitations diminish the generalisability of these findings to other
settings. Furthermore the survey of healthcare workers knowledge was embedded in a larger
study of prevalence of monitoring for MetS and as such was not the primary focus of the study.
Closer to home, in a small qualitative Irish study, McDonald(2008) explored the views and
practices of Community Mental Health Nurses(CMHNs) in relation to metabolic syndrome.
Three themes emerged from the data which were „concerns‟, „CMHN practices‟ and „barriers
13
to care‟. Although concerned about the physical health of service users the participants stated
they were unable to expand their practice due to large caseloads and lack of resources.
Regarding current practices of screening the results indicated that screening was haphazard
and inconsistent as McDonald(2008:48) reported screening is not performed routinely, nil
protocols are in place and as one respondent states “is a hit and miss effort”. Barriers to
screening of MetS are described as a lack of collaboration between primary and secondary
care and the possibility that service users needs are falling between these services. This is
reinforced in the literature by Cohn & Serynak 2006 who suggests there is a debate regarding
responsibility for the detection, prevention and management of Metabolic Syndrome.
This study indicated that participants were aware of the various components of MetS however
were not familiar with the actual term itself. The author states that the CMHN‟s had a broad
understanding of the syndrome however the participants actual responses „physical condition as a
result of treatments used ( P3)‟ and „a certain correlation between medication and increased
weight and diabetes (P7)‟ indicates a more one dimensional view of MetS as entirely
iatrogenically linked.
This study of 7 CMHN‟s was conducted by a novice researcher with self reported inexperience
with the process and the interviews therefore the findings should be examined with caution. It
was published as a Masters dissertation as such is grey literature and was not subject to peer
review
1.2.5 Conclusion
This literature review has revealed that high rates of MetS in people with SMI have been
attributed predominantly to unhealthy lifestyles; iatrogenic effects of medication and genetic
predisposition. International consensus groups have called for screening of these population
groups based on several prominent definitions. Current practice does not reflect these
recommendations however specific screening tools have ranged from simple cost effective
analysis of BMI (Tirupati and Chua, 2007) to more systematic tools such as the MSST developed
by Brunero and Lamont, (2009). The final theme addressing Nurses knowledge and practices
revealed a lack of knowledge and confidence in the assessment and interpretation of MetS
parameters and also a desire for further training in this area.
14
As stated the literature is predominantly quantitative in nature and a distinct gap is a qualitative
exploration of MHN‟s knowledge and experiences of screening for MetS in order to ascertain
nurse‟s current role in this emerging pathological threat. This can in turn inform the depth and
breadth of training that may be required in order to help nurses play a pivotal role in the
detection and prevention of MetS. Therefore this author proposes to explore and in consequence
describe Irish MHN‟s knowledge and experiences of screening for metabolic syndrome among
people with SMI.
1.3 Research Question:
What are the experiences of Mental Health Nurses working in an acute unit in the screening for
metabolic syndrome among people with SMI?
1.4 Aim:
The exploration of the knowledge and experiences of Mental Health Nurses working in an acute
unit in the screening for metabolic syndrome among people with SMI.
1.5 Objectives:
To explore and describe Mental Health nurses knowledge of Metabolic Syndrome as a cluster of
risk factors in the physical health of people with SMI.
To explore and describe mental health nurses experiences of screening for Metabolic Syndrome
among people with SMI.
15
CHAPTER TWO
2.1 Design/proposed methodology:
In order to meet the aims and objectives of the proposed study this researchers primary task is to
decide on an appropriate research design/ methodology. The chosen design will direct the selection of
a population, procedures for sampling, methods of measurement and plans for data collection and
analysis(Burns and Grove 2007). Within nursing research there are two broad paradigms namely
qualitative and quantitative, which although distinctive in philosophical characteristics can also
compliment each other as they generate different types of knowledge to inform evidence based
nursing practice.
Quantitative research stems from the logical positivist philosophy and is an objective, rigorous and
systematic process for generating information with the emphasis on collecting measurable data and
statistics (Vivar et al, 2007). Although often afforded considerable stature as a method of inquiry Polit
and Beck (2008) state that many of the intriguing, moral and ethical issues linked to healthcare cannot
be examined entirely through scientific examination.
Qualitative research has been described as evolving in response to the inadequacy of purely
quantitative enquiry (Bogdan and Biklen, 1982). It is rooted in the naturalistic interpretive philosophy
and aims to elicit meaning, discovery and understanding of human experience. Naturalistic
researchers emphasise the complexity of humans, their ability to shape their own existence and the
idea that truth is a composite of realities (Polit and Beck 2008).
According to Houser (2008) the demands of the research question should dictate the design
employed. This study proposes to explore MHN‟s knowledge and experiences of screening
for MetS among people with SMI. Qualitative research as a subjective, interactive approach
can help to describe and promote our understanding of human experiences (Burns and Grove,
2009). Therefore this study will be framed by this qualitative design as it aims to explore and
describe the knowledge and lived experiences of MHN‟s in the screening of MetS among
people with SMI.
Three prominent approaches exist within qualitative research which are phenomenology,
grounded theory and ethnography each of which carries their own distinct methodological
framework. Initially an ethnographic approach was considered as the researcher regarded
16
MHN‟s experiences of screening for MetS to be strongly influenced by their primary focus
on mental health, the culture of the in-patient unit; and their role and autonomous decision
making ability within the wider MDT. However novice researchers may only have a naive
understanding of specific philosophical approaches and often do not have the skill or
competence to conduct this research with misunderstood findings resulting in „sloppy
science‟ (Streubert-Speziale and Carpenter 2007; Houser,2008).
Remaining cognisant of this researcher‟s limitations an exploratory qualitative descriptive
design is proposed. Sandelowski (2000) states that qualitative descriptive is the method of
choice when straight description of phenomena is desired and an independently valuable
methodological approach. She further states that tones and textures of the aforementioned
specific approaches may resonate within a straight descriptive study. This approach affords
the novice researcher the freedom to explore and describe phenomena without being
constrained by a specific qualitative methods niche. Furthermore the exploratory nature of
this study aims to develop the body of knowledge of this particular phenomenon of interest
thus broadening the evidence base to support practice.
2.2 Population/Sample
A sample is a subset of a population from which data can potentially be collected
(Parahoo,2006) of which there are two main types; Probability and Non Probability sampling.
Probability sampling often known as random sampling is primarily used in quantitative
research and refers to the fact that every element (member) of the population has an equal
chance of being selected for a study (Burns and Grove, 2009).
Within Non-Probability sampling there are three primary sampling methods employed in
qualitative research which are, Purposive, Snowball, and Convenience sampling (Polit and
Beck, 2008). The goal of the sampling strategy in qualitative research is credibility where the
researcher must utilise judgement in purposively selecting participants who can best inform
the study (Houser, 2008). In addition (Holloway and Wheeler 2002) also identify
homogenous sampling as selection of a particular group of people who share similar
characteristics or circumstances such as occupation. Therefore the researcher proposes to use
purposive sampling of a homogenous group which will allow the researcher to select
17
participants that are most likely to yield a thick and exhaustive description of the
phenomenon of interest whom in this case will be: MHN‟s working in an acute Mental
Health in-patient unit.
2.2.1Sampling Criteria
Because of the in depth nature of the data uncovered and the detailed analysis required
qualitative research usually employs small sample sizes (Cormack, 2000). Qualitative
research designs must satisfy the sampling principle of adequacy or saturation which is
achieved when the researcher “concludes that the responses are repetitive and no new
information is being generated” (Houser, 2008:225). For practical planning purposes however
the researcher proposes to select 10 participants who meet the inclusion criteria (Appendix 3).
2.2.2 Access to research site and participant recruitment
The researcher proposes to recruit participants from an acute in-patient mental health service
in Dublin. The researcher will write a letter (Appendix 4) to the Director of Nursing seeking
permission to gain access to the mental health service in question. If permission is granted the
researcher will then write a further letter (Appendix 5) to the Clinical Nurse manager III
(CNM III) whom has been identified as the gatekeeper seeking permission to gain access to
staff and distribute information. Gatekeepers co-ordinate admission to a site and influence
those who work in that setting therefore negotiation is an integral part of the research process
(Roach (2009). The researcher will remain cognisant of this in the compilation of the
aforementioned letters and employ professionalism and sensitivity in communicating with the
CNM III. A participant information leaflet (Appendix 6) and letter of invitation (Appendix 7)
will be enclosed for distribution to potential participants. The researcher will seek ethical
approval from the Faculty of Health Sciences Research Ethics Committee in Trinity College
Dublin(Appendix 8) and a further correspondence will be made to the relevant health services
research ethics committee(Appendix 9).
Once permission has been granted from all relevant parties the CNM III will be asked to
distribute the participant information to staff who meet the inclusion criteria. The information
leaflet will explain the purpose of the study and briefly, the proposed requirements of
18
participants. Contact details for the researcher will be supplied and interested staff will be
encouraged to make contact directly. The researcher will arrange a brief one to one meeting
with interested staff where a detailed description of the interview format and process will be
given. Potential participants will then be given one week to consider the information before
making an informed decision at which stage the researcher will invite them to sign a consent
form (Appendix 10).
2.3 Data Collection
Burns and Grove (2007) state that the interview is most often the data collection method of
choice in a qualitative inquiry. These can range from totally unstructured interviews whereby
content is controlled by the participant to a structured format in which the researcher guides
the interview with the aid of an interview protocol and schedule of questions. Despite this
structure the interview will be more than a mechanistic formal exercise but a dynamic
interaction with the aim of elucidating the importance of a persons experience and the
subjective data thereby generated (Houser, 2008).
2.3.1 Semi-structured interviews.
In order to elicit the knowledge and experience of MHN‟s in the screening practices for MetS
the researcher proposes to use a semi-structured interview. The structure in question will be
in the shape of an interview guide comprising of broad open ended statements and questions
(Appendix 11). Within these broad questions the researcher will also have prompts that can
aid with refocusing the interview in the event of what Field and Morse (1985) termed „Dross‟
or issues arising that are unrelated to the topic in hand.
2.3.2 The Interview
The interview location will be in a place free of distractions such as noise, visual stimuli and
interruptions and allow interviewees to comprehend the question Cormac (2000). This
location should be convenient for the participants and if acceptable the researcher proposes to
use a small room (to enhance the acoustics) in the hospital environment yet away from the
potential distractions of the unit. The interview strategy will be to phrase the questions
carefully using open ended words such as „how‟ „what‟ or „why‟. These questions will be

19
without double meaning and clear and logical. Questions will be posed sequentially allowing
the participant to feel at ease and introducing more depth of questioning as the interview
progresses (Polit and Beck, 2008).
It is envisaged the interview will last between 45 and 90 minutes and this will become more
apparent following the pilot study. The researcher proposes to audiotape recordings using a
digital voice recorder placed unobtrusively but within sufficient proximity to clearly record
the participant‟s responses. The recorder will be a Panasonic RR-QR230 which can record up
to 45 hours of data and is password protected for additional security. This allows interviewers
to turn transient data into permanent data which can be analysed in more detail over a longer
period of time (Cormack, 2000). Spare batteries, note pads and pens and refreshments will
also be available.
At the end of the interview any clarification sought will be given and the participant will also
be asked if they need an explanation of anything that arose during the interview. This can
ensure a „positive closure‟ to the process (Polit and Beck, 2008). Observations will be written
in field notes immediately following the interview so as not to disturb the actual interview
process and also to ensure the integrity of the data. A reflective journal will be maintained to
record this researcher‟s insights and personal reflections on the interviews.
This researcher recognises personal limitations in interviewing techniques and will attend a
two day workshop on qualitative interviewing in order to better develop these skills. Despite
this inexperience the researcher will utilise good interpersonal skills such as active listening,
maintaining appropriate eye contact and remaining open to all responses. This will help to
build trust and develop rapport with the participants and also serve to put them at ease during
the process.
2.4 Rigor and Trustworthiness
Methodological rigor can be assured by having a transparent audit trail of raw data collection
and analysis; consistent evidence of reflexivity; demonstrating saturation; and using vivid,
thick descriptions of the phenomenon. (Barreca Wilkins, 2008). Lincoln and Guba (1985)
identified four measures of rigour to assess trustworthiness in qualitative studies which are;
Credibility, dependability, confirmability, and transferability.
20
2.4.1 Credibility
Credibility refers to authenticity and how true the data reflects the participant‟s experiences
of the phenomenon under study (Vivar et al, 2007). Strategies identified to achieve credibility
include prolonged engagement with the participants, peer debriefing, and member checking.
Within this study „member checking‟ will be the primary means of achieving credibility. This
researcher specifically chose Collaizzi‟s (1978) framework to enhance credibility. Within this
framework verbatim transcripts will be provided to the participants throughout the process for
validation and an exhaustive description will be given at the end for further validation as to
the accuracy of the information recorded.
2.4.2 Dependability
This criterion is met once researchers have demonstrated credibility of a study and refers to
the stability of the data and whether the findings were likely to be replicated in the same
context with the same participants over time (Polit and Beck, 2008). The researcher proposes
to initiate an inquiry audit whereby an external auditor will examine the data collection
process and all decisions made in the transformation of data into concise schema (Burns and
Grove, 2008).
2.4.3 Confirmability
Confirmability is related to the aforementioned inquiry audit and is achieved through
reflexive and objective reporting of the participant‟s responses. This researcher will leave an
audit trail which is a seamless recording of all decisions made that can illustrate the evidence
and thought processes that led to the conclusions (Streubert-Speziale and Carpenter, 2007).
This audit trail can then be examined to assess whether the information gathered is
representative of the conclusions reached.
2.4.4 Transferability
21
This relates to the extent that the findings of the study can be transferred to other settings or
groups (Polit and Hungler, 1999). The judgement as to the transferability however rests with
the potential users of the findings and not the researcher. The responsibility of the researcher
is to give a clear and distinct description of the research context, culture, and process
(Graneheim and Lundman, 2004). This researcher proposes to achieve this by providing a
rich and thick description of participants responses interspersed with relevant quotations that
accurately reflect the experiences of MHN‟s.
2.5 Data Analysis
Qualitative data analysis occurs in three stages: description, analysis and
interpretation.(Burns and Grove, 2008).With qualitative research traditions however analysis
often occurs simultaneously with data collection and is referred to as constant comparison
(Houser, 2008). Challenges associated with Qualitative data analysis are; a lack of cogent
rules and procedures for analysis, sheer volume of data to be organised and interpreted, and
the reduction of this data for reporting purposes whilst maintaining the richness and value of
the data (Polit and Beck, 2008).
This researcher will follow Colaizzi‟s (1978) 7 step framework for data analysis (Appendix
12). Within these framework participants descriptions of their knowledge and experiences
will be collected. Following a return to the original transcripts significant statements will be
extracted. The meanings of these statements will be interpreted and information will be
organised into themes. An exhaustive description of these experiences will then be compiled.
Finally the researcher will feedback this description to participants to ensure they validly
reflect the totality of MHN‟s experiences (Polit and Beck, 2008).
Streubert-Speziale and Carpenter(2007) states that qualitative data analysis requires
considerable levels of reading, intuiting, analysing, and reporting of discoveries. To assist in
this process the researcher proposes to use computer assisted qualitative data analysis
software (CAQDAS). The program in question is Nvivo8 which can help researchers find
patterns in the data and can also assist in classifying, sorting and arranging thousands of
pieces of information(Polit and Beck,2008; QSR International.com, 2010). This software also
enables data to be imported directly from the digital audio recorder for immediate analysis.
22
2.6 Pilot study
A pilot study is a smaller version of the proposed study with the aim of refining the research
methodology (Burns and Grove, 2008). This pilot can test the feasibility of the study design,
the data collection techniques, logistical issues and can also provide an opportunity to analyse
the data (Cormack, 2000; Burns and Grove, 2008). Furthermore the pilot study can serve to
give the novice researcher experience with the data collection instruments and also valuable
interviewing experience. Repetitive or unclear questions can be identified and an assessment
of the potential duration of the interview can also be ascertained. The researcher proposes to
use two colleagues who meet the inclusion criteria to provide feedback on the
appropriateness of the interview guide. All responses will be recorded, analysed and returned
for validation as planned for the main study. This interview will take place in a room
available from 2 to 4 pm adjacent to these colleagues unit following a short 5 hour shift. The
data obtained in the pilot will not be used in the main study due to the potential for what
Teijlingen and Hundley (2001) call „contamination‟ in which methodological flaws evident in
the pilot may pollute the main study.
2.7 Ethical considerations
Failure to identify and address ethical issues can place the conduct and the findings of a study
in jeopardy (Oberle and Allen, 2006). This researcher will be guided by the basic ethical
principles set out in the Belmont report (1979) which are: Respect for persons; Beneficence;
and Justice. Furthermore the personal nature of qualitative inquiry requires the researcher to
pay close scrutiny to several considerations such as informed consent, protection of
participants, confidentiality, and anonymity (Vivar et al, 2007).
2.7.1 Informed consent
Informed consent is defined as “a process of information exchange in which participants are
provided understandable information needed to make a participation decision” (Houser,
2008). However Allbutt and Masters (2009) argue that in qualitative research, the term
„informed consent‟ is something of a misnomer as participants are unable to predict with
certainty what they will be asked at the interview or what information will be divulged.
23
Therefore this researcher proposes to use process consent whereby consent is obtained at the
beginning of the process but also informally at further critical points of data collection
leading to dissemination of results (Keogh and Doyle, 2009).
The 4 elements necessary for informed consent are: disclosure of essential information to the
participant; participants understanding of this information; capacity to give consent; and
voluntarily providing consent to participate (Burns and Grove, 2007). With these four
elements in place this researcher will ask the participant to read and sign a consent form at
the beginning of the process. Participants will furthermore be reminded of their right to
withdraw at any stage without prejudice.
2.7.2 Protection of participants
The researcher has a responsibility to ensure that participants in this study are free from harm
at all stages of the process. Although MHN‟S are not a vulnerable group as such and the topic
does not strike obvious emotional chords this is a presumption and the researcher will
endeavour to protect participants from any financial, physical, emotional, or social stress.
2.7.3 Confidentiality and Anonymity
Confidentiality relates to the researchers management of personal information shared by the
participants while anonymity exists when the participant cannot be linked with their
individual responses (Burns and Grove, 2007). Participants names will be replaced by code
numbers which will be used throughout the study and all other personal details will not be
disclosed to third parties. Within qualitative reports individuals may inadvertently be
identified through the use of long quotations. In order to prevent this, the researcher will
remove any of these identifying quotations and will also ask the participant at the stage of
member checking to further identify any information that may disclose their involvement in
the study.
All data, notes, and sundry information obtained in the study whether written or digital will
be encrypted, password protected and stored securely in a locked premises controlled solely
by the researcher. This data will be stored for 5 years post study completion as recommended
by Trinity College Faculty of health sciences research ethics committee (2009). However this

24
data must be fully anonymised and any information that can identify specific participants will
be retained only for the duration of the study and then immediately shredded or deleted.
Chapter 3
3.1 Proposed Outcomes of Study.
This study proposes to explore the knowledge and experiences of Mental Health Nurses
working in an acute unit in the screening for metabolic syndrome among people with SMI.
The researcher proposes to meet with the aims and objectives of the study. All steps in this
research process will be documented from the initial design to dissemination of results. The
collected data will be analysed and summarised succinctly. The final report will provide a
vivid and thick description of MHN‟s knowledge and experiences of screening for MetS
among people with SMI. Implications for nursing practice will be discussed and included in
the final report. It is envisaged that the findings of this study will indirectly increase
awareness of MetS among MHN‟s and allow them to reflect on their physical health care
practices among people with SMI. More directly it is anticipated that findings of this study
can lead to recommendations for:
1. Clearly identified further training for MHN‟s in this area.
2. The development of local policies and protocols for screening of MetS.
3. The development of specific screening methods at local level.
4. Rigorous further research in this area possibly examining variables that influence the
screening for MetS among people with SMI.
3.1.2 Limitations
The primary limitation of this study is the researcher‟s inexperience with the process.
However potential methodological errors will be lessened by training in qualitative research
methods prior to the study and adherence to the qualitative descriptive method. The single
site nature of this study and the small sample size will mean that findings cannot be directly
generalisable however the rich and thick description of findings will allow readers to draw
their own inferences from the study.
25
3.1.3Research Dissemination
The design and findings of this study will be presented in textual format and submitted for
publication in national and international nursing journals. The researcher will also aim to
make a presentation of the findings to colleagues at in-service training seminars. Furthermore
the researcher will aim to present a brief summary of findings to the local multidisciplinary
team with invitations extended to linked primary care and service user representatives.
Finally the researcher will aim to make presentations of the study at national nursing
conferences.
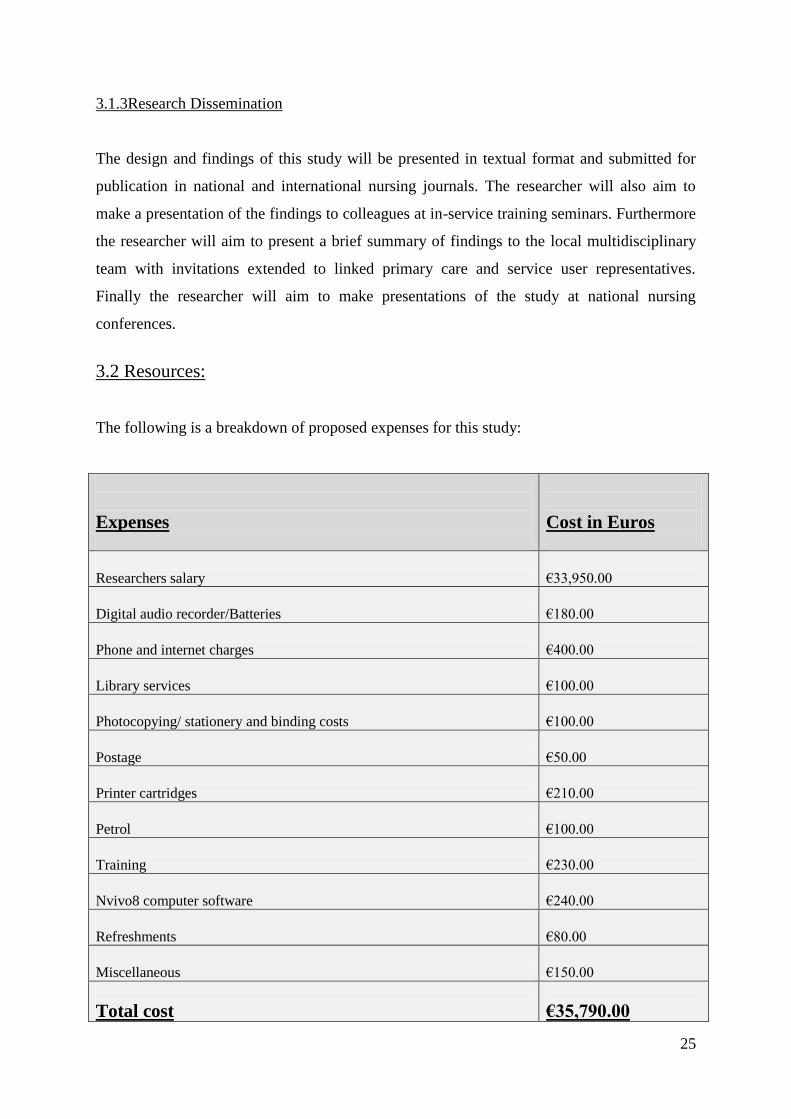
3.2 Resources:
The following is a breakdown of proposed expenses for this study:
Expenses
Cost in Euros
Researchers salary
€33,950.00
Digital audio recorder/Batteries
€180.00
Phone and internet charges
€400.00
Library services
€100.00
Photocopying/ stationery and binding costs
€100.00
Postage
€50.00
Printer cartridges
€210.00
Petrol
€100.00
Training
€230.00
Nvivo8 computer software
€240.00
Refreshments
€80.00
Miscellaneous
€150.00
Total cost
€35,790.00
26
References
Keogh B. & Doyle L. (2009) The Ethics of Conducting Research with Mental Health
Service Users British Journal of Nursing 18 (5) 277-281.
Allbutt H. & Masters H.(2009) Ethnography and the ethics of undertaking research in different
mental healthcare settings. Journal of Psychiatric and Mental Health Nursing. Retrieved from
www.interscience.wiley.com10.1111/j.1365-2850.2009.01493 on 9th February 2010.
Alberti G.M., Zimmet P. & Shaw J. (2005) IDF Epidemiology Task Force Consensus
Group. The metabolic syndrome--a new worldwide definition. Lancet 366 (9491) 1059-62.
Allison D.B. Mentore J.L. Heo M. Chandler L.P. Cappelleri J.C. Infante M.C. & Weiden P.J.
(1999) Antipsychotic-induced weight gain: a comprehensive research synthesis. American
Journal of Psychiatry 156, 1686–1696.
BarnesT.R., Paton C., Cavanagh M.R., Hancock E. & Taylor, D. (2007) UK audit of screening
for the metabolic side effects of antipsychotics in community patients. Schizophrenia Bulletin
33, 1397–1403.
Barnett A.H., Mackin P., Chaudhry I., Farooqi A., Gadsby R., Heald A., Hill J., Millar H.,
Peveler R., Rees A., Singh V., Taylor D., Vora J. & Jones P.B. ( 2007) Minimising metabolic
and cardiovascular risk in schizophrenia: diabetes, obesity and dyslipidaemia. Journal of
Psychopharmacology 21, 357.
Barreca M. & Wilkins S. (2008) Experiences of nurses working in a stroke rehabilitation
unit. Journal of Advanced Nursing 63 (1) 36-44.
Bogdan R. & Biklen S. K. (1982). Qualitative Research for Education: An introduction
to theory and methods. Allyn & Bacon: Boston.
Brown S. (1997) Excess mortality of schizophrenia - a Meta analysis. British Journal of
Psychiatry 171, 502–508.
Brown S., Birtwistle J., Roe, L., & Thompson, C. (1999). The unhealthy lifestyle of people
with schizophrenia Psychological Medicine, 29, 697 – 701.
BruneroS. & Lamont S.(2009) Systematic screening for metabolic syndrome in consumers
with severe mental illness. International Journal of Mental Health Nursing 18, 144–150.
Burns N. & Grove S.K. (eds) (2007) Understanding Nursing Research, 4th
edn. Saunders
Elsevier: MA
Cahill M. & Jackson A. (2008) Monitoring the physical health of individuals with serious
mental illness. Irish Journal of Psychological Medicine 25 (3) 108-115.
Clark N.G. (2004). Consensus Development Conference on Antipsychotic Drugs and Obesity
and Diabetes. Diabetes Care 27 (2) 596-601.
27
Cohn T.A. and Sernyak M.J. (2006) Medication monitoring for patients treated with
antipsychotic medications. Canadian Journal of Psychiatry 51, 492–501.
Collaizzi P. (1978) Psychological research as the phenomenologist views it. In Existential
phenomenology: Alternatives for psychology (Valle R.S. & King M., eds), Oxford
University Press, New York.
Cormack D. (eds) (2000) The Research Process in Nursing 4th
edn, Blackwell Science,
Oxford.
De Nayer A., De Hert M., Scheen A., Van Gaal L. & Peuskens J. (2005) Belgian consensus on
metabolic problems associated with second-generation antipsychotics. International Journal of
Psychiatry in Clinical Practice 9,130–137.
Department of Health, (2006) A Vision for Change: Report of the Expert Group on Mental
Health Policy. Dublin: Stationary Office.
Field P. & Morse, J. (1985) Nursing Research- The application of qualitative approaches.
Chapman and Hall, London.
Graneheim U. H. & Lundman B. (2004) Qualitative content analysis in nursing research:
concepts, procedures and measures to achieve trustworthiness. Nurse Education Today
24, 105-112.
Harris E.C. & Barraclough B. (1998). Excess mortality of mental disorders. British Journal of
Psychiatry 173, 11 – 53.
Hasnain M.W., Vieweg V.R., Fredrikson S.K., Beatty-Brooks M., Fernandez A. &
Pandurangie A.K. (2008) Clinical monitoring and management of the metabolic syndrome in
patients receiving atypical antipsychotic medications. Primary Care Diabetes 3(1) 5-15.
Holloway I. & Wheeler S. (2002) Qualitative Research in Nursing 2nd
edn. Blackwell
Science, Oxford:
Houser J. (ed). (2008) Nursing Research. Jones and Bartlett Publishers Inc, Toronto
International Diabetes Federation (IDF) (2005) The IDF consensus worldwide definition of the
metabolic syndrome, Brussels. Retrieved from http://www.idf.org/webdata/docs/IDF on 5th
April 2009.
Jarboe K.S. (2007) Considering the impact on overall patient health when choosing
antipsychotic therapy. Journal of the American Psychiatric Nurses Association 13, S23-S28.
Jones M. and Jones A (2008) The effect of antipsychotic medication on metabolic syndrome.
Nursing Standard 22 (48) 43-48.
Keogh B. & Doyle L. (2009) The Ethics of Conducting Research with Mental Health
Service Users British Journal of Nursing 18 (5) 277-281
28
Lambert T. & Chapman L. (2004). Diabetes, Psychotic Disorders and Antipsychotic Therapy, a
Consensus Statement. Members for the Australian Consensus Panel for Diabetes. Psychotic
Disorders and Antipsychotic Therapy. Sydney.
Lincoln T. & Guba E. (eds) (1985) Naturalistic inquiry, Sage Publications, CA.
Ludwick J.J & Oosthuizen P.P. (2009) Screening for and monitoring of cardio-metabolic risk
factors in outpatients with severe mental illness in a primary care setting.
African Journal of Psychiatry 12, 4.
Marder S.R., Essock S.M., Miller A.L., Buchanan R.W. Casey D.E., Davis J.M., Kane, J.M.
Lieberman J.A., Schooler, N.R. Covell, N. Stroup, S. Weissman, E.M. Wirshing, D.A. Hall,
C.S. Pogach, L. Pi-Sunyer, X. Bigger Jr., J.T. Friedman, A. Kleinberg, D. Yevich, S.J. Davis,
B. & Shon, S. (2004) Physical health monitoring of patients with schizophrenia. American
Journal of Psychiatry 161, 1334–1349.
McCreadie R.G. (2003). Diet, smoking and cardiovascular risk in people with schizophrenia.
British Journal of Psychiatry 183, 534–539.
McDonald A. (2008) An exploration of the views and practices of Community Mental Health
Nurses in relation to metabolic syndrome. Unpublished Masters Dissertation Waterford
Institute of Technology:.
McEvoy J.P., Meyer J.M., Goff D.C., Nasrallah H.A., Davis S.M., Sullivan, L. Meltzer, H.Y.
Hsiao, J. Scott S.T. & Lieberman, J.A. (2005) Prevalence of the metabolic syndrome in
patients with schizophrenia: baseline results from the Clinical Antipsychotic Trials of
Intervention Effectiveness (CATIE) schizophrenia trial and comparison with national estimates
from NHANES III, Schizophrenia Research. 80, 19–32.
Meyer J.M. & Stahl S.M. (2009) The metabolic syndrome and schizophrenia. Acta
Psychiatrica Scandinavica 119, 4–14.
Meyer J.M., Davis V.G., Goff D.C., McEvoy J.P., Nasrallah H.A., Davis S.M., Rosenheck,
R.A. Daumit, G.L. Hsiao, J. Swartz, M.S. Stroup, T.S. & Lieberman J.A. (2008) Change in
metabolic syndrome parameters with antipsychotic treatment in the CATIE Schizophrenia
Trial: prospective data from phase 1. Schizophrenia Research 101, 273–286.
Muir-Cochrane, E. (2006) Medical co-morbidity risk factors and barriers to care for people
with schizophrenia. Journal of Psychiatric and Mental Health Nursing. 13, 447-452.
Nash M (2005) Physical care skills: a training needs analysis of inpatient and
community mental health nurses. Mental Health Practice 9, 4.
Nash M. (2009) Mental health nurses diabetes care skills - a training needs analysis. British
Journal of Nursing, 18, (10) 626 – 630.
National Cholesterol Education Program (2001) Executive summary of the third report of the
(NCEP) expert panel on detection, evaluation and treatment of high blood cholesterol in adults
(Adult Treatment Panel III). Journal of the American Medical Association 285, 2486–2497.
29
Oberle k. & Allen M. Ethical Considerations for Nurses in Clinical Trials. Nursing Ethics
13, (2) 180-186.
O‟Brien,S. Devitt, E. Ahmed, M. McDonald, C. (2007) High prevalence of risk factors for
physical illness in a long-stay psychiatric unit. Irish Journal of Psychological Medicine.
24(2) 55-58.
Ohlsen R.I., Peacock G. & SMITH S. (2005) Developing a service to monitor and improve
physical health in people with serious mental illness Journal of Psychiatric and Mental
Health Nursing 12, 614–619.
Parahoo K. (ed) (2006) Nursing Research: Principles, Process and Issues. 2nd
edn
Macmillan, London.
Phelan M., Stradins L. & Morrison S. (2001) Physical health of people with severe mental
illness. British Medical Journal. 322, (7284) 443-4.
Polit D.F. & Beck C.T, (eds) (2008) Nursing Research-Generating and Assessing Evidence
for Nursing Practice, 8th
edn. Lippincott Williams& Wilkins: Philadelphia
Polit, D.F., & Hungler B.P.(eds) (1999) Nursing Research: Principles and Methods. 6th
edn, Lippincott, Pennsylvania.
Ereaut G. (2010) What is qualitative research. Retrieved from
http://www.qrsinternational.com/products_nvivo.aspx on 10th February 2010.
Roach P. Duxbury JA. Wright K. Bradley D. & Harris N. (2009) Conducting research on acute
mental health admission wards Nurse Researcher. 16, 4.
Roberts L. Roalfe S. Wilson S. & Lester H. (2007) Physical health care of patients with
schizophrenia in primary care: a comparative study. Family Practice 24, 34-40.
Robson D. Gray R. (2007) Serious mental illness and physical health problems: A discussion
paper. International Journal of Nursing Studies. 44, 457-466.
The National Commission for the Protection of Human Subjects of Biomedical and Behavioral
Research. (1979) The Belmont Report Ethical Principles and Guidelines for the protection of
human subjects of research. Department of Health, Education, and Welfare. Retrieved from
http://www.hhs.gov/ohrp/humansubjects/guidance/belmont.htm. on 1st January 2010.
Saha S. Chant D. & McGrath J. (2007) A systematic review of mortality in schizophrenia. Is
the differential mortality gap worsening over time? Arch Gen Psychiatry 64, (10) 1123-1131.
Sandelowski M. (2000) Whatever Happened to Qualitative Description? Research in
Nursing & Health 23 334-340.
Straker D. Correll C. Kramer-Ginsberg E. Abdulhamid N. Koshy F. Rubens E. Saint-Vil R.
Kane J.M. & Manu P.(2005). Cost effective screening for the metabolic syndrome in patients
30
treated with second generation antipsychotic medications. American Journal of Psychiatry 162,
1217–1221.
Streubert-Speziale H.J. & Carpenter D.R., (eds) (2007) Qualitative Research in Nursing:
Advancing the Humanistic Imperative 3rd
edition, Lippincott Williams and Wilkins,
Philadelphia.
Teijlingen E.R. & Hundley V. (2001)The importance of pilot studies. Social Research update.
Retrieved from http://sru.soc.surrey.ac.uk/SRU35.pdf on 27th November 2009.
Thakore J. (2004) Metabolic Disturbance in first episode schizophrenia. British Journal of
Psychiatry 184 (S47), S76-S79.
Tirupati S. and Chua L.E. (2007) Body mass index as a screening test for metabolic syndrome
in schizophrenia and schizoaffective disorders. Australasian Psychiatry 15, (6),470-473.
Vivar C.G., McQueen A., Whyte D.A. & Armayor N.C. (2007) Getting started with
qualitative research: developing a research proposal. Nurse Researcher 14, 3.
Von Hausswolff-Juhlin Y., Bjartveit M., Lindström E. & Jones P. Schizophrenia and physical
health problems. Acta Psychiatrica Scandinavica Suppl. (438):15-21.
World Health Organization (WHO) (1999) Definition, Diagnosis and Classification of
Diabetes Mellitus and its Complications. Report of a WHO Consultation. Part 1: Diagnosis and
Classification of Diabetes Mellitus. World Health Organization, Geneva.