avoiding mandibular nerve impairment, part one · pdf fileavoiding mandibular nerve...
TRANSCRIPT

Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of
specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and
courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to
contact their state dental boards for continuing education requirements.
Continuing Education
Avoiding Mandibular NerveImpairment, Part One: Anatomical and Intraoperative
Considerations
Authored by Carl E. Misch, DDS, MDS, PhD (hc), and Randolph R. Resnik, DMD, MDS
Upon successful completion of this CE activity 3 CE credit hours will be awarded
Volume 33 No. 11 Page 96

ABOUT THE AUTHORSDr. Misch was clinical professor anddirector of oral implantology at TempleUniversity, Philadelphia. He was adjunctprofessor at the University of MichiganSchool of Dentistry in the department ofperiodontics/geriatrics and was adjunct
professor at the School of Engineering in the department ofbiomechanics at the University of Alabama at Birmingham.He has maintained a private practice restricted to implantsurgery (bone grafting and implant placement) and relatedprosthetics for more than 30 years. He is currently retiredfrom private practice in Beverly Hills, Mich. He can bereached at via e-mail at [email protected].
Disclosure: Dr. Misch reports no disclosures.
Dr. Resnik is a graduate of the Universityof Pittsburgh, with a specialty degree inprosthodontics, surgical fellowship in oralimplantology, and a master’s degree inradiology. He is a clinical professor of oralimplantology at Temple University, a staff
member at Allegheny General Hospital, and surgicaldirector of the Misch International Implant Institute. He is aleading educator, clinician, and researcher in the field ofprosthodontics and oral implantology. He maintains aprivate practice in Pittsburgh limited to oral implantology. Hecan be reached at via e-mail at [email protected].
Disclosure: Dr. Resnik reports no disclosures.
INTRODUCTIONIn implant dentistry, iatrogenic injuries to the third division ofthe trigeminal nerve are a common and complex problem.
Neuro sensory impairment in the mandibular posterior regionaffects the patient’s quality of life and potentially can lead tosignificant medico-legal implications for the clinician. Toprevent damage to this vital structure, it is imperative for theimplant dentist to have a comprehensive radiographic surveyof the region, a thorough knowledge of normal versus variantanatomy, and awareness of intraoperative surgical techniquesto minimize the possibility of nerve impairment.
In part one of this 3-part series, anatomical andintraoperative considerations will be discussed to aid theimplant dentist in avoiding neurosensory impairmentcomplications. Part 2 of this paper will discuss radiographicand surgical technique considerations for the prevention ofnerve impairments, and Part 3 will outline the evaluationand treatment protocols of nerve impairment complications.These principles and techniques have been taught to morethan 5,000 dentists at the Misch International Instituteduring the last 30 years with overwhelming success.
ANATOMICAL CONSIDERATIONSMandibular NerveThe mandibular nerve (V3) exits foramen ovale in theinfratemporal fossa and enters the mandibular foramen on themedial surface of the ascending mandibular ramus. Within themandibular canal (MC), the V3 is termed the inferior alveolarnerve as it runs obliquely and anteriorly in the ramus area andthen horizontally to the mental foramen. In approximately thefirst molar region, the inferior alveolar nerve divides into 2terminal branches: the incisive and mental nerves.1 Themental nerve passes through the mental foramen with 3 nervebranches. One innervates the skin of the mental area, and theother 2 proceed to the skin of the lower lip, mucousmembranes, and the gingiva as far posteriorly as the secondpremolar. The incisive nerve branch supplies innervation tothe mandibular first premolar, canine, and incisor teeth. Theexact location of the inferior alveolar nerve within the body ofthe mandible must be accurately determined to avoidneurosensory disturbances secondary to implant placement.
Position of the Mandibular Canal VariesIn implant dentistry today, a common belief exists that thevertical position of the MC is relatively constant below theapices of the natural teeth within the mandible. How ever,studies have confirmed the inferior-superior (vertical)
Continuing Education
1
Avoiding Mandibular NerveImpairment, Part One: Anatomical and IntraoperativeConsiderationsEffective Date: 11/1/2014 Expiration Date: 11/1/2017
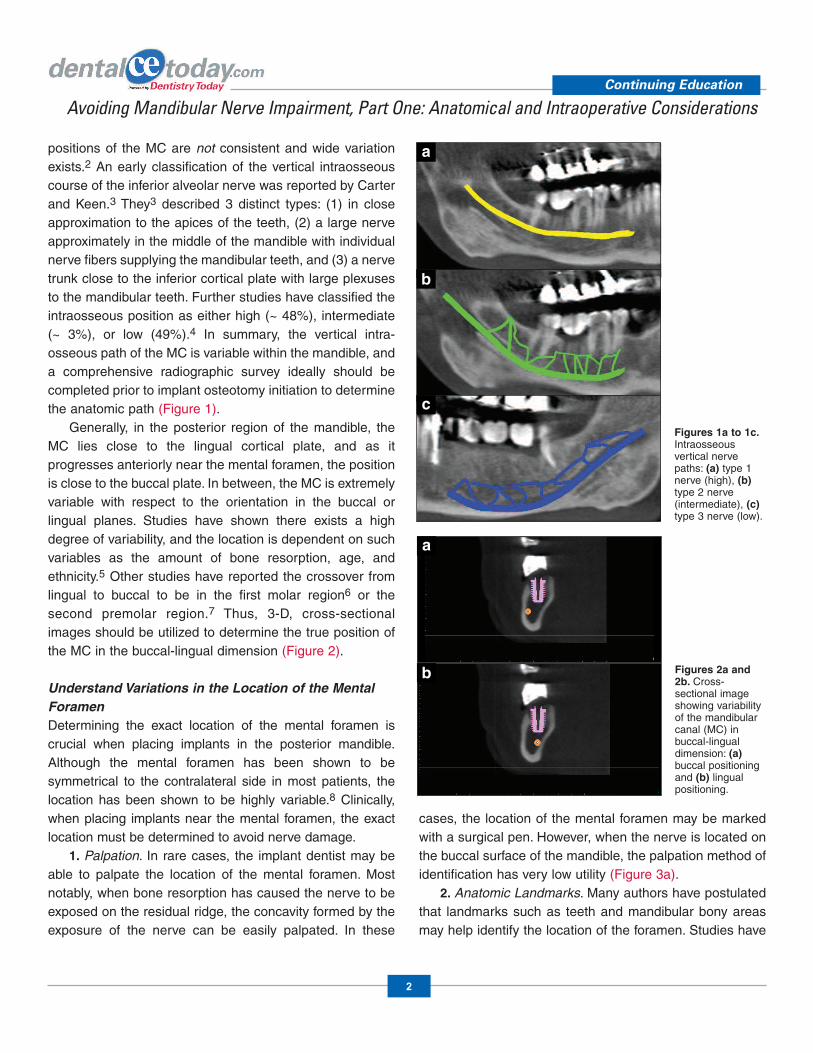
positions of the MC are not consistent and wide variationexists.2 An early classification of the vertical intra os seouscourse of the inferior alveolar nerve was reported by Carterand Keen.3 They3 described 3 distinct types: (1) in close ap proximation to the apices of the teeth, (2) a large nerveapproximately in the middle of the mandible with individualnerve fibers supplying the mandibular teeth, and (3) a nervetrunk close to the inferior cortical plate with large plexusesto the mandibular teeth. Further studies have classified theintraosseous position as either high (~ 48%), intermediate(~ 3%), or low (49%).4 In summary, the vertical intra-osseous path of the MC is variable within the mandible, anda comprehensive radiographic survey ideally should becompleted prior to implant osteotomy initiation to determinethe anatomic path (Figure 1).
Generally, in the posterior region of the mandible, theMC lies close to the lingual cortical plate, and as itprogresses anteriorly near the mental foramen, the positionis close to the buccal plate. In between, the MC is extremelyvariable with respect to the orientation in the buccal orlingual planes. Studies have shown there exists a highdegree of variability, and the location is dependent on suchvariables as the amount of bone resorption, age, andethnicity.5 Other studies have reported the crossover fromlingual to buccal to be in the first molar region6 or thesecond premolar region.7 Thus, 3-D, cross-sectionalimages should be utilized to determine the true position ofthe MC in the buccal-lingual dimension (Figure 2).
Understand Variations in the Location of the MentalForamenDetermining the exact location of the mental foramen iscrucial when placing implants in the posterior man dible.Although the mental foramen has been shown to besymmetrical to the contralateral side in most pa tients, thelocation has been shown to be highly variable.8 Clinically,when placing implants near the mental foramen, the exactlocation must be determined to avoid nerve damage.
1. Palpation. In rare cases, the implant dentist may beable to palpate the location of the mental foramen. Mostnotably, when bone resorption has caused the nerve to beexposed on the residual ridge, the concavity formed by theexposure of the nerve can be easily palpated. In these
cases, the location of the mental foramen may be markedwith a surgical pen. However, when the nerve is located onthe buccal surface of the mandible, the palpation method ofidentification has very low utility (Figure 3a).
2. Anatomic Landmarks. Many authors have postulatedthat landmarks such as teeth and mandibular bony areasmay help identify the location of the foramen. Studies have
Continuing Education
2
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
Figures 1a to 1c.Intraosseousvertical nervepaths: (a) type 1nerve (high), (b)type 2 nerve(intermediate), (c)type 3 nerve (low).
a
b
c
Figures 2a and2b. Cross-sectional imageshowing variabilityof the mandibularcanal (MC) in buc cal-lingualdimension: (a)buccal positioningand (b) lingualpositioning.
a
b

shown no correlation with the location of the mentalforamen and a particular tooth (ie, first premolar, secondpremolar, between apices of the premolars) or anatomicstructure. The location has been shown to be variableanywhere between the canine and as far posterior as thefirst molar with a significant dependence on gender, age,and race.9 The use of certain bony landmarks (ie, alveolarridge, mandibular symphysis, and infraorbital foramen)have been associated with a general location of theforamen, although these measurements are extremelyvariable and dependent on the extent of bone resorption,skeletal relationships, and anatomic variants (Figure 3b).
3. Two-Dimensional Radio graphs. Studies have shownthat in more than 50% of periapical and panoramicradiographs, the mental foramen is not in the location asdepicted on the image.10 Conventional 2-D radiographyshould never be used as the sole diagnostic modality inevaluating the foramen position.
4. Three-Dimensional Radio graphy. The literature hasshown that 3-D imaging is the most accurate radiographicmodality to ascertain the exact location of the mentalforamen. Reformatted 3-D images and pano ramic imagesare the easiest and most accurate way of determining exactforamen location.
Continuing Education
3
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
Figures 3a to 3c. (a) Palpation is difficult unless nerve dehiscence is present. (b) Vertical line from pupil-infraorbital foramen—mental foramen. (c) Direct exposure of the mental foramen.
Figures 4a to 4c. (a) The 3-D CBCT showing double foramen containing 2 large nerve trunks. (b) Smaller accessory foramen. (c) Reformatted coronal image showing 2 nerve foramens.
a
a b c
Figures 5a to 5c. (a and b) An anterior loop maybe verified radiographically (axial images) by marking the anterior component of mental foramen and scrolling through the axial images in an inferior position. Clinical evaluation of anterior loop to determine patency of canal; (c) patency confirmed so no anterior loop is present.
a b c
b c
5. Direct Evaluation. The most precise techniqueavailable today to determine the exact location of themental foramen is by direct evaluation. A full thicknessreflection is carried out to reflect the tissue anterior andposterior to the mental foramen. A wet gauze is used togently expose the coronal aspect of the mental foramen.This procedure can be accomplished with very lowmorbidity; however, it is dependent on the implant dentist’straining and experience (Figure 3c).
6. Three-Dimensional Ultra sound. The most promisingimaging technique for mental foramen identification in thefuture is ultrasound. Ultrasound has the advantage of noionizing radiation and the ability to reconstruct 3-D imagesof bone surfaces to within an accuracy level of 24 µm.However, at this time, ultrasound units are not available thatare specific for dental use (Figure 3).
Always Evaluate the Patient for Accessory (Double)ForamensStudies have shown in approximately 2% to 10% of
patients, an accessory (double) foramen is present.9 In themajority of patients, small accessory foramens usuallycontain a small branch of the mental nerve, which are notproblematic because of cross innervation. However, insome cases, a larger branch of the mental nerve (equal orlarger size foramen) may exit the mental foramen. Specialcare should be extended in this area as it may containcomponents of one of the 3 branches of the mental nerve.Accessory foramens are believed to be the result of earlybranching of the inferior alveolar nerve, prior to exiting themental foramen during the twelfth week of gestation.11
Double foramens are easily seen in reformatted 3-D andcoronal images (Figure 4).
Evaluate for Anterior Loops of the Mental NerveAs the mental nerve proceeds anteriorly in the mandible, itsometimes will extend beyond the anterior boundary of themental foramen. This anterior and caudal component of themental nerve is termed an “anterior loop,” which will exit themental foramen in a posterior direction. Recently, CT and
Continuing Education
4
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
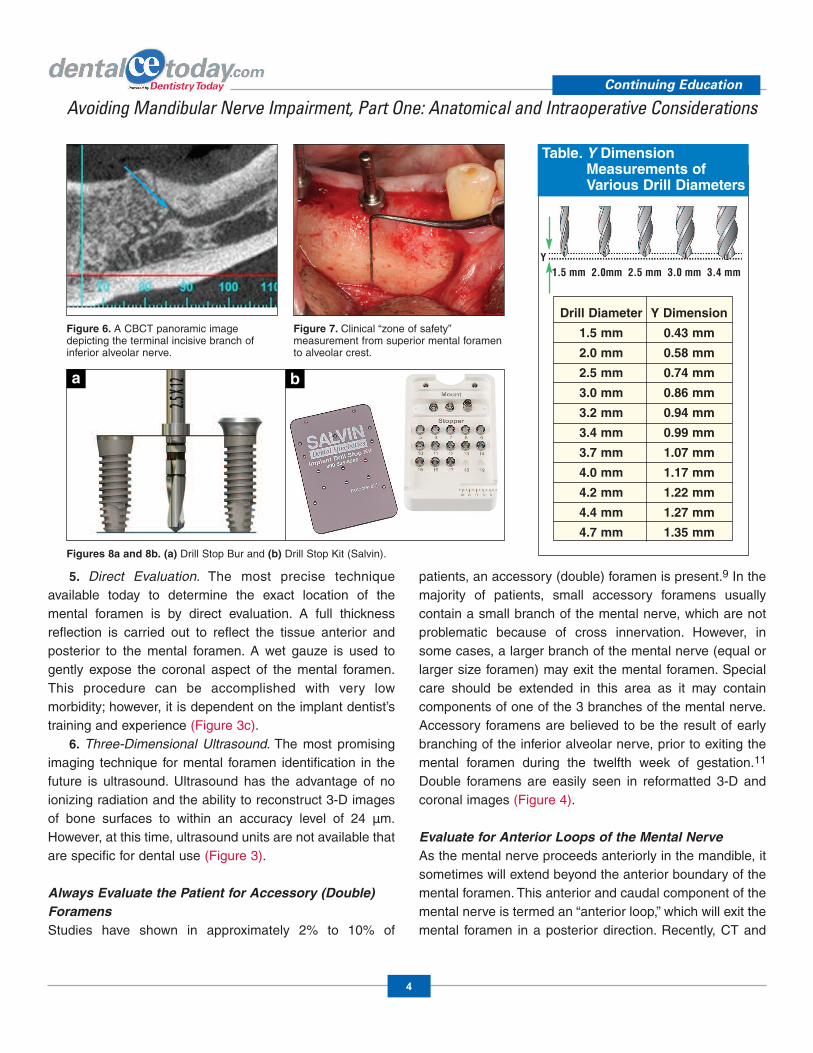
Figure 6. A CBCT panoramic imagedepicting the terminal incisive branch ofinferior alveolar nerve.
Figure 7. Clinical “zone of safety”measurement from superior mental foramento alveolar crest.
Figures 8a and 8b. (a) Drill Stop Bur and (b) Drill Stop Kit (Salvin).
a b
1.5 mm 2.0mm 2.5 mm 3.0 mm 3.4 mm
Table. Y DimensionMeasurements ofVarious Drill Diameters
Y Dimension
0.43 mm
0.58 mm
0.74 mm
0.86 mm
0.94 mm
0.99 mm
1.07 mm
1.17 mm
1.22 mm
1.27 mm
1.35 mm
Drill Diameter
1.5 mm
2.0 mm
2.5 mm
3.0 mm
3.2 mm
3.4 mm
3.7 mm
4.0 mm
4.2 mm
4.4 mm
4.7 mm
Y
dissection studies have shown a higher prevalence (~ 70%)of anterior loops than what was once thought with a meandistance of 1.16 mm anteriorly. The anterior loop may bedepicted most predictably on reformatted axial CT imageswith 2-D radiographs being totally unreliable.12 Clinically, ananterior loop may be determined by probing within themental foramen in a posterior direction. The importance ofdetermining the presence of an anterior loop is critical whenplacing implants anterior to the mental foramen. Inability toestablish the existence of an anterior loop may result inneurosensory impairment of the mental nerve (Figure 5).
Do Not Confuse the Incisive Nerve Branch as anAnterior LoopThe incisive nerve branch has no sensory innervation; thusimplants may be placed in proximity to this nerve withoutneurosensory impairment. Studies have shown that incisivecanals have a mean diameter of 1.8 mm with anapproximate location 9.7 mm from the lower corticalborder.13 The incisive nerve has been recognized as animportant anatomic structure that must be taken intoconsideration when performing surgery in this area. It isfrequently mistaken as an anterior loop in the mandible.Excessive bleeding has been reported as a significantintraoperative complication in this area when perforatedduring osteotomy preparation (Figure 6).
INTRAOPERATIVE CONSIDERATIONSUtilize the “Misch Zone of Safety Principle”To prevent impingement of a dental implant on the inferioralveolar nerve or mental foramen, Misch and Crawford14 in1990 identified the “zone of safety” concept. The zone ofsafety technique reflects the measurement from the superior
aspect of the mental foramen to the crest of the alveolar ridge.It was concluded that the vertical height of bone coronal to themental foramen is present 100% of the time posterior to themiddle half of mandibular first molar, and 97.5% of the time tothe distal of the first molar. Additionally, the correspondingsafety height measurement extends posterior to the mesialhalf of the second molar 43% of the time (Figure 7).14
Maintain a Safety ZoneA 2.0-mm safety zone with osteotomy preparation and finalimplant placement is paramount in preventing neurosensoryimpairments. Com pression-related injuries (neuropraxia) canoccur by encroaching on the inferior alveolar nerve (IAN)without actual contact or invasion of the MC. Bleeding andresultant hematomas have been shown to cause nervedamage because of final implant positioning too close to theneurovascular canal.15 Addition ally, the IAN superior corticalbone can be compressed, thus causing pressure necrosis,with resultant nerve impairment.16 Interactive treatmentplanning software programs (ie, SimPlant [Material ize Dental])allow the implant dentist to accurately assess the idealplacement and insure adequate distance from the MC.
Understand the True Implant Bur Drilling DepthsCare should always be exercised when performing osteotomiesover vital structures, most importantly in the posterior mandible.The implant dentist should always double check the markingdepth on the burs prior to initiating the osteotomy. The principleof measure twice and drill once should be followed to preventiatrogenic overpreparation of the implant site. Also, the ydimension of the implant system being used must be known.The depth of the millimeter lines inscribed on surgical drills donot always coincide with the actual depth of the drill. Most drills
Continuing Education
5
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
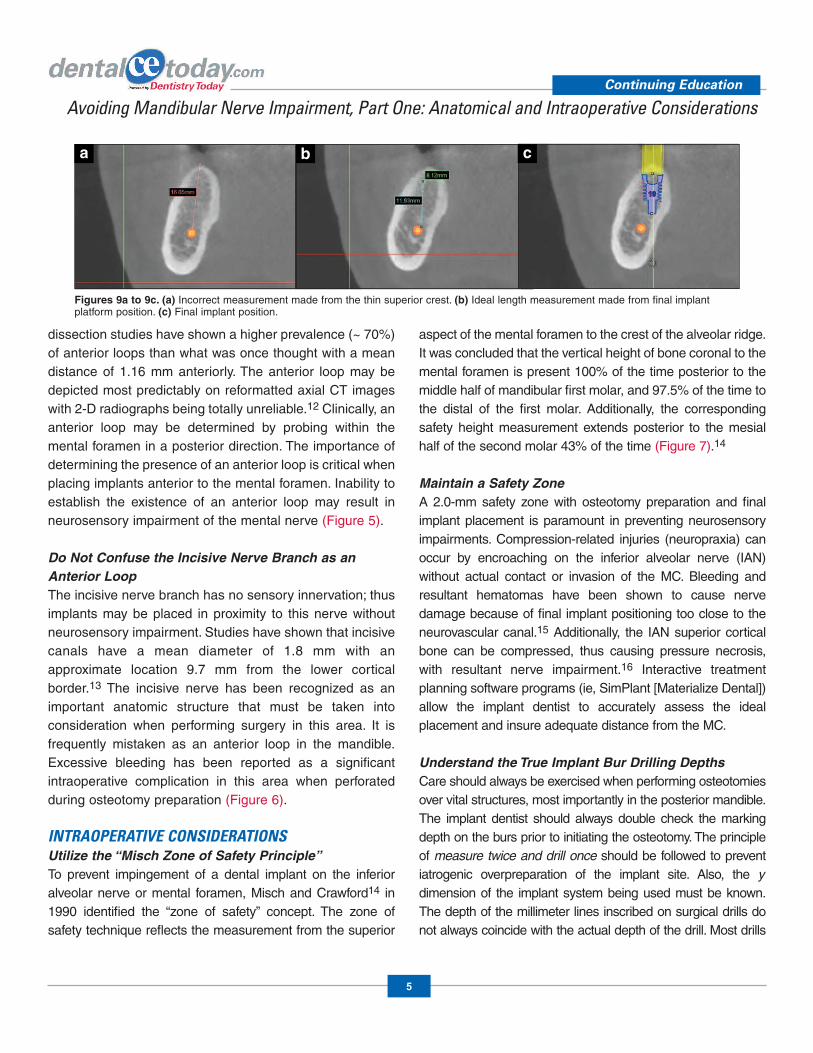
Figures 9a to 9c. (a) Incorrect measurement made from the thin superior crest. (b) Ideal length measurement made from final implant platform position. (c) Final implant position.
a b c

contain a v-shaped apical portion, which isdesigned for cutting efficiency (y dimension).Usually, the wider the drill, the greater the ydimension.17 Therefore, the implant dentistshould always evaluate the manufacturer’s drilllength with respect to the length of the implantprior to performing the osteotomy. If this conceptis not adhered to, overpreparation of the site mayoccur, resulting in nerve damage (Table).
Use Drill Stops to Prevent OverpreparationTo obtain precise depth control duringosteotomy preparation, the use of specialdrills with predetermined “stops” can be used.These stop drills prevent overpreparation ofthe osteotomy site and are extremelybeneficial in the mandibular posterior area,especially when visibility and access arecompromised. Generic drill stop kits areavailable which may be used universally withmost implant surgical systems (ie, Salvin CorpDrill Kit). This autoclavable, reusable kit maybe used with all implant systems and corresponds to any sizelength implant and corresponding drill (Figure 8).
Understand Bony Crest AnatomyAfter extraction, normal bone resorption results with thealveolar ridge becoming compromised in width (Division BBone) at the expense of the buccal plate. When measuringavailable bone height, special consideration should be givento the final location of the superior aspect of the implantplatform, not the crest of the ridge. It will often appear thatadequate vertical height for implant placement is sufficient;however, when the osteotomy is initiated, the thin crest will belost, thus the implant will be placed inferior to where it isoriginally intended. This can lead to unexpected depth drillingand an implant that is placed too close to the MC. Thus, theclinician should either augment the ridge to maintain verticalheight or reduce the height calculation by the amount ofosteoplasty during osteotomy preparation (Figure 9).
Maintain Total Control of the HandpieceWhen performing osteotomies in the posterior mandible,
special care should be noted to maintain complete control ofthe surgical handpiece. Large marrow spaces (lack of or thintrabecular bone) are often present, which may allow theosteotomy site to become deeper than expected. This willresult in the implant being placed more apically, leading toneurosensory impairment. A CBCT comprehensiveevaluation will allow the implant dentist to evaluate the bonequality prior to surgery. Additionally, when drilling osteotomysites near the mental foramen, care should be exercised notto bend the wrist when drilling the osteotomy. This canpotentially redirect the drill or im plant placement in anunwanted position (ie, near the mental foramen, into a toothroot). Also, to minimize this complication, surgical templatesand guides may be utilized (Figure 10).
Do Not Place Bone Graft Material in CloseApproximation to the NerveAfter mandibular posterior tooth extractions, especially inthe man dibular premolar areas, care should be exercised inplacing bone graft material (autologous, allogenic,xenogenic) in direct contact with an exposed MC. Whether
Continuing Education
6
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
Figures 10a and 10b. (a) Ideal placement with respect to the nerve. (b) Misdirection of theimplant from improper drilling technique.
a b
Figure 11. Cross section showing closeapproximation of apical root and nervecanal.
Figure 12. During osteotomy preparation,copious amounts of irrigation must be usedto decrease heat generation.
socket grafting or in conjunction with implantplacement, case studies have shownresultant neurosensory impairment frombone graft material causing compression,crushing, or chemical burn injuries.18 Whensocket grafting in this area is indicated,excessive pressure should be avoided whenplacing the graft material (Figure 11).
Use Copious IrrigationOverheating the bone during oste otomypreparation may produce thermal stimuli,which may lead to peri-implant necrosis andsecondary postoperative nerve damage. Thethickness of the necrotic area is proportionalto the amount of heat generated duringpreparation.19 Thus, the implant dentist mustbe cautious with respect to overheating thebone. This can be minimized by “bonedancing,” which involves drilling in shortintervals and allowing irrigation to enter the osteotomy.Addi tionally, new (sharp) and intermediate sized drills bursmay be used to reduce heat generation along withsecondary irrigation. Overheating the bone is more criticalwhen harder bone density or bone with compromisedvascularity is present (Figure 12).
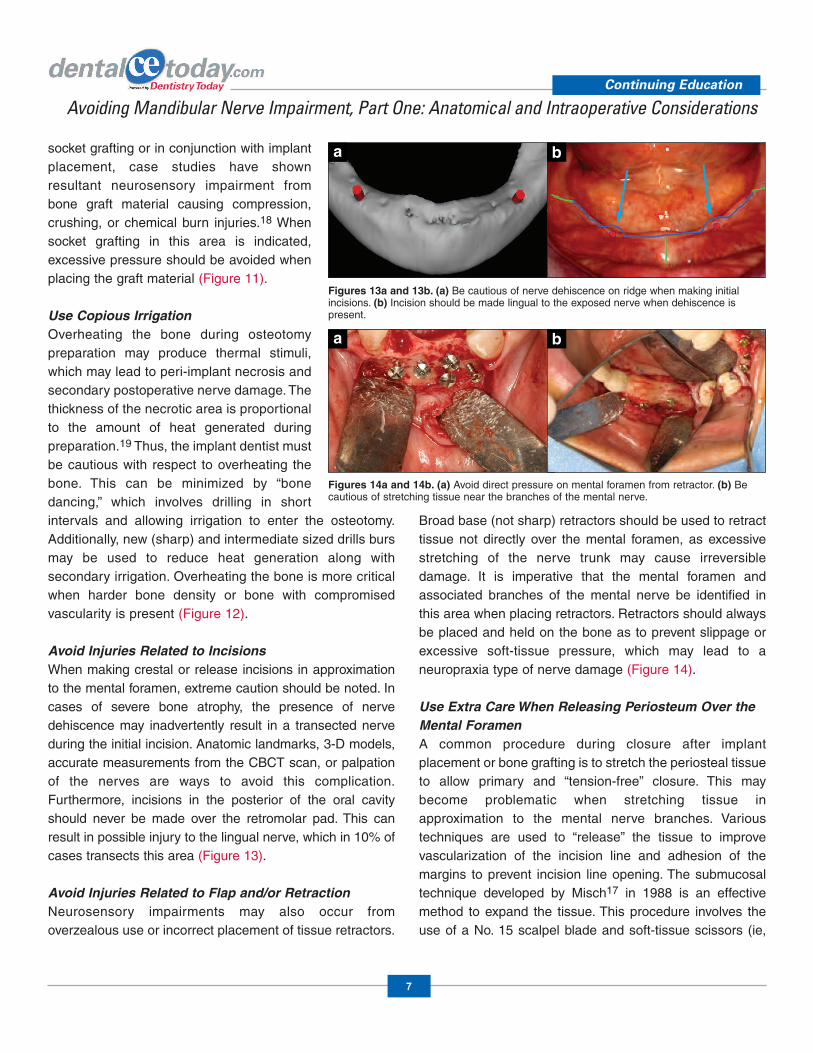
Avoid Injuries Related to IncisionsWhen making crestal or release incisions in approximationto the mental foramen, extreme caution should be noted. Incases of severe bone atrophy, the presence of nervedehiscence may inadvertently result in a transected nerveduring the initial incision. Anatomic landmarks, 3-D models,accurate measurements from the CBCT scan, or palpationof the nerves are ways to avoid this complication.Furthermore, incisions in the posterior of the oral cavityshould never be made over the retromolar pad. This canresult in possible injury to the lingual nerve, which in 10% ofcases transects this area (Figure 13).
Avoid Injuries Related to Flap and/or Retraction Neurosensory impairments may also occur fromoverzealous use or incorrect placement of tissue retractors.
Broad base (not sharp) retractors should be used to retracttissue not directly over the mental foramen, as excessivestretching of the nerve trunk may cause irreversibledamage. It is imperative that the mental foramen andassociated branches of the mental nerve be identified inthis area when placing retractors. Retrac tors should alwaysbe placed and held on the bone as to prevent slippage orexcessive soft-tissue pressure, which may lead to aneuropraxia type of nerve damage (Figure 14).
Use Extra Care When Releasing Periosteum Over theMental ForamenA common procedure during closure after implantplacement or bone grafting is to stretch the periosteal tissueto allow primary and “tension-free” closure. This maybecome problematic when stretching tissue inapproximation to the mental nerve branches. Varioustechniques are used to “release” the tissue to im provevascularization of the incision line and adhesion of themargins to prevent incision line opening. The submucosaltechnique developed by Misch17 in 1988 is an effectivemethod to expand the tissue. This procedure involves theuse of a No. 15 scalpel blade and soft-tissue scissors (ie,
Continuing Education
7
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
Figures 13a and 13b. (a) Be cautious of nerve dehiscence on ridge when making initial incisions. (b) Incision should be made lingual to the exposed nerve when dehiscence is present.
a b
Figures 14a and 14b. (a) Avoid direct pressure on mental foramen from retractor. (b) Becautious of stretching tissue near the branches of the mental nerve.
a b
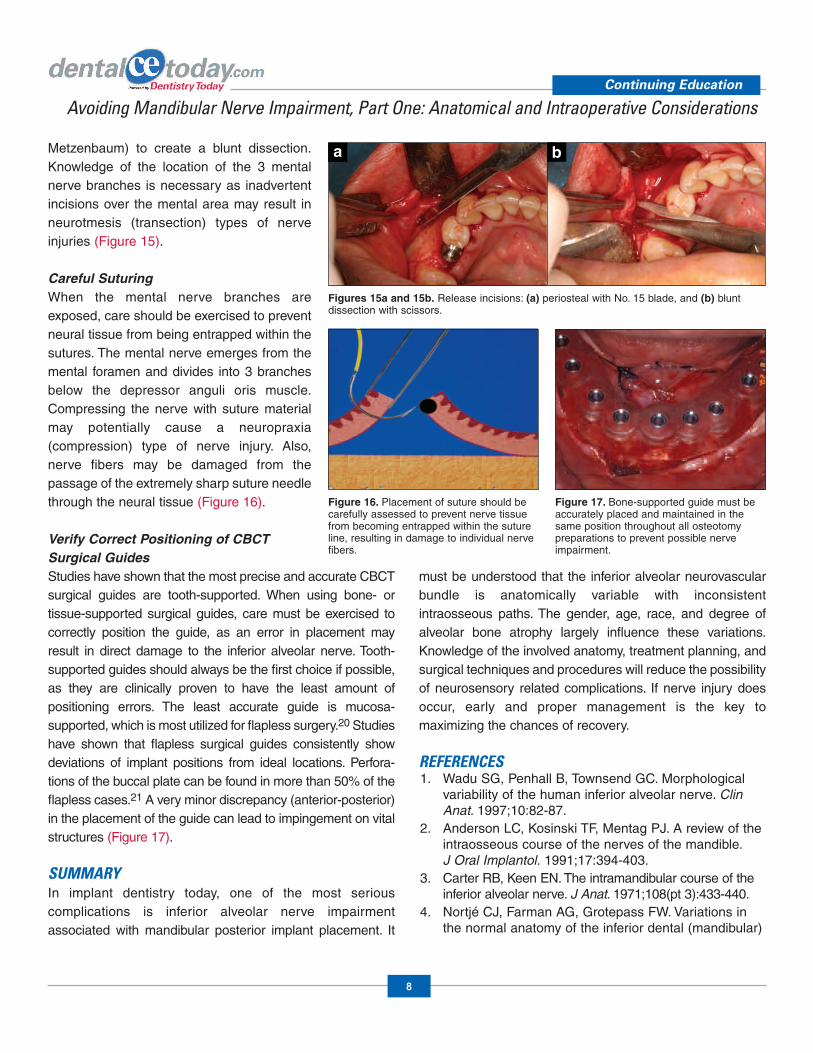
Metzenbaum) to create a blunt dissection.Knowledge of the location of the 3 mentalnerve branches is necessary as inadvertentincisions over the mental area may result inneurotmesis (transection) types of nerveinjuries (Figure 15).
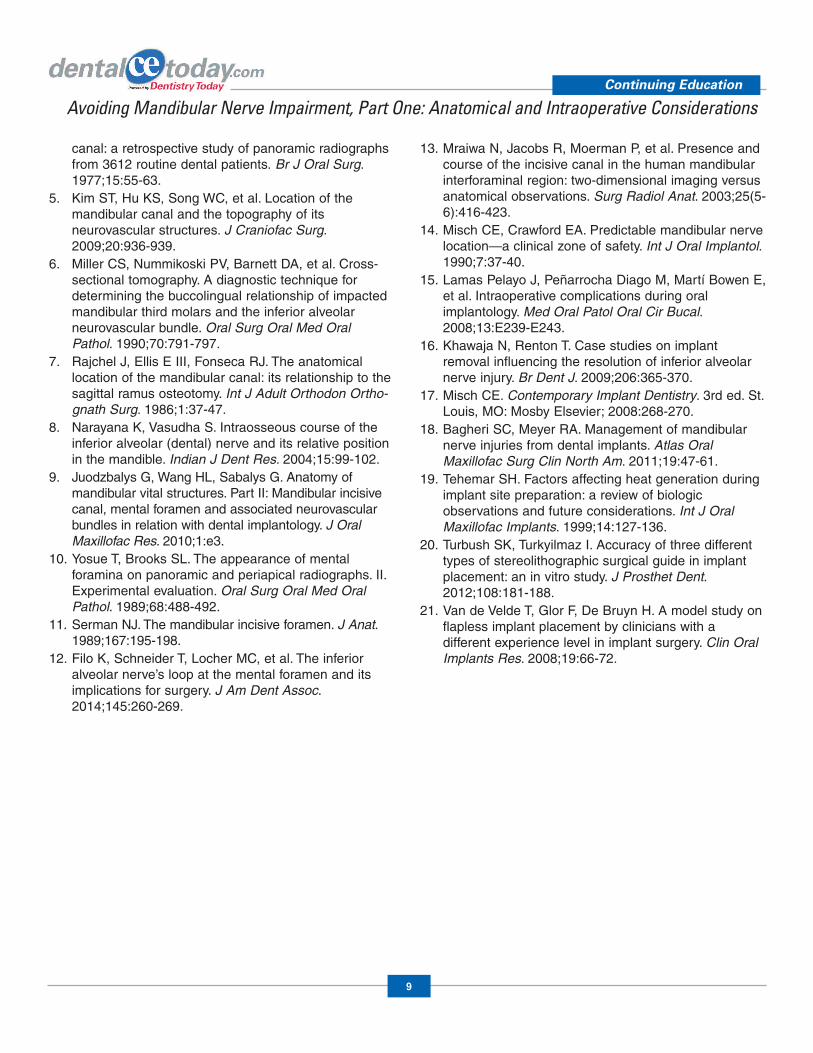
Careful SuturingWhen the mental nerve branches areexposed, care should be exercised to preventneural tissue from being entrapped within thesutures. The mental nerve emerges from themental foramen and divides into 3 branchesbelow the depressor anguli oris muscle.Compressing the nerve with suture materialmay potentially cause a neuropraxia(compression) type of nerve injury. Also,nerve fibers may be damaged from thepassage of the extremely sharp suture needlethrough the neural tissue (Figure 16).
Verify Correct Positioning of CBCTSurgical GuidesStudies have shown that the most precise and accurate CBCTsurgical guides are tooth-supported. When using bone- ortissue-supported surgical guides, care must be exercised tocorrectly position the guide, as an error in placement mayresult in direct damage to the inferior alveolar nerve. Tooth-supported guides should al ways be the first choice if possible,as they are clinically proven to have the least amount ofpositioning errors. The least accurate guide is mucosa-supported, which is most utilized for flapless surgery.20 Studieshave shown that flapless surgical guides consistently showdeviations of im plant positions from ideal locations. Perfora -tions of the buccal plate can be found in more than 50% of theflapless cases.21 A very minor discrepancy (anterior-posterior)in the placement of the guide can lead to impingement on vitalstructures (Figure 17).
SUMMARYIn implant dentistry today, one of the most seriouscomplications is inferior alveolar nerve impairmentassociated with mandibular posterior implant placement. It
must be understood that the inferior alveolar neurovascularbundle is anatomically variable with inconsistentintraosseous paths. The gender, age, race, and degree ofalveolar bone atrophy largely influence these variations.Knowledge of the involved anatomy, treatment planning, andsurgical techniques and procedures will reduce the possibilityof neurosensory related complications. If nerve injury doesoccur, early and proper management is the key tomaximizing the chances of recovery.
REFERENCES1. Wadu SG, Penhall B, Townsend GC. Morpho logical
variability of the human inferior alveolar nerve. ClinAnat. 1997;10:82-87.
2. Anderson LC, Kosinski TF, Mentag PJ. A review of theintraosseous course of the nerves of the mandible. J Oral Implantol. 1991;17:394-403.
3. Carter RB, Keen EN. The intramandibular course of theinferior alveolar nerve. J Anat. 1971;108(pt 3):433-440.
4. Nortjé CJ, Farman AG, Grotepass FW. Variations inthe normal anatomy of the inferior dental (mandibular)
Continuing Education
8
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
Figures 15a and 15b. Release incisions: (a) periosteal with No. 15 blade, and (b) blunt dissection with scissors.
Figure 16. Placement of suture should becarefully assessed to prevent nerve tissuefrom becoming entrapped within the sutureline, resulting in damage to individual nervefibers.
Figure 17. Bone-supported guide must beaccurately placed and maintained in thesame position throughout all osteotomypreparations to prevent possible nerveimpairment.
a b
canal: a retrospective study of panoramic radiographsfrom 3612 routine dental patients. Br J Oral Surg.1977;15:55-63.
5. Kim ST, Hu KS, Song WC, et al. Location of themandibular canal and the topography of itsneurovascular structures. J Craniofac Surg.2009;20:936-939.
6. Miller CS, Nummikoski PV, Barnett DA, et al. Cross-sectional tomography. A diagnostic technique fordetermining the buccolingual relationship of impactedmandibular third molars and the inferior alveolarneurovascular bundle. Oral Surg Oral Med OralPathol. 1990;70:791-797.
7. Rajchel J, Ellis E III, Fonseca RJ. The anatomicallocation of the mandibular canal: its relationship to thesagittal ramus osteotomy. Int J Adult Orthodon Or tho- gnath Surg. 1986;1:37-47.
8. Narayana K, Vasudha S. Intraosseous course of theinferior alveolar (dental) nerve and its relative positionin the mandible. Indian J Dent Res. 2004;15:99-102.
9. Juodzbalys G, Wang HL, Sabalys G. Anatomy ofmandibular vital structures. Part II: Mandibular incisivecanal, mental foramen and associated neurovascularbundles in relation with dental implantology. J OralMaxillofac Res. 2010;1:e3.
10. Yosue T, Brooks SL. The ap pearance of mentalforamina on panoramic and periapical radio graphs. II.Experimental eval uation. Oral Surg Oral Med OralPathol. 1989;68:488-492.
11. Serman NJ. The mandibular incisive foramen. J Anat.1989;167:195-198.
12. Filo K, Schneider T, Locher MC, et al. The inferioralveolar nerve’s loop at the mental foramen and itsimplications for surgery. J Am Dent Assoc.2014;145:260-269.
13. Mraiwa N, Jacobs R, Moerman P, et al. Pres ence andcourse of the in cisive canal in the human mandibularinterforaminal region: two-dimensional imaging versusanatomical observations. Surg Radiol Anat. 2003;25(5-6):416-423.
14. Misch CE, Crawford EA. Predictable mandibular nervelocation—a clinical zone of safety. Int J Oral Implantol.1990;7:37-40.
15. Lamas Pelayo J, Peñar rocha Diago M, Martí Bowen E,et al. Intra operative complications during oralimplantology. Med Oral Patol Oral Cir Bucal.2008;13:E239-E243.
16. Khawaja N, Renton T. Case studies on implantremoval influencing the resolution of inferior alveolarnerve injury. Br Dent J. 2009;206:365-370.
17. Misch CE. Contemporary Implant Dentistry. 3rd ed. St.Louis, MO: Mosby Elsevier; 2008:268-270.
18. Bagheri SC, Meyer RA. Management of mandibularnerve injuries from dental implants. Atlas OralMaxillofac Surg Clin North Am. 2011;19:47-61.
19. Tehemar SH. Factors affecting heat generation duringimplant site preparation: a review of biologicobservations and future considerations. Int J OralMaxillofac Implants. 1999;14:127-136.
20. Turbush SK, Turkyilmaz I. Accuracy of three differenttypes of stereolithographic surgical guide in implantplacement: an in vitro study. J Prosthet Dent.2012;108:181-188.
21. Van de Velde T, Glor F, De Bruyn H. A model study onflapless implant placement by clinicians with adifferent experience level in implant surgery. Clin OralImplants Res. 2008;19:66-72.
Continuing Education
9
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
POST EXAMINATION INFORMATION
To receive continuing education credit for participation in thiseducational activity you must complete the program post examinationand answer 9 out of 12 questions correctly.
Traditional Completion Option:You may fax or mail your answers with payment to Dentistry Today(see Traditional Completion Information on following page). Allinformation requested must be provided in order to process theprogram for credit. Be sure to complete your “Payment,” “PersonalCertification Information,” “Answers,” and “Evaluation” forms. Yourexam will be graded within 72 hours of receipt. Upon successfulcompletion of the post-exam (answer 9 out of 12 questionscorrectly), a letter of completion will be mailed to the addressprovided.
Online Completion Option:Use this page to review the questions and mark your answers.Return to dentalcetoday.com and sign in. If you have notpreviously purchased the program, select it from the “OnlineCourses” listing and complete the online purchase process. Oncepurchased the program will be added to your User History pagewhere a Take Exam link will be provided directly across from theprogram title. Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate grade report willbe provided. Upon receiving a passing grade, complete the onlineevaluation form. Upon submitting the form, your Letter ofCompletion will be provided immediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time in thefuture to access previously purchased programs and view or printletters of completion and results.
POST EXAMINATION QUESTIONS1. Studies have confirmed the inferior-superior (vertical)
positions of the MC are consistent and wide variation does notexist.
a. True b. False
2. Although the mental foramen has been shown to besymmetrical to the contralateral side in most patients, thelocation has been shown to be highly variable.
a. True b. False
3. Studies have shown that in more than 80% of periapical andpanoramic radiographs, the mental foramen is in the locationas depicted on the image.
a. True b. False
4. Studies have shown in approximately 2% to 10% of patients, anaccessory (double) foramen is present.
a. True b. False
5. The anterior loop may be depicted most predictably onreformatted axial CT images; however, even 2-D radiographicdepiction is totally reliable.
a. True b. False
6. Studies have shown incisive canals have a mean diameter of1.8 mm with an approximate location 9.7 mm from the lowercortical border.
a. True b. False
7. Bleeding and resultant hematomas have been shown to causenerve damage because of final implant positioning too close tothe neurovascular canal.
a. True b. False
8. The principle of “measure twice and drill once” should befollowed to prevent iatrogenic over preparation of the implantsite.
a. True b. False
9. The thickness of the necrotic area is proportional to theamount of heat generated during preparation.
a. True b. False
10. Additionally, incisions in the posterior of the oral cavity shouldalways be made over the retromolar pad.
a. True b. False
11. When the mental nerve branches are exposed, care should beexercised to prevent neural tissue from being entrapped withinthe sutures.
a. True b. False
12. The most accurate guide is mucosa-supported, which are mostutilized for flapless surgery.
a. True b. False
Continuing Education
10
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.
PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer 9 of the 12questions correctly.
Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $60.00 Credit Hours: 3
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.
o I am using a credit card.
My Credit Card information is provided below.
o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.
Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved.
Content was useful and benefited your clinical practice.
Review questions were clear and relevant to the editorial.
Illustrations and photographs were clear and relevant.
Written presentation was informative and concise.
How much time did you spend reading the activity and completing the test?
What aspect of this course was most helpful and why?
What topics interest you for future Dentistry Today CE courses?
Continuing Education
Avoiding Mandibular Nerve Impairment, Part One: Anatomical and Intraoperative Considerations
ANSWER FORM: VOLUME 33 NO. 11 PAGE 96Please check the correct box for each question below.
1. o a. True o b. False 7. o a. True o b. False
2. o a. True o b. False 8. o a. True o b. False
3. o a. True o b. False 9. o a. True o b. False
4. o a. True o b. False 10. o a. True o b. False
5. o a. True o b. False 11. o a. True o b. False
6. o a. True o b. False 12. o a. True o b. False
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
11
This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.