autonomic pharmacology - cardiovascular system trachte [email protected] 8:00 am 9/18/08
TRANSCRIPT
Autonomic Pharmacology - Cardiovascular System
Trachte
8:00 AM 9/18/08
Goals
• To understand where & how a drug acts and what its effect on the cardiovascular system is.
• While side effects and routes of administration will be presented, it is unlikely that they will appear on examinations.
• Side effects predicted from a drug's mechanism of action are fair game.
• Drugs in boldface lettering are the ones you are expected to know (about 50 in autonomics).
Definition of Autonomic Nervous
System•Generally have two efferent fibers - preganglionic and post ganglionic
•Control vegetative functions
Divisions
• Parasympathetic– Origins (midbrain, medulla oblongata, sacrum)- medulla important for cardiovascular
– Usually long preganglionic fiber causing discrete (localized) responses
– Neurotransmitter is acetylcholine• Sympathetic
– Origin - thoracic-lumbar cord– Characteristically short preganglionic fibers- release acetylcholine
– Diffuse response- para vertebral, prevertebral, and terminal ganglia
– Postganglionic neurotransmitter is normally norepinephrine, can also be acetylcholine, possibly ATP, epinephrine (adrenal gland) & neuropeptide Y
Major Receptors
•Parasympathetic
– nicotinic receptor - located on postsynaptic surface of postganglionic nerve; causes activation of postganglionic nerve
– muscarinic receptor - all end-organ responses by activating phospholipase C or suppressing adenylyl cyclase activity (latter more important in heart)
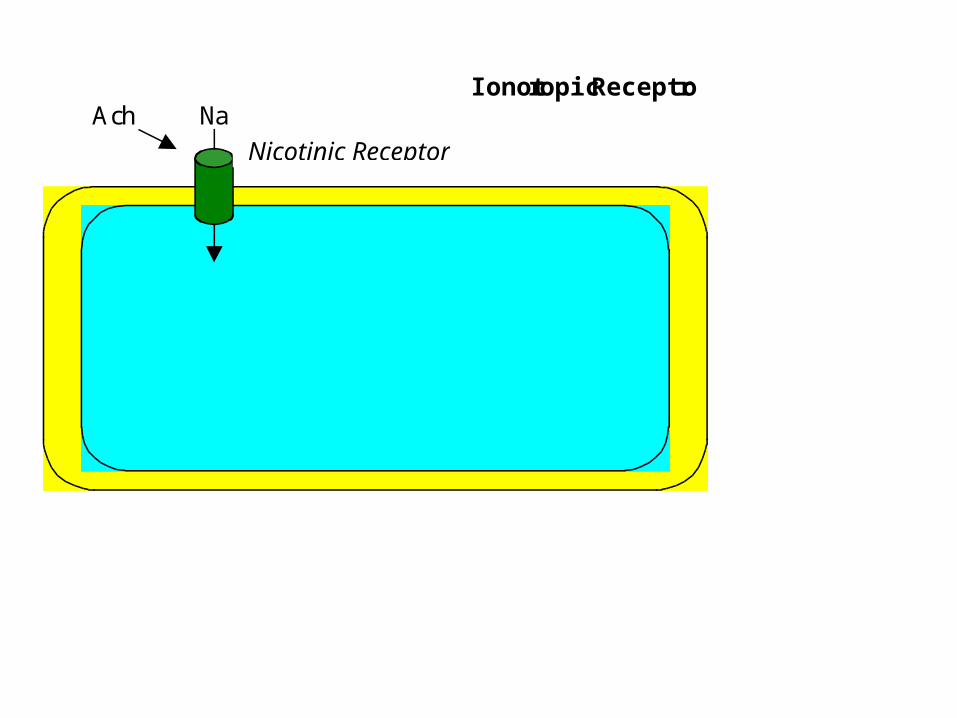
Ionotropic Receptor Ach Na Na
Nicotinic Receptor
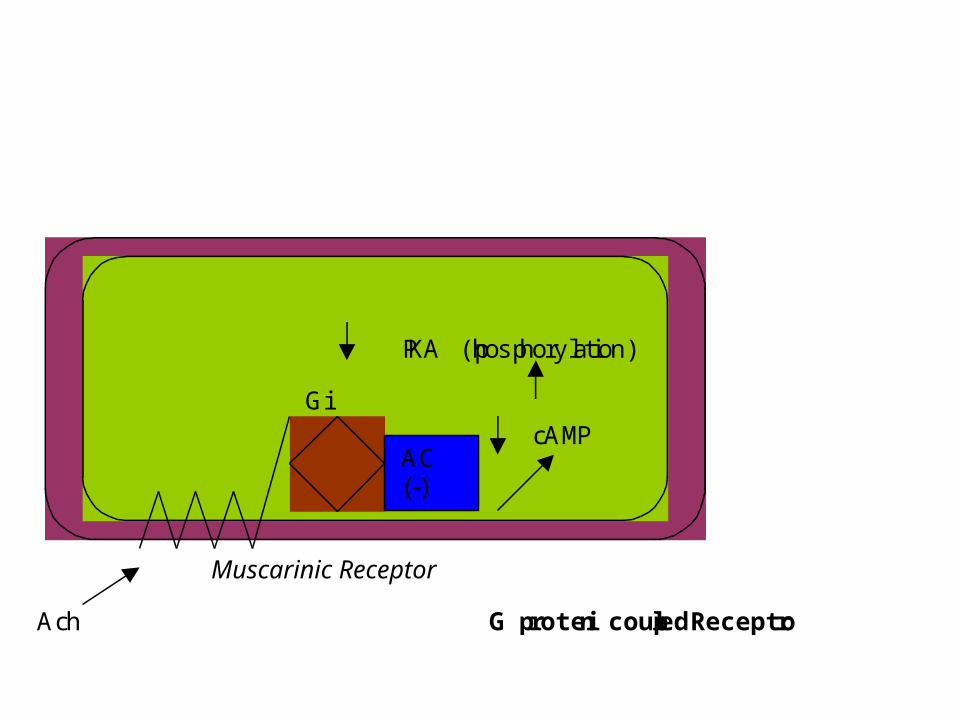
Ach G protein coupled Receptor
PKA (phosphorylation) cAMP
Muscarinic Receptor
Gi
AC (-)
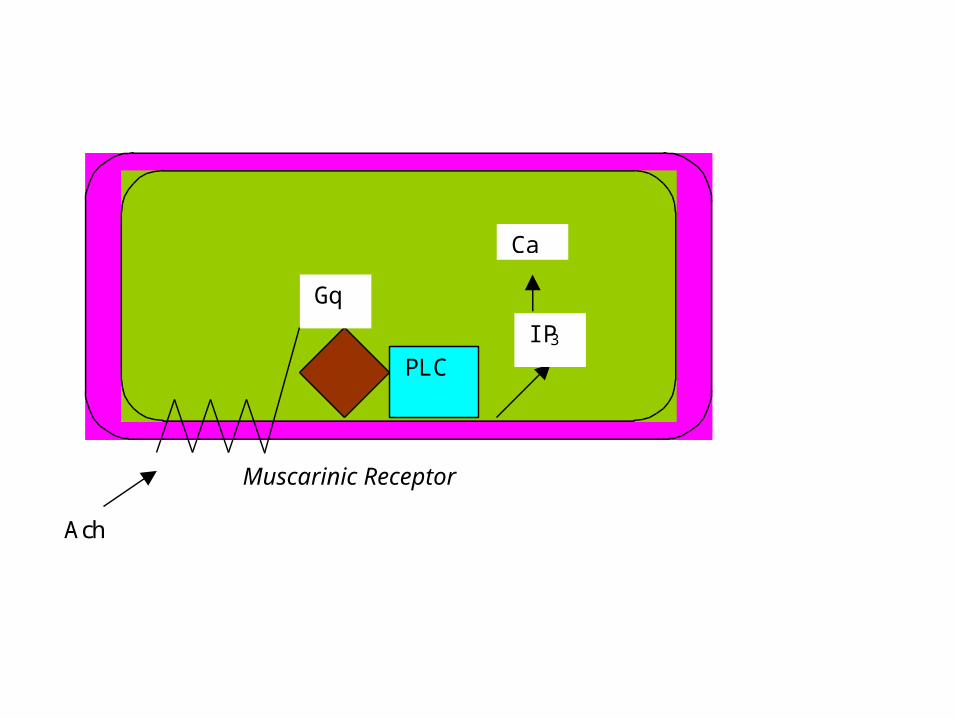
Muscarinic Receptor
Gq
PLC
IP3
Ca
Ach
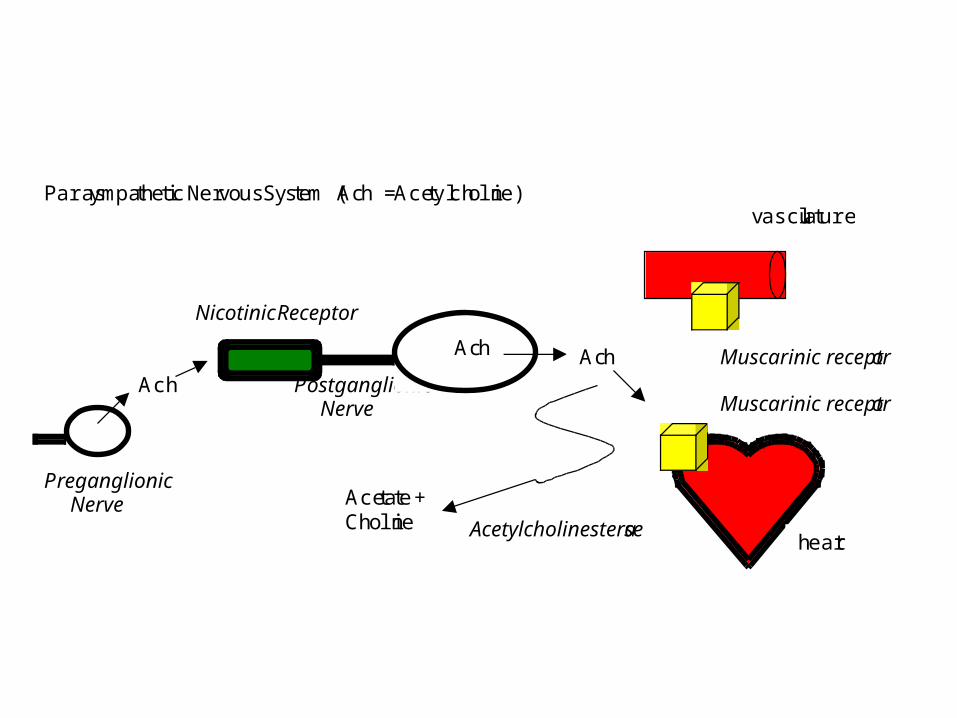
Parasympathetic Nervous System (Ach = Acetylcholine) Nicotinic Receptor Ach Postganglionic Nerve Ach Preganglionic Nerve
Ach Muscarinic receptor
Muscarinic receptor
Ach
Acetate + Choline Acetylcholinesterase
heart
vasculature
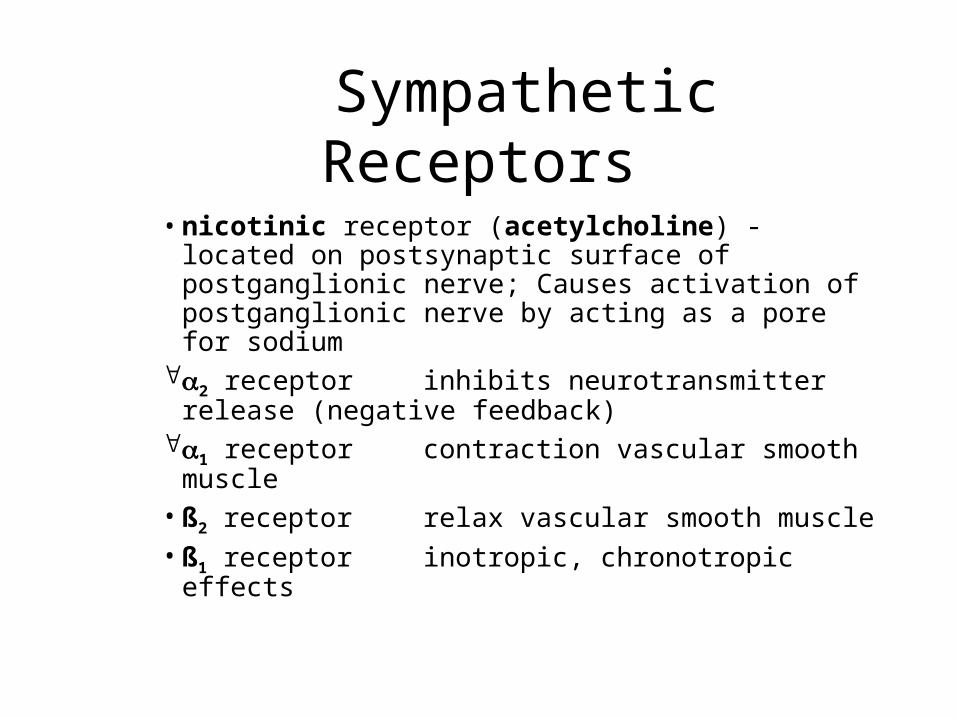
Sympathetic Receptors
•nicotinic receptor (acetylcholine) - located on postsynaptic surface of postganglionic nerve; Causes activation of postganglionic nerve by acting as a pore for sodium
2 receptor inhibits neurotransmitter release (negative feedback)
1 receptor contraction vascular smooth muscle
•ß2 receptor relax vascular smooth muscle
•ß1 receptor inotropic, chronotropic effects
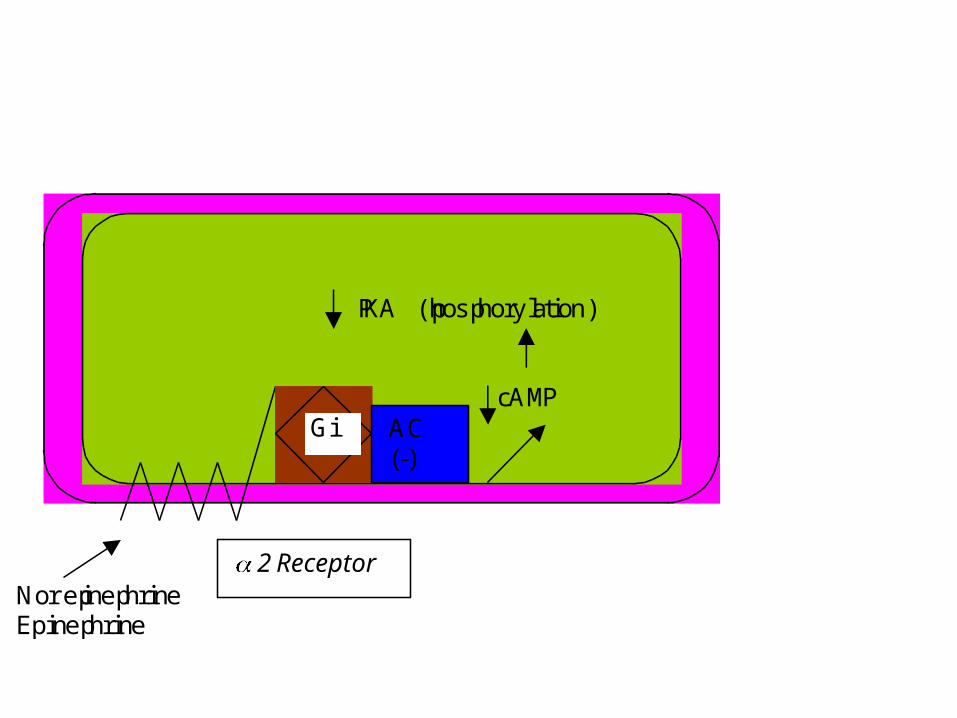
Norepinephrine Epinephrine
PKA (phosphorylation) cAMP
2 Receptor
Gi AC (-)
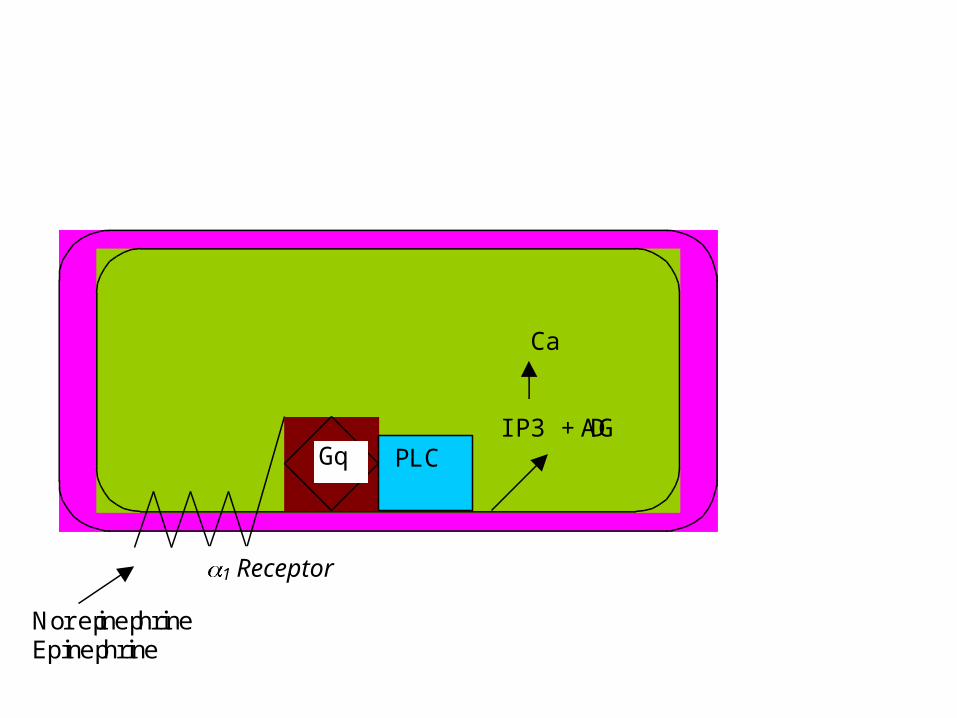
Norepinephrine Epinephrine
Ca IP3 + DAG
1 Receptor
Gq PLC

Norepinephrine or Epinephrine
PKA (phosphorylation) cAMP
ß 1 Receptor
Gs AC
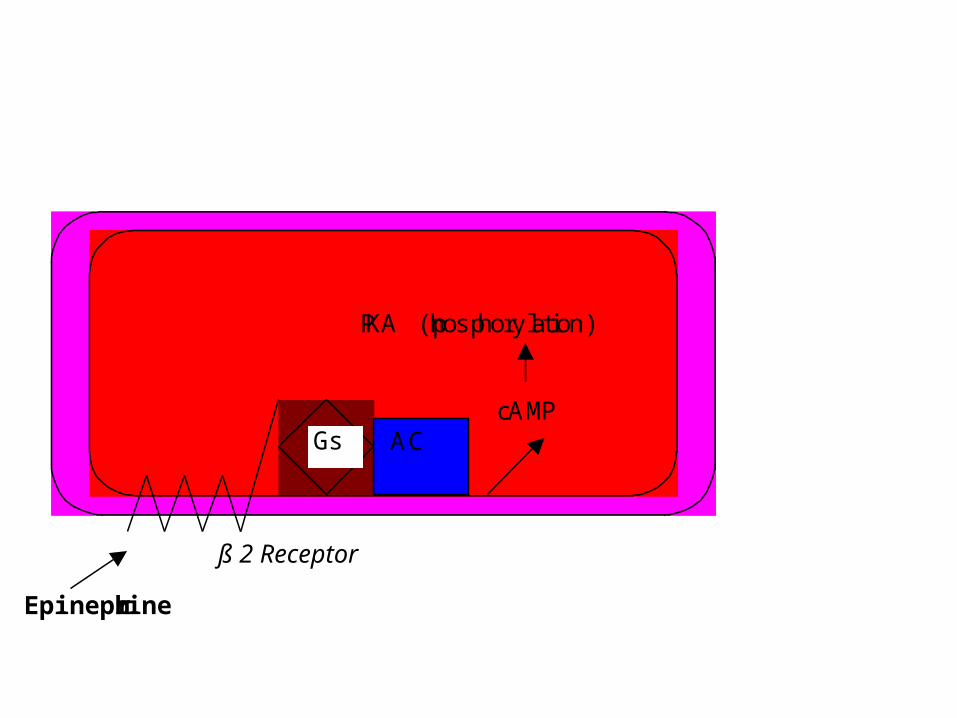
Epinephrine
PKA (phosphorylation) cAMP
ß 2 Receptor
Gs AC
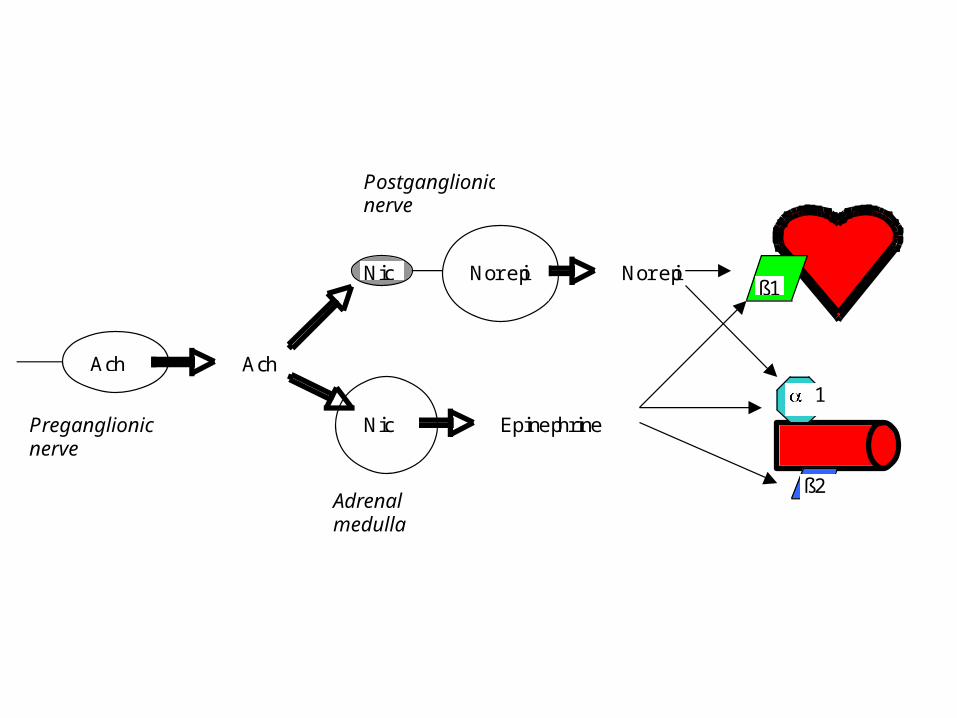
Ach Ach
Norepi
Epinephrine Preganglionic nerve
Postganglionic nerve
Adrenal medulla
Norepi
ß2
ß1
1
Nic
Nic
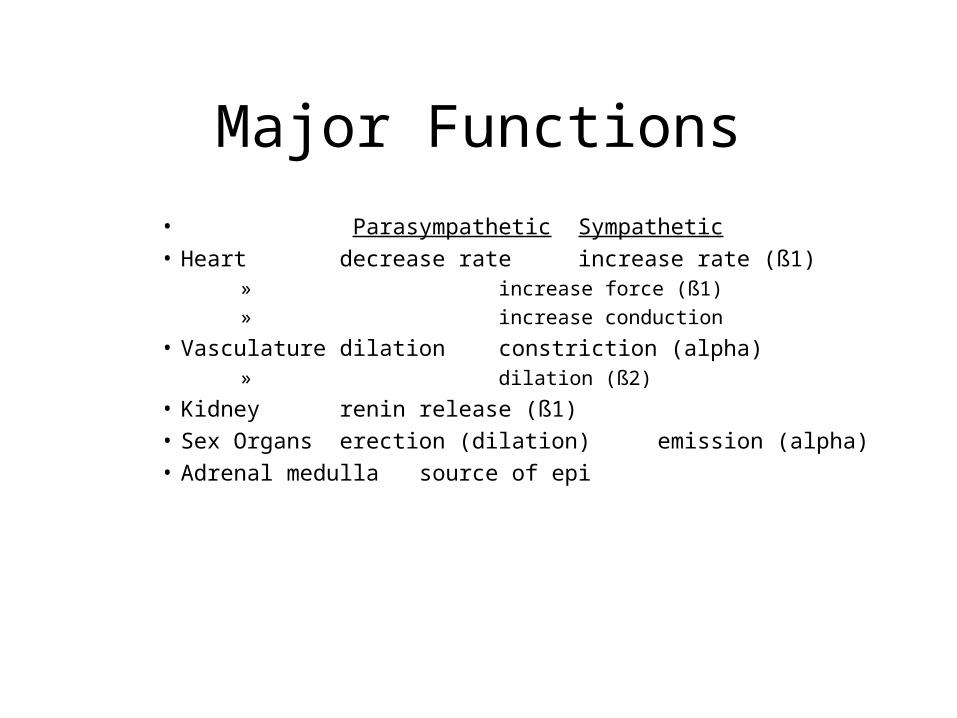
Major Functions
• Parasympathetic Sympathetic• Heart decrease rate increase rate (ß1)
» increase force (ß1)
» increase conduction
• Vasculature dilation constriction (alpha)
» dilation (ß2)
• Kidney renin release (ß1)• Sex Organs erection (dilation) emission (alpha)
• Adrenal medulla source of epi
So, what would you do to treat bradycardia?
• Stimulate parasympathetics
• Inhibit parasympathetics
• Stimulate sympathetics
• Inhibit sympathetics
So what would you do to treat tachycardia?
• Stimulate parasympathetics
• Inhibit parasympathetics
• Stimulate Sympathetics
• Inhibit sympathetics
Parasympathetic Nervous System
• Acetylcholine– Synthesis– Storage– Release– Termination
Synthesis and Degradation of Acetylcholine
• Synthesis and storage
•choline acetyltransferase [choline + acetyl CoA --> acetylcholine + CoA (cytoplasm)]
•Acetylcholine stored in vesicles
Synthesis and Degradation of Acetylcholine
• Acetylcholine release from post-ganglionic nerves– induced by depolarization, usually after
acetylcholine stimulates nicotinic receptors on post-synaptic surface of postganglionic nerve
– depolarization activates voltage-sensitive calcium influx
– agents blocking acetylcholine release• Clostridium botulinum toxin• Tetracycline, streptomycin
– black widow spider venom (latratoxin) promotes excessive release
Synthesis and Degradation of Acetylcholine
• Removal by degradation involving acetylcholinesterase– similar enzyme, butyryl cholinesterase is present in liver, etc.
– choline is taken up by nerve terminal
– hemicholinium inhibits choline uptake
CHOLINOMIMETICS AND ACETYLCHOLINE
• Acetylcholine
• Cholinomimetic Alkaloids
• Choline Esters
Acetylcholine (Miochol intraocular)
Diffuse actions (when administered parenterally), include stimulation of: parasympathetic end organs (muscarinic); ganglia and adrenal medulla (nicotinic); CNS synapses (muscarinic); skeletal muscle (nicotinic); eccrine sweat glands and dilation of skeletal muscle vasculature (sympathetic-muscarinic)– a) major effects of i.v. injection are vasodilation and bradycardia (also gut contraction and digestive enzyme secretion (i.e., muscarinic activation))
– b) vasodilator effect dependent on the production of a vasodilator (nitric oxide) by vascular endothelium - the nitric oxide increases cyclic GMP generation in smooth muscle
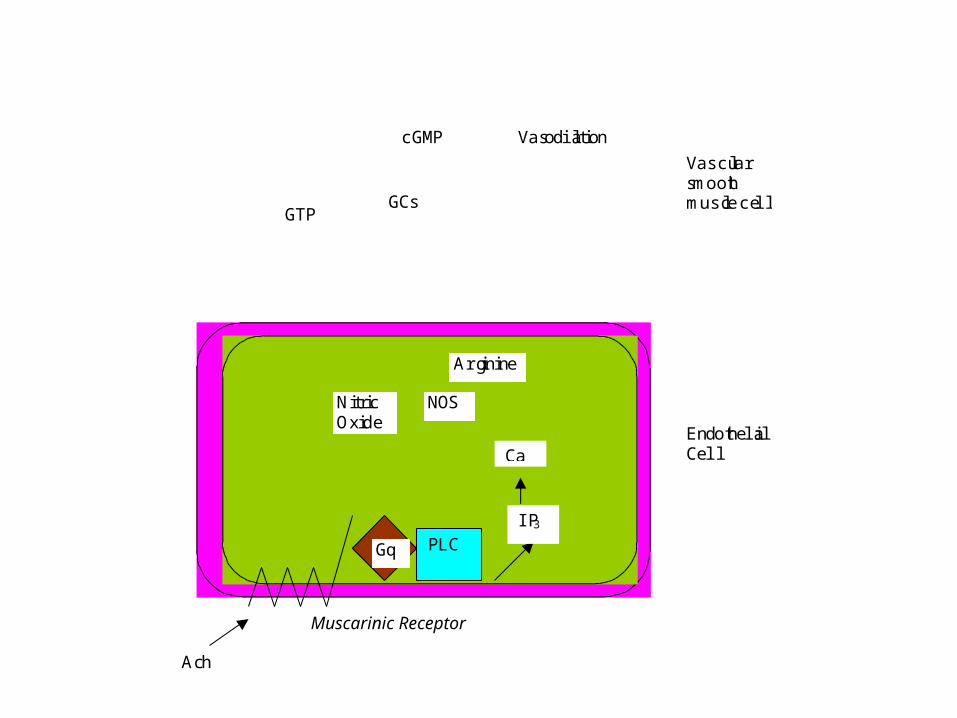
Muscarinic Receptor
Gq PLC
IP3
Ca
Ach
NOS
Arginine
Nitric Oxide
GCs GTP
cGMP Vasodilation
Endothelial Cell
Vascular smooth muscle cell
Acetylcholine (Miochol intraocular)
Muscarinic receptors ATROPINE is classic antagonist;muscarine is classic agonist
mechanism of action• Nicotinic receptors
– NICOTINE classic agonist– mediate skeletal muscle contraction, adrenal catechole secretion and depolarization of postganglionic nerves
– mechanism to increase Na+ permeability (it’s a cation channel)
– numerous receptor isoforms (different receptors on skeletal muscle and ganglia)
Acetylcholine (Miochol intraocular)
•Absorption of acetylcholine from the GI tract is poor (quaternary ammonium compound)
•Therapeutic Uses of acetylcholine- ophthalmic effects
So what will acetylcholine (i.v.) do to blood pressure?
• Raise it
• Nothing
• Lower it
Choline esters• Bethanecol (Bethanecol, Duvoid, Myotomachol, Urecholine injection)– resistant to metabolism– selective for GI and urinary bladder after oral administration (10 to 50 mg 3 to 4/day)
– therapeutic uses - to contract gut or urinary bladder
• Administration of choline esters - oral, sub. cut., intraocular
• Contraindication and toxicity of choline esters - coronary insufficiency (lower diastolic pressure) – [also asthma (bronchoconstriction), hyperthyroidism, peptic ulcer (increase acid secretion)]
Cholinomimetic alkaloids
•Pilocarpine (Pilocar opthalmic solutions; Selagen)– predominantly muscarinic actions, so actions are those of parasympathetic stimulation
– [used to treat glaucoma or xerostomia (dry mouth)]
•Muscarine almost purely muscarinic; derived from mushrooms; parasympathetic actions
ANTICHOLINESTERASE AGENTS
• Acetylcholinesterase
•Two types - acetylcholinesterase and butyrocholinesterase
•Acetylcholinesterase is a tetramer with molecular weight of 320,000 (has an anionic site & is a serine esterase)
Anticholinesterases
•useful in treating glaucoma, myasthenia gravis and atropine poisoning; they potentiate skeletal muscle contraction (nicotinic receptors) and muscarinic effects– Reversible– Irreversible - organophosphorous compound
Effects• Those of parasympathetic stimulation because they increase acetylcholine concentrations outside the nerve (i.e., in the vicinity of the muscarinic receptor)- bradycardia and vasodilation
• Neuromuscular junction - contract skeletal muscle (nicotinic) because they increase acetylcholine concentrations in the vicinity of the nicotinic receptor (i.e., outside the somatic nerve)
• Ganglia - can activate postganglionic nerve (nicotinic) by increasing acetylcholine concentrations in the synapse - less likely to occur
Mechanism of action of anticholinesterases•Bind to active site (edrophonium)
•Organophosphorous compounds serve as hemisubstrates (irreversible)
•Carbamyl esters are acted on slowly
Cardiovascular Use
• paroxysmal atrial tachycardia• ATROPINE intoxication
Specific Anticholinesterases
Carbamates (reversible)
– Physostigmine (Antilirium injectable)» Parenteral (2 mg i.m.) or ophthalmic administration
» Used for poisoning with anticholinergics (like ATROPINE)
Other reversible inhibitors
– Edrophonium (Tensilon injectable)-potential use in paroxysmal supraventricular tachycardia
Toxicology of Anticholinesterases• Symptoms of cholinergic crisis
– muscarinic - sweating, salivation, lacrimation, bradycardia, hypotension, blurred vision
– nicotinic - muscle fasciculation, hypertension, tachycardia
– CNS - restlessness, insomnia, tremors, confusion, ataxia, convulsions, circulatory collapse
• Diagnosis- cholinesterase activity of red blood cell
• Treatment– ATROPINE (muscarinic receptor antagonist; 2 to 6 mg parenterally)- reverses only muscarinic symptoms
– pralidoxime for organophosphorous inhibitors (1 to 2 g i.v.; can be given i.m.)
ANTIMUSCARINIC AGENTS
• Naturally occurring alkaloids - ATROPINE, scopolamine
• Actions are to oppose parasympathetic effects to slow heart rate, so they elevate heart rate– They are competitive antagonists of muscarinic receptors
– ATROPINE affects: salivary, bronchial, sweating > cardiac vagal effects > urinary, GI tract > gastric secretion
• Absorption and Excretion - well absorbed, excreted in urine
Toxicity of Atropine
•Symptoms - dry mouth, blurred vision, hyperthermia, tachycardia, hot dry skin, delirium, coma, respiratory paralysis
•Treatment - physostigmine (1 mg i.v.)
Therapeutic Uses of Atropine
• Cardiovascular system (to treat):– Choline-ester toxicity– Hyperactive carotid sinus reflex
– Bradycardia– AV block
Specific Antimuscarinics
• Natural alkaloids
– ATROPINE (antispasmotic capsules, Antrocol, atropine, etc.)
» a. increase heart rate (500 to 1000 µg, i.v.)
» b. treatment for toxicity to choline esters, anticholinesterases or mushrooms
What will atropine do to hypotension caused by
bradycardia• Raise blood pressure
• No effect
• Lower blood pressure