autologous transfusions: when to use ‘em & when to lose ‘em christopher j. gresens, md...
TRANSCRIPT
Autologous Transfusions: When to Use ‘em & When to
Lose ‘em
Christopher J. Gresens, MD
Associate Medical Director
BloodSource
Preview
• Types of Autologous Donations/Transfusions– Preoperative– Perioperative (e.g., intra- and postoperative)– Acute Normovolemic Hemodilution
• Gann Act• Marshall-BloodSource Experience• Pros/Cons of Autologous Blood• Wrap up
Overview of Autologous Options
• Before Surgery– Preoperative collection
• During Surgery– Intraoperative blood salvage
• After Surgery– Postoperative blood salvage
• Acute Normovolemic Hemodilution
Preoperative Autologous Collection
• Donated before surgery• “Target” usually is RBCs• Eligibility criteria relaxed• Minimum Hct 33%• No absolute minimum age• No weight limits• Increased donation frequency
Preop Auto Blood--Contraindications
• Significant cardiac abnormalities (e.g., aortic stenosis, severe CAD or CHF)
• Very recent MI or CVA • Potential bacteremia• Hematocrit < 33%• Surgery <72 hours from time of
donation
Preop Auto Blood--Risks
• Development of anemia due to donation process (see Kanter et al)
• Small risk of septic & several other transfusion reactions
• Remote risk of wrong unit being transfused
• Blood may not be immediately available in an emergency
Preop Auto Blood--Other Issues
• Venous access• Iron supplementation• Special handling• Fees• Unused autologous
units destroyed
Preop Auto Blood--Other Issues• Crossover to allogeneic supply—Virtually never done• Frozen autologous blood—To be discouraged, except
when strong clinical indication exists• Transfusion criteria for autologous blood are sometimes
debated (should they be same as/different from allo?)• Local hospitals have varying policies regarding the use of
confirmed HBV- and HIV-infected units (ADA Act)• Certain patient populations (e.g., elective hysterectomy
patients) generally should not give autologous blood • Cost-effectiveness—May never by cost-effective, per
traditionally utilized criteria.
Preop Auto Blood--Other Issues• The ADA, HIV, & Autologous Blood Donations• Supreme Court’s Bragdon vs. Abbott Decision: HIV+
patient (A) successfully sued dentist (B) for refusing to fill his cavity anywhere other than in a hospital.
• “Extrapolated” Opinion of AABB’s Lawyers: “Bragdon may render unlawful those policies that deny HIV-infected patients the opportunity to use their own blood. Blood centers and hospitals that have such policies or procedures should, with the assistance of counsel, consider carefully whether they can defend their actions successfully given the sweep of the Bragdon decision and the ADA’s prohibitions.”
Preop Auto Blood--Other Issues
• Preop Auto Blood Donations Before Elective Hyster-ectomy. M.H. Kanter et al. JAMA. 1996; 276: 798-801.
• Design: Retrospective; compared 140 elective hyster-ectomy patients who gave auto blood with 123 who didn’t.
• Results: 25 of 140 auto donors were transfused (3 with allo RBCs); 1 of the other 123 was transfused (p < 0.001).
• Conclusion: “For hysterectomy patients, donation of autologous blood causes anemia and is associated with a more liberal transfusion policy. Elimination of preoperative autologous donation for these patients should not result in frequent exposure to allogeneic blood”
Autologous Blood Transfusions in Total Joint Replacement
Surgery:The Marshall
Hospital/BloodSource Experience
C. Gresens et al. Transfusion 2002; 42 (Suppl): 18S-19S.
Marshall Hospital/BloodSource Total Joint Replacement Surgery
Blood Use Study
• Background: Many orthopedic surgeons advise their TJR surgery patients to consider making preoperative autologous blood donations (PABDs) to reduce the need for perioperative allogeneic transfusions.
• We recently examined the blood transfusion use of such patients to understand better the impact of PABDs on perioperative transfusion requirements.
Marshall Hospital/BloodSource TJR Surgery Blood Use Study
• Methods: Retrospective review of primary, one-joint TJR surgery patient charts (at Marshall Hospital) and autologous donor charts (at BloodSource).
• Blood volume estimated as: Patient mass (kg) x 0.069 L/kg (male) or 0.065 L/kg (female).
• Autologous blood was transfused as pRBCs.• Perioperative blood salvage was not used.• Criteria for transfusion of autologous and allogeneic blood
were identical.
Marshall Hospital/BloodSource TJR Surgery Blood Use Study
• Results• Date Range: July 2000-March, 2001• N = 43 (19 male; 24 female)• Surgical Procedures: Primary, unilateral joint
replacement surgeries:– Knee--29 (67%); Hip--14 (33%)
• Ages of Patients: Mean = 67.1 (45-86 years)
Marshall Hospital/BloodSource TJR Surgery Blood Use Study
• Twenty-four patients (57%) made PABDs:– 17 (71%) were knee surgery patients– 7 (29%) were hip surgery patients
• PABD Profile– Mean # of PABDs = 1.9 (1-2) units– In total, 45 PABDs were made by these 24 patients.
Marshall Hospital/BloodSource TJR Surgery Blood Use Study
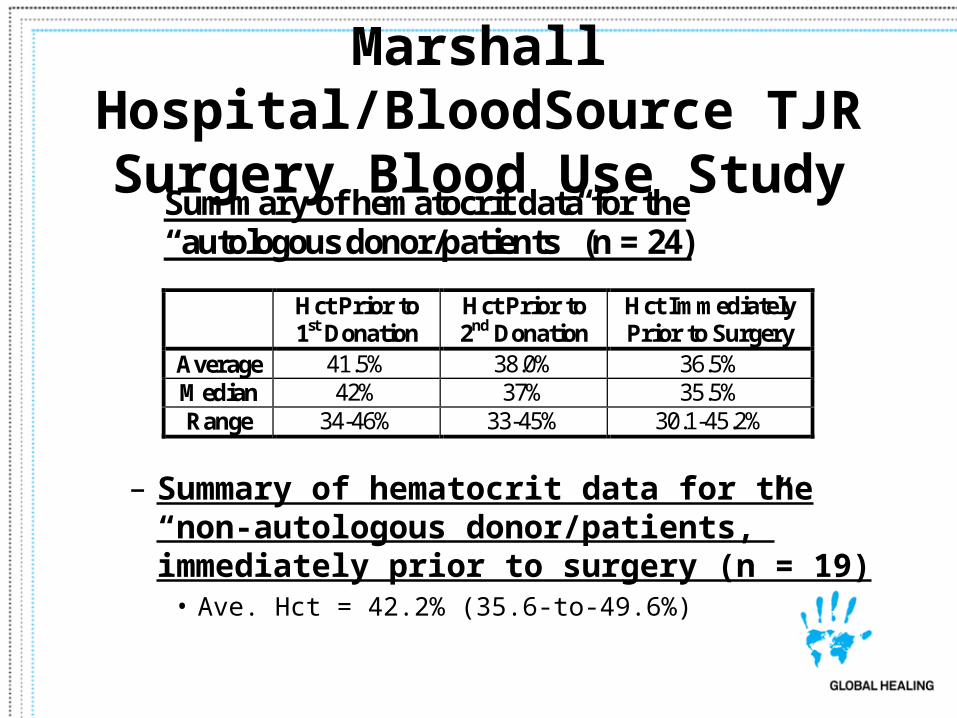
– Summary of hematocrit data for the “non-autologous donor/patients,” immediately prior to surgery (n = 19)
• Ave. Hct = 42.2% (35.6-to-49.6%)
Summary of hematocrit data for the “autologous donor/patients” (n = 24)
Hct Prior to
1st Donation Hct Prior to 2nd Donation
Hct Immediately Prior to Surgery
Average 41.5% 38.0% 36.5% Median 42% 37% 35.5% Range 34-46% 33-45% 30.1-45.2%
Marshall Hospital/BloodSource TJR Surgery Blood Use Study
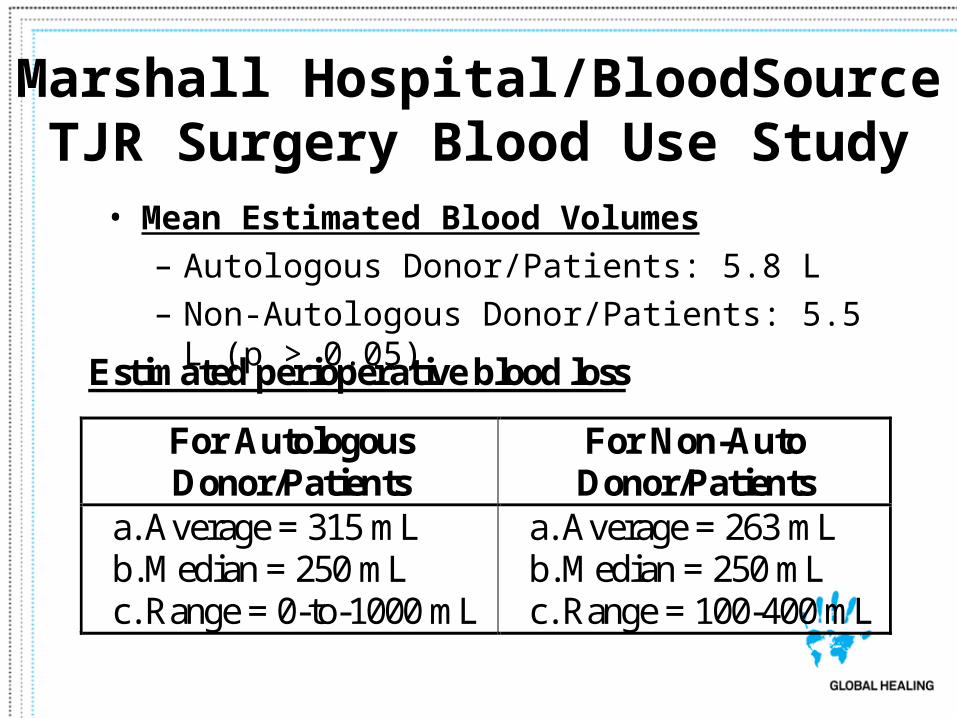
• Mean Estimated Blood Volumes– Autologous Donor/Patients: 5.8 L– Non-Autologous Donor/Patients: 5.5 L (p > 0.05)
Estimated perioperative blood loss
For Autologous Donor/Patients
For Non-Auto Donor/Patients
a. Average = 315 mL b. Median = 250 mL c. Range = 0-to-1000 mL
a. Average = 263 mL b. Median = 250 mL c. Range = 100-400 mL
Marshall Hospital/BloodSource TJR Surgery Blood Use Study
• Nine of the 24 autologous donor/patients (39%) required perioperative autologous RBC transfusions– Mean = 1.9; Median = 2; Range = 1-2 units;– Five (56%) were knee and 4 (44%) were hip;– 17 total auto units transfused.
• Only one of the 19 non-auto donor/patients (5%) required a single allogeneic RBC transfusion (p < 0.05).
Marshall Hospital/BloodSource TJR Surgery Blood Use Study
• Conclusions:• PABDs prior to TJR surgery were associated with:
– A moderate reduction in patient hematocrits;– A large increase in perioperative transfusions;– 62% of PABDs not transfused.
• PABDs no longer are routinely recommended for primary, one-joint TJR surgery patients at Marshall Hospital.
Preop Auto Blood--Other Issues• The Cost Effectiveness of Preoperative
Autologous Blood Donations. J Etchason, L Petz, et al. NEJM. 1995; 332: 719-724.
• Design: Decision-analysis model for cost effectiveness assessment (based upon 1992, UCLA data); looked at THR, CABG, abdom. hysterectomy, & TURP patients.
• Results: “The cost-effectiveness values ranged from $235,000 to over $23 million per quality-adjusted year of life saved.”
• Conclusion: “The increased protection afforded by donat-ing autologous blood … may not justify the increased cost.
Intraoperative Blood Salvage• Collection and re-infusion of
blood lost during surgery• Alternative to pre-operative
collection• Can be especially useful for
massively bleeding patients• Semi-automated systems
are available for this purpose
Intraop Blood--Considerations• Washed vs. unwashed• Guaranteed blood
compatibility• Up to 50% of RBCs
(sometimes more) are lost
• May be acceptable to Jehovah’s Witnesses (particularly if the collection/reinfusion circuit is circular)
Intraop Blood--Contraindications
• Infection/contamination of surgical field
• Cancer involving surgical field
Post-operative Blood Salvage
• Cardiac & Orthopedic surgical patients
• Blood collected from drainage devices
• Defibrinogenated• Unwashed• Can only be stored for
up to 6 hours at room temperature
Post-operative Blood Salvage• Red Cell Loss Following Orthopedic Surgery:
The Case Against Postoperative Blood Salvage. J. Umlas et al. Transfusion. 1994; 34: 402-406.
• Design: The volume of salvaged RBCs was measured for the 1st 6 hours postop & compared to total RBC loss and volume of allogeneic RBCs transfused.
• Results: Mean postop RBC losses in 31 THR & 20 TKR patients were 55 + 29 and 121 + 50 mL, respectively.
• Conclusion: “The relatively small red cell loss in the postoperative period in most arthroplasty patients does not appear to justify the routine use of this technique.”
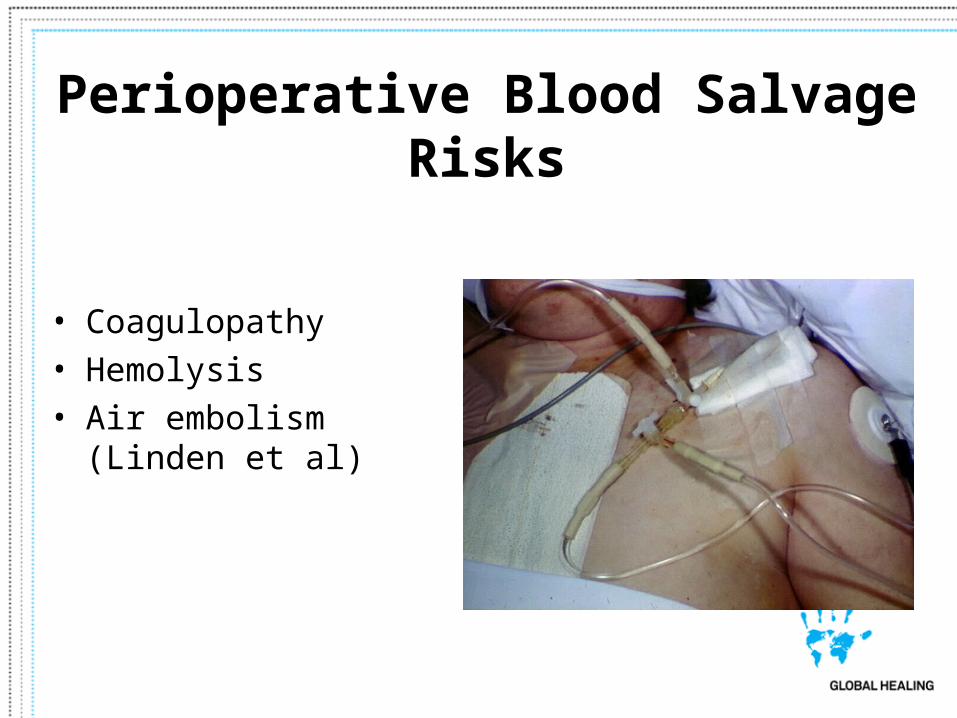
Perioperative Blood Salvage Risks
• Coagulopathy• Hemolysis• Air embolism (Linden
et al)
Perioperative Blood Salvage Risks• Fatal Air Embolism Due to Perioperative Blood
Recovery. J.V. Linden et al. Anesth Analg. 1997; 84: 422-426.
• Design: Retrospective review of 127,586 periop blood salvage procedures (PBSPs) and 8,955,619 conventional transfusions(CTs); 1990-1995.
• Results: 4 fatal air embolism cases occurred in associ-ation with PBSPs (1 in 30,000-38,000); none with CTs.
• Conclusion: Even when considering all the other risks associated with CTs, the risk for a fatal complication during PBSP is far higher than that for CTs.
Acute Normovolemic Hemodilution• ANH involves collecting blood from a
patient in the OR at the start of surgery, for re-infusion later in the surgery or during the immediate postoperative period.
• > 4 units may be removed (with simultaneous 3:1 crystalloid or 1:1 albumin replacement).
• In properly selected and monitored patients, a target Hct of 20-25% may be acceptable.
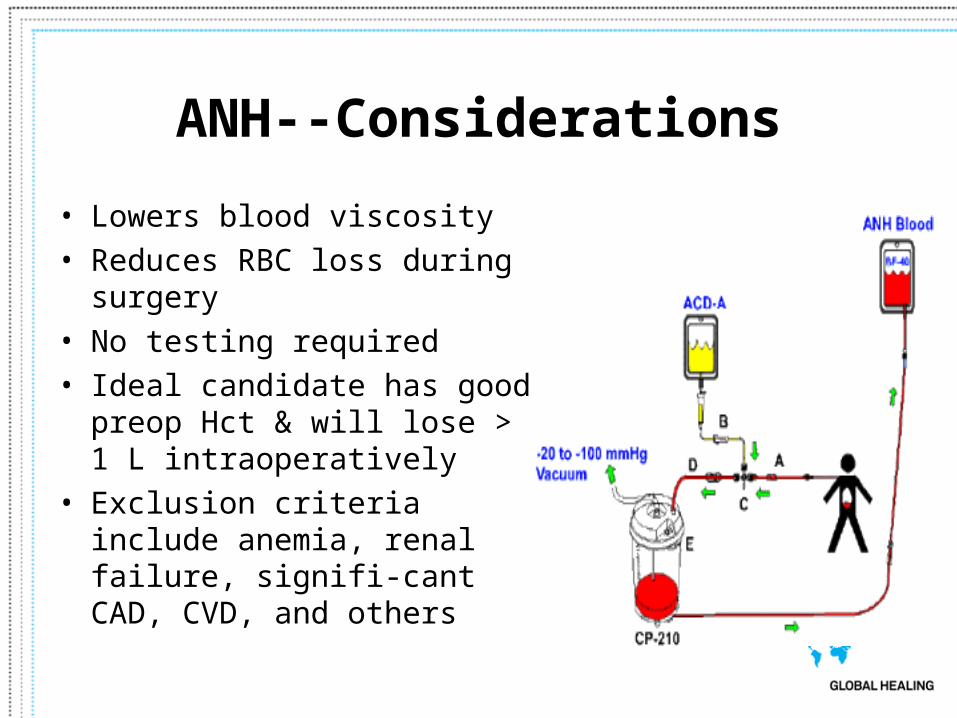
ANH--Considerations
• Lowers blood viscosity• Reduces RBC loss during
surgery• No testing required• Ideal candidate has good
preop Hct & will lose > 1 L intraoperatively
• Exclusion criteria include anemia, renal failure, signifi-cant CAD, CVD, and others
ANH--Risks
• Critical organ ischemia• Dilutes circulating
coagulation factors
Paul Gann Blood Safety Act
California Health and Safety Code, Section 1645
“Whenever there is a reasonable possibility, as determined by a physician and surgeon, that a blood
transfusion may be necessary as a result of medical or surgical procedure, the physician and surgeon, by means of a standardized written summary … shall
inform the patient of the positive and negative aspects of receiving autologous blood and directed and non-
directed homologous blood from volunteers.”
Paul Gann Blood Safety Act
• What constitutes a “reasonable possibility” (“that a blood transfusion may be necessary”)?
– T + C (i.e., Type + Cross) equals Gann Act– T + S (i.e., Type + Screen) does not equal Gann Act
Paul Gann Blood Safety Act
• The Gann Act does not apply “when medical contraindications or a life-threatening emergency exists.”
Pros and Cons for Auto/Allo Blood Benefits
Allogeneic Autologous
Available 24/7 Your own blood
Fully tested Fully tested (sometimes we even identify
heretofore unknown infections)
Completely compatible (if correct unit is used)
Pros and Cons for Auto/Allo Blood Risks
Allogeneic Autologous
Infection Infection (? Less risk)
Immune reactions Remote risk of incompatibility or allergic/anaphylactic (if wrong
unit or synthetic allergen introduced)
Circulatory overload, Same
citrate toxicity, etc.
Mild anemia
Not often available for emergency
Pros and Cons for Auto/Allo Blood
• One more “risk” of autologous blood:
» Cost
Conclusion• Types of Autologous
Donations/Transfusions– Preoperative– Perioperative– Acute Normovolemic
Hemodilution• Gann Act• Marshall-BloodSource
Experience• Pros/Cons of Autologous Blood