(atopic dermatitis) - dcareusa.com · pimecrolimus are favoured over topi - ... (atopic dermatitis)...
TRANSCRIPT
Atop ic dermat i t i s (AD) i s a chronic inf lammator y sk in d i sease which commonly begins in ear ly infancy and i s accompanied by intense pru-r i tus . Loss-of-func t ion mutat ions of the F i laggr in gene are detec ted in 15-50% of pat ient s wi th AD, lead-ing to a def ic iency of the sk in bar r ie r func t ion. A h igh propor t ion of AD pat ient s i s co lonized wi th S . aureus . Numerous t r igger fac tor s have been ident i f ied for AD over the las t dec-ades , such as inhalat i ve and food a l le rgens , i r r i t at i ve subs tances , psy-cho logica l s t ress , and infec t ious microorganisms l ike Staphy lococcus aureus and Malassez ia. Moreover, contac t a l le rgy e.g. to ingred ient s of emol l ient s , ex ternal drugs , and occu-pat ional a l le rgens may compl icate AD. The ident i f i cat ion and, whenever poss ib le, the avo idance of ind iv idual t r igger fac tor s i s the bas i s of long-term management of AD.
S ince AD i s assoc iated wi th sk in bar-r ie r abnormal i t ies a l so in nonle -s ional sk in, emol l ient s should be app l ied cont inuous ly to the whole body sur face. Ant i - inf lammator y top -ica l agent s are used for les ional sk in only. Accord ing to cur rent gu ide l ines and pos i t ion paper s , top ica l g luco -cor t icos tero ids are s t i l l a f i r s t- l ine ant i - inf lammator y t reatment which i s used on an as-needed-bas i s . A con-sequent base l ine emol l ient care com-b ined wi th ear ly ant i - inf lammator y t reatment he lps to prevent severe f lares and to spare s tero ids . In body areas prone to sk in at rophy such as the face, the geni ta l area, the ax i l -lar and inguina l fo lds and for long-term management , the top ica l ca l -c ineur in inh ib i tor s tacro l imus and p imecro l imus are favoured over top i -ca l cor t icos tero ids . There are no pre -c l in ica l or c l in ica l data ind icat ing an increased r i sk of l ymphoma or pho-tocarc inogenic i t y for top ica l ca l -c ineur in inh ib i tor s yet . However, accord ing to gu ide l ines and pos i -
t ion paper s , UV protec t ion e.g. wi th sunscreens i s recommended. Both top ica l ca lc ineur in inh ib i tor s are approved in the EU for use in adul t s and ch i ldren f rom 2 year s and above.
The s t rategy of “proac t i ve” ant i -inf lammator y therapy of AD has been eva luated in severa l c l in ica l s tud-ies in recent year s . The t reatment i s s tar ted wi th a more intense use of top ica l ant i - inf lammator y drugs such as g lucocor t icos tero ids or ca lc ineu-r in inh ib i tor s unt i l the les ions have c leared. Thereaf ter, t reatment i s con-t inued wi th intermit tent app l icat ion of ant i - inf lammator y agent s on pre -v ious ly inf lamed sk in areas . In most t r ia l s , top ica l s tero ids or tacro l imus were app l ied twice week ly, and pro -ac t i ve therapy resu l ted in s ign i f i -cant ly less exacerbat ions of AD and increased the t ime unt i l f i r s t re lapse. S ince S . aureus der i ved tox ins may t r igger eczema, pat ient s wi th a h igh dens i t y of co lonizat ion may bene -f i t f rom a temporar y use of top ica l ant i sept ic s l ike t r i c losan or ch lorhex-id ine. In pat ient s wi th head-neck-shoulder dermat i t i s malassez ia spe -c ies may p lay a ro le as exacerbat-ing fac tor and sys temic ketoconazo le and top ica l c ic lop i roxo lamine have demonstrated s ign i f i cant improve -ment.
For pat ient s wi th moderate or severe AD phototherapy may be added to the top ica l t reatment . Medium UVA1 has recent ly been shown to have a s imi lar ef f i cacy as nar row band UVB therapy in AD.
Sys temic ant i - inf lammator y therapy i s app l ied in pat ient s wi th severe AD res i s tant to top ica l therapy. Due to potent ia l s ide ef fec t s , ora l cor t icos-tero ids should not be g iven longer than a few week s . Cyc lospor ine i s approved for the t reatment of AD in many EU countr ies , whereas aza-th iopr in, mycophenolate mof t i l and
Therapy of Neurodermatitis (Atopic dermatitis)
EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
A media service of the European Academy of Dermatology & Venereology - No. 9 / 2010
Media InfoSheet Media InfoSheet
In This Issue
Therapy of Neurodermatitis 1-2
Hair loss and the dermatological treatment options 2-3
Blood Platelet Concentrate.....a breakthrough therapy inregenerative medicine 4
Announcement: Future EADV Meetings 5
Page 2 Info Sheet no 9
Therapy of Neurodermatitis
methotrexat have been shown to be ef fec t i ve in case repor t s and smal ler t r ia l s on ly and are not approved for AD yet . Conf l i c t ing resu l t s have been repor ted for the ant i - IgE ant ibody omal izumab, which i s approved as addi t ional therapy in severe reca lc i t rant a l le rg ic as thma, poss ib ly due to d i f-ferences in pat ient sever i t y and IgE leve l s . Ant i -TNF ant ibodies , approved as seond- l ine t reatment of moderate to severe psor ias i s , showed benef ic ia l ef fec t s in p i lot s tud ies , but large randomized, p la -cebo contro l led s tud ies are s t i l l miss ing. A l le rgen-speci f i c immunotherapy (S IT ) improved AD in sev-era l case repor t s and smal l t r ia l s but larger s tud ies have not been pub l i shed yet . Therefore, S IT should be l imi ted to AD pat ient s wi th concomitant a l le rg ic rh in i t i s or mi ld as thma.In las t year s educat ion programmes for pat ient s
and parent s invo lv ing dermato logis t s , paediat r i -c ians , psychologis t s , and d ietar y counse l lor s have been es tab l i shed. These programmes have been shown to be ef f i c ient in terms of d i sease symp-toms and qual i t y of l i fe and par t ic ipat ion should be encouraged.
Volker Ste inkraus, Kr ist ian Reich, Kr ist ine BreuerStephansp lat z 5D - 20354 HamburgTe l + 49 40 351075 0Fax + 49 40 351075 10E-mai l : breuer@dermato logikum.de (cor responding author)
A lmost ever ybody dur ing l i fet ime exper iences a cer ta in t ype of ha i r loss , ranging f rom an acute te logen ef f luv ium af ter a phys ica l s t ress , such as a crash d iet , to the common androgenet ic a lopecia. Bes ide sever i t y and durat ion, ha i r loss may cause severe emot ional d i s t ress: anx iet y and low se l f-es teem are common compla ins of pat ient s wi th ha i r loss prob lems.
Th is exp la ins why the market of ha i r produc t s i s cont inuous ly increas ing. Hundreds of compounds, which are so ld on Internet , in pharmacies , in nat-
ura l shops… cla im to increase ha i r grow th. The tendency to se l f-admin is ter a cure i s w idespread among pat ient s wi th ha i r loss , lead ing to poor resu l t s and cons iderab le f rus t rat ion.
There are severa l ev idence -based t reatment s that can prov ide improvement or cure of the most common forms of ha i r loss , but they should be prescr ibed and admin is tered in the opt imal way by a t ra ined dermato logis t . The f i r s t s tep for cor rec t management of a lopecia i s in fac t a cor rec t d iag-nos i s , which can be made only by a dermato logis t .
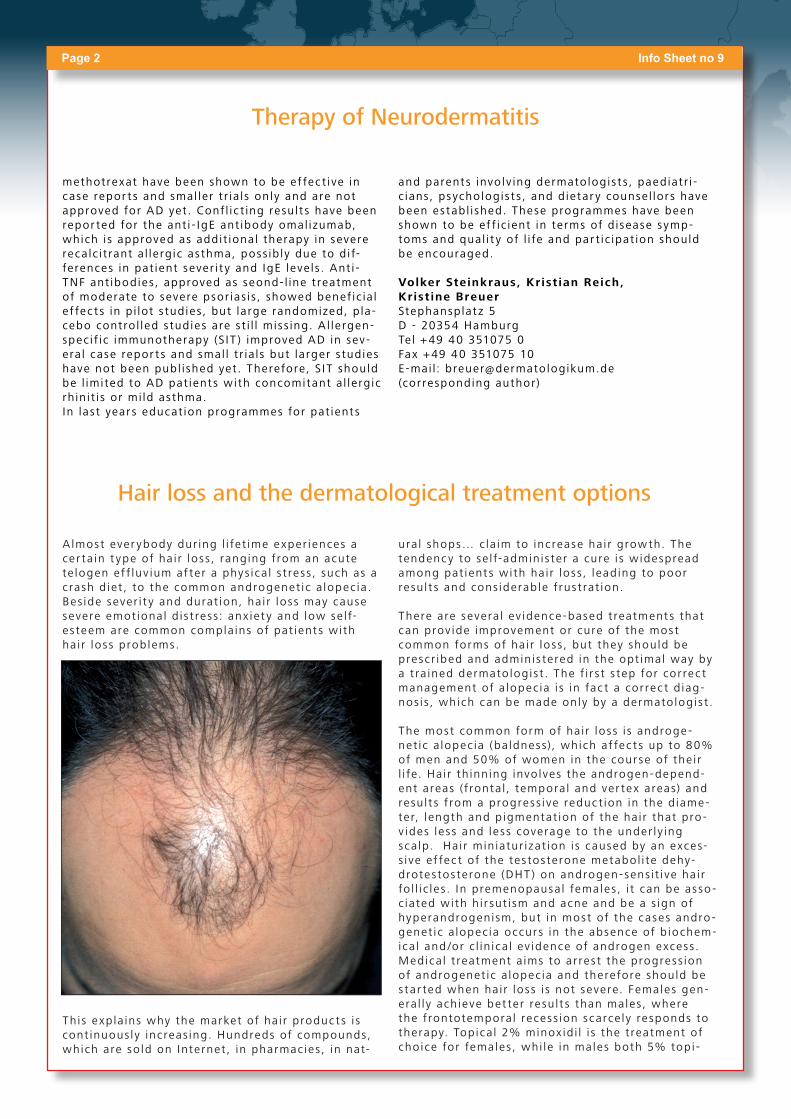
The most common form of ha i r loss i s androge -net ic a lopecia (ba ldness), which af fec t s up to 80% of men and 50% of women in the cour se of the i r l i fe. Hai r th inn ing invo lves the androgen-depend-ent areas ( f ronta l , tempora l and ver tex areas) and resu l t s f rom a progress ive reduc t ion in the d iame-ter, length and p igmentat ion of the ha i r that pro -v ides less and less coverage to the under ly ing sca lp. Hai r min iatur izat ion i s caused by an exces-s i ve ef fec t of the tes tos terone metabol i te dehy-drotes tos terone (DHT ) on androgen-sens i t i ve ha i r fo l l i c les . In premenopausal females , i t can be asso -c iated wi th h i r sut i sm and acne and be a s ign of hyperandrogenism, but in most of the cases andro -genet ic a lopecia occur s in the absence of b iochem-ica l and /or c l in ica l ev idence of androgen excess . Medica l t reatment a ims to ar res t the progress ion of androgenet ic a lopecia and therefore should be s tar ted when hai r loss i s not severe. Females gen-era l l y ach ieve bet ter resu l t s than males , where the f rontotempora l recess ion scarce ly responds to therapy. Top ica l 2% minox id i l i s the t reatment of cho ice for females , whi le in males both 5% top i -
Hair loss and the dermatological treatment options
Info Sheet no 9 Page 3
ca l minox id i l and ora l f inas ter ide 1 mg are poss i -b le opt ions . C l in ica l improvement i s most ly due to th ickening of the preex i s t ing ha i r and occur s af ter at leas t 6 months of t reatment . Therapy should never be d i scont inued to mainta in ef f i cacy.
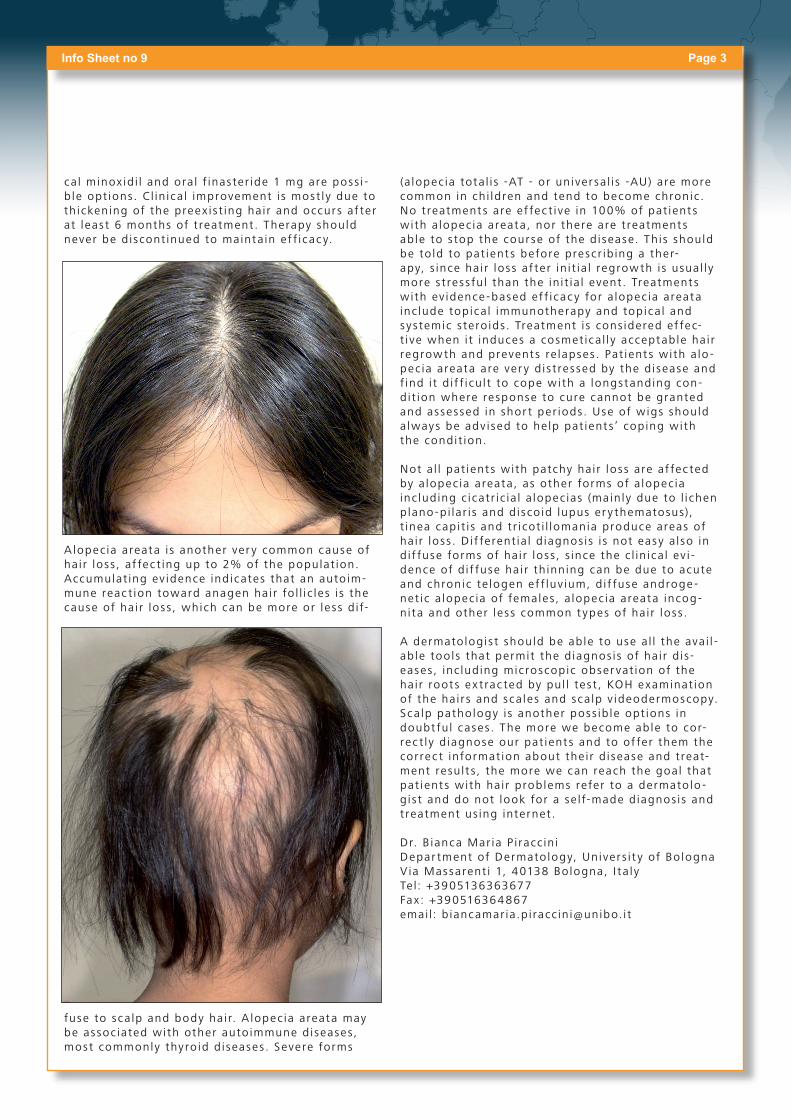
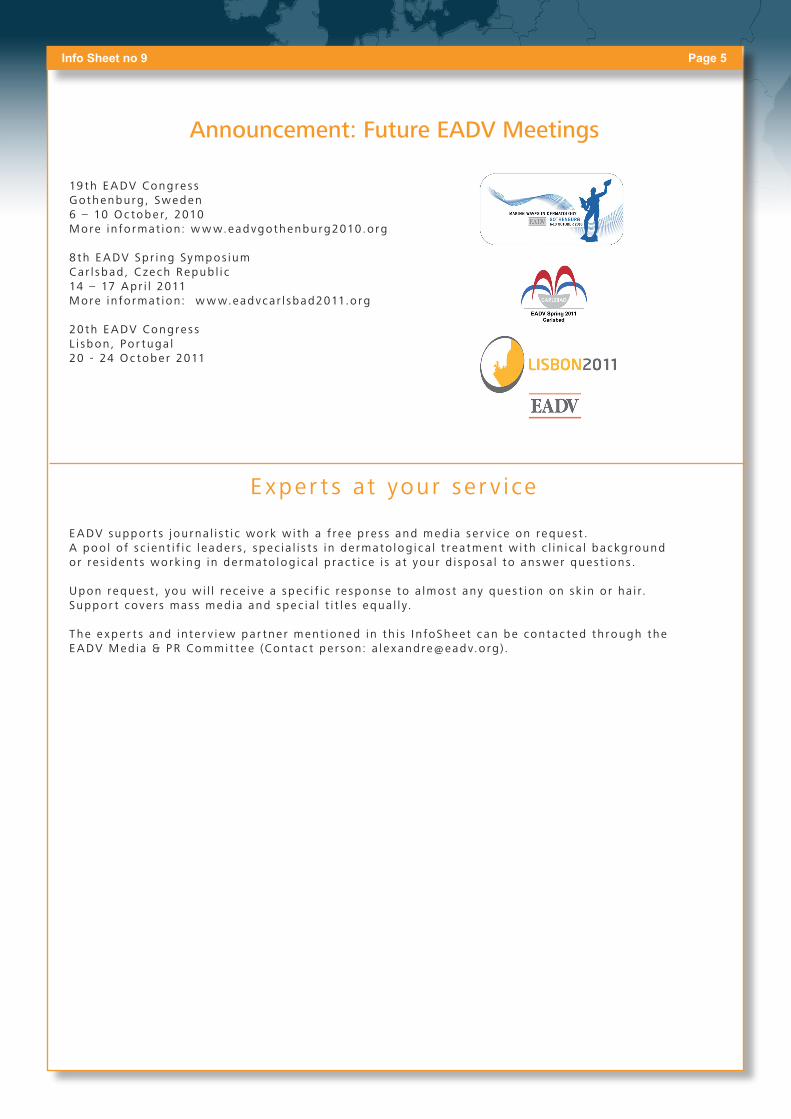
A lopecia areata i s another ver y common cause of ha i r loss , af fec t ing up to 2% of the populat ion. Accumulat ing ev idence ind icates that an auto im-mune reac t ion toward anagen hai r fo l l i c les i s the cause of ha i r loss , which can be more or less d i f-
fuse to sca lp and body hai r. A lopecia areata may be assoc iated wi th other auto immune d iseases , most commonly thy ro id d i seases . Severe forms
(a lopecia tota l i s -AT - or un iver sa l i s -AU) are more common in ch i ldren and tend to become chronic. No t reatment s are ef fec t i ve in 100% of pat ient s wi th a lopecia areata, nor there are t reatment s ab le to s top the cour se of the d i sease. Th is should be to ld to pat ient s before prescr ib ing a ther-apy, s ince ha i r loss af ter in i t ia l regrow th i s usual l y more s t ress fu l than the in i t ia l event . Treatment s wi th ev idence -based ef f i cacy for a lopecia areata inc lude top ica l immunotherapy and top ica l and sys temic s tero ids . Treatment i s cons idered ef fec-t i ve when i t induces a cosmet ica l l y acceptab le ha i r regrow th and prevent s re lapses . Pat ient s wi th a lo -pec ia areata are ver y d i s t ressed by the d i sease and f ind i t d i f f i cu l t to cope wi th a longs tanding con-d i t ion where response to cure cannot be granted and assessed in shor t per iods . Use of wigs should a lways be adv ised to he lp pat ient s’ cop ing wi th the condi t ion.
Not a l l pat ient s wi th patchy ha i r loss are af fec ted by a lopecia areata, as other forms of a lopecia inc lud ing c icat r ic ia l a lopecias (main ly due to l i chen p lano-p i lar i s and d i sco id lupus er y thematosus), t inea cap i t i s and t r i cot i l lomania produce areas of ha i r loss . D i f ferent ia l d iagnos is i s not easy a l so in d i f fuse forms of ha i r loss , s ince the c l in ica l ev i -dence of d i f fuse ha i r th inn ing can be due to acute and chronic te logen ef f luv ium, d i f fuse androge -net ic a lopecia of females , a lopecia areata incog-n i ta and other less common t ypes of ha i r loss .
A dermato logis t should be ab le to use a l l the ava i l -ab le too ls that permit the d iagnos i s of ha i r d i s-eases , inc lud ing microscop ic obser vat ion of the ha i r root s ex t rac ted by pu l l tes t , KOH examinat ion of the ha i r s and sca les and sca lp v ideodermoscopy. Sca lp patho logy i s another poss ib le opt ions in doubt fu l cases . The more we become ab le to cor-rec t l y d iagnose our pat ient s and to of fer them the cor rec t informat ion about the i r d i sease and t reat-ment resu l t s , the more we can reach the goal that pat ient s wi th ha i r prob lems refer to a dermato lo -g i s t and do not look for a se l f-made d iagnos is and t reatment us ing internet .
Dr. B ianca Mar ia P i racc in iDepar tment of Dermato logy, Univer s i t y of Bo lognaV ia Massarent i 1, 40138 Bo logna, I t a lyTe l: +3905136363677Fax: +390516364867emai l : b iancamar ia.p i racc in i@unibo. i t

Page 4 Info Sheet no 9
Blood Platelet Concentrate.....a breakthrough therapy in regenerative medicine
Numerous clinical studies in vari-ous medical disciplines have sup-ported the efficacy of regen-erative therapies. Regenerative medicine describes innovative and new therapies to support and accelerate the healing and tissue regeneration process.
Platelet Rich Plasma (PRP) has played a prominent role and has been proven as a safe and effi-cient treatment option for a number of medical conditions. PRP describes a high concen-tration of platelets in a small volume of plasma. It is an autol-ogous treatment, which means that the patient acts as own source for the injected sub-stance.
The concentration of the plasma is enabled by a gel within the tube in which the blood has been drawn. During the short five minute spinning cycle, the gel effectively separates the platelets and leucocytes from the erythrocytes.
Platelet Concentrate was first explored in dental and oral maxillofacial surgery to accelerate the healing post per-iodontal surgery or aesthetic dental implant reconstruc-tion. PRP has also been found effective to treat indica-tions in the field of sports medicine. The platelet concen-trate is hereby injected along the defect tendons or lig-aments. The injected platelets release a variety of differ-ent growth factors that initiate and control the healing process. A high concentration of growth factors acceler-ates the natural healing process significantly. In the past, there was a controversy if the use of PRP was infring-ing doping regulations. Golf pro Tiger Woods, along with other famous American Football and Baseball players, confessed to have undergone PRP treatment. After more and more studies were published, supporting the use of PRP in sports medicine, it was finally declared as legal in January 2010. Now PRP has also become a popular treat-ment option for team physicians of various professional soccer clubs, to have their players recover faster after injuries.
In Dermatology, PRP has been used for years to treat dif-ficult to treat wounds. Hereby the platelet concentrate is mixed with an activating solution, that turns the liquid PRP to a sticky and formable membrane which then can be topically applied on the wound. A number of pub-lished clinical studies have shown that PRP can signifi-cantly improve the healing.
Platelet Rich Plasma has also become a revolutionary and popular new treatment to treat signs of skin ageing like fine lines and wrinkles, skin laxity as well as dry skin. The treatment, which has also been titled in the press as “Dracula therapy”, is designed for patients that are look-ing for a natural treatment supporting the body´s own rejuvenation potential instead of using substances like Hyaloronic Acid or Botolinum Toxin.
The patient acceptance is superior to most other aes-thetic treatments. The spectrum of indications is broad, PRP can be used to treat fine lines and wrinkles, it improves the texture of skin and can be applied on hands, cheeks, forehead or around the eyes.
By injecting a high concentration of platelets into the dermis, the natural tissue healing process is being signif-icantly accelerated and the production of collagen initi-ated. Platelet Rich Plasma can be applied as liquid con-centrate as Mesotherapy or mixed with an autologous activating solution (autologous serum thrombin) that turns the liquid to a gel-like substance, to be used as a volumetric filler.
Harnessing the proven wound healing potential of PRP, PRP can also effectively reduce the down time after aes-thetic treatments like laser or peelings and can avoid the risk of post inflammatory hyperpigmentation. Hereby the platelet concentrate is mixed with a crème, especially designed to calm and nourish the skin after a treatment. The cellular mask is applied directly after the aesthetic treatment for 30-45 minutes. The mask reduces the risk of scarring and infection and is also comfortable for the patient.
Dr. Alain Gondinet6 Ruelle des Coins78770 ThoiryFranceTel. +33 1 34874793
Dr. Walter TrettelMönckebergstrasse 520095 HamburgTel. +49 40 35711122
Info Sheet no 9 Page 5
Announcement: Future EADV Meetings
19 th E A DV Congre s sG othenburg , Sweden6 – 10 Oc tobe r, 2010More i n fo rmat ion: w w w.eadvgothenburg2010.o rg
8 th E A DV Sp r ing Sy mpos iumC ar l sbad , C zech Repub l i c14 – 17 A p r i l 2011More i n fo rmat ion: w w w.eadvc a r l sbad2011.o rg
20 th E A DV Congre s sL i sbon , Po r tuga l20 - 24 Oc tobe r 2011
E xper t s at your ser v i ce E A DV suppor t s j ou rna l i s t i c work w i th a f ree p re s s and med ia s e r v i ce on reques t . A poo l o f s c i en t i f i c l eade r s , spec i a l i s t s i n de rmato log i c a l t rea tment w i th c l i n i c a l backg round o r re s i dent s work ing i n de rmato log i c a l p rac t i ce i s a t you r d i spos a l to ans wer que s t i ons .
Upon reques t , you w i l l r e ce i ve a spec i f i c re sponse to a lmos t any que s t i on on sk in o r ha i r.Suppor t cove r s mas s med ia and spec i a l t i t l e s equa l l y.
T he e xpe r t s and i n te r v i ew pa r tne r ment ioned i n th i s I n foShee t c an be cont ac ted th rough the E A DV Med ia & PR Commi t tee (Cont ac t pe r son: a l e xand [email protected] rg ) .
Page 7 Info Sheet 9
R e p l y F o r m
Please return to Alexandre Dewaide by e-mail ([email protected]) or by fax to the
following number: + 32 2650 00 98.
Yes, I would like more information on the contents of this issue :
EUROPEAN ACADEMY OF
DERMATOLOGY AND VENEREOLOGY /ACADEMIE EUROPEENNE DE
DERMATOLOGIE ET DE VENEREOLOGIE
A non profit association / Association sans but lucratif
EADV Info Sheet The EADV Info Sheet is a publication of the European Academy of Dermatology & Venereology
Editor: Dr. Colm O’MahonyTechnical Editor: Juliane PeterhanslCoordinator: Alexandre Dewaide
EADV (Headquarters)Via delle Scuole, 12CH- 6900 Lugano, Switzerland
EADV (Succursale belge)Avenue General de Gaulle, 38B- 1050 Brussels, Belgium
Website: www.eadv.org
Layout / Coordination content:ART.media Public RelationsJuliane PeterhanslStromstrasse 410555 Berlin – GermanyTel. +49 (0) 30 - 7 40 74 47 - [email protected]
Contact details
Name: ________________________________________________
Street: ______________________________________________
Post Code:___________ City:______________________________
Country:_______________________________________________
Tel: ________________________________________________ __
Fax:__________________________________________________
E-mail: _______________________________________________
Please send me a Press Release on: ______________________
Please send me a Fact Sheet on: ________________________
Please put me in direct contact with an EADV expert on:
________________________________________________
Further remarks
_________________________________________________
_________________________________________________
_________________________________________________
_________________________________________________