appraising iniparib, the parp inhibitor that never was—what must we learn?
TRANSCRIPT
688 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrclinonc
Drug Development Unit, Division of Cancer Therapeutics and Division of Clinical Studies, The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research, Downs Road, Sutton, Surrey SM2 5PT, UK (J. Mateo, M. Ong, D. S. P. Tan, M. A. Gonzalez, J. S. de Bono).
Correspondence to: J. S. de Bono johann.de-bono@ icr.ac.uk
Appraising iniparib, the PARP inhibitor that never was—what must we learn?Joaquin Mateo, Michael Ong, David S. P. Tan, Michael A. Gonzalez and Johann S. de Bono
Abstract | Several drugs targeting poly(ADP-ribose) polymerase (PARP) enzymes are under development. Responses have been observed in patients with germline mutations in BRCA1 and BRCA2, with further data supporting antitumour activity of PARP inhibitors in sporadic ovarian cancer. Strategies to identify other predictive biomarkers remain under investigation. Iniparib was purported to be a PARP inhibitor that showed promising results in randomized phase II trials in patients with triple-negative breast cancer. Negative results from a phase III study in this disease setting, however, tempered enthusiasm for this agent. Recently, data from in vitro experiments suggest that iniparib is not only structurally distinct from other described PARP inhibitors, but is also a poor inhibitor of PARP activity. In this context, the negative iniparib phase III data might have erroneously promulgated the notion that PARP inhibition is not an effective therapeutic strategy. Here, we scrutinize the development of iniparib from preclinical studies to registration trials, and identify and discuss the pitfalls in the development of anticancer drugs to prevent future late-stage trial failures.
Mateo, J. et al. Nat. Rev. Clin. Oncol. 10, 688–696 (2013); published online 15 October 2013; doi:10.1038/nrclinonc.2013.177
IntroductionOver the past 5 years, around 4,800 early phase clinical trials have been initiated in cancer medicine. During this period, more than 2,300 phase III studies were initiated. Sadly, the rate of failure in oncology for novel compounds undergoing clinical evaluation continues to be high compared with other medical specialties, such as cardio vascular diseases, and might even be rising with the advent of targeted therapies.1–3 Costs of drug development also continue to increase, and may now be more than US$3 billion per drug approved; moreover, the market narrows the room for new approvals,4 impacting the price of compounds when approved and jeopardizing the sustainability of health services.5,6 Failures in latephase registration clinical trials are especially disappoint ing, as they represent an enormous expenditure of money and time from pharmaceutical companies and academic institutions, and signify potential suffering of huge numbers of patients with advancedstage cancer and their families.
Why are promising results observed in preclinical research often not translated into clinical success? Several causes contribute to failures including: limited know ledge of cancer biology (despite ongoing and encouraging advances), selection of pharmacological compounds with suboptimal pharmacological properties, poorly predictive preclinical models, inappropriate trial designs, or decisionmaking based on nonrelevant end points.7–11
Iniparib (BiPar Sciences and Sanofi) is a compound that was initially developed as a poly(ADP–ribose)
polymerase (PARP) inhibitor, a class of drugs that impairs singlestranded DNA break repair. In general, PARP inhibitors have been useful in one of two strategies: first, ‘synthetic lethality’, capitalizing on the sensitivity of cells with defective homologousrecombination (HR)mediated DNA repair, and second, sensitization of cells to DNAdamaging therapies. Indeed, several PARP inhibitors have demonstrated promising preclinical and clinical antitumour activity with wide therapeutic indices in the setting of tumours with BRCA1 or BRCA2 germline inactivating mutations.12–15 Moreover, numerous preclinical models have also demonstrated that PARP inhibition can sensitize cells to the DNAdamaging effects of ionizing radiation, alkylating agents, and t opoisomerase I targeting.16–19
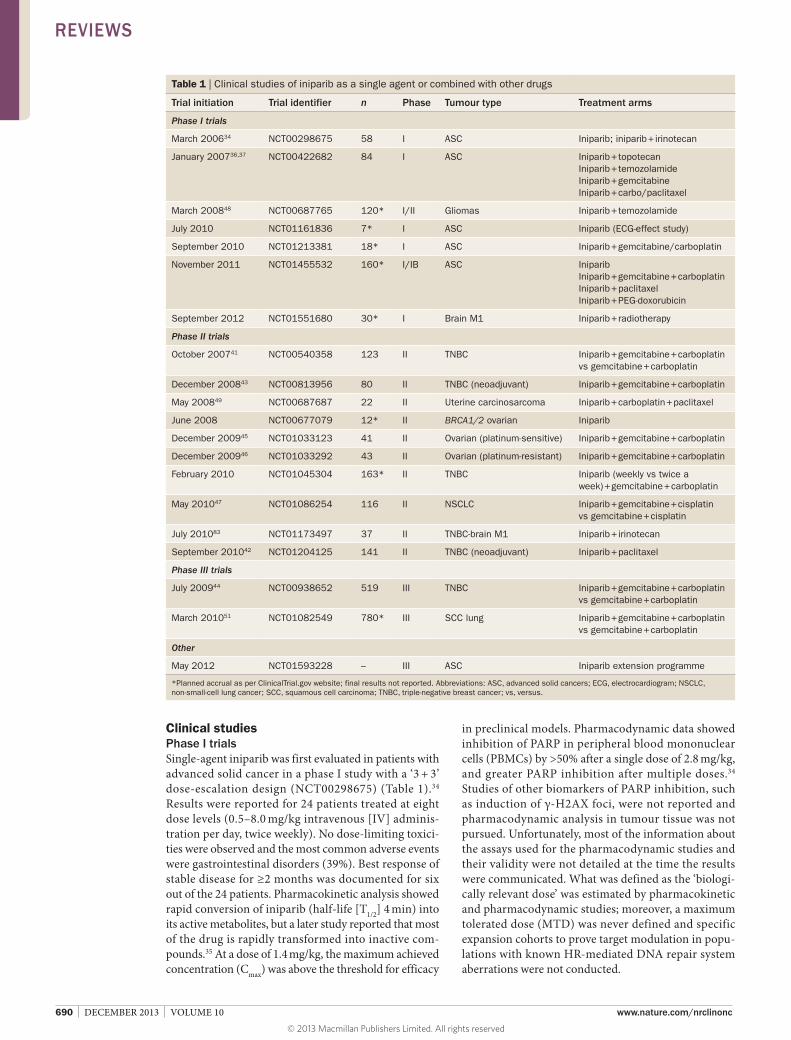
Recent studies have raised concerns that iniparib is not a bona fide PARP inhibitor.20,21 The implications of these new data must be carefully considered, because over 2,500 patients have been treated in clinical trials of iniparib that were designed with PARP inhibition as a therapeutic goal (Table 1). These new data should caution against generalizing the negative results of i niparib trials to the ongoing development of other PARP inhibitors. In this Review, we retrace the development of iniparib from preclinical studies through to phase I–III studies and analyse lessons we must learn to optimize the d evelopment of other t argeted drugs.
Preclinical studiesIniparib was developed as a prodrug of the more reactive, but unstable, 4iodo3nitrosobenzamide (INOBA). INOBA inactivates PARP via two mechanisms: first, zincejection following oxidation of the first zincfinger
Competing interestsThe authors declare no competing interests.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 10 | DECEMBER 2013 | 689
domain of the PARP protein resulting in loss of DNAstimulated PARP activity without loss of DNA binding capacity; second, induction of PARPdegrading aminopeptidases that generate a characteristic polypeptide degradation product.22–25 Importantly, these purported mechanisms of action for iniparib differed significantly from ‘classic’ PARP inhibitors, which specifically target the NAD+ binding site of PARP1 or PARP2, mimicking the NAD+ substrate by resembling the NAD+ moiety and competitively blocking PARP activity.26
Interestingly, the antitumour activity of INOBA also seemed to depend on the levels of glutathione and other reducing compounds. Depletion of glutathione in vitro enhanced antitumour activity and the lack of reducing flavoproteins in malignant cells, that convert INO2BA into nontoxic amines rather than to INOBA, was proposed as a mechanism of selective tumoricidal action of INO2BA in cancer cell cultures, but not in fibroblast cultures.27 Importantly, with or without glutathione depletion, in vitro experiments required substantial concen trations of INO2BA for inhibition of PARP a ctivity and antitumour activity.
There are limited published preclinical studies of inipa rib either as a single agent or in combi nation with chemotherapy; antiproliferative effects have been reported in cancer cell lines including triple negative breast cancer (TNBC; oestrogen [ER]receptornegative, progesterone [PR]receptornegative, and HER2negative) in which iniparib caused cellcycle arrest in the G2/M phase.27,28 However, whereas synthetic lethality in BRCAmutant cell lines was confirmed for other NAD+competitive PARP inhibitors before clinical evaluation,12,26 potent activity of iniparib related to selective inhibition of PARP in BRCAdeficient cultured cells has yet to be reported. Moreover, very few results were available within the public domain on the capacity of iniparib to sensitize cells to DNAdamaging chemotherapy, including p latinum agents,29,30 at the time the clinical trials started.
In vitro studies, however, have suggested that i niparib does not exhibit the properties of a classic PARP inhibitor. The effects of two different structural classes of NAD+competitive PARP inhibitors (benzimidazole and pyridazinone derivatives) were compared with the effects of iniparib and its Cnitroso metabolite (INOBA).26 The effects of these compounds were tested on BRCA1deficient (MDAMB436, exon 20 mutation), BRCA2deficient (DLD1–/–) and BRCA1/2proficient (MDAMB231 and DLD1+/+) breast cancer cell lines. All NAD+competitive PARP inhibitors showed high selectivity for PARP, inhibited PARP enzymatic activity at nanomolar concentrations, inhibited autoribosylation of PARP1, potentiated alkylating chemotherapy (temozolomide), and showed selective activity in BRCAdeficient tumour cell lines and xenograft models. By contrast, iniparib and its metabolite were not able to inhibit PARP enzymatic activity, diminish poly(ADP–ribose) formation, potentiate temozolomide, or show activity in either BRCAdeficient or BRCAproficient cell lines or xenograft models.26 The doses of iniparib required to
achieve a cytotoxic effect were very high (>40 μmol/l). Furthermore, depletion of glutathione, a potential mediator of resistance, did not appreciably alter these observations. Instead of selective potent activity, iniparib was found to nonspecifically react and form adducts with proteins containing cysteine residues, including the PARP1 zinc finger domain.
In a separate study, three different BRCAproficient TNBC cell lines were tested against iniparib and three different NAD+competitive PARP inhibitors: AG014699 (rucaparib, PfizerClovis), AZD2281 (olaparib, AstraZeneca) and ABT888 (veliparib, Abott Laboratories),21 showing lower potency of PARP inhibition and antitumour activity for iniparib. BRCA1 knockdown sensitized cells to iniparib, but it did not result in an increase of γH2AX formation as occurred with rucaparib, olaparib, and veliparib. An in vitro study of 12 breast cancer cell lines demonstrated higher IC50 concentrations for iniparib (13–70 μM) when compared with olaparib (IC50 range 3.7–31 μM).31
Another study exposed HRdeficient cells (BRCA2deficient PEO1 human ovarian cancer cells and ATMdeficient GM16666 fibroblasts) and HRproficient cells (BRCA2revertant PEO4 ovarian cancer cells and ATMrestored GM16667 fibroblasts) to veliparib, olaparib, and iniparib.32 The HRdeficient cells were selectively sensitive to veliparib and olaparib; however, iniparib did not selectively target HRdeficient cells. Furthermore, iniparib—unlike the other tested agents—did not syner gize with either topoisomerase I poisons, cisplatin, gemcitabine, or paclitaxel in various cell lines, and failed to inhibit poly(ADP–ribose) formation even at c oncentrations of 100 μmol/l.
Overall, these preclinical data suggest that the potential cytotoxic effects of iniparib are not mediated by PARP inhibition, but by mechanisms that are yet to be elucidated that might be related to stimulation of intracellular production of reactive oxygen species.33 These findings became apparent only after the pursuit of a large and expensive drug development programme, and clearly question whether the preclinical evidence was strong enough to justify the initiation of clinical trials.
Key points
■ Iniparib is not a bona fide inhibitor of poly(ADP-ribose) polymerase (PARP), so the clinical results in this context should not be extrapolated to other PARP inhibitors in development
■ Preclinical data on iniparib did not sufficiently elucidate the mechanism of action of this agent before clinical trials were initiated
■ Phase I trials should provide proof of mechanism and, ideally, proof of concept, in expansion cohorts to test biological hypotheses; early clinical trials of iniparib lacked proof of mechanism
■ Selection of a patient population, and implementation and validation of predictive biomarkers, are critical to optimize drug development
■ Randomized phase II trials have a significant rate of false positivity, so promising results should be interpreted prudently until other confirmatory studies are reported
■ Preclinical and clinical studies with negative results and efforts evaluating reproducibility of previously published data should be publically available to minimize the risk of publication bias
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
690 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrclinonc
Clinical studiesPhase I trialsSingleagent iniparib was first evaluated in patients with advanced solid cancer in a phase I study with a ‘3 + 3’ doseescalation design (NCT00298675) (Table 1).34 Results were reported for 24 patients treated at eight dose levels (0.5–8.0 mg/kg intravenous [IV] administration per day, twice weekly). No doselimiting toxicities were observed and the most common adverse events were gastro intestinal disorders (39%). Best response of stable disease for ≥2 months was documented for six out of the 24 patients. Pharmacokinetic analysis showed rapid conversion of iniparib (halflife [T1/2] 4 min) into its active metabolites, but a later study reported that most of the drug is rapidly transformed into inactive compounds.35 At a dose of 1.4 mg/kg, the maximum achieved concen tration (Cmax) was above the threshold for efficacy
in preclinical models. Pharmacodynamic data showed inhibition of PARP in peripheral blood mononuclear cells (PBMCs) by >50% after a single dose of 2.8 mg/kg, and greater PARP inhibition after multiple doses.34
Studies of other biomarkers of PARP inhibition, such as induction of γH2AX foci, were not reported and pharmaco dynamic analysis in tumour tissue was not pursued. Unfortunately, most of the information about the assays used for the pharmaco dynamic studies and their validity were not detailed at the time the results were communicated. What was defined as the ‘biologically relevant dose’ was estimated by pharmaco kinetic and pharmacodynamic studies; moreover, a maximum toler ated dose (MTD) was never defined and specific expansion cohorts to prove target modulation in populations with known HRmediated DNA repair system a berrations were not conducted.
Table 1 | Clinical studies of iniparib as a single agent or combined with other drugs
Trial initiation Trial identifier n Phase Tumour type Treatment arms
Phase I trials
March 200634 NCT00298675 58 I ASC Iniparib; iniparib + irinotecan
January 200736,37 NCT00422682 84 I ASC Iniparib + topotecanIniparib + temozolamideIniparib + gemcitabineIniparib + carbo/paclitaxel
March 200848 NCT00687765 120* I/II Gliomas Iniparib + temozolamide
July 2010 NCT01161836 7* I ASC Iniparib (ECG-effect study)
September 2010 NCT01213381 18* I ASC Iniparib + gemcitabine/carboplatin
November 2011 NCT01455532 160* I/IB ASC IniparibIniparib + gemcitabine + carboplatinIniparib + paclitaxelIniparib + PEG-doxorubicin
September 2012 NCT01551680 30* I Brain M1 Iniparib + radiotherapy
Phase II trials
October 200741 NCT00540358 123 II TNBC Iniparib + gemcitabine + carboplatinvs gemcitabine + carboplatin
December 200843 NCT00813956 80 II TNBC (neoadjuvant) Iniparib + gemcitabine + carboplatin
May 200849 NCT00687687 22 II Uterine carcinosarcoma Iniparib + carboplatin + paclitaxel
June 2008 NCT00677079 12* II BRCA1/2 ovarian Iniparib
December 200945 NCT01033123 41 II Ovarian (platinum-sensitive) Iniparib + gemcitabine + carboplatin
December 200946 NCT01033292 43 II Ovarian (platinum-resistant) Iniparib + gemcitabine + carboplatin
February 2010 NCT01045304 163* II TNBC Iniparib (weekly vs twice a week) + gemcitabine + carboplatin
May 201047 NCT01086254 116 II NSCLC Iniparib + gemcitabine + cisplatinvs gemcitabine + cisplatin
July 201083 NCT01173497 37 II TNBC-brain M1 Iniparib + irinotecan
September 201042 NCT01204125 141 II TNBC (neoadjuvant) Iniparib + paclitaxel
Phase III trials
July 200944 NCT00938652 519 III TNBC Iniparib + gemcitabine + carboplatinvs gemcitabine + carboplatin
March 201051 NCT01082549 780* III SCC lung Iniparib + gemcitabine + carboplatinvs gemcitabine + carboplatin
Other
May 2012 NCT01593228 – III ASC Iniparib extension programme
*Planned accrual as per ClinicalTrial.gov website; final results not reported. Abbreviations: ASC, advanced solid cancers; ECG, electrocardiogram; NSCLC, non-small-cell lung cancer; SCC, squamous cell carcinoma; TNBC, triple-negative breast cancer; vs, versus.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 10 | DECEMBER 2013 | 691
A phase Ib study combined iniparib with four differ ent chemotherapy regimens: topotecan (n = 14), gemcita bine (n = 22), temozolomide (n = 17), and carbo platin plus paclitaxel (n = 13) (NCT00422682).36 The doses of iniparib explored ranged from 1.1–11.2 mg/kg (IV, days 1 and 4 of every week). Surprisingly, no doselimiting toxicities were reported, and seven of 66 patients (10%) achieved radiological partial or complete responses as their best response to treatment. Further safety data from an expansion cohort who received carbo platin (AUC6, day 1) plus paclitaxel (200 mg/m2, day 1) with iniparib (5.6 mg/kg, IV, days 1, 4, 8, and 11) again showed a low incidence of grade 3 or 4 adverse effects neutropenia (13.3%) and anaemia (6.7%).37 These data contrast with PARP inhibitor trials in which singleagent doseescalation was limited by haematological toxi city, which was further potentiated by combination with chemotherapy.14,38,39
Phase II trials in TNBCAn openlabel, randomized phase II study in 123 patients with TNBC evaluated gemcitabine (1,000 mg/m2, days 1 and 8) plus carboplatin (AUC 2, days 1 and 8)40 with or without iniparib (initially 4.0 mg/kg, days 1, 4, 8, and 11; later amended to 5.6 mg/kg on the same schedule) once every 3 weeks (NCT00540358).41 The majority of patients (58.5%) had no prior systemic treatment for metastatic disease. The efficacy analyses evaluated the intentiontotreat population but, unlike the later phase III trial, radiological response assessments were performed by the investigators and were not subjected to an external blinded review. Patients with or without BRCA mutations were eligible, but the number of patients with BRCA mutations and their outcome have not been reported.
The clinical benefit rate (CBR), which is the rate of complete or partial radiological response together with stable disease >6 months, and objective response rate (ORR) were 34% and 32% in the chemotherapy alone arm, and 56% and 52% in the iniparib arm, respectively. The trial was designed to detect an improvement in CBR, assuming a rate of 0.45 in the control group and expecting a CBR >0.60 in the experimental arm (with a power of 80% and accepting a twosided α error of 0.05). Consequently, the study was considered positive (P = 0.001 for CBR; P = 0.002 for ORR). Secondary survival end points were also positive, but subject to very broad 95% confidence intervals; median progressionfree survival (PFS) was 3.6 (2.6–5.2) months in the chemotherapy alone group versus 5.9 (4.5–7.2) months in the iniparib group (P = 0.01). Overall survival was 7.7 (6.5–13.3) months compared with 12.3 (9.8–21.5) months (P = 0.01) for the iniparib arm. Interestingly, no difference in the rate of adverse events, including haemato logical events, was observed between the two arms, again raising concerns regarding the lack of classtype t oxicities associated with PARP inhibitors.
A neoadjuvant trial of weekly paclitaxel (80 mg/m2, day 1) alone or with iniparib once weekly (11.2 mg/kg, IV, day 1) or iniparib twice weekly (5.6 mg/kg, IV) was also pursued in patients with TNBC (NCT01204125).42 Overall, 141 patients were recruited; the trial did not detect differences in the primary end point, rate of
pathological complete response (pCR) of the primary breast tumour. In another trial, 80 patients received 4–6 cycles of neoadjuvant gemcita bine (1,000 mg/m2, IV), carboplatin (AUC2, IV, days 1 and 8) and iniparib (5.6 mg/kg, IV, days 1, 4, 8, and 11) once every 3 weeks (NCT00813956). A pCR rate of 47% (90% CI 27–69%) was reported for the 19 carriers of BRCA mutation treated; for the BRCA wildtype p articipants, the pCR rate was 33% (90% CI 23–44%).43
Phase III trial in TNBCIniparib quickly entered into phase III trials, labelled as a PARP inhibitor following the promising phase II data.41 A randomized openlabel phase III study enrolled patients with TNBC who had undergone up to two prior lines of treatment.44 Patients were randomly assigned (1:1) to gemcitabine–carboplatin alone (gemcitabine 1,000 mg/m2, IV) and carboplatin (AUC 2; , IV, days 1 and 8) or the same regimen plus iniparib (5.6 mg/kg, IV, days 1, 4, 8, and 11) every 3 weeks. The trial was planned with two coprimary end points: overall survival and PFS. The sample size was calculated with the aim of detecting, with a power of 90%, a HR of 0.65 for PFS and 0.66 for overall survival between the two arms. The type 1 error accepted (0.05, twosided) was divided for the two coprimary end points (0.04 for overall survival and 0.01 for PFS). The trial was to be considered positive if either one of the two primary end points was met. Between July 2009 and March 2010, 519 patients were enrolled and randomly assigned, which constituted overrecruitment of patients as the statistical design demanded 420 patients to test the hypothesis. Patient demographics suggested a similar population to the prior phase II trial. In total, 152 of 258 patients (59%) on the chemotherapy only arm crossed over to receive chemotherapy and iniparib following disease progression. ORR was not signifi cantly different (30% versus 34%), nor was the study positive for either of the coprimary end points.44
Clinical trials in other tumour typesTwo singlearm trials in both platinumsensitive and platinum resistant recurrent ovarian carcinoma have tested iniparib in combination with carboplatin and gemcitabine (NCT01033123 and NCT01033292).45,46 A significant number of BRCAmutation carriers were enrolled, but no relationship between BRCA status and objective response was observed.14,38
Other trials have explored the antitumour activity of iniparib in combination with several chemotherapy regimens in lung cancer, gliomas, and uterine carcino sarcoma.47–49 Overall, none of these trials has provi ded either proof of concept of chemosensitization with inipa rib or identified predictive biomarkers of response. A phase II trial in patients with lung cancers and all histologies but largely nonsquamous did not report improvement of overall survival or PFS.47 In parallel, a large randomized phase III study in patients with newly diagnosed squamouscell lung cancer was pursued (NCT01082549).50 Final results are yet to be presented, but a negative outcome has been announced in a press note (Table 1).51
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

692 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrclinonc
Appraising iniparib: critical questionsWas sufficient preclinical data acquired?When the early clinical trials began, limited published preclinical data supported the clinical evaluation of inipa rib in patients with cancer. Iniparib was ‘labelled’ as a potent and selective PARP inhibitor, and clinical trials were designed to recruit patients with presumed DNA repair deficiency. Later attempts to evaluate iniparib by independent investigators failed to find supporting evidence of potent and selective PARP inhibition. This inability to validate the mechanism of action, the lack of in vitro data supporting a selective effect on HRdeficient cell lines, and the lack of robust evidence of synergy in combination with chemotherapy raises signifi cant concerns that the preclinical evidence was insufficient to initiate clinical studies.
Reproducibility of research results is an often underestimated concern, at least in part because of academic and/or industry pressures to accelerate drug development programmes, maximize fiscal return, and achieve academic recognition. When selecting a compound to enter clinical evaluation, careful scrutiny is needed of the available preclinical data, the validity of the assays used, and the robustness of the results to justify the high amount of personal and monetary resources to be employed. Two independent studies evaluating the reproducibility of results published by either academic researchers or pharma ceutical industry investigators in highimpact publications have recently exposed the problem: only 11–25% of published results could be replicated by two groups of industry investigators, even when using identical reagents (usually provided by the original laboratories).52,53 The issue is also relevant when developing drug combinations, as the concept of ‘synergy’ is often overestimated and clinical trials too often fail to confirm the expectations derived from preclinical results.54 Investigators, industry, and editors should also be encouraged to report and accept for publication ‘negative’ preclinical studies to limit such publication bias, and to await a robust confirmation and appraisal of preclinical data before clinical trials are commenced.
Were proof of mechanism and concept pursued?Given the extremely short reported T1/2 of iniparib (4–11 min),34 a major concern is whether systemic exposure to iniparib or its active metabolites are significant enough for clinical activity. Although Cmax plasma levels of iniparib exceeded concentrations necessary for in vitro activity, few data are available regarding plasma exposure (such as AUC) necessary for antitumour activity. Although early phase trials reported a T1/2 of 2–4 h for the active metabolites, Verweij et al.35 presented contra dicting data that T1/2 of metabolites was <2 h, with substantial inactivation of the parent compound by gluta thione. Furthermore, pharmacokinetic exposures were not c orrelated with target modulation in tumour tissue, as no pharmaco dynamic data from paired tumour samples were reported. This issue is particularly important because no radiological antitumour activity was observed in the original singleagent iniparib dosefindin g trial.34
The low incidence of haematological adverse events and lack of singleagent antitumour activity in early phase trials could prompt concerns of a possible alternative mechanism of action.14,38 In this situation, proofofmechanism or proofofconcept studies are particularly critical to demonstrate robust target modulation via validated pharmacodynamic assays in samples of relevance. As mentioned, the effect of iniparib on target PARP modulation was reported only in PBMCs, but not in paired tumour tissue biopsies. Although normal tissue pharmacodynamic studies (in PBMCs, skin, or hair follicles) might suggest biological target modulation and assist in identifying the optimal time points to perform tumour biopsies, such analyses are limited in predicting effects in tumour tissue owing to limitations in drug delivery and tumour heterogeneity.55,56 Ultimately, in the absence of observed radiological responses and/or clinical toxicity, analysis of paired tumour biopsies are necessary to understand the relationship between drug dose and potency and duration of target pharmaco dynamic modulation.57,58 Ideally, evaluation of PARP inhibition by assessment of diminished formation of poly(ADP–ribose) polymerase polymers, inhibition of PARP1 activity, and induction of γH2AX in tumour samples would have provided s ignificant support of the proof of the mechanism for iniparib.
The ‘biologically active dose’ and recommended phase II dose for iniparib (5.6 mg/kg, IV, twice weekly) was—critically—not defined on the basis of evidence of objective singleagent radiological response, doselimiting toxicities, or robust pharmacodynamic data. Such data should be crucial to make informed go/nogo decisions in drug development.59 Defining antitumour activity and toxicity of drug doses well above the lowest biologically active dose is important, because poor drug penetration is commonly a mechanism of treatment resistance.60 It is advisable to evaluate the antitumour activity of the MTD versus the minimum biologically active dose of novel agents while acquiring detailed pharmaco dynamic data. Ideally, this should be done in specific expansion cohorts of phase I trials while focusing on the appropriate population for the biological context.
Indeed, in the field of PARP inhibition, some evidence suggests a doseactivity relationship above the lowest biologically active dose. In the phase I trial of olaparib, the pharmacodynamic studies defined 100 mg twice daily as a biologically effective dose whereas the MTD of the drug, based on the tolerability profile, was 400 mg.14 Phase II trials comparing 100 mg versus 400 mg twice daily in sequentially enrolled cohorts showed clear superior ity for 400 mg twice daily dose in both patients with breast cancer and ovarian cancer.61,62
What was the target population?The advent of targeted therapies has necessitated a shift in histologically driven selection of target populations to molecularly selected groups of patients. Characterization of the appropriate population should happen in concert with the preclinical studies characterizing the properties of a new compound and establishing practical methods
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 10 | DECEMBER 2013 | 693
to identify those patients with a validated biomarker. As a purported PARP inhibitor, iniparib was developed in populations thought to be defective in HR DNA repair, as well as populations thought to benefit from potential chemosensitization.
Several trials of iniparib were conducted in women with TNBC on the basis of favourable preclinical data, an unmet medical need, and the suggestion that the basallike group of breast cancers is associated with functional defects in HRmediated DNA repair.63–65 Moreover, preclinical data showed significant upregulation of PARP in TNBC in comparison with other subtypes of breast cancer.66 However, defining TNBC as a target population is challenging as it is characterized by the absence of three biomarkers (ER, PR and HER2) rather than by a positive selection biomarker indicative of HRmediated DNArepair deficiency. Moreover, although the TNBC population has been shown to be enriched (perhaps up to 71%) in those with basallike breast cancers,67 the explora tory Affimetrix geneexpression profiling of the inipa rib phase III study revealed considerable molecular heterogeneity in the trial population.44 Even if iniparib were a potent PARP inhibitor, the estimated frequency of BRCA1 and BRCA2 germline mutations in unselected TNBC is approximately 10–20%.68,69 Furthermore, even accepting that there is accumulation of PARP1 in several tumour types, including TNBC,66 and that PARP1 might act as a BRCA2expression downregulator,70 no clinical data supports PARP1 upregulation as a predictive marker of sensitivity to PARP inhibitors.
At present, no validated strategy is available to identi fy patients with TNBC who have DNArepair deficiencies to participate in trials of PARP inhibitors other than testing for germline BRCA1/2 mutations, which might have been used to demonstrate proof of concept for single agent iniparib. An alternative approach is to design trials attempting clinical validation of other candidate biomarkers, such as a panel of immuno histochemical markers, namely ER, HER2, CK5, CK6, and EGFR, which have been used to retrospectively identify basallike tumours with high specificity and sensitivity71 or functional assays for HR competency, which are currently being developed.72
The optimal target population for PARP inhibitors has been explored in a number of trials, for example, Gelmon et al.13 recruited patients with ovarian cancer and TNBC to receive olaparib, and prospectively evaluated the results on the basis of the presence of BRCA1/2 mutations. Among nonBRCAmutated patients, the cohort of patients with ‘sporadic’ TNBC was rapidly closed after no signs of anticancer activity were detected in the first 15 patients. However, consistent with earlier studies,73 a cohort of predominantly platinum sensitive nonBRCA-mutated patients with ovarian cancer responded to olaparib treatment. One potential reason contributing to the lower number of responses in the BRCA-mutated breast cancer cohort and the complete lack of benefit for the unselected TNBC group might be the high number of prior treatment regimens received by these patients (the median prior lines of chemotherapies was
three, and ranged from one to seven), which included patients with platinumresistant or refractory disease; however, detailed information on prior treatments was not a vailable for this study.
Overall, these findings strongly reinforce the importance of pursuing proof of concept in carefully selected target populations when designing clinical studies. In hindsight, the iniparib trials might have taken both attention and resources away from the patients proven to benefit most from PARP inhibitors, the BRCA m utation carriers.
Transition from phase I to phase III Frameworks such as the Pharmacological Audit Trail (PhAT)58,74 can subject a new compound that is transition ing from preclinical to clinical trials to critical performance criteria. These frameworks ask a series of questions that require demonstration of proof of concept and testing of mechanistic hypotheses (Figure 1) to better select drugs that merit further evaluation. In this transition to phase III trials, we must continually reinforce and match knowledge gained from preclinical and clinical studies so that each stage of development benefits from all available information.
When iniparib was entering phase II trials, preclinical synergistic cytotoxicity data was reported for iniparib when combined with gemcitabine and carboplatin in TNBC cell lines;75 however, activity and toxicity of the gemcitabine–carboplatin combination was not studied in earlier phase I trials. A dosefinding study of iniparib in combination with carboplatin and gemcitabione was initiated in Japan at the request of the Japanese regulatory authorities, after the phase II/III trials in patients with TNBC were recruiting (NCT01213381).76 These findings bring into question how the backbone of carboplatin (AUC2, days 1 and 8) in combination with gemcitabine (1,000 mg/m2, days 1 and 8) every 3 weeks was chosen for the subsequent phase II and phase III trials, considering prior trials that used gemcitabine–carboplatin with targeted agents in breast cancer had used a moreintense dosing of carboplatin.77,78 Since the CBR of 34% (primary end point of the iniparib randomized phase II trial) in the control group was lower than expected (45%), one must question whether this relates to underdosing of carboplatin.
Allowing crossover in randomized trials is another factor that merits discussion in the development of inipa rib. Crossover was permitted in the phase II study, which can be justified and frequently practiced for ‘ethical reasons’. In this case, 30 of 59 (51%) patients randomly assigned to the gemcitabine–carboplatin arm received gemcitabine–carboplatin–iniparib at disease progression, but 83% of those patients discontinued the triple treatment after two cycles or fewer, so the crossover did not translate into any significant signal of benefit. Despite these findings, the phase III trial also allowed patients in the gemcitabine–carboplatin arm to receive gemcitabine–carboplatin–iniparib at disease progression. Considering how crossover undeniably complicates the interpretation of overall survival results, because patients in both arms
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

694 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrclinonc
receive the experimental agent, the phase III design should have considered the lack of benefit patients would receive who were crossed over in the previous study. One additional consideration is that if gemcitabine–ca rboplatin–iniparib is truly inferior to gemcitabine–carboplatin alone, a crossover design might benefit the experi mental arm because those who crossover to iniparib remain on ineffec tive treatment after disease p rogression when receiving gemcitabine–carboplatin.79
End point selection is also a critical factor in the design of registration studies. The phase III trial of gemcitabine–carboplatin–iniparib in patients with TBNC was designed with coprimary end points of overall survival and PFS, but it is important to mention that PFS has not been demonstrated to be a surrogate marker of overall survival in metastatic breast cancer, as was shown for bevacizumab.80–82 Despite the benefits of using PFS, especially if presented together with improvement in qualityoflife parameters, concerns should be raised about the continued selection of PFS as a primary end point in registration trials, particularly when p ermitting the potential impact of crossover on overall survival.
ConclusionsA successful drug development programme demands a plausible biological hypothesis supported by robust and reproducible preclinical data, early trials providing proof of desired target modulation, analysis and/or validation of putative predictive/patient enrichment bio markers, transparent rules to make ‘nogo’ decisions early in develop ment, and, finally, a multidisciplinary translational strategy that produces continuous r eiterative f eedback between preclinical and clinical research.
In hindsight, the development of iniparib proceeded without sufficient preclinical and pharmacodynamic data to warrant larger trials. This included a failure to acquire proof of target modulation and antitumour activity in the BRCA-mutated population on the basis of a predictive biomarker. Ultimately, the phase III trial in TNBC failed to meet its coprimary end points, promulgating the notion that PARP is not a good therapeutic target, despite significant antitumour activity demonstrated by other PARP inhibitors.38,60,61 Ironically, negative results from the phase III trials in TNBC were communicated to the media only 22 days after the phase II study was
Population identi�cation
Targeted drug candidate
Validated predictive assayfor molecular aberration
Pharmacokinetics
Pharmacodynamics
Biochemical pathwaymodulation
Achievement ofbiological effect
Hypothesis testing usingintermediate end points
of clinical response
Reassessment of molecularalterations at disease
progression
Inhibition of resistantbiological pathways
4-iodo-3-nitrobenzamide(Iniparib)
Generic PhAT Questions of PhAT
Yes, adequate concentrationsin plasma achieved
Unknown—no tumour biopsy datashowing PARP inhibition
PARP zinc-ejection (inactivation)Induction of PARP proteases
Sensitization of chemotherapy
BRCA1/2 germline mutation valid‘BRCAness’ not validated
No marker for chemosensitization
PBMC PARP inhibition seenbut insuf�ciently robust data
No tumour biopsy data available
No
No
Are adequate concentrations of drugand metabolites in plasma achieved?
Are adequate concentrations of drugand metabolites in tumour achieved?
What are the proposed mechanism(s)of the novel drug candidate?
What are the validated predictiveassays for the target of the drug?
What are the pharmacodynamic effectsin surrogate normal cells?
What are the pharmacodynamiceffects in tumour cells?
Is there a proposed population to betargeted by the novel drug?
Is there modulation of thetargeted biochemical pathway?
Is there evidence of wanted biologicaleffect or clinical response?
Is there modulation of circulating tumourcells, tumour markers, or other markers?
Is there evidence of mechanism(s)of resistance to drug?
Is there a mechanism of overcomingmechanisms of resistance?
BRCA1/2 germline mutation‘BRCAness’ in TNBC and ovarian cancer
population sensitive to DNA-damaging agents
Glutathione inactivation has notbeen pursued
Single-agent activity very limitedCombination data heterogeneous
In plasma perhapsNo tumour biopsy data
Figure 1 | Confronting the Pharmacological Audit Trail (PhAT). Adapted from Yap et al.58 (left) with the published data from the iniparib preclinical and clinical studies (right). Permission obtained from Nature Publishing Group © Yap, T. A. et al. Nat. Rev. Cancer 10, 514–523 (2010).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 10 | DECEMBER 2013 | 695
published in a highimpact journal. Overall, the story of iniparib is a compendium of results released in abstract form or never published, with few results in peerreview publications, making it difficult to examine by i ndependent investigators.
Overall, these outcomes should challenge us to systematic ally scrutinize each step during drug discovery and development, as well as understand the context of phase II trials and the significant risk of falsepositive results from randomized phase II studies. This case should at least guide the scientific community to a consensus about the characteristics a PARP1 inhibitor must exhibit in preclinical and early clinical studies.
Clinical development of iniparib has now been interrupted; considering the enormous time and money invested on it, the story of iniparib clearly merits the attention of academics and industry and the reflection
that without a clear understanding of the mechanism of action of a new compound, analytically validated biomarkers to guide dose and schedule selection, and predictive biomarkers to define the optimal target population, drug development efforts remain at high risk of failure.
Review criteria
We searched the MEDLINE and PubMed databases for original articles focusing on iniparib published between 2005 and 2013, as well as abstract databases from ASCO, ESMO and AACR between 2005 and 2013. The search terms we used were “iniparib”, “BSI-201” or “4-iodo-3-nitrobenzamide” and “PARP”. All papers and abstracts identified were English-language full-text papers or abstracts. We also searched the reference lists of identified articles for further papers.
1. Arrowsmith, J. Trial watch: phase III and submission failures: 2007–2010. Nat. Rev. Drug Discov. 10, 87 (2011).
2. Arrowsmith, J. Trial watch: phase II failures: 2008–2010. Nat. Rev. Drug Discov. 10, 328–329 (2011).
3. Kola, I. & Landis, J. Can the pharmaceutical industry reduce attrition rates? Nat. Rev. Drug Discov. 3, 711–715 (2004).
4. Collier, R. Rapidly rising clinical trial costs worry researchers. CMAJ 180, 277–278 (2009).
5. Bach, P. B. Limits on Medicare’s ability to control rising spending on cancer drugs. N. Engl. J. Med. 360, 626–633 (2009).
6. Sullivan, R. et al. Delivering aff ordable cancer care in high-income countries. Lancet Oncol. 12, 933–980 (2011).
7. Amiri-Kordestani, L. & Fojo, T. Why do phase III clinical trials in oncology fail so often? J. Natl Cancer Inst. 104, 568–569 (2012).
8. Hutchinson, L. & Kirk, R. High drug attrition rates—where are we going wrong? Nat. Rev. Clin. Oncol. 8, 189–190 (2011).
9. Ocana, A., Pandiella, A., Siu, L. L. & Tannock, I. F. Preclinical development of molecular-targeted agents for cancer. Nat. Rev. Clin. Oncol. 8, 200–209 (2010).
10. Kola, I. & Landis, J. Can the pharmaceutical industry reduce attrition rates? Nat. Rev. Drug Discov. 3, 711–715 (2004).
11. LoRusso, P. M. et al. Translating clinical trials into meaningful outcomes. Clin. Cancer Res. 16, 5951–5955 (2010).
12. Farmer, H. et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 434, 917–921 (2005).
13. Gelmon, K. A. et al. Olaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: a phase 2, multicentre, open-label, non-randomised study. Lancet Oncol. 12, 852–861 (2011).
14. Fong, P. C. et al. Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA mutation carriers. N. Engl. J. Med. 361, 123–134 (2009).
15. Bryant, H. E. et al. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature 434, 913–917 (2005).
16. Russo, A. L. et al. In vitro and in vivo radiosensitization of glioblastoma cells by the poly(ADP-ribose) polymerase inhibitor E7016. Clin. Cancer Res. 15, 607–612 (2009).
17. Calabrese, C. R. et al. Anticancer chemosensitization and radiosensitization by
the novel poly(ADP-ribose) polymerase-1 inhibitor AG14361. J. Natl Cancer Inst. 96, 56–67 (2004).
18. Senra, J. M. et al. Inhibition of PARP-1 by olaparib (AZD2281) increases the radiosensitivity of a lung tumor xenograft. Mol. Cancer Ther. 10, 1949–1958 (2011).
19. Treszezamsky, A. D. et al. BRCA1- and BRCA2-deficient cells are sensitive to etoposide-induced DNA double-strand breaks via topoisomerase II. Cancer Res. 67, 7078–7081 (2007).
20. Patel, A. G., De Lorenzo, S. B., Flatten, K. S., Poirier, G. G. & Kaufmann, S. H. Failure of iniparib to inhibit poly(ADP-Ribose) polymerase in vitro. Clin. Cancer Res. 18, 1655–1662 (2012).
21. Chuang, H. C., Kapuriya, N., Kulp, S. K., Chen, C.-S. & Shapiro, C. L. Differential anti-proliferative activities of poly(ADP-ribose) polymerase (PARP) inhibitors in triple-negative breast cancer cells. Breast Cancer Res. Treat. 134, 649–659 (2012).
22. Chuang, A. J., Killam, K. F. Jr, Chuang, R. Y., Mendeleyev, J. & Kun, E. Comparison of the cytotoxic and antiretroviral effects of 3-nitrosobenzamide and 4-iodo-3-nitrobenzamide. Proc. West. Pharmacol. Soc. 37, 117–119 (1994).
23. Mendeleyev, J., Kirsten, E., Hakam, A., Buki, K. G. & Kun, E. Potential chemotherapeutic activity of 4-iodo-3-nitrobenzamide. Metabolic reduction to the 3-nitroso derivative and induction of cell death in tumor cells in culture. Biochem. Pharmacol. 50, 705–714 (1995).
24. Kirsten, E. & Kun, E. Cancer cell selectivity of 5-iodo-6-aminobenzopyrone (INH2BP) and methyl-3,5-diiodo-4(4'-methoxyphenoxy) benzoate (DIME). Int. J. Mol. Med. 5, 279–281 (2000).
25. Bauer, P. I. et al. Anti-cancer action of 4-iodo-3-nitrobenzamide in combination with buthionine sulfoximine: inactivation of poly(ADP-ribose) polymerase and tumor glycolysis and the appearance of a poly(ADP-ribose) polymerase protease. Biochem. Pharmacol. 63, 455–462 (2002).
26. Liu, X. et al. Iniparib nonselectively modifies cysteine-containing proteins in tumor cells and is not a bona fide PARP inhibitor. Clin. Cancer Res. 18, 510–523 (2012).
27. Kun, E., Mendeleyev, J., Hakam, A. & Kirsten, E. Enzymatic mechanism of the tumoricidal action of 4-iodo-3-nitrobenzamide. Mol. Med. Rep. 2, 739–742 (2009).
28. Ossovskaya, V. et al. BSI-201 enhances the activity of multiple classes of cytotoxic agents and irradiation in triple negative breast cancer [abstract]. Proc. 100th Annu. Meeting Am. Assoc. Cancer Res. a5552 (2009).
29. Ossovskaya, V. et al. The chemosensitizing properties of iniparib in combination with DNA-damaging agents in the MDA-MB-468(-) triple-negative breast cancer (TNBC) cell line [abstract]. Cancer Res. 71 (Suppl.), aLB-401 (2011).
30. Ossovskaya, V. et al. Cell cycle effects of iniparib, a PARP inhibitor, in combination with gemcitabine and carboplatin in the MDA-MB-468(–) triple-negative breast cancer (TNBC) cell line [abstract P5-06-09]. Cancer Res. 70 (Suppl.), aP5-06-09 (2010).
31. Cotter, M. B. et al. Preclinical evaluation of PARP inhibition in breast cancer: Comparative effetiveness of olaparib and iniparib [abstract]. J. Clin. Oncol. 30 (Suppl.), a1042 (2012).
32. Patel, A. G., De Lorenzo, S. B., Flatten, K. S., Poirier, G. G. & Kaufmann, S. H. Failure of iniparib to inhibit poly(ADP-Ribose) polymerase in vitro. Clin. Cancer Res. 18, 1655–1662 (2012).
33. Licht, S. et al. Mechanism of action of iniparib: stimulation of reactive oxygen species (ROS) production in an iniparib-sensitive breast cancer cell line [abstract]. Mol. Cancer Ther. 10 (Suppl.), a226 (2011).
34. Kopetz, S. et al. First in human phase I study of BSI-201, a small molecule inhibitor of poly ADP-ribose polymerase (PARP) in subjects with advanced solid tumors [abstract]. J. Clin. Oncol. 26 (Suppl.), a3577 (2008).
35. Verweij, J. et al. Pharmacokinetics and metabolism of iniparib for the treatment of metastatic triple-negative breast cancer (TNBC) [abstract]. Mol. Cancer Ther. 10 (Suppl.), aA134 (2011).
36. Mahany, J. J. et al. A phase IB study evaluating BSI-201 in combination with chemotherapy in subjects with advanced solid tumors [abstract]. J. Clin. Oncol. 26 (Suppl.), a3579 (2008).
37. Mita, A. C. et al. A phase IB trial of iniparib (BSI-201) in combination with carboplatin (C)/paclitaxel (P) in patients with non-small cell lung cancer (NSCLC) [abstract]. J. Clin. Oncol. 29 (Suppl.), a7570 (2011).
38. Sandhu, S. K. et al. The poly(ADP-ribose) polymerase inhibitor niraparib (MK4827) in BRCA mutations carriers and patients with sporadic cancer: a phase 1 dose-escalation trial. Lancet Oncol. 14, 882–892 (2013).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
696 | DECEMBER 2013 | VOLUME 10 www.nature.com/nrclinonc
39. Rajan, A. et al. A phase I combination study of olaparib with cisplatin and gemcitabine in adults with solid tumors. Clin. Cancer Res. 18, 2344–2351 (2012).
40. Calvert, A. H. et al. Carboplatin dosage: prospective evaluation of a simple formula based on renal function. J. Clin. Oncol. 7, 1748–1756 (1989).
41. O’Shaughnessy, J. et al. Iniparib plus chemotherapy in metastatic triple-negative breast cancer. N. Engl. J. Med. 364, 205–214 (2011).
42. Llombart, A. et al. SOLTI NeoPARP: A phase II, randomized study of two schedules of iniparib plus paclitaxel and paclitaxel alone as neoadjuvant therapy in patients with triple-negative breast cancer (TNBC) [abstract]. J. Clin. Oncol. 30 (Suppl.), a1011 (2012).
43. Telli, M. L. et al. PrECOG 0105: Final efficacy results from a phase II study of gemcitabine (G) and carboplatin (C) plus iniparib (BSI-201) as neoadjuvant therapy for triple-negative (TN) and BRCA1/2 mutation-associated breast cancer [abstract]. J. Clin. Oncol. 31 (Suppl.), a1003 (2013).
44. O’Shaughnessy, J. et al. A randomized phase III study of iniparib (BSI-201) in combination with gemcitabine/carboplatin (G/C) in metastatic triple-negative breast cancer (TNBC) [abstract]. J. Clin. Oncol. 29 (Suppl.), a1007 (2011).
45. Penson, R. T. et al. A phase II trial of iniparib (BSI-201) in combination with gemcitabine/carboplatin (GC) in patients with platinum-sensitive recurrent ovarian cancer [abstract]. J. Clin. Oncol. 29 (Suppl.), a5004 (2011).
46. Birrer, M. J. et al. A phase II trial of iniparib (BSI-201) in combination with gemcitabine/carboplatin (GC) in patients with platinum-resistant recurrent ovarian cancer [abstract]. J. Clin. Oncol. 29 (Suppl.), a5005 (2011).
47. Novello, S. et al. Results of a phase 2 study of gemcitabine/cisplatin/iniparib (GCI) versus gemcitabine/cisplatin (GC) in patients with advanced NSCLC [abstract]. Eur. J. Cancer 47 (Suppl.), a9006 (2011).
48. Blakeley, J. O. et al. Poly (ADP- ribose) polymerase -1 (PARP1) inhibitor BSI- 201 in combination with temozolomide (TMZ) in malignant glioma [abstract]. J. Clin. Oncol. 28 (Suppl. 15), a2012 (2010).
49. Aghajanian, C., Sill, M. W., Secord, A. A., Powell, M. A. & Steinhoff, M. Iniparib plus paclitaxel and carboplatin as initial treatment of advanced or recurrent uterine carcinosarcoma: a Gynecologic Oncology Group Study. Gynecol. Oncol. 126, 424–427 (2012).
50. US National Library of Medicine. Clinicaltrials.gov [online], http://clinicaltrials.gov/show/NCT01082549 (2012).
51. Sanofi. Press release: Sanofi provides update on phase 3 studies of two investigational compounds [online], http://en.sanofi.com/Images/ 33127_20130603_rdupdate_en.pdf (2013).
52. Begley, C. G. & Ellis, L. Drug development: Raise standards for preclinical cancer research. Nature 483, 531–533 (2012).
53. Prinz, F., Schlange, T. & Asadullah, K. Believe it or not: how much can we rely on published data on potential drug targets? Nat. Rev. Drug Discov. 10, 712 (2011).
54. Ocana, A., Amir, E., Yeung, C., Seruga, B. & Tannock, I. F. How valid are claims for synergy in
published clinical studies? Ann. Oncol. 23, 2161–2166 (2012).
55. Workman, P. Challenges of PK/PD measurements in modern drug development. Eur. J. Cancer 38, 2189–2193 (2002).
56. Minchinton, A. I. & Tannock, I. F. Drug penetration in solid tumours. Nat. Rev. Cancer 6, 583–592 (2006).
57. Sandhu, S. K., Yap, T. A. & de Bono, J. S. Poly(ADP-ribose) polymerase inhibitors in cancer treatment: a clinical perspective. Eur. J. Cancer 46, 9–20 (2010).
58. Yap, T. A., Sandhu, S. K., Workman, P. & de Bono, J. S. Envisioning the future of early anticancer drug development. Nat. Rev. Cancer 10, 514–523 (2010).
59. de Bono, J. S. & Ashworth, A. Translating cancer research into targeted therapeutics. Nature 467, 543–549 (2010).
60. Postel-Vinay, S. et al. Clinical benefit in phase-I trials of novel molecularly targeted agents: does dose matter? Br. J. Cancer 100, 1373–1378 (2009).
61. Tutt, A. et al. Oral poly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2 mutations and advanced breast cancer: a proof-of-concept trial. Lancet 376, 235–244 (2010).
62. Audeh, M. W. et al. Oral poly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2 mutations and recurrent ovarian cancer: a proof-of-concept trial. Lancet 376, 245–251 (2010).
63. Perou, C. M. et al. Molecular portraits of human breast tumours. Nature 406, 747–752 (2000).
64. Sørlie, T. et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl Acad. Sci. USA 98, 10869–10874 (2001).
65. Rakha, E. A., Reis-Filho, J. S. & Ellis, I. O. Basal-like breast cancer: a critical review. J. Clin. Oncol. 26, 2568–2581 (2008).
66. Ossovskaya, V., Koo, I. C., Kaldjian, E. P., Alvares, C. & Sherman, B. M. Upregulation of poly (ADP-Ribose) polymerase-1 (PARP1) in triple-negative breast cancer and other primary human tumor types. Genes Cancer 1, 812–821 (2010).
67. Bertucci, F. et al. How basal are triple-negative breast cancers? Int. J. Cancer 123, 236–240 (2008).
68. Gonzalez-Angulo, A. M. et al. Incidence and outcome of BRCA mutations in unselected patients with triple receptor-negative breast cancer. Clin. Cancer Res. 17, 1082–1089 (2011).
69. Hartman, A. R. et al. Prevalence of BRCA mutations in an uselected population of triple-negative breast cancer. Cancer 118, 2787–2795 (2011).
70. Wang, J. et al. Poly(ADP-ribose) polymerase-1 down-regulates BRCA2 expression through the BRCA2 promoter. J. Biol. Chem. 283, 36249–36256 (2008).
71. Nielsen, T. O. et al. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin. Cancer Res. 10, 5367–5374 (2004).
72. Graeser, M. et al. A marker of homologous recombination predicts pathologic complete response to neoadjuvant chemotherapy in primary breast cancer. Clin. Cancer Res. 16, 6159–6168 (2010).
73. Fong, P. C. et al. Poly(ADP)-ribose polymerase inhibition: frequent durable responses in BRCA carrier ovarian cancer correlating with platinum-free interval. J. Clin. Oncol. 28, 2512–2519 (2010).
74. Workman, P. Auditing the pharmacological accounts for Hsp90 molecular chaperone inhibitors: unfolding the relationship between pharmacokinetics and pharmacodynamics. Mol. Cancer Ther. 2, 131–138 (2003).
75. Hastak, K., Alli, E. & Ford, J. M. Synergistic chemosensitivity of triple-negative breast cancer cell lines to poly(ADP-ribose) polymerase inhibition, gemcitabine, and cisplatin. Cancer Res. 70, 7970–7980 (2010).
76. US National Library of Medicine. Clinicaltrials.gov [online], http://clinicaltrials.gov/show/NCT01213381
77. Yardley, D. A. et al. A phase II trial of gemcitabine/carboplatin with or without trastuzumab in the first-line treatment of patients with metastatic breast cancer. Clin. Breast Cancer 8, 425–431 (2008).
78. Loesch, D. et al. Phase II trial of gemcitabine/carboplatin (plus trastuzumab in HER2-positive disease) in patients with metastatic breast cancer. Clin. Breast Cancer 8, 178–186 (2008).
79. Fojo, T., Amiri-Kordestani, L. & Bates, S. E. Potential pitfalls of crossover and thoughts on iniparib in triple-negative breast cancer. J. Natl Cancer Inst. 103, 1738–1740 (2011).
80. Burzykowski, T. et al. Evaluation of tumor response, disease control, progression-free survival, and time to progression as potential surrogate end points in metastatic breast cancer. J. Clin. Oncol. 26, 1987–1992 (2008).
81. Miller, K. et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N. Engl. J. Med. 357, 2666–2676 (2007).
82. Robert, N. J. et al. RIBBON-1: randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab for first-line treatment of human epidermal growth factor receptor 2-negative, locally recurrent or metastatic breast cancer. J. Clin. Oncol. 29, 1252–1260 (2011).
83. Anders, C. K. et al. TBCRC018: phase II study of iniparib plus chemotherapy to treat triple-negative breast cancer (TNBC) central nervous system (CNS) metastases (mets) [abstract 515]. J. Clin. Oncol. 31 (Suppl.), a515 (2013).
AcknowledgementsThe Drug Development Unit of the Royal Marsden NHS Foundation Trust and The Institute of Cancer Research is supported in part by a programme grant from Cancer Research UK. Support was also provided by the Experimental Cancer Medicine Centre (to The Institute of Cancer Research) and the National Institute for Health Research Biomedical Research Centre (jointly to the Royal Marsden NHS Foundation Trust and The Institute of Cancer Research).
Author contributionsAll authors researched data for the article and made a substantial contribution to discussions of the content and contributed to writing the manuscript. J. Mateo, M. Ong, and J. S. de Bono reviewed and edited the manuscript before submission.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved