application for leave of absence - northeastern.edu · family leave for personal illness or family...
TRANSCRIPT
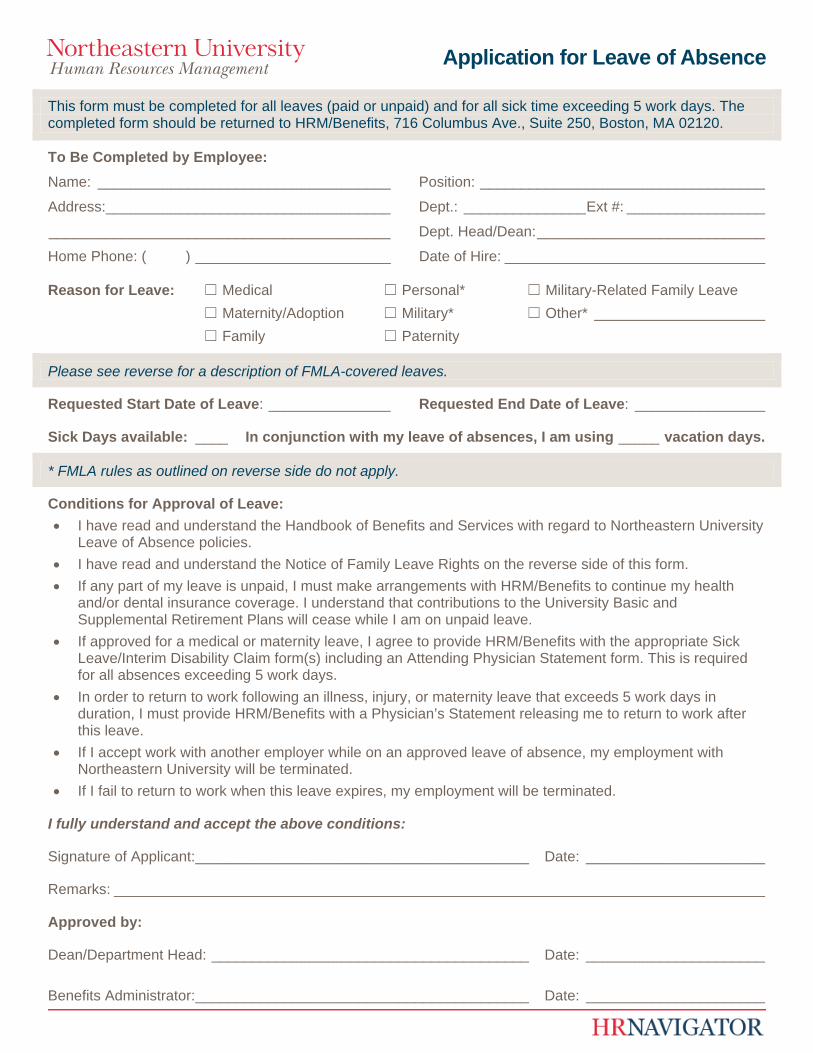
Application for Leave of Absence
This form must be completed for all leaves (paid or unpaid) and for all sick time exceeding 5 work days. The completed form should be returned to HRM/Benefits, 716 Columbus Ave., Suite 250, Boston, MA 02120.
To Be Completed by Employee:
Name: ____________________________________ Position: ___________________________________
Address: ___________________________________ Dept.: _______________ Ext #: _________________
__________________________________________ Dept. Head/Dean: ____________________________
Home Phone: ( ) ________________________ Date of Hire: ________________________________
Reason for Leave: ☐ Medical ☐ Personal* ☐ Military-Related Family Leave
☐ Maternity/Adoption ☐ Military* ☐ Other* _____________________
☐ Family ☐ Paternity
Please see reverse for a description of FMLA-covered leaves.
Requested Start Date of Leave: _______________ Requested End Date of Leave: ________________
Sick Days available: ____ In conjunction with my leave of absences, I am using _____ vacation days.
* FMLA rules as outlined on reverse side do not apply.
Conditions for Approval of Leave:
I have read and understand the Handbook of Benefits and Services with regard to Northeastern University Leave of Absence policies.
I have read and understand the Notice of Family Leave Rights on the reverse side of this form.
If any part of my leave is unpaid, I must make arrangements with HRM/Benefits to continue my health and/or dental insurance coverage. I understand that contributions to the University Basic and Supplemental Retirement Plans will cease while I am on unpaid leave.
If approved for a medical or maternity leave, I agree to provide HRM/Benefits with the appropriate Sick Leave/Interim Disability Claim form(s) including an Attending Physician Statement form. This is required for all absences exceeding 5 work days.
In order to return to work following an illness, injury, or maternity leave that exceeds 5 work days in duration, I must provide HRM/Benefits with a Physician’s Statement releasing me to return to work after this leave.
If I accept work with another employer while on an approved leave of absence, my employment with Northeastern University will be terminated.
If I fail to return to work when this leave expires, my employment will be terminated.
I fully understand and accept the above conditions:
Signature of Applicant: _________________________________________ Date: ______________________
Remarks: ________________________________________________________________________________
Approved by:
Dean/Department Head: _______________________________________ Date: ______________________
Benefits Administrator: _________________________________________ Date: ______________________
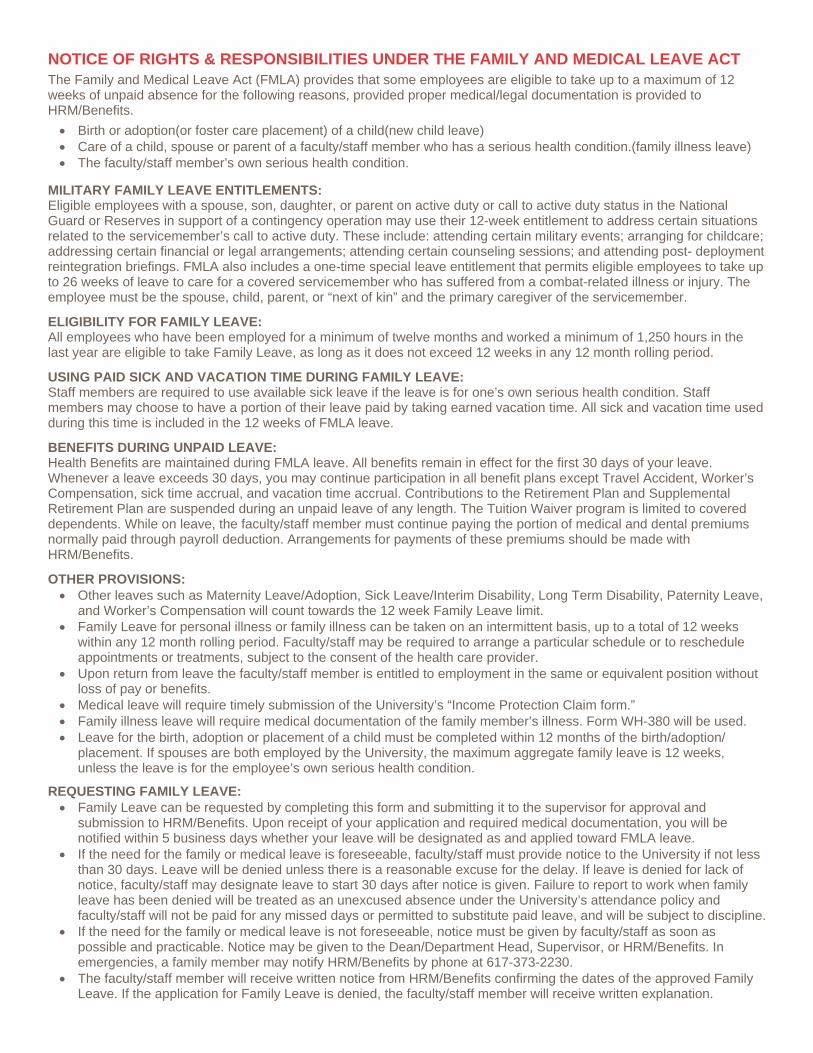
NOTICE OF RIGHTS & RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT The Family and Medical Leave Act (FMLA) provides that some employees are eligible to take up to a maximum of 12 weeks of unpaid absence for the following reasons, provided proper medical/legal documentation is provided to HRM/Benefits.
Birth or adoption(or foster care placement) of a child(new child leave) Care of a child, spouse or parent of a faculty/staff member who has a serious health condition.(family illness leave) The faculty/staff member’s own serious health condition.
MILITARY FAMILY LEAVE ENTITLEMENTS: Eligible employees with a spouse, son, daughter, or parent on active duty or call to active duty status in the National Guard or Reserves in support of a contingency operation may use their 12-week entitlement to address certain situations related to the servicemember’s call to active duty. These include: attending certain military events; arranging for childcare; addressing certain financial or legal arrangements; attending certain counseling sessions; and attending post- deployment reintegration briefings. FMLA also includes a one-time special leave entitlement that permits eligible employees to take up to 26 weeks of leave to care for a covered servicemember who has suffered from a combat-related illness or injury. The employee must be the spouse, child, parent, or “next of kin” and the primary caregiver of the servicemember.
ELIGIBILITY FOR FAMILY LEAVE: All employees who have been employed for a minimum of twelve months and worked a minimum of 1,250 hours in the last year are eligible to take Family Leave, as long as it does not exceed 12 weeks in any 12 month rolling period.
USING PAID SICK AND VACATION TIME DURING FAMILY LEAVE: Staff members are required to use available sick leave if the leave is for one’s own serious health condition. Staff members may choose to have a portion of their leave paid by taking earned vacation time. All sick and vacation time used during this time is included in the 12 weeks of FMLA leave.
BENEFITS DURING UNPAID LEAVE: Health Benefits are maintained during FMLA leave. All benefits remain in effect for the first 30 days of your leave. Whenever a leave exceeds 30 days, you may continue participation in all benefit plans except Travel Accident, Worker’s Compensation, sick time accrual, and vacation time accrual. Contributions to the Retirement Plan and Supplemental Retirement Plan are suspended during an unpaid leave of any length. The Tuition Waiver program is limited to covered dependents. While on leave, the faculty/staff member must continue paying the portion of medical and dental premiums normally paid through payroll deduction. Arrangements for payments of these premiums should be made with HRM/Benefits.
OTHER PROVISIONS: Other leaves such as Maternity Leave/Adoption, Sick Leave/Interim Disability, Long Term Disability, Paternity Leave,
and Worker’s Compensation will count towards the 12 week Family Leave limit. Family Leave for personal illness or family illness can be taken on an intermittent basis, up to a total of 12 weeks
within any 12 month rolling period. Faculty/staff may be required to arrange a particular schedule or to reschedule appointments or treatments, subject to the consent of the health care provider.
Upon return from leave the faculty/staff member is entitled to employment in the same or equivalent position without loss of pay or benefits.
Medical leave will require timely submission of the University’s “Income Protection Claim form.” Family illness leave will require medical documentation of the family member’s illness. Form WH-380 will be used. Leave for the birth, adoption or placement of a child must be completed within 12 months of the birth/adoption/
placement. If spouses are both employed by the University, the maximum aggregate family leave is 12 weeks, unless the leave is for the employee’s own serious health condition.
REQUESTING FAMILY LEAVE: Family Leave can be requested by completing this form and submitting it to the supervisor for approval and
submission to HRM/Benefits. Upon receipt of your application and required medical documentation, you will be notified within 5 business days whether your leave will be designated as and applied toward FMLA leave.
If the need for the family or medical leave is foreseeable, faculty/staff must provide notice to the University if not less than 30 days. Leave will be denied unless there is a reasonable excuse for the delay. If leave is denied for lack of notice, faculty/staff may designate leave to start 30 days after notice is given. Failure to report to work when family leave has been denied will be treated as an unexcused absence under the University’s attendance policy and faculty/staff will not be paid for any missed days or permitted to substitute paid leave, and will be subject to discipline.
If the need for the family or medical leave is not foreseeable, notice must be given by faculty/staff as soon as possible and practicable. Notice may be given to the Dean/Department Head, Supervisor, or HRM/Benefits. In emergencies, a family member may notify HRM/Benefits by phone at 617-373-2230.
The faculty/staff member will receive written notice from HRM/Benefits confirming the dates of the approved Family Leave. If the application for Family Leave is denied, the faculty/staff member will receive written explanation.