appendicitis management protocol echazarreta-gallego … · ultrasonography to detect acute...
TRANSCRIPT

APPENDICITIS
MANAGEMENT
PROTOCOL
Echazarreta-
Gallego et al.
Surgery Department Hospital Clínico Universitario de Zaragoza

1
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
APPENDICITIS MANAGEMENT PROTOCOL
AUTHORS
Echazarreta-Gallego, Estíbaliz. MD
Elía-Guedea, Manuela. PhD
Córdoba-Díaz de Laspra, Elena. PhD
Ramírez-Rodríguez, Jose Manuel. PhD
Gracia-Solanas, Jose Antonio. PhD
Allué-Cabañuz, Marta. MD
Gascón-Domínguez, María de los Ángeles. MD
Millán-Gallizo, Guillermo. MD
Aguilella-Diago, Vicente. PhD

2
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
INDEX
1. Introduction 1.2. HCUZ’S Situation
3 3
2. Protocol’s objectives
4
3. Care process. Diagram
6
4. Protocol development 4.1 Diagnosis 4.2 Treatment
7 7
9
5. Conclusions
17
6.Other references 17
7. Annexes 7.1 Alvarado Score 7.2 AIR Score 7.3 Diagram 7.4 Caprini Score Model 7.5 Apfel Score
18 18
18
19
20
20
3
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
APPENDICITIS MANAGEMENT PROTOCOL
1. INTRODUCTION
Acute appendicitis (AA) is the most common cause of abdominal emergency surgery. The
lifetime risk of developing an AA is approximately 7% with an estimated incidence of 90-10
cases /100,000 inhabitants / year. It can occur in any decade of life, but it is more prevalent in
adolescents and young adults. Surgical management is not free of complications and these
strongly increase the morbidity associated with the process, being the most common:
incisional infection with rates ranging from 3.3-10.3% and organ space infections (9.4%). Today
there is great variability within the surgical management and outcome of AA based on: surgical
approach and technique applied, type of antibiotic used, duration of antibiotherapy, surgical
wound closure, etc. Kelmer1 in 2012 published in Annals of Surgery that the standardization of
cares can achieve significant results in terms of reducing surgical site infection, hospital stay
and patient comfort.
1.2. HCUZ’S SITUATION:
In order to evaluate the results of a common emergency surgical procedure and searching for
improvement areas, we carried out a retrospective review of all patients undergoing surgery
for AA between January 2013 and March 2015 in the Department of Surgery of HCUZ (n = 415).
Of the 415 appendectomy practiced during this period, 85 patients presented postoperative
adverse events (20.5%), being the most common the postoperative ileus in 31 patients (7.5%).
The rate of wound infection was of 4.8% with an incidence of intraabdominal abscess of 4.8%.
We observed an increased frequency of incisional infection in open appendectomy group (OA)
compared with laparoscopic appendectomy (LA) (2% vs 11.7%) being statistically significant (p
<0.000). There was no significant difference in the incidence of intra-abdominal abscess when
analyzing laparoscopic appendectomy (LA) 5.1% vs. open appendectomy (OA) 4.2% (p=0.692)
nor in the presence of ileus (7.8% vs 6.7). The average length of hospital stay in days was of
3.82 days (+/- 3,707).
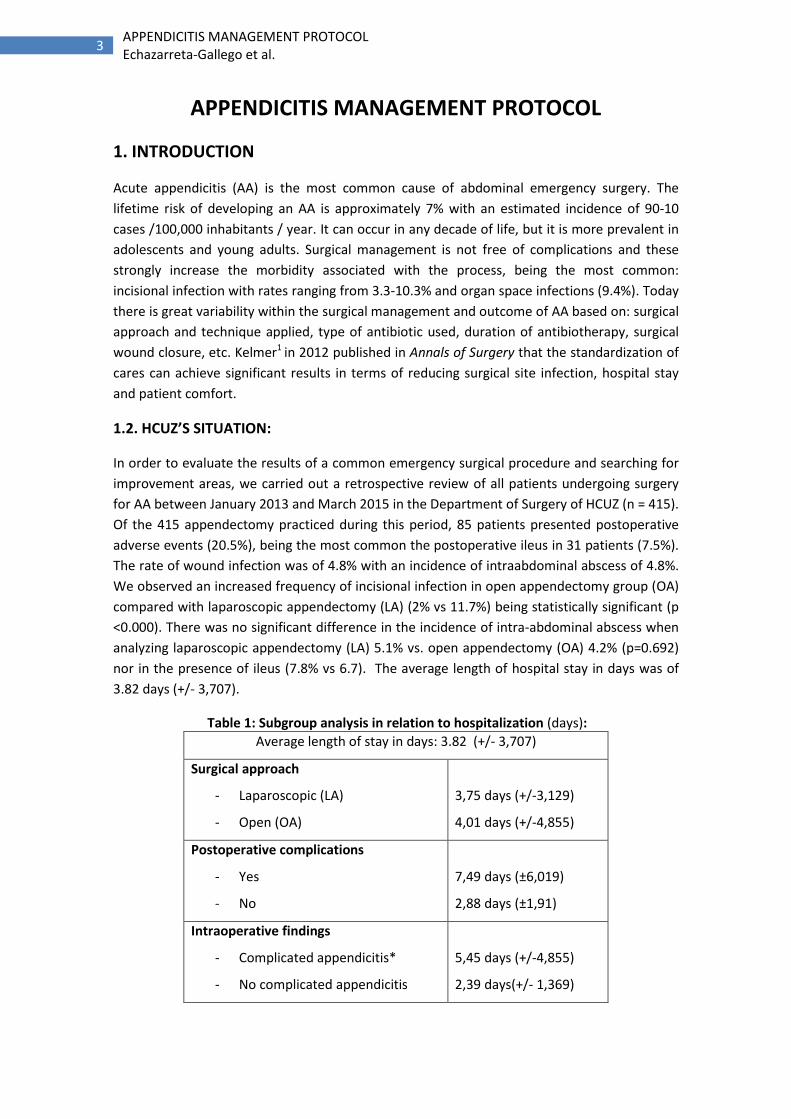
Table 1: Subgroup analysis in relation to hospitalization (days):
Average length of stay in days: 3.82 (+/- 3,707)
Surgical approach
- Laparoscopic (LA)
- Open (OA)
3,75 days (+/-3,129)
4,01 days (+/-4,855)
Postoperative complications
- Yes
- No
7,49 days (±6,019)
2,88 days (±1,91)
Intraoperative findings
- Complicated appendicitis*
- No complicated appendicitis
5,45 days (+/-4,855)
2,39 days(+/- 1,369)

4
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
* Complicated appendicitis included: gangrenous appendicitis, perforated appendicitis, appendicular “mass” or +/- presence of located or generalized peritonitis.
2. PROTOCOL’S OBJECTIVES
Currently, the goal of clinical practice include quality cares that improve patient`s safety. This
system is based on reducing to an acceptable minimum all the unnecessary procedures or
actions associated with health care that may cause harm. In this point the main aims of this
protocol are:
- Standardizing the management of a common clinical practice, adapting this protocol to
the evidence published in the literature.
- Improving clinical results by reducing postoperative complications. The percentage of
patients who presented complications was 20.5% (n = 85). The most frequent
complications were: postoperative ileus (n=31 patients, 7.5%), wound infection (n= 20,
4.8%) and intra-abdominal abscess (n= 20, 4.8%). Global data about surgical site
infection are similar to those reported in the literature, however if wound infection is
analyzed in specific subgroups we observed it was significantly more frequent (2% vs
11.7%) in the OA versus LA group (p <0.000). On the other hand there was no
significant difference (p 0.692) when analyzing the incidence of intra-abdominal
abscess depending on the surgical approach (5.1% LA vs 4.2% OA). At this point the
purpose of our guide is to reduce the rate of surgical wound infection and intra-
abdominal abscess by encouraging the use of the laparoscopic access and applying the
antibiotic prophylaxis recommendations established by our hospital PROA group.
- Improving length of hospital stay. The average stay is an indicator of effectiveness that
evaluates the time that the hospital needs to perform the diagnosis and treatment of
diseases. The average stay of our series was of 3.82 days (+/- 3.707). Comparing days
of hospitalization in the different subgroups described in table nº 1 we observed
higher hospitalization in OA (4.01 days +/- 4,855) vs 3.75 days +/- 3,129 in LA group;
we also found higher hospital stay in the group of patients who had suffered
postoperative complications (7.49 ± 6.019) vs does who had not undergone
postoperative complications (2.88 ± 1.91), and in those patients defined as
"complicated appendicitis" grouped in the intraoperative finding (5.45 +/- 4,855 days)
vs those described as "no complicated" (2.39 +/- 1.369 days). We consider this
parameter an important value of the clinical effectiveness, since complications and
adverse effects prolong the hospitalization.
In response to these issues, we propose three paths:
Early discharge within 24 hours that has proven to be safe and feasible if
adequate patient selection is made. We consider that this range of action will
benefit patients with non-complicated appendicitis and no comorbidities, even
though nowadays, some series describe a rapid discharged similar to an

5
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
ambulatory process (<12h) with good results in terms of readmission and
morbidity2
Hospitalization increases with postoperative complications, so the
introduction of measures such as: optimization of the patient, appropriate
antibiotic treatment, laparoscopic approach etc. would decrease complications
resulting in a reduction of stay.
In our series comparing with the literature, there was a high rate of AA defined
as complicated appendicitis that is directly related with a longer
hospitalization rate. Another purpose for the implementation of this protocol
is to adequate timings and medical care, decreasing the interval from the
evaluation of the patient to diagnosis by trained personnel at the emergency
department, offering early consultation with the surgical team on guard that
should be prepared to apply a suitable surgical care.
Another parameter we think should be considered to evaluate the quality of care is the costs
of the process. Appendectomy is a surgical procedure with an average cost of 3.106,00€
(SALUD INFORMA). Each day of hospitalization represents 685,00€, a specialized care
consultation 49,00€ and consultation in the emergency department 136,00€. In our series 330
patients (79.5%) showed no postoperative complications with 2.88 (± 1.91) hospitalization
days, in this group of patients, globally 424,974€ could be save, considering a 24 hours
reduction stay. On the other side, it is well known that postoperative complications increases
health spending. So surgical site infection or intaabdominal infection involves additional costs
resulting local treatment, antibiotics, prolonged hospital stay and/or requiring in some cases
reoperation.
Many factors contribute in the pathogenesis of adverse events, some of which are hard-coded
(comorbidities, age, time between beginning of process and consultation), but it is also well
known that many others could contribute to improve a safer clinical practice reducing costs
when applying adequate corrective actions or improvement areas.
6
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
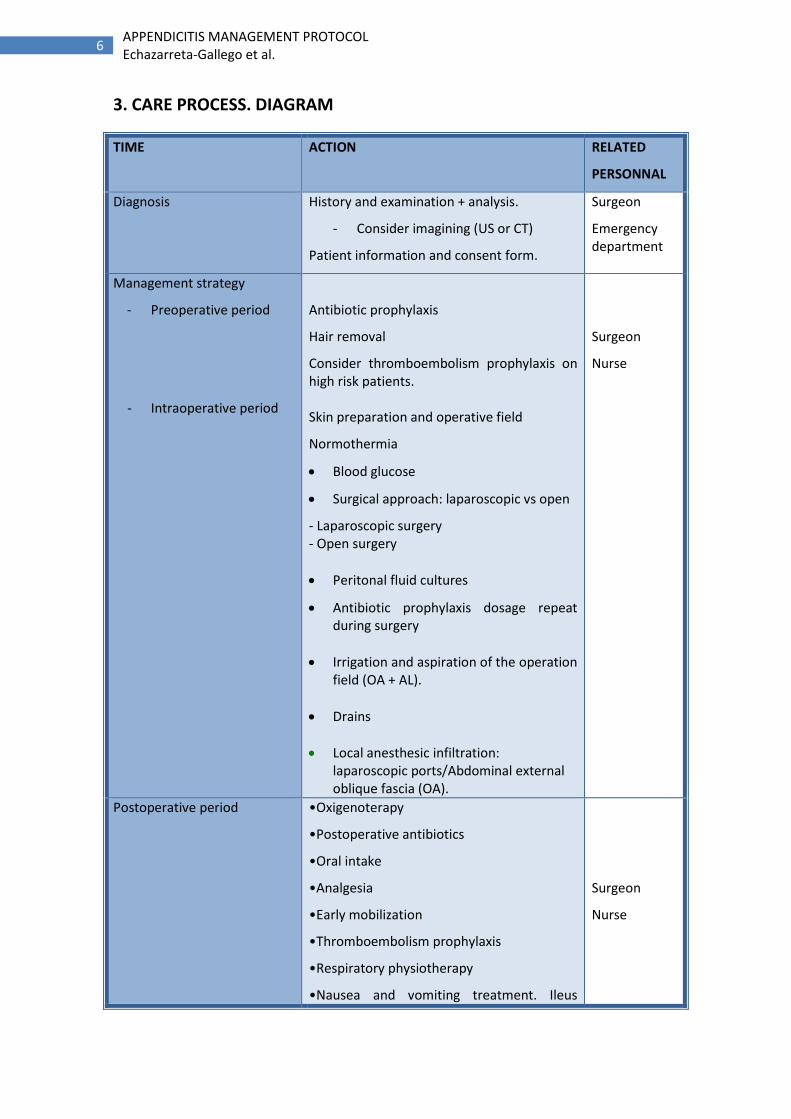
3. CARE PROCESS. DIAGRAM
TIME ACTION RELATED
PERSONNAL
Diagnosis
History and examination + analysis.
- Consider imagining (US or CT)
Patient information and consent form.
Surgeon
Emergency department
Management strategy
- Preoperative period
- Intraoperative period
Antibiotic prophylaxis
Hair removal
Consider thromboembolism prophylaxis on high risk patients. Skin preparation and operative field
Normothermia
Blood glucose
Surgical approach: laparoscopic vs open
- Laparoscopic surgery - Open surgery
Peritonal fluid cultures
Antibiotic prophylaxis dosage repeat during surgery
Irrigation and aspiration of the operation field (OA + AL).
Drains
Local anesthesic infiltration: laparoscopic ports/Abdominal external oblique fascia (OA).
Surgeon
Nurse
Postoperative period
•Oxigenoterapy
•Postoperative antibiotics
•Oral intake
•Analgesia
•Early mobilization
•Thromboembolism prophylaxis
•Respiratory physiotherapy
•Nausea and vomiting treatment. Ileus
Surgeon
Nurse

7
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
prophylaxis
Discharged •Depending on severity:
- Non complicated: 24 h - Complicated appendicitis: once
they tolerate a regular diet and there is no other complication
•Offer care instruction
•Surgical postoperative consultation
appointment
4. PROTOCOL DEVELOPMENT
4.1 Diagnosis
The ideal diagnostic method for appendicitis, which offers high accuracy while avoiding
adverse effects (radiation), has not been achieved yet despite the variety of available tools.
The percentage of negative appendectomies was located historically in the 15% having
reduced to 10% after the introduction of computed tomography (CT) in the diagnosis.
o Physical examination: throughout history, there have been described numerous clinical
signs associated with AA that facilitate the diagnostic, however they lack adequate
sensitivity and specificity.
o Blood analysis: No analytical marker has a sensitivity and specificity adequate to confirm
the diagnosis. The moderate increase of leukocytes with left shift is the most common
finding, present in 80% of patients. Other markers of acute inflammation such as C-
reactive protein CRP or procalcitonin PCT may be useful. It is recommended to perform a
pregnancy test in the differential diagnosis in all women of childbearing age.
o Risk scales: these scales combine different parameters trying to get a more accurate
diagnosis. Among the most widely used scale is Alvarado (Annex 1), several studies have
demonstrated a high sensitivity but low specificity. The latest AIR score (Appendicitis
Inflammatory Response) (Annex 2) has greater precision than the scale of Alvarado.
o Ultrasound: the data that best relates to AA is an image of cecal appendix > 6 mm. The US
in the diagnosis of AA has moderate sensitivity (86%- 95%, CI 83-88) and specificity (81%,
CI 78-84).
Kollar D, McCartan DP, Bourke M, Cross KS, Dowdall J. Predicting acute appendicitis? A comparison of the Alvarado score, the appendicitis inflammatory response score and clinical assessment. World J Surg 2015; 39: 104–09
Terasawa T, Blackmore CC, Bent S, Kohlwes RJ. Systematic review: computed tomography and ultrasonography to detect acute appendicitis in adults and adolescents. Ann Intern Med 2004;141: 537–46.

8
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
o TC: image findings suggestive of acute appendicitis is appendiceal thickening greater than
6 mm and / or occlusion of light, appendiceal wall thickening, rarefaction of
periappendiceal fat appendicolith presence (25% of patients). The sensitivity of this
imaging test is 93%.
In this diagram we propose the attitude for diagnostic and therapeutic management in
patients having pain in right lower quadrant. (Annex 3)
PATIENT INFORMATION
Once established the indication for surgery the patient must be informed of the treatment
options available and the possible risks arising. The information provided must be adapted to
the characteristics of the patient.
4.2 TREATMENT
Appendectomy remains the gold standard treatment of appendicitis approved in all clinical
guidelines and recommended by the American College of Surgeons, the Association of
Digestive Tract Surgery and the World Society of Emergency Surgery. The alternative non-
operative approach (conservative antibiotic treatment) has been studied in detail in many
meta-analyzes and systematic reviews, including Cochrane 2011, whose authors concluded
that appendectomy remains the standard treatment and antibiotic treatment would be
relegated to patients or specific conditions in which the surgery is contraindicated.
4.2.1 Preoperative period
4.2.1.1 Antibiotic prophylaxis
Bhangu A, Søreide K, Di Saverio S, Assarsson JH, Drake FT. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet. 2015 Sep 26;386(10000):1278-87. doi: 10.1016/S0140-6736(15)00275-5.
Maessen J, Dejong CH, Hausel J, et al. A protocol is not enough to implement an enhanced recovery programme for colorectal resection. Br J Surg 2007;94:224-31
- Sartelli M, Viale P, Catena F, Ansaloni L, Moore E, Malangoni M, Moore FA, Velmahos G, Coimbra R, Ivatury R, Peitzman A, Koike K, Leppaniemi A, Biffl W, Burlew CC, Balogh ZJ, Boffard K, Bendinelli C, Gupta S, Kluger Y, Agresta F, Di Saverio S, Wani I, Escalona A, Ordonez C, Fraga GP, Junior GA, Bala M, Cui Y, Marwah S, Sakakushev B, Kong V, Naidoo N, Ahmed A, Abbas A, Guercioni G, Vettoretto N, Díaz-Nieto R, Gerych I, TranàC, Faro MP, Yuan KC, Kok KY, Mefire AC, Lee JG, Hong SK, Ghnnam W, Siribumrungwong B, Sato N, Murata K, Irahara T, Coccolini F, Segovia Lohse HA, Verni A, Shoko T. 2013 WSES guidelines for management of intra-abdominal infections. World J Emerg Surg. 2013;8(1):3. Epub 2013 Jan 8.
- Flum DR. Clinical practice. Acute appendicitis--appendectomy or the "antibiotics first" strategy. Engl J Med. 2015 May;372(20):1937-43
- Wilms IM, de Hoog DE, de Visser DC, Janzing HM. Appendectomy versus antibiotic treatment for acute appendicitis. Cochrane Database Syst Rev. 2011 Nov 9;(11):CD008359. doi: 10.1002/14651858.CD008359.pub2.

9
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
The administration of prophylactic antibiotics is critical in the prevention of surgical wound
infection and intra-abdominal abscess3. The most common flora in this pathology is the enteric
gram-negative bacilli, anaerobes and enterococci (E. coli, Kleibsiella, Proteus and Bacteroides).
We recommend the following instructions:
* Risk criteria for E. coli or Klebsiella ESBL spp productor: severe / shock sepsis, previous use of quinolones or cephalosporins,
repetive urinary tract infection, urinary catheter, diabetes mellitus
The Cochrane systematic review on "Antibiotic treatment vs placebo in the prevention of
infection postappendectomy" concluded that:
a) Antibiotic prophylaxis in the prevention of postoperative complications in appendectomy is
effective if it is administered pre, per or postoperatively. It should be considered for routine
use in emergency appendectomy.
b) The results of the meta-analysis showed that a single antibiotic dose has the same impact as
multiple doses. In order to reduce costs, toxicity and the risk of developing bacterial resistance
it is desirable to establish the shortest and effective prophylactic regimen to prevent
postoperative complications.
c) In patients in whom perforated appendicitis is suspected, empirical antibiotic treatment will
be administrated following the above recommendations and it must be adjusted if necessary
to culture results.
4.2.1.3 Time intervention
According to the latest "Up to date" recommendation published, once the diagnosis of
appendicitis is established early surgery should be advised in order to prevent progression to
perforation. Prior to surgery, hydration fluid must be provided, and electrolyte disturbances
should be corrected.
Daskalakis K, Juhlin C, Påhlman L. The use of pre- or postoperative antibiotics in surgery for appendicitis: a systematic review. Scand J Surg. 2014 Mar;103(1):14-20. doi: 10.1177/1457496913497433. Epub 2013 Sep 20.
Andersen BR, Kallehave FL, Andersen HK. Antibiotics versus placebo for prevention of
postoperative infection after appendicectomy. Cochrane Data base Syst Rev. 2005 Jul
20;(3):CD001439.
Papandria D, Goldstein SD, Rhee D, et al. Risk of perforation increases with delay in recognition
and surgery for acuteappendicitis. J Surg Res 2013;184:723—9.
Amoxicillin-clavulanate 2gr ev 5 min (before surgery)
Risk of ESBL*: ertapenem ev 1g
Allergic patients: Clindamicine 600 mg + Gentamicine 2 mg/kg (30 min before anhestesic induction).

10
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
However, some epidemiological studies have found no correlation between a delay of 6-12
hours from the time of hospital admission and surgery with the rate of perforation and / or
postoperative complications.
4.2.1.3 Hair Removal
Hair removal has not been shown to reduce the incidence of surgical infections. In cases where
necessary, clippers are recommended instead of conventional shaving.
4.2.2 INTRAOPERATIVE
4.2.2.1 Preparation of the skin and surgical field
Skin antisepsis must be made in concentric circles around surgical incision with chlorhexidine-
alcohol 1% solution
It is recommended to make skin antisepsis with an agent that contains alcohol unless there is a
contraindication. Alcohol is a powerful bactericide, effective in skin antisepsis but not if used
alone. It could be achieved a quick, effective and cumulative antisepsis in combination with
clorehixidine or iodine-solution.
4.2.2.2 Normothermia
Ingraham AM, Cohen ME, Bilimoria KY, et al. Effect of delay tooperation on outcomes in adults
with acute appendicitis. Arch Surg 2010;145:886—92.
Drake FT, Mottey NE, Farrokhi ET. Time to appendectomy and risk of perforation in acute
appendicitis. JAMA Surg2014;149:837—44.
Tanner J, Woodings D, Moncaster K. Preoperative hair removal to reduce surgical site infection. Cochrane Database Syst Rev. 2006 Jul 19;(3):CD004122.
Lefebvre A, Saliou P, Lucet JC, Mimoz O, Keita-Perse O, Grandbastien B, Bruyère F, Boisrenoult P, Lepelletier D, Aho-Glélé LS; French study group for the preoperative prevention of surgical site infections. Preoperative hair removal and surgical site infections: network meta-analysis of randomized controlled trials. J Hosp Infect. 2015 Oct;91(2):100-8. doi: 10.1016/j.jhin.2015.06.020. Epub 2015 Aug 4.
.
Dumville JC, McFarlane E, Edwards P, Lipp A, Holmes A. Preoperative skin antiseptics for
preventing surgical wound infections after clean surgery.Cochrane DatabaseSyst Rev. 2013 Mar
28;3:CD003949. doi: 10.1002/14651858.CD003949.pub3.
Anderson DJ, Podgorny K, Berríos-Torres SI, Bratzler DW, Dellinger EP, Greene L, Nyquist AC,
Saiman L, Yokoe DS, Maragakis LL, Kaye KS. Strategies to prevent surgical site infections in acute
care hospitals: 2014 update. Infect Control HospEpidemiol. 2014 Jun;35(6):605-27. doi:
10.1086/676022.
Darouiche RO, Wall MJ Jr, Itani KM, Otterson MF, Webb AL, Carrick MM, Miller HJ, Awad SS,
Crosby CT, Mosier MC, Alsharif A, Berger DH Chlorhexidine-Alcohol versus Povidone-Iodine for
Surgical-Site Antisepsis. N Engl J Med. 2010 Jan 7;362(1):18-26. doi: 10.1056/NEJMoa0810988.

11
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
Normothermia reduces some surgery related complications as intraoperative bleeding or SSI
(surgical site infection), decreasing the hospital stay. Hypothermia impairs the action of
neutrophils and causes subcutaneous tissue vasoconstriction and hypoxia. All these facts could
increase blood loss, the development of bruising in the wound, aspects that increase the rate
of SSI. The use of warming devices is recommended to prevent hypothermia.
4.2.2.3 Glycaemia
Postoperative hyperglycemia increases complications rate. During surgery, blood glucose
should be monitored. The maintenance of normoglycemia has a positive outcome in the
postoperative period. The goal of treatment of postoperative hyperglycemia in diabetic
patients is not formally defined, however values below 110 mg / dl or greater than 150 mg / dl
seem to be detrimental and should be avoided.
4.2.2.4 Technique
Laparoscopic vs open approach
The laparoscopic approach (LA) has gradually increased in recent years. The latest Cochrane
review published in 2010 concluded that laparoscopy offers advantages over open surgery
(OA) if the clinical circumstances, surgical team and proper equipment is available. The use of
laparoscopy is especially recommended for young women, obese and active workers.
There have also been observed advantages with the LA in elderly population. Harrel
(observational cohort) described in uncomplicated appendicitis a lower hospital stay (4.6
versus 7.3 days), less requirement of intermediate care (91 versus 79%), less complications (13
versus 22%) and lower mortality (0.4 versus 2.1%) in the laparoscopy group compared with
OA. He also described in the group of patients with perforated appendicitis treated by LA a
Anderson DJ, Podgorny K, Berríos-Torres SI, Bratzler DW, Dellinger EP, Greene L, Nyquist AC, Saiman L,
Yokoe DS, Maragakis LL, Kaye KS. Strategies to prevent surgical site infections in acute care hospitals:
2014 update. Infect Control HospEpidemiol. 2014 Jun;35(6):605-27. doi: 10.1086/676022.
Melling AC, Ali B, Scott EM, Leaper DJ. Effects of preoperative warming on the incidence of wound
infection after clean surgery: a randomised controlled trial. Lancet. 2001 Sep 15;358(9285):876-80.
Wong PF, Kumar S, Bohra A, Whetter D, Leaper DJ.Randomized clinical trial of perioperative systemic
warming in major elective abdominal surgery. Br J Surg 2007;94(4):421-6198.
Sajid MS, Shakir AJ, Khatri K, Baig MK.The role of perioperative warming in surgery: a Systematic
Review. Sao Paulo Med J 2009;127(4):231-7200.
Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic versus open surgery for suspected
appendicitis. Cochrane Data base Syst Rev. 2010 Oct 6;(10): CD001546. doi:
10.1002/14651858.CD001546.pub3.
Harrell AG, Lincourt AE, Novitsky YW, Rosen MJ, Kuwada TS, Kercher KW, Sing RF, Heniford BT.
Advantages of laparoscopic appendectomy in the elderly. Am Surg. 2006 Jun;72(6):474-80.

12
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
decreased hospital stay (6.8 versus 9.0 days) a lower rate of intermediate care when discharge
home (87 versus 71% ) with equivalent rates of mortality when compared to OA.
Laparoscopic approach
The patient is placed supine on the operating table with his left arm positioned along the body.
The monitor is located on the right side of the patient.
- Placement of ports: there are several options but all of them must respect the principle of
triangulation of instruments and appendix. One method is to place a 12 mm periumbilical port
and two-port of 5 mm in left lower quadrant and suprapubic midline. For retrocecale
appendicitis better exposure is achieved by situating a 5mm trocar in the epigastric region.
- Mobilization and resection:
After identifying the appendix, adhesions if necessary are released and the structure is
continued until its insertion in the cecal base. It is then identified the appendiceal artery and
sectioned by hemoclips, coagulation or stapler (GIA). In case of using the stapler for
mesoappendix ligation, a single reload including mesoappendix and appendix must be used
whenever possible.
The method for closing and transecting the appendix stump depends on the intraoperative
findings and experience of the surgeon. The use of endoloops has demonstrated safe results
comparable to the endo-stapler in observational studies.
Evaluating the effectiveness cost, the use of endoloops or clips is recommended in single
appendicecal inflammation conditions with appendicular based less than 16 mm. If there is
inflammation of the base of the cecum it is advisable to employ endo-stapler.
- Removing the surgical specimen in bag
It is recommend to extract the surgical specimen in a plastic bag to prevent contamination of
the surgical wound trocar.
Open approach
- A curvilinear incision on McBurney point in the outer third of the line between the superior
iliac spine and the navel is recommended. Some authors recommend a transverse incision,
easily to extend. It is recommended to examine the patient after anesthetic induction and if
Galatioto C, Guadagni S, Zocco G, Mazzilo M, Bagnato C, Lippolis PV, Seccia M. Mesoappendix and appendix stump treatment in laparoscopic appendectomy: a retrospective study in 1084 patients. Ann Ital Chir. 2013 May-Jun;84(3):269-74.
Sahm M, Kube R, Schmidt S, Ritter C, Pross M, Lippert H. Current analysis of endoloops in appendiceal stump closure. SurgEndosc. 2011 Jan;25(1):124-9. doi: 10.1007/s00464-010-1144-5. Epub 2010 Jun 15.

13
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
any palpable mass corresponded to the inflammatory process appendicular incision must be
done above that mass.
- Mobilization and resection: after dissection of the subcutaneous tissue, longitudinally
sectioned external oblique fascia and muscle fibers are splitted to expose the peritoneum,
which is elevated prior section to prevent intestinal damage. The appendix is located, the
mesoappendix dissected and sectioned after making a ligature with an absorbable suture 3/0.
The cecal appendix is cut with a scalpel and the stump tied with a 2/0 absorbable suture stump
mucosa is coagulated with electrocautery. The appendiceal stump is inverted into the cecal
base with a purse string suture.
- Closure of surgical wound is performed by planes with a continuous 2/0 absorbable suture.
Wash-saline irrigation of each plane is performed and primary closure of the wound with
subcuticular sutures or staples are recommended.
4.2.2.5 Peritoneal fluid cultures
Taking peritoneal fluid cultures systematically in each intervention is controversial. It is
advisable to take in patients in whom there is a risk of ESBL or a possibility of failure of focus
control. However, in our hospital, we propose peritoneal fluid culture to identify the
responsible local flora and arrange epidemiological study.
4.2.2.6 Re-dosing antibiotic if necessary.
Although it is unusual in this type of intervention, it is recommended to re-dose if time exceed
twice the average life of the antibiotic or excessive blood loss occurs.
4.2.2.7 Irrigation and aspiration operative field
Irrigation / aspiration of the surgical field with saline solution is recommended in both open
and laparoscopic appendectomy. Volume of irrigation will be in relation with the degree of
peritonitis.
4.2.2.8 Drains
The use of drains is not recommended because they have not shown to decrease the rate of
wound infection and intra-abdominal abscess, increasing the length of hospital stay.
Soffer D, Zait S, Klausner J, Kluger Y. Peritoneal cultures and antibiotic treatment in patients with
perforated appendicitis. Eur J Surg. 2001 Mar;167(3):214-6.
Anderson DJ, Podgorny K, Berríos-Torres SI, Bratzler DW, Dellinger EP, Greene L, Nyquist AC,
Saiman L, Yokoe DS, Maragakis LL, Kaye KS. Strategies to prevent surgical site infections in acute
care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014 Jun;35(6):605-27. doi:
10.1086/676022..
14
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
4.2.2.3 Infiltration with local anesthetic
Although the studies are very heterogeneous it is convenient to infiltrate laparoscopic ports or
external oblique fascia in order to reduce the need for postoperative analgesia.
4.2.3 POSTOPERATIVE
4.2.3.1 Oxygen therapy
It is suggested to maintain adequate oxygen saturation. Infection of surgical wound is favored
in an atmosphere with low oxygen concentrations due to decreased microvascular flow that
alters the leukocyte function. Some studies have postulated that increasing the fraction of
inspired oxygen might improve neutrophil function by decreasing the incidence of surgical
wound infection.
4.2.3.2 Postoperative antibiotic
• The use of postoperative antibiotics on uncomplicated appendicitis is NOT suitable.
Uncomplicated cases of appendicitis are considered contaminated clean-surgery when the
infection site is removed, and therefore only require prophylaxis. Prolongation of antibiotic
Petrowsky H, Demartines N, Rousson V, Clavien PA. Evidence-based value of prophylactic
drainage in gastrointestinal surgery: a systematic review and meta-analyses. Ann Surg. 2004
Dec;240(6):1074-84; discussion 1084-5.
Cheng Y, Zhou S, Zhou R, Lu J, Wu S, Xiong X, Ye H, Lin Y, Wu T, Cheng N. Abdominal drainage to
prevent intra-peritoneal abscess after open appendectomy for complicated
appendicitis.Cochrane DatabaseSyst Rev. 2015 Feb 7;2:CD010168. doi:
10.1002/14651858.CD010168.pub2.
Joshi GP, Bonnet F, Kehlet H; PROSPECT collaboration.Evidence-based postoperative pain
management after laparoscopic colorectal surgery. Colorectal Dis. 2013 Feb;15(2):146-55. doi:
10.1111/j.1463-1318.2012.03062.x.
Ventham NT1, O'Neill S, Johns N, Brady RR, Fearon KC. Evaluation of novel local anesthetic
wound infiltration techniques for postoperative pain following colorectal resection surgery: a
meta-analysis. Dis Colon Rectum. 2014 Feb;57(2):237-50. doi: 10.1097/DCR.0000000000000006.
Vía Clínica de Recuperación Intensificada en Cirugía Abdominal (RICA). Grupo de Trabajo de la
Vía Clínica de Recuperación Intensificada en Cirugía Abdominal (RICA). Noviembre 2014.
Ministerio de Sanidad, Servicios Sociales e Igualdad/Instituto Aragonés de Ciencias de la Salud
Gottrup F. Oxygen in wound healing and infection. World J Surg. 2004 Mar;28(3):312-5. Epub
2004 Feb 17.
Hovaguimian F, Lysakowski C, Elia N, Tramèr MR. Effect of intraoperative high inspired oxygen
fraction on surgical site infection, postoperative nausea and vomiting, and pulmonary function:
systematic review and meta-analysis of randomized controlled trials. Anesthesiology. 2013
Aug;119(2):303-16. doi: 10.1097/ALN.0b013e31829aaff4.

15
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
treatment has not proven useful in preventing the onset of SSI and it may instead promote the
development of resistant microorganism and adverse effects such as diarrhea by antibiotics.
• In complicated appendicitis it is appropriated to extend the empirical antibiotic treatment
administration for 5 days. The Clinical Antibiotic Treatment Guide of our Hospital (HCUZ)
recommends the following administration:
The administration can be oral when
- Clinical syndrome is controlled and tolerance is present.
- The antimicrobial must have good oral bioavailability.
4.2.3.3 Diet
In patients with uncomplicated appendicitis diet might be started 6-8 hours after surgery.
Patients with peritonitis often associate postoperative ileus. Ileus is a temporary deficiency (at
least three days) of intestinal motility characterized by abdominal distension, absent bowel
sounds, accumulation of gas and liquid in bowel and delayed expulsion of flatus and
defecation. The only drug that has proven useful in the management of this adverse event is
the Almipovan (opioid antagonist), provided they are involved in the etiopathogenesis opiates.
In these patients the start of the diet is recommended when the intestinal motility is secured.
Andersen BR, Kallehave FL, Andersen HK. Antibiotics versus placebo for prevention of
postoperative infection after appendicectomy.Cochrane DatabaseSyst Rev. 2005 Jul
20;(3):CD001439.
Asociación Española de Cirujanos. Recomendaciones programa “Compromiso por la Calidad de
las Sociedades Científicas en España”. Ministerio de Sanidad, Servicios Sociales e Igualdad.
http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/pdf/ASOCIACION_ESP_CIRUJANOS_0
K.pdf
Coakley BA, Sussman ES, Wolfson TS, Bhagavath AS, Choi JJ, Ranasinghe NE, Lynn ET, Divino CM.
Postoperative antibiotics correlate with worse outcomes after appendectomy for nonperforated
appendicitis. J Am Coll Surg. 2011 Dec;213(6):778-83. doi: 10.1016/j.jamcollsurg.2011.08.018.
Epub 2011 Sep 29.
- Amoxicillin Clavulanate 1 g/8 h or (Cefotaxime 1 gr/8 h + metronidazole 500 mg/8 h) +/- gentamicine 5 mg/kg/day or amikacin 15 mg/kg/day
- Risk of ESBLs ESBL spp productor: severe / shock sepsis, previous use of quinolones or cephalosporins, repetive urinary tract infection, urinary catheter, diabetes mellitus: Ertapenem 1 gr/24 h ev
- Penicillin alergic: aztreonam 1 gr/ 8 h + metronidazole 500 mg/8h or tigecicline 100 mg 1 dose followed by 50 mg/12 h
16
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
4.2.3.4 Analgesia
Postsurgical analgesia intravenous regimen based on Paracetamol + NSAIDs. Promote the
employ of visual analog scale
4.2.3.5 Early mobilization
Immobilization after surgery is related to the occurrence of cardiovascular, respiratory and
thromboembolic complications and therefore prolonged hospital stay. Early mobilization has
been related with reduction of these complications and hospitalization time. Mobilization of
the patient is recommended after the first six hours postoperative.
4.2.3.6 Thromboembolic prophylaxis
The risk of postoperative deep vein thrombosis is not unifactorial. Its development is
influenced by patients intrinsic factors such as history, comorbidities etc. and others from the
surgical procedure itself. Despite many attempts to quantify this risk, there is no universal
method accepted. Caprini modified scale (Annex 4) was established by the guide ACCP11 in
2012 to build the risk of postoperative thromboembolic events.
Early mobilization is mandatory for patients with very low risk (Caprini 0). For low-risk (Caprini
1-2) mechanical prophylaxis with pneumatic compression stockings is prescribed. If the risk is
moderate (Caprini 3-4) the recommendation is based in the use of low molecular weight
heparins. When the risk is high (Caprini equal to or greater than 5) the use of low molecular
weight heparins with elastic stockings or mechanical compression is suggested.
4.2.3.7 Treatment of nausea and vomiting
Prophylaxis of nausea and vomiting during surgery should be performed after individual
evaluation with Apfel scale (Annex 5). If the patient has received prophylaxis, treatment should
begin with a different antiemetic drug from the initial one. If the patient has not required any
antiemetic drug, treatment might be started with low dose of ondansetron.
4.2.4 Discharge
Douglas Smink, David I Soybel.Management of acute appendicitis in adults. Uptodate
2015.www.uptodate.com
Vlug MS, Bartels SA, Wind J, Ubbink DT, Hollmann MW, Bemelman WA; Collaborative LAFA Study
Group. Which fast-track elements predict early recovery after colon cancer surgery? Colorectal
Dis. 2012;14(8):1001-8.
Henriksen MG, et al., Enforced mobilization,early oral feeding, and balanced analgesia improve
convalescence after colorectal surgery. Nutrition 2002;18(2):147-52
Kazemi-Kjellberg F, Henzi I, Tramèr MR. Treatment of established postoperative nausea and
vomiting: a quantitative systematic review. BMC Anesthesiol 2001;1:2-12

17
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
5. CONCLUSION
For uncomplicated appendicitis it is recommended early discharge within 24 hours if no signs
of complication or no presence of comorbidities that could contraindicated it. In complicated
appendicitis discharge will vary depending on the patient's progress and the presence of
adverse events, but in all cases it should be proved the restoration of intestinal transit and the
absence of signs of complication.
Patients at discharge should be informed of the care to be followed at home and monitoring
which are having and will be needing in next days. Adequate information, favored by the
development of standardized documents, reduces the readmission rate and increases patient
satisfaction.
6. OTHER REFERENCES
1. Helmer KS1, EK Robinson, Lally KP, JC Vasquez, KL Kwong, TH Liu, DW Mercer. Standardized
patient care guidelines reduce infectious morbidity in patients appendectomy. Am J Surg. 2002
Jun; 183 (6): 608-13.
2. Genser L, Vons C. abdominal surgical emergencies Can be Treated in an ambulatory setting?
Visc J Surg. 27. October 2015 PII: S1878-7886 (15) 00122-8. doi: 10.1016 /
j.jviscsurg.2015.09.015. [Epub ahead of print]
3. Bratzler DW, Hunt DR. The surgical infection prevention and surgical care improvement
projects: National Initiatives to Improve outcomes for patients Having surgery. Clin Infect Dis.
2006; 43 (3): 322.

18
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
7. ANNEXED
7.1 Alvarado Score
Symptoms Scores
Migratory/right iliac fossa pain 1
Nausea/Vomiting 1
Anorexia 1
Signs
Tenderness in right iliac fossa 2
Rebound tenderness in right iliac fossa
1
Elevated temperature 1
Laboratory findings
Leucocytosis 2
Shift to the left of neutrophils 1
Total 10 5-6: Possible 7-8: Probable >9 Very probable
7.2 APPENDICITIS INFLAMMATORY RESPONSE (AIR) SCORE
Vomiting 1
Pain in right iliac fossa 1
Rebound tenderness or muscular defense Light Medium Strong
1 2 3
Body temperature > 38,5 1
Polymorphonuclear leucocytes 70-84% > 85%
1 2
WBC count >10.0-14.9 x 109/l >15 x 109 /l
1 2
CRP concentration 10-49 g/l >50 g/l
1 2
Total score 12

19
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
7.3 DIAGRAM THERAPEUTIC DIAGNOSIS

20
APPENDICITIS MANAGEMENT PROTOCOL Echazarreta-Gallego et al.
7.4 CAPRINI SCORE MODEL
Each risk factor represent 1 point Age 41-60 Minor surgery Obesity IMC >25 Swollen legs (current) Varicose veins Sepsis (<1 month) Serious lung disease including pneumonia (< 1 month) Abnormal pulmonary function (COPD) Acute myocardial infarction Congestive heart failure (<1 month) History of inflammatory bowel disease Medical patient currently at bed rest
Each risk factor represents 1 point (only women) Oral contraceptives or hormone replacement therapy Pregnancy or postpartum (< 1 month) History of unexplained stillborn infant , recurrent spontaneous abortion (>3), premature birth with toxemia or growth-restricted infant
Each risk factor represents 2 points Age 61 -74 years Arthroscopic surgery Major surgery (>45 min) Laparoscopic surgery (>45 min) Malignancy (present or previous) Patient confined to bed (> 72 hours) Cental venous access Plaster cast (< 1 month)
Risk level Points
Very low 0
Low 1-2
Moderate 3-4
High > 4
7.5 APFEL SCORE
Risk fastor
Female gender 1
Nonsmoker 1
History of PONV or motion sickness 1
Use of opioids > 100 mcg fentanyl or equivalent
1 Low risk 0 or 1 Moderate risk 2 High 3 or 4