anticoagulant update - american college of physicians
TRANSCRIPT
1
Update on Anticoagulants
Jay Gaddy, MD, PhD
Indiana Hemophilia & Thrombosis Center
Indianapolis, Indiana
Disclosures
• None
Overview
• General discussion of anticoagulants
• New oral anticoagulants (NOACs) and their
targets
• Oral direct thrombin inhibitor - Dabigatran
• Oral factor Xa Inhibitors – Rivaroxaban,
Apixaban
• Reversal of anticoagulants
The ‘Ideal’ Oral Anticoagulant
• Good bioavailability
• No food or drug interactions
• Rapid onset of action
• Wide therapeutic window
• Predictable anticoagulant response
• Available antidote
• No unexpected toxicities
• Reasonable cost
• Mechanism to ensure compliance with therapy
Bauer, KA. Hematology, 2006:1;250
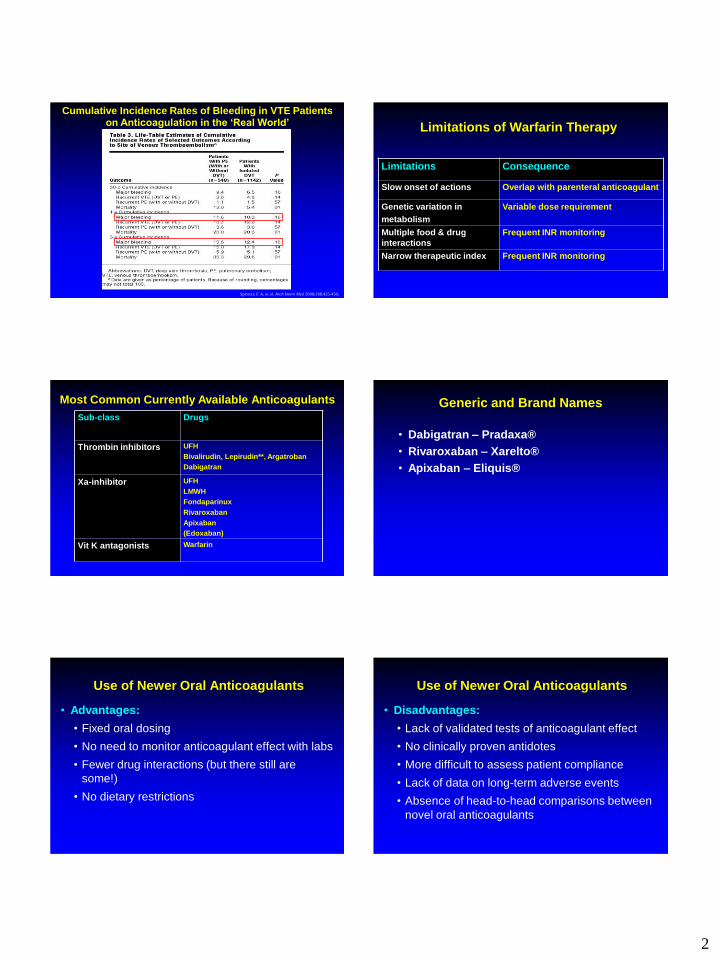
Warfarin
• When warfarin therapy is started, its anticoagulant
effects may not be apparent for several days.
• The duration of action of a single dose is 2–5 days.
• The therapeutic effect of warfarin exists within a
narrow therapeutic window as dictated by the INR.
• Considerable inter- and intra-individual dose
variability may be affected by a wide range of
physiologic (liver and thyroid function), genetic, and
environmental (eg, diet, other drugs) factors.
• Regular monitoring is required to avoid excessive or
insufficient anticoagulation.
Turpie, A. G.G. Eur Heart J 2008 29:155-165
Warfarin’s Therapeutic Window in A-fib
2
Spencer, F. A. et al. Arch Intern Med 2008;168:425-430.
Cumulative Incidence Rates of Bleeding in VTE Patients on Anticoagulation in the ‘Real World’ Limitations of Warfarin Therapy
Limitations Consequence
Slow onset of actions Overlap with parenteral anticoagulant
Genetic variation in
metabolism
Variable dose requirement
Multiple food & drug
interactions
Frequent INR monitoring
Narrow therapeutic index Frequent INR monitoring
Sub-class Drugs
Thrombin inhibitors UFH
Bivalirudin, Lepirudin**, Argatroban
Dabigatran
Xa-inhibitor UFH
LMWH
Fondaparinux
Rivaroxaban
Apixaban
(Edoxaban)
Vit K antagonists Warfarin
Most Common Currently Available Anticoagulants Generic and Brand Names
• Dabigatran – Pradaxa®
• Rivaroxaban – Xarelto®
• Apixaban – Eliquis®
Use of Newer Oral Anticoagulants
• Advantages:
• Fixed oral dosing
• No need to monitor anticoagulant effect with labs
• Fewer drug interactions (but there still are
some!)
• No dietary restrictions
Use of Newer Oral Anticoagulants
• Disadvantages:
• Lack of validated tests of anticoagulant effect
• No clinically proven antidotes
• More difficult to assess patient compliance
• Lack of data on long-term adverse events
• Absence of head-to-head comparisons between
novel oral anticoagulants

3
Targeting Specific Coagulation Factors
• Newer oral anticoagulants target specific points
in the coagulation cascade:
• Factor Xa inhibitors (eg, rivaroxaban, apixaban) target
factor Xa, preventing the conversion of prothrombin to
thrombin.
• Direct thrombin inhibitors (eg, dabigatran, ximelagatran)
target thrombin (factor IIa), blocking the conversion of
fibrinogen to fibrin.
• The goal of novel oral anticoagulants is to offer
more specific targeting and to afford more
predictable responses than current
anticoagulant therapies offer.
Targets of New Oral Anticoagulants Comparison of New Oral Agents
Feature
Dabigatran etexilate
Rivaroxaban Apixaban
Target Thrombin Factor Xa Factor Xa
Prodrug Yes No No
Dosing Fixed, 1-2x daily Fixed, once daily Fixed, twice daily
Bioavailability (%) 6 80 50
Time to onset (hrs) 2 2-4 1-3
Coagulation monitoring No No No
Half-life (h) 12–17 9-13 8-15
Renal clearance (%) 80 65 25
Interactions
P-gp inhibitors*
H2 blockers, PPIs
Combined P-gp and CYP3A4 inhibitors†
Combined P-gp and CYP3A4 inhibitors†
USA approved indications
A-fib VTE prevention and
treatment, A-fib A-fib
Weitz, Thrombosis and Haemostasis, 1/2010
Phase III Randomized Controlled Trials for VTE
Prevention
Drug Hip Arthroplasty Knee Arthroplasty Medical Surgical
Dabigatran RE-NOVATE RE-MODEL ... ...
RE-NOVATEII RE-MOBILIZE
Rivaroxaban RECORD1 RECORD3 MAGELLAN ...
RECORD2 RECORD4
Apixaban ADVANCE3 ADVANCE1 ADOPT ...
ADVANCE2
Eikelboom et al Circulation 2010 (121(1))
Phase III Randomized Controlled Trials non-VTE
prophylaxis
Anticoagulant VTE Treatment ACS AF
Idrabiotaparinux CASSIOPEA ... BOREALIS-AF
Dabigatran RE-COVER I RE-LY
RE-COVER II RELY-ABLE
RE-MEDY
RE-SONATE
Rivaroxaban EINSTEIN-DVT ATLAS JapaneseAF
EINSTEIN-PE ROCKET-AF
EINSTEIN-Extension
Apixaban Apixaban VTE APPRAISE2 AVERROES
Apixaban VTE extension ARISTOTLE
Edoxaban Hokusai-DVT ... ENGAGEAF TIMI48
Eikelboom et al Circulation 2010 (121(1))
4
FDA Approvals
• Dabigatran
• CVA and systemic embolism prevention in non-valvular A-fib
• Rivaroxaban
• CVA and systemic embolism prevention in non-valvular A-fib
• VTE prevention in TKR and THR
• Treatment of VTE/PE
• Apixaban
• CVA and systemic embolism prevention in non-valvular A-fib
Pradaxa® (dabigatran etexilate). Summary of product characteristics. Apr 2008
Dabigatran etexilate
• Oral prodrug, converted to Dabigatran
• Binds clot-bound and free thrombin
with high affinity and specificity
• Bioavailability: 6.5%
• Renal excretion: 80%
• Half-life: 12–17 hours
• No interaction with food
Pradaxa® (dabigatran etexilate). Summary of product characteristics. Apr 2008
Dabigatran etexilate
• No participation with CYP450
• Predictable anticoagulant effect – no need for
monitoring
• No liver toxicity based on available clinical data
• Dyspepsia is a side effect
• PPIs and H2 blockers may affect absorption
• Potential medication interactions with P-gp affecting
drugs – Amiodarone, Dronedarone, Quinidine, Verapamil,
Ketoconazole, Rifampin, St Johns Wort
Pradaxa® (dabigatran etexilate). Summary of product characteristics. Apr 2008
Dabigatran
● Other considerations
– Hygroscopic
Capsules should not be removed from original
container except for immediate use
Capsules only approved for 60 days after opening
bottle
Capsule should not be placed in pill boxes
Cannot crush or open pills for use in feeding tubes
Dabigatran: FDA Approval
• RE-LY (stroke prevention in patients with A-fib)
• 18,113 patients
• Dabigatran 110 and 150 mg bid compared with warfarin
• Treatment duration up to 3 years, median follow-up of 2 yrs
• 110 mg associated with rates of stroke or systemic embolism that were similar to those associated with warfarin, as well as lower rates of major hemorrhage
• Dabigatran administered at a dose of 150 mg, as compared with warfarin, was associated with lower rates of stroke or systemic embolism but similar rates of major hemorrhage
Connolly, New England Jl Med, 2009
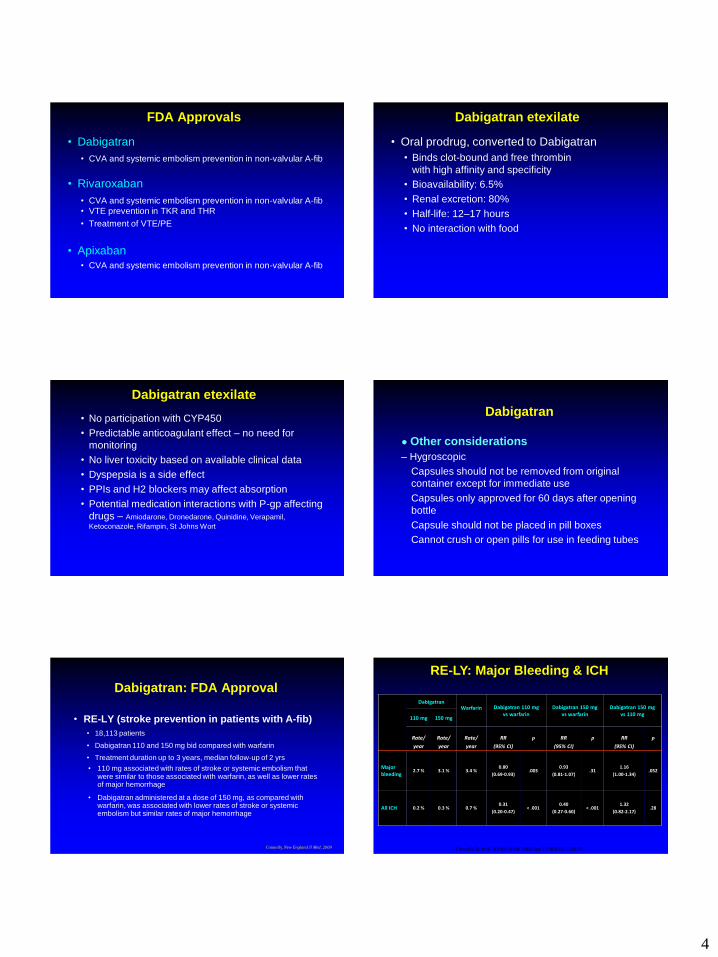
RE-LY: Major Bleeding & ICH
Dabigatran
Warfarin Dabigatran 110 mg vs warfarin
Dabigatran 150 mg vs warfarin
Dabigatran 150 mg vs 110 mg
110 mg 150 mg
Rate/
year
Rate/
year
Rate/
year
RR
(95% CI)
P RR
(95% CI)
P RR
(95% CI)
P
Major bleeding
2.7 % 3.1 % 3.4 % 0.80
(0.69-0.93) .003
0.93
(0.81-1.07) .31
1.16
(1.00-1.34) .052
All ICH 0.2 % 0.3 % 0.7 % 0.31
(0.20-0.47) < .001
0.40
(0.27-0.60) < .001
1.32
(0.82-2.17) .28
Connolly SJ. et al. N Engl J Med. 2009 Sep 17;361(12):1139-51.
5
RE-LY: Sites of Major Bleeding
Dabigatran Warfarin Dabigatran 110mg
vs Warfarin Dabigatran 150mg vs.
Warfarin
110mg 150mg
Annual
rate
RR
95% CI P
RR
95% CI P
Annual
rate
Annual
rate
Intracranial
0.23 % 0.30 % 0.74 % 0.31
0.20-0.47 < .001
0.40
0.27-0.60 < .001
Major Bleed 2.71 % 3.11 % 3.36% 0.80
0.69-0.93 .003
0.93
0.81-1.07 .31
Gastro-intestinal
1.12% 1.51 % 1.02% 1.10
0.86-1.41 .43
1.50
1.19-1.89 < .001
Connolly, SJ. et al. N Engl J Med 2009;361:1139-1151.
RE-LY: GI Major Bleeding & MI
Dabigatran
Warfarin Dabigatran 110 mg vs warfarin
Dabigatran 150 mg vs warfarin
Dabigatran 150 mg vs 110 mg 110 mg 150 mg
Rate/
Year
Rate/
Year
Rate/
Year
RR
(95% CI) P
RR
(95% CI) P
RR
(95% CI) P
GI Major Bleed
1.1 % 1.5 % 1.0 % 1.10
(0.86-1.41) .43
1.50
(1.19-1.89) <.001
1.36
(1.09-1.70) .007
MI 0.72% 0.74% 0.53% 1.35
(0.98-1.87) .07
1.38
(1.00-1.91) .048
1.02
(0.76-1.38) .88
Connolly SJ. et al. N Engl J Med. 2009 Sep 17;361(12):1139-51.
RE-LY: Drug Discontinuation
Variable
Dabigatran 110 mg
(n = 6015)
Dabigatran 150 mg
(n = 6076) Warfarin (n = 6022) P-value a
Discontinued at 1 year, % 15% 16% 10% < .001
Discontinued at 2 years, % 21% 21% 17% < .001
a. Rates of discontinuation at 1 and 2 years were higher with dabigatran than with warfarin (P < .001). Rates are based on Kaplan-Meier estimates
Connolly, SJ. et al. N Engl J Med 2009;361:1139-1151.
Dabigatran: Dosing in US
• CrCl > 30 – 150mg bid
• CrCl 15-30 – 75mg bid
• CrCl < 15 – not recommended
• CrCl should be assessed yearly in patients > 75
Connolly, New England Jl Med, 2009
Rivaroxaban
• Predictable pharmacology
• High bioavailability
• Fixed dose
• No requirement for monitoring
• Inhibits free and thrombus associated Xa
• Contraindicated in severe renal insufficiency
• Drug interactions with meds that affect P-gp
and CYP3A4 – Ketoconazole, Rifampin,
Clarithromycin, St Johns Wort and HIV-protease
inhibitors (ritonavir)
Perzborn et al. 2005; Kubitza et al. 2005; 2006; 2007; Roehrig et al, 2005
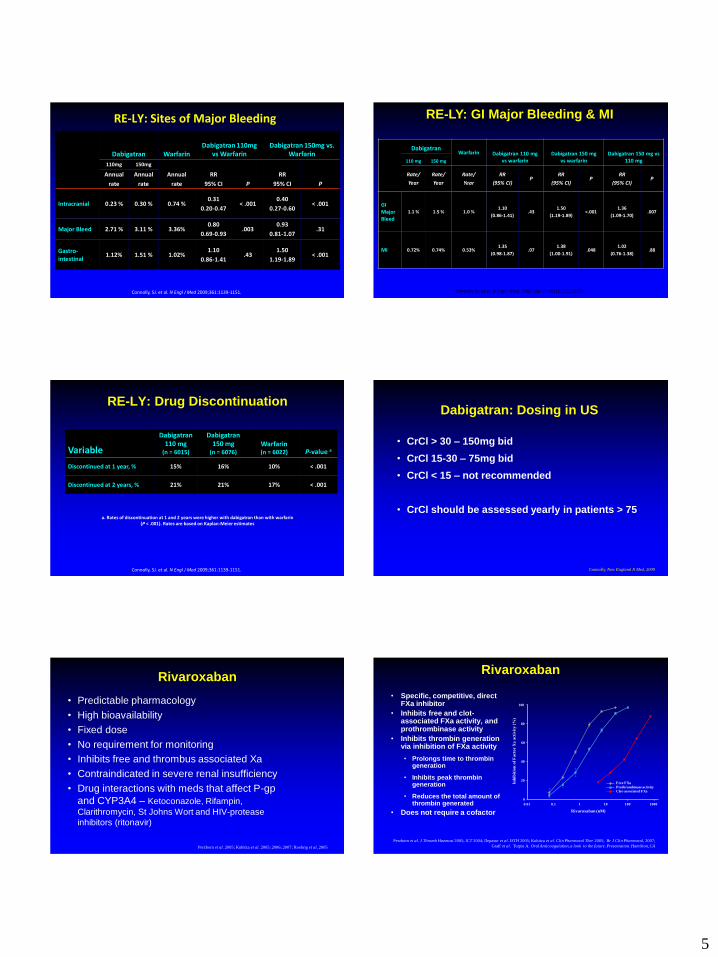
Rivaroxaban
• Specific, competitive, direct FXa inhibitor
• Inhibits free and clot-associated FXa activity, and prothrombinase activity
• Inhibits thrombin generation via inhibition of FXa activity
• Prolongs time to thrombin generation
• Inhibits peak thrombin generation
• Reduces the total amount of thrombin generated
• Does not require a cofactor
Perzborn et al. J Thromb Haemost 2005; ICT 2004; Depasse et al. ISTH 2005; Kubitza et al. Clin Pharmacol Ther 2005; Br J Clin Pharmacol, 2007;
Graff et al. Turpie A. Oral Anticoagulation, a look to the future. Presentaiton. Hamilton, CA
Rivaroxaban (nM)
0.01 0.1 1 10 100 1000
Inh
ibit
ion
of
Fa
cto
r X
a a
ctiv
ity (
%)
0
20
40
60
80
100
Free FXa
Prothrombinase activity
Clot-associated FXa
6
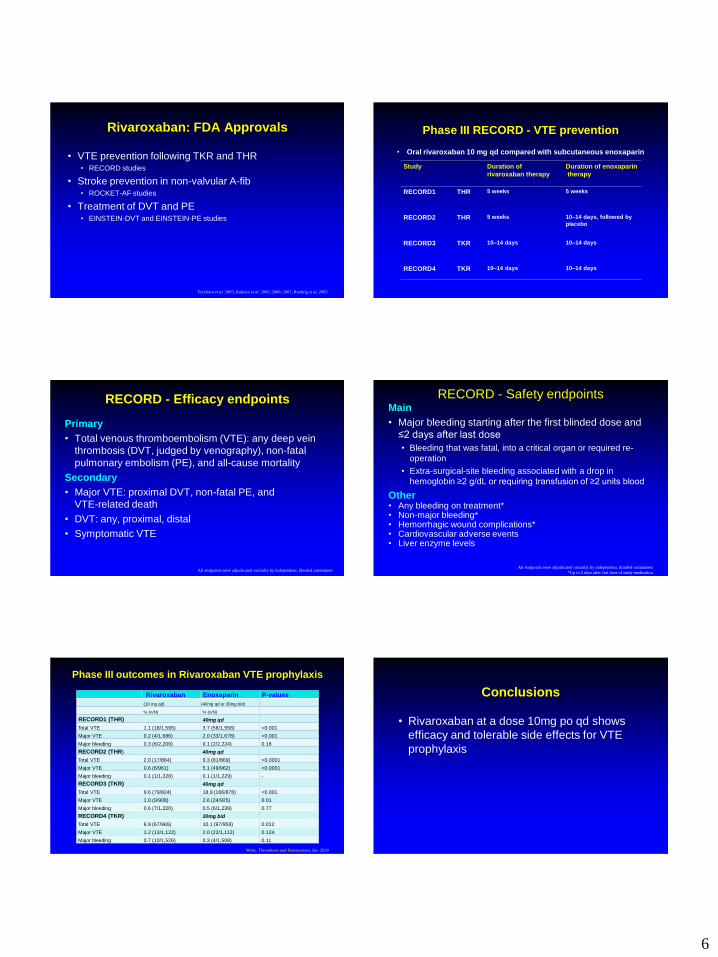
Rivaroxaban: FDA Approvals
• VTE prevention following TKR and THR • RECORD studies
• Stroke prevention in non-valvular A-fib • ROCKET-AF studies
• Treatment of DVT and PE • EINSTEIN-DVT and EINSTEIN-PE studies
Perzborn et al. 2005; Kubitza et al. 2005; 2006; 2007; Roehrig et al, 2005
Phase III RECORD - VTE prevention
• Oral rivaroxaban 10 mg qd compared with subcutaneous enoxaparin
Study Duration of
rivaroxaban therapy
Duration of enoxaparin
therapy
RECORD1 THR 5 weeks 5 weeks
RECORD2 THR 5 weeks 10–14 days, followed by
placebo
RECORD3 TKR 10–14 days 10–14 days
RECORD4 TKR 10–14 days 10–14 days
RECORD - Efficacy endpoints
Primary
• Total venous thromboembolism (VTE): any deep vein
thrombosis (DVT, judged by venography), non-fatal
pulmonary embolism (PE), and all-cause mortality
Secondary
• Major VTE: proximal DVT, non-fatal PE, and
VTE-related death
• DVT: any, proximal, distal
• Symptomatic VTE
All endpoints were adjudicated centrally by independent, blinded committees
RECORD - Safety endpoints Main
• Major bleeding starting after the first blinded dose and
≤2 days after last dose
• Bleeding that was fatal, into a critical organ or required re-
operation
• Extra-surgical-site bleeding associated with a drop in
hemoglobin ≥2 g/dL or requiring transfusion of ≥2 units blood
Other • Any bleeding on treatment* • Non-major bleeding* • Hemorrhagic wound complications* • Cardiovascular adverse events • Liver enzyme levels
All endpoints were adjudicated centrally by independent, blinded committees
*Up to 2 days after last dose of study medication
Phase III outcomes in Rivaroxaban VTE prophylaxis
Rivaroxaban Enoxaparin P-values
(10 mg qd) (40mg qd or 30mg bid)
% (n/N) % (n/N)
RECORD1 (THR) 40mg qd
Total VTE 1.1 (18/1,595) 3.7 (58/1,558) <0.001
Major VTE 0.2 (4/1,686) 2.0 (33/1,678) <0.001
Major bleeding 0.3 (6/2,209) 0.1 (2/2,224) 0.18
RECORD2 (THR) 40mg qd
Total VTE 2.0 (17/864) 9.3 (81/869) <0.0001
Major VTE 0.6 (6/961) 5.1 (49/962) <0.0001
Major bleeding 0.1 (1/1,228) 0.1 (1/1,229) -
RECORD3 (TKR) 40mg qd
Total VTE 9.6 (79/824) 18.9 (166/878) <0.001
Major VTE 1.0 (9/908) 2.6 (24/925) 0.01
Major bleeding 0.6 (7/1,220) 0.5 (6/1,239) 0.77
RECORD4 (TKR) 30mg bid
Total VTE 6.9 (67/965) 10.1 (97/959) 0.012
Major VTE 1.2 (13/1,122) 2.0 (22/1,112) 0.124
Major bleeding 0.7 (10/1,526) 0.3 (4/1,508) 0.11
Weitz, Thrombosis and Haemostasis, Jan. 2010
Conclusions
• Rivaroxaban at a dose 10mg po qd shows
efficacy and tolerable side effects for VTE
prophylaxis
7
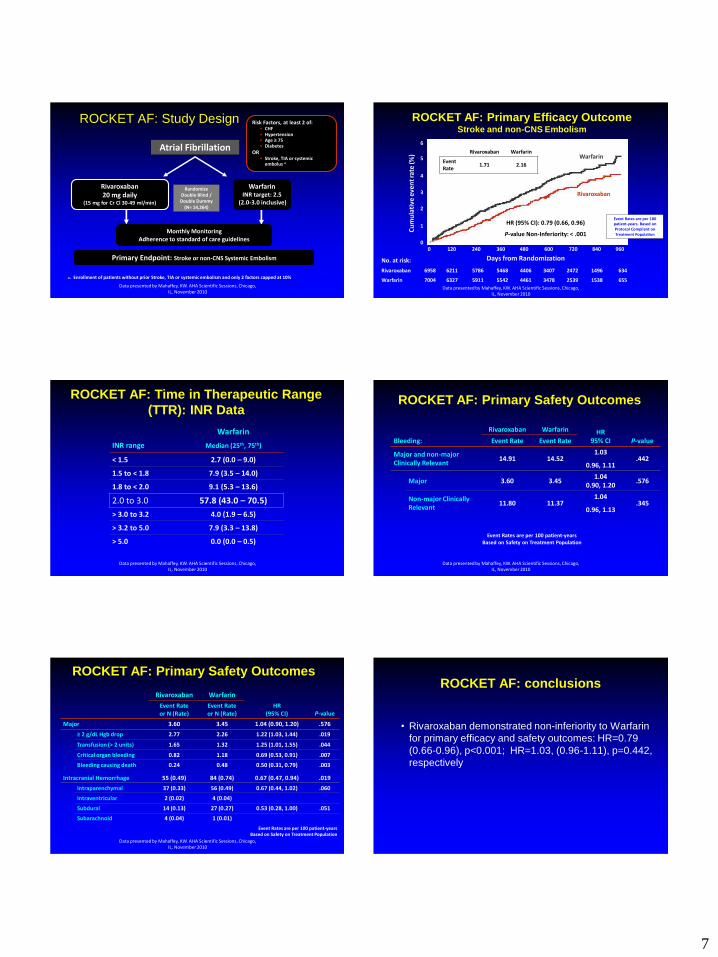
Rivaroxaban 20 mg daily
(15 mg for Cr Cl 30-49 ml/min)
Warfarin INR target: 2.5
(2.0-3.0 inclusive)
Primary Endpoint: Stroke or non-CNS Systemic Embolism
Atrial Fibrillation
Randomize Double Blind / Double Dummy
(N= 14,264)
Monthly Monitoring Adherence to standard of care guidelines
ROCKET AF: Study Design
a. Enrollment of patients without prior Stroke, TIA or systemic embolism and only 2 factors capped at 10%
Risk Factors, at least 2 of: • CHF • Hypertension • Age 75 • Diabetes
OR • Stroke, TIA or systemic
embolus a
Data presented by Mahaffey, KW. AHA Scientific Sessions, Chicago, IL, November 2010
No. at risk:
Rivaroxaban 6958 6211 5786 5468 4406 3407 2472 1496 634
Warfarin 7004 6327 5911 5542 4461 3478 2539 1538 655
ROCKET AF: Primary Efficacy Outcome Stroke and non-CNS Embolism
Event Rates are per 100 patient-years. Based on Protocol Compliant on Treatment Population
Warfarin
HR (95% CI): 0.79 (0.66, 0.96)
P-value Non-Inferiority: < .001
Days from Randomization
Cu
mu
lati
ve e
ven
t ra
te (%
)
Rivaroxaban
Rivaroxaban Warfarin
Event Rate
1.71 2.16
0
1
2
3
4
5
6
0 120 240 360 480 600 720 840 960
Data presented by Mahaffey, KW. AHA Scientific Sessions, Chicago, IL, November 2010
ROCKET AF: Time in Therapeutic Range
(TTR): INR Data
INR range
Warfarin
Median (25th, 75th)
< 1.5 2.7 (0.0 – 9.0)
1.5 to < 1.8 7.9 (3.5 – 14.0)
1.8 to < 2.0 9.1 (5.3 – 13.6)
2.0 to 3.0 57.8 (43.0 – 70.5)
> 3.0 to 3.2 4.0 (1.9 – 6.5)
> 3.2 to 5.0 7.9 (3.3 – 13.8)
> 5.0 0.0 (0.0 – 0.5)
Data presented by Mahaffey, KW. AHA Scientific Sessions, Chicago, IL, November 2010
ROCKET AF: Primary Safety Outcomes
Bleeding:
Rivaroxaban Warfarin HR 95% CI P-value Event Rate Event Rate
Major and non-major Clinically Relevant
14.91 14.52 1.03
0.96, 1.11 .442
Major 3.60 3.45 1.04
0.90, 1.20 .576
Non-major Clinically Relevant
11.80 11.37 1.04
0.96, 1.13 .345
Event Rates are per 100 patient-years Based on Safety on Treatment Population
Data presented by Mahaffey, KW. AHA Scientific Sessions, Chicago, IL, November 2010
Rivaroxaban Warfarin
HR (95% CI) P-value
Event Rate or N (Rate)
Event Rate or N (Rate)
Major 3.60 3.45 1.04 (0.90, 1.20) .576
≥ 2 g/dL Hgb drop 2.77 2.26 1.22 (1.03, 1.44) .019
Transfusion (> 2 units) 1.65 1.32 1.25 (1.01, 1.55) .044
Critical organ bleeding 0.82 1.18 0.69 (0.53, 0.91) .007
Bleeding causing death 0.24 0.48 0.50 (0.31, 0.79) .003
Intracranial Hemorrhage 55 (0.49) 84 (0.74) 0.67 (0.47, 0.94) .019
Intraparenchymal 37 (0.33) 56 (0.49) 0.67 (0.44, 1.02) .060
Intraventricular 2 (0.02) 4 (0.04)
Subdural 14 (0.13) 27 (0.27) 0.53 (0.28, 1.00) .051
Subarachnoid 4 (0.04) 1 (0.01)
Event Rates are per 100 patient-years Based on Safety on Treatment Population
ROCKET AF: Primary Safety Outcomes
Data presented by Mahaffey, KW. AHA Scientific Sessions, Chicago, IL, November 2010
ROCKET AF: conclusions
• Rivaroxaban demonstrated non-inferiority to Warfarin
for primary efficacy and safety outcomes: HR=0.79
(0.66-0.96), p<0.001; HR=1.03, (0.96-1.11), p=0.442,
respectively
8
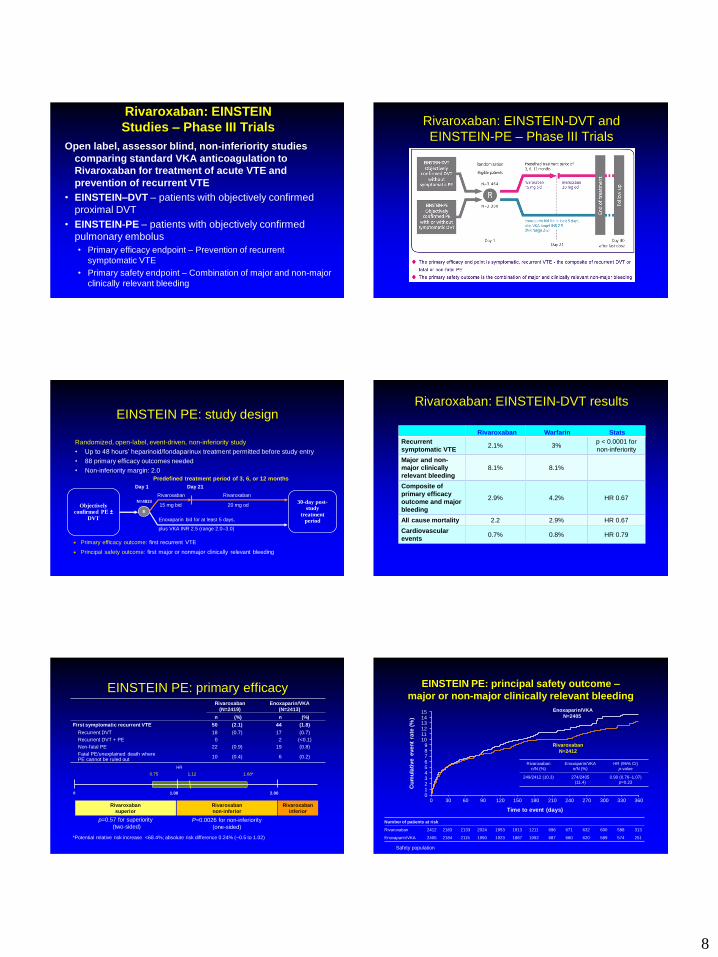
Rivaroxaban: EINSTEIN
Studies – Phase III Trials
Open label, assessor blind, non-inferiority studies
comparing standard VKA anticoagulation to
Rivaroxaban for treatment of acute VTE and
prevention of recurrent VTE
• EINSTEIN–DVT – patients with objectively confirmed
proximal DVT
• EINSTEIN-PE – patients with objectively confirmed
pulmonary embolus
• Primary efficacy endpoint – Prevention of recurrent
symptomatic VTE
• Primary safety endpoint – Combination of major and non-major
clinically relevant bleeding
Rivaroxaban: EINSTEIN-DVT and
EINSTEIN-PE – Phase III Trials
EINSTEIN PE: study design
Randomized, open-label, event-driven, non-inferiority study
• Up to 48 hours’ heparinoid/fondaparinux treatment permitted before study entry
• 88 primary efficacy outcomes needed
• Non-inferiority margin: 2.0
Predefined treatment period of 3, 6, or 12 months
15 mg bid
Rivaroxaban
Day 1 Day 21
Enoxaparin bid for at least 5 days,
plus VKA INR 2.5 (range 2.0–3.0)
20 mg od N=4833
Rivaroxaban
R
Objectively confirmed PE ±
DVT
30-day post-study
treatment period
Primary efficacy outcome: first recurrent VTE
Principal safety outcome: first major or nonmajor clinically relevant bleeding
Rivaroxaban: EINSTEIN-DVT results
Rivaroxaban Warfarin Stats
Recurrent
symptomatic VTE 2.1% 3%
p < 0.0001 for
non-inferiority
Major and non-
major clinically
relevant bleeding
8.1% 8.1%
Composite of
primary efficacy
outcome and major
bleeding
2.9% 4.2% HR 0.67
All cause mortality 2.2 2.9% HR 0.67
Cardiovascular
events 0.7% 0.8% HR 0.79
EINSTEIN PE: primary efficacy Rivaroxaban
(N=2419)
Enoxaparin/VKA
(N=2413)
n (%) n (%)
First symptomatic recurrent VTE 50 (2.1) 44 (1.8)
Recurrent DVT 18 (0.7) 17 (0.7)
Recurrent DVT + PE 0 2 (<0.1)
Non-fatal PE 22 (0.9) 19 (0.8)
Fatal PE/unexplained death where PE cannot be ruled out
10 (0.4) 6 (0.2)
Rivaroxaban
superior
Rivaroxaban
non-inferior
Rivaroxaban
inferior
P=0.0026 for non-inferiority
(one-sided)
p=0.57 for superiority
(two-sided)
1.00 0 2.00
0.75 1.12 1.68*
*Potential relative risk increase <68.4%; absolute risk difference 0.24% (–0.5 to 1.02)
HR
EINSTEIN PE: principal safety outcome –
major or non-major clinically relevant bleeding
Rivaroxaban
n/N (%)
Enoxaparin/VKA
n/N (%)
HR (95% CI)
p-value
249/2412 (10.3) 274/2405
(11.4)
0.90 (0.76–1.07)
p=0.23
Safety population
0 30 60 90 120 150 180 210 240 270 300 330 360
15 14
10
13 12 11
9 8 7 6 5 4 3 2 1 0
Number of patients at risk
Rivaroxaban 2412 2183 2133 2024 1953 1913 1211 696 671 632 600 588 313
Enoxaparin/VKA 2405 2184 2115 1990 1923 1887 1092 687 660 620 589 574 251
Time to event (days)
Rivaroxaban
N=2412
Enoxaparin/VKA
N=2405
Cu
mu
lati
ve e
ven
t ra
te (
%)

9
Safety population
3.0
2.5
2.0
1.5
1.0
0.0
0.5
0 30 60 90 120 150 180 210 240 270 300 330 360
Cu
mu
lati
ve e
ven
t ra
te (
%)
Time to event (days)
Rivaroxaban
N=2412
Enoxaparin/VKA
N=2405
Number of patients at risk
Rivaroxaban 2412 2281 2248 2156 2091 2063 1317 761 735 700 669 659 350
Enoxaparin/VKA 2405 2270 2224 2116 2063 2036 1176 746 719 680 658 642 278
EINSTEIN PE: major bleeding
Rivaroxaban
n/N (%)
Enoxaparin/VKA
n/N (%)
HR (95% CI)
p-value
26/2412
(1.1)
52/2405
(2.2)
0.49 (0.31–0.79)
p=0.0032
EINSTEIN PE: conclusions
• In patients with acute symptomatic PE with or without
DVT, Rivaroxaban showed:
• Non-inferiority to LMWH/VKA for efficacy: HR=1.12 (0.75–
1.69);
pnon-inferiority =0.0026 for non-inferiority margin of 2.0
• Similar findings for principal safety outcome: HR=0.90
(0.76–1.07); p=0.23
• Superiority for major bleeding: HR=0.49 (0.31–0.79) p=0.0032
• Consistent efficacy and safety results irrespective of age, body
weight, gender, kidney function and cancer
• No evidence for liver toxicity
Rivaroxaban: Dosing in US
• A-fib
• 20mg daily with evening meal if CrCl >50
• 15mg daily with evening meal if CrCl 15-50
• DVT/PE
• 15mg bid with meals x 21 days followed by 20mg
daily with meal
• For patients with CrCl > 30
• Joint replacement surgery
• 10mg daily, 12 days for TKR, 35 days for THR
• For patients with CrCl > 30
Connolly, New England Jl Med, 2009
Apixaban
• Predictable pharmacology
• High bioavailability
• Fixed dose
• No requirement for monitoring
• Inhibits free and thrombus associated Xa
• Contraindicated in severe renal insufficiency
• Drug interactions with meds that affect P-gp and
CYP3A4 – Ketoconazole, Rifampin, Clarithromycin, St
Johns Wort and HIV-protease inhibitors (ritonavir)
Apixaban: FDA Approval
• Stoke and thromboembolic prevention in non-
valvular AF
• ARISTOTLE and AVERROES Studies
10
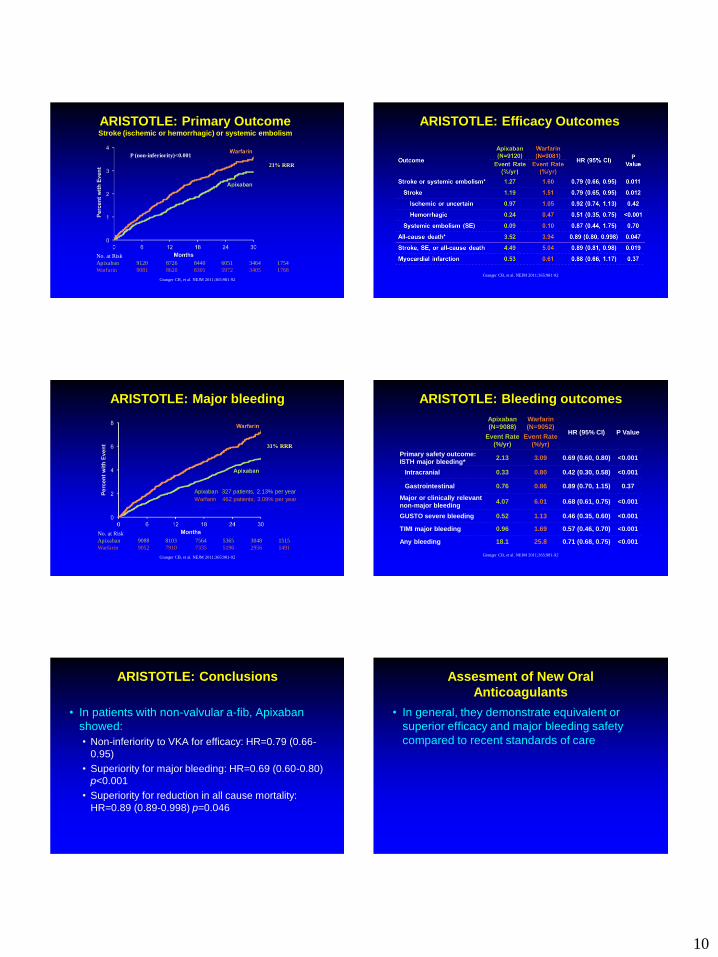
ARISTOTLE: Primary Outcome Stroke (ischemic or hemorrhagic) or systemic embolism
No. at Risk
Apixaban 9120 8726 8440 6051 3464 1754
Warfarin 9081 8620 8301 5972 3405 1768
21% RRR
P (non-inferiority)<0.001
Granger CB, et al. NEJM 2011;365:981-92
ARISTOTLE: Efficacy Outcomes
Granger CB, et al. NEJM 2011;365:981-92
ARISTOTLE: Major bleeding
Apixaban 327 patients, 2.13% per year
Warfarin 462 patients, 3.09% per year
HR 0.69 (95% CI, 0.60–0.80); P<0.001
No. at Risk
Apixaban 9088 8103 7564 5365 3048 1515
Warfarin 9052 7910 7335 5196 2956 1491
31% RRR
Granger CB, et al. NEJM 2011;365:981-92
Apixaban (N=9088)
Warfarin (N=9052)
HR (95% CI) P Value Event Rate
(%/yr) Event Rate
(%/yr)
Primary safety outcome: ISTH major bleeding*
2.13 3.09 0.69 (0.60, 0.80) <0.001
Intracranial 0.33 0.80 0.42 (0.30, 0.58) <0.001
Gastrointestinal 0.76 0.86 0.89 (0.70, 1.15) 0.37
Major or clinically relevant non-major bleeding
4.07 6.01 0.68 (0.61, 0.75) <0.001
GUSTO severe bleeding 0.52 1.13 0.46 (0.35, 0.60) <0.001
TIMI major bleeding 0.96 1.69 0.57 (0.46, 0.70) <0.001
Any bleeding 18.1 25.8 0.71 (0.68, 0.75) <0.001
ARISTOTLE: Bleeding outcomes
Granger CB, et al. NEJM 2011;365:981-92
ARISTOTLE: Conclusions
• In patients with non-valvular a-fib, Apixaban
showed:
• Non-inferiority to VKA for efficacy: HR=0.79 (0.66-
0.95)
• Superiority for major bleeding: HR=0.69 (0.60-0.80)
p<0.001
• Superiority for reduction in all cause mortality:
HR=0.89 (0.89-0.998) p=0.046
Assesment of New Oral
Anticoagulants
• In general, they demonstrate equivalent or
superior efficacy and major bleeding safety
compared to recent standards of care

11
Comparison of New Oral
Anticoagulants
• **There are no head to head trials comparing
these agents. Trends that may suggest any
comparative superiority are only hypothesis
generating and need confirmation in head to head
trials
Comparable Efficacy of NOACs
in A-Fib
Copyright © The American College of Cardiology.
All rights reserved.
Comparable Major Bleeding
with NOACs in A-Fib
Copyright © The American College of Cardiology.
All rights reserved.
Time Warfarin in Therapeutic
Range (TTR)
● RE-LY (DABIGATRAN)
– 64% in Warfarin-experienced, 61% in Warfarin-naive
● ROCKET AF (RIVAROXABAN)
– Mean 55%, Median 58%
● ARISTOTLE (APIXABAN)
– Mean 62%, Median 66%
Testing of Hemostatic Function
● DABIGATRAN
– aPTT, thrombin clotting time (TCT) and ecarin cloting time
are prolonged
– TCT has a linear correlation with concentration but prolongs
quickly
– If TCT is not prolonged, Dabigatran level likely is low
● RIVAROXABAN
– Prothrombin time (PT) and anti-Xa affected
– Prothrombin time (PT) shows a linear dose response and is
prolonged to a similar extent as the degree of inhibition of
Xa (assay dependent)
Testing of Hemostatic Function
● APIXABAN
– Prothrombin time (PT) and anti-Xa affected
● Predictive ability of coag assays has not been clinically proven and
target drug levels have not been determined. trough levels may
not be detected.
● Anti-Xa activities can be measured against standard curves for
each Xa inhibitor but currently unsure what levels are consistent
with clinical efficacy or safety
12
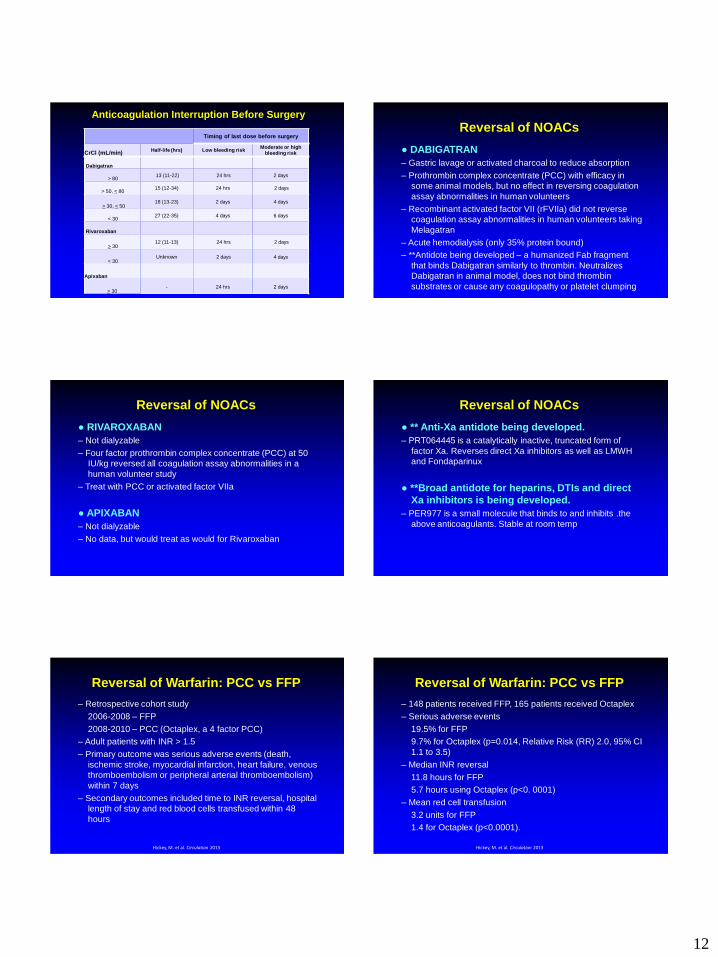
Timing of last dose before surgery
CrCl (mL/min) Half-life (hrs) Low bleeding risk
Moderate or high bleeding risk
Dabigatran
> 80 13 (11-22) 24 hrs 2 days
> 50, < 80 15 (12-34) 24 hrs 2 days
> 30, < 50 18 (13-23) 2 days 4 days
< 30 27 (22-35) 4 days 6 days
Rivaroxaban
> 30 12 (11-13) 24 hrs 2 days
< 30 Unknown 2 days 4 days
Apixaban
> 30 - 24 hrs 2 days
Anticoagulation Interruption Before Surgery
Reversal of NOACs
● DABIGATRAN
– Gastric lavage or activated charcoal to reduce absorption
– Prothrombin complex concentrate (PCC) with efficacy in
some animal models, but no effect in reversing coagulation
assay abnormalities in human volunteers
– Recombinant activated factor VII (rFVIIa) did not reverse
coagulation assay abnormalities in human volunteers taking
Melagatran
– Acute hemodialysis (only 35% protein bound)
– **Antidote being developed – a humanized Fab fragment
that binds Dabigatran similarly to thrombin. Neutralizes
Dabigatran in animal model, does not bind thrombin
substrates or cause any coagulopathy or platelet clumping
Reversal of NOACs
● RIVAROXABAN
– Not dialyzable
– Four factor prothrombin complex concentrate (PCC) at 50
IU/kg reversed all coagulation assay abnormalities in a
human volunteer study
– Treat with PCC or activated factor VIIa
● APIXABAN
– Not dialyzable
– No data, but would treat as would for Rivaroxaban
Reversal of NOACs
● ** Anti-Xa antidote being developed.
– PRT064445 is a catalytically inactive, truncated form of
factor Xa. Reverses direct Xa inhibitors as well as LMWH
and Fondaparinux
● **Broad antidote for heparins, DTIs and direct
Xa inhibitors is being developed.
– PER977 is a small molecule that binds to and inhibits .the
above anticoagulants. Stable at room temp
Reversal of Warfarin: PCC vs FFP
– Retrospective cohort study
2006-2008 – FFP
2008-2010 – PCC (Octaplex, a 4 factor PCC)
– Adult patients with INR > 1.5
– Primary outcome was serious adverse events (death,
ischemic stroke, myocardial infarction, heart failure, venous
thromboembolism or peripheral arterial thromboembolism)
within 7 days
– Secondary outcomes included time to INR reversal, hospital
length of stay and red blood cells transfused within 48
hours
Hickey, M. et al. Circulation 2013
Reversal of Warfarin: PCC vs FFP
– 148 patients received FFP, 165 patients received Octaplex
– Serious adverse events
19.5% for FFP
9.7% for Octaplex (p=0.014, Relative Risk (RR) 2.0, 95% CI
1.1 to 3.5)
– Median INR reversal
11.8 hours for FFP
5.7 hours using Octaplex (p<0. 0001)
– Mean red cell transfusion
3.2 units for FFP
1.4 for Octaplex (p<0.0001).
Hickey, M. et al. Circulation 2013

13
Advantages of New Agents vs. VKAs
● RAPID ONSET OF ACTION
– May replace parenteral anticoagulants
for selected conditions
– Eliminates need for two anticoagulant
regimen (i.e. heparin and warfarin)
● PREDICTABLE THERAPEUTIC
EFFECT WITH FIXED OR WEIGHT-
BASED DOSING
– No routine coagulation monitoring
required
● LIMITED OR NO FOOD OR DRUG
INTERACTIONS
● SHORT HALF-LIFE
– Effect wears off more quickly than
VKAs
● NO NEED FOR BRIDGING AC FOR
INVASIVE PROCEDURES
Phillips et al. Jl Thromb Haem. 2010
● MORE CONVENIENT FOR PATIENT
– No routine monitoring, dietary limitations
and limited drug interactions
● MORE CONVENIENT FOR PHYSICIAN
– No routine coagulation monitoring
● POTENTIAL FOR GREATER USE
– Barriers removed that limit more
widespread use
● MORE COST EFFECTIVE?
– No routine coagulation monitoring
– Fewer adverse events
● POSSIBLE SUPERIOR EFFICACY
● POSSIBLE SUPERIOR SAFETY
Disadvantages of New Agents vs. VKAs
● NO ROUTINE COAGULATION MONITORING
– Cannot titrate dose
– Determination of failure of therapy vs. poor compliance
● SHORT HALF-LIFE
– Anticoagulation effect declines quickly if
compliance poor
– Poor compliance may affect efficacy more than with VKA
● NO CLINICALLY PROVEN ANTIDOTES
● NO MONITORING LAB MARKER AVAILABLE TO
RELIABLY MEASURE DRUG ACTIVITY IF NEEDED
● POTENTIAL DOSE ADJUSTMENT REQUIRED FOR
RENAL OR HEPATIC DYSFUNCTION
● COST?
Phillips et al. Jl Thromb Haem. 2010
Populations That Should be Initially Treated
with or Remain on Warfarin Rather Than be
Placed on a Newer Oral Anticoagulant
● ALREADY TAKING WARFARIN WITH EXCELLENT INR CONTROL
– RE-LY data demonstrated equivalent efficacy but increased GI bleeding
when comparing Dabigatgran 150mg bid to Warfarin with excellent control
● RENAL INSUFFICIENCY
– Consider if CrCl < 30 and definitely if < 15
● MECHANICAL HEART VALVES
● PREDISPOSITION TO GI BLEEDING
● POOR COMPLIANCE
– Concern regarding the quick loss of anticoagulant effect (question this)
● CAN’T AFFORD NEWER DRUG
Populations That Should Consider Treating
With Newer Oral Anticoagulants
● THOSE WITH UNEXPLAINED POOR INR CONTROL
– RE-LY data demonstrated equivalent efficacy but increased GI bleeding
when comparing Dabigatran 150mg bid to Warfarin with excellent control
● POOR INR CONTROL DUE TO UNAVOIDABLE DRUG INTERACTION
– Recurrent antibiotics, Amiodarone, Chemotherapy, APAP, Azathioprine,
polypharmacy
● NEW PATIENTS ON ANTICOAGULATION WITHOUT SIGNIFICANT
RENAL INSUFFICIENCY
● CAN AFFORD THE NEW DRUGS
Acknowledgments
• Gina Bryant
• Amy Shapiro, M.D.
• Chirag Amin, M.D.