anti ifn-gamma autoantibody associated with adult-onset immunodeficiency
TRANSCRIPT
Autoantibody to Interferon-gamma
Associated with Adult-Onset Immunodeficiency
Suda Sibunruang, M.D.
Outline • Reported cases
• Interferon and interleukin-12 pathways
• Natural anti–INF- antibodies
• Landmark study & present data
• Associated reactive dermatoses
• Autoantibodies to cytokines
• Mendelian susceptibility to mycobacterial infection
• Prognosis
• Treatment

ทมแพทย รพ.ศรนครนทร ม.ขอนแกน คนพบ“โรคภมคมกนบกพรองทไมใชเอดส”
เปนครงแรกของโลก (พ.ศ.2543)
Access from www.kku.ac.th and www.rcpt.org January 2, 2015
AIDS-like illness which occurs in otherwise immunocompetent adults
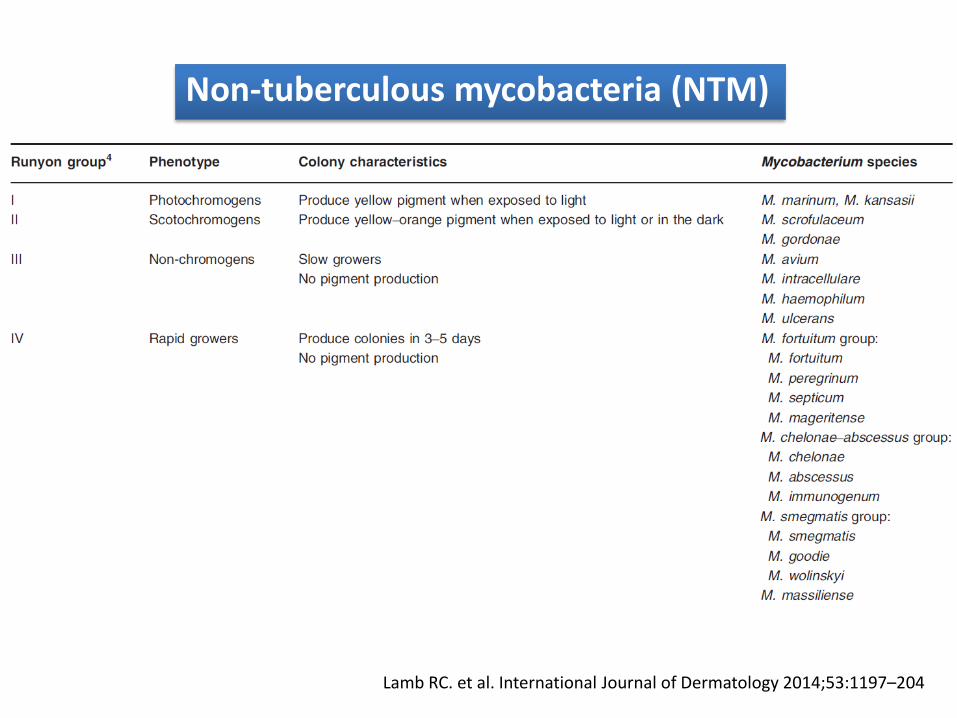
Lamb RC. et al. International Journal of Dermatology 2014;53:1197–204
Non-tuberculous mycobacteria (NTM)
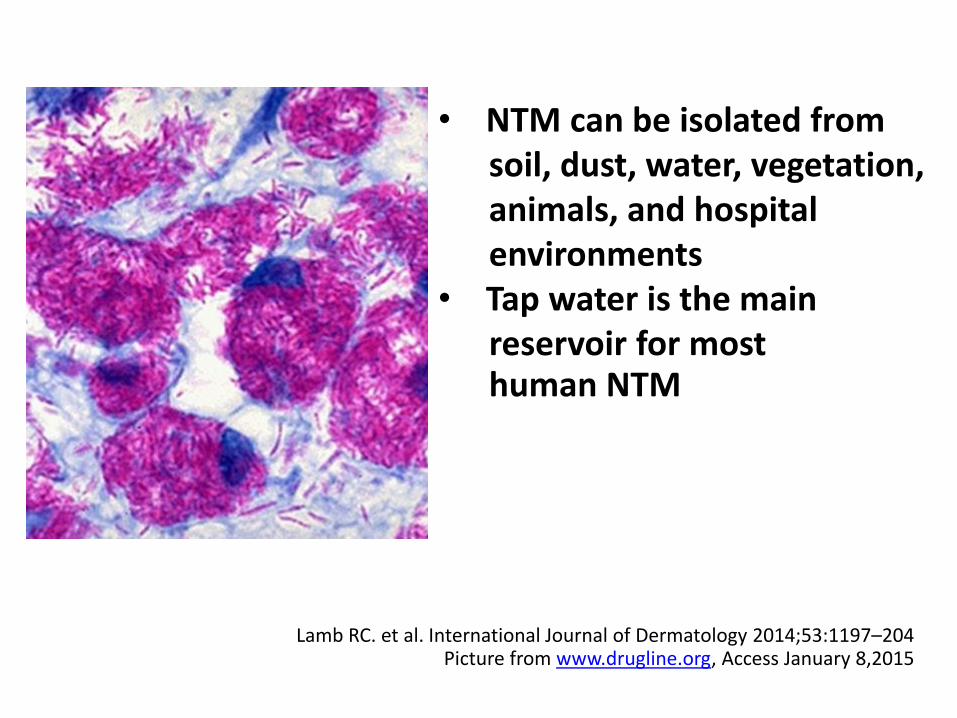
Lamb RC. et al. International Journal of Dermatology 2014;53:1197–204 Picture from www.drugline.org, Access January 8,2015
• NTM can be isolated from soil, dust, water, vegetation, animals, and hospital environments • Tap water is the main reservoir for most human NTM
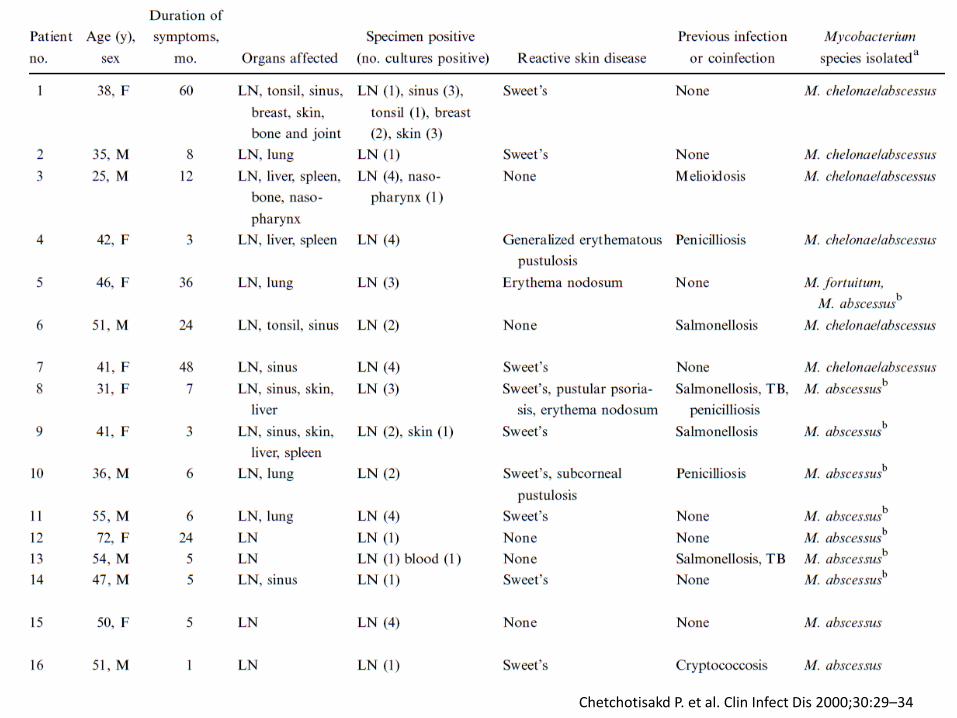
Chetchotisakd P. et al. Clin Infect Dis 2000;30:29–34
Reported 16 cases of rapidly growing Mycobacterium (RGM) from 1994 - 1998 • All had chronic bilateral cervical lymphadenopathy • 12/16 had involvement of other organs (sinuses, 6; lungs, 4; liver, 4; spleen, 3; skin, 3; bone and joint, 2; and tonsils, 2)
Chetchotisakd P. et al. Clin Infect Dis 2000;30:29–34
• 11/16 had 14 episodes of reactive skin manifestations (Sweet’s syndrome, 9; generalized pustulosis and erythema nodosum, 2 each; and pustular psoriasis, 1) • 8/16 had 11 episodes of other opportunistic
pathogens (salmonellosis, 4; penicilliosis, 3; pulmonary tuberculosis, 2; and melioidosis and cryptococcosis, 1 each)
Chetchotisakd P. et al. Clin Infect Dis 2000;30:29–34
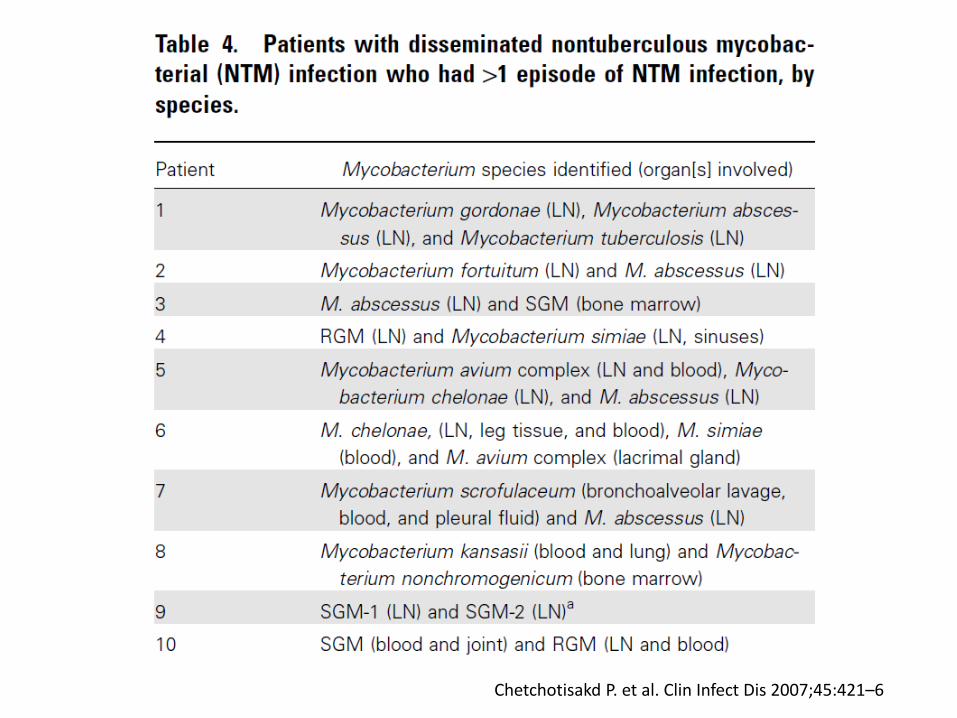
Chetchotisakd P. et al. Clin Infect Dis 2007;45:421–6
From 1994-2006, there were 129 cases • All patients but 1 were adults • 99 cases due to RGM and 34 due to SGM
Chetchotisakd P. et al. Clin Infect Dis 2007;45:421–6
Chetchotisakd P. et al. Clin Infect Dis 2007;45:421–6
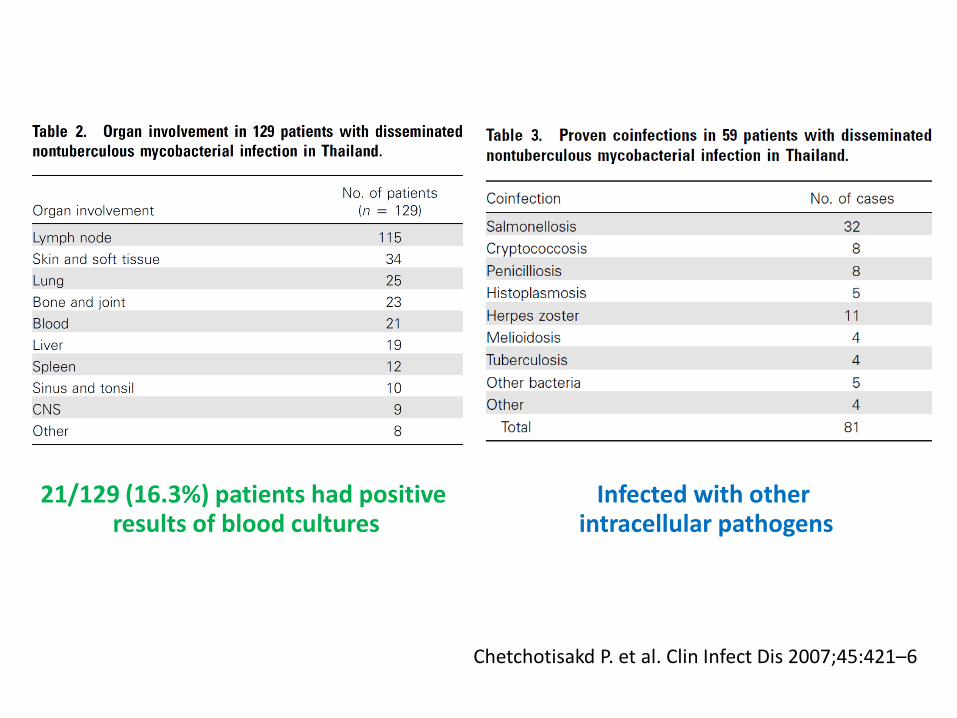
21/129 (16.3%) patients had positive results of blood cultures
Infected with other intracellular pathogens
Chetchotisakd P. et al. Clin Infect Dis 2007;45:421–6
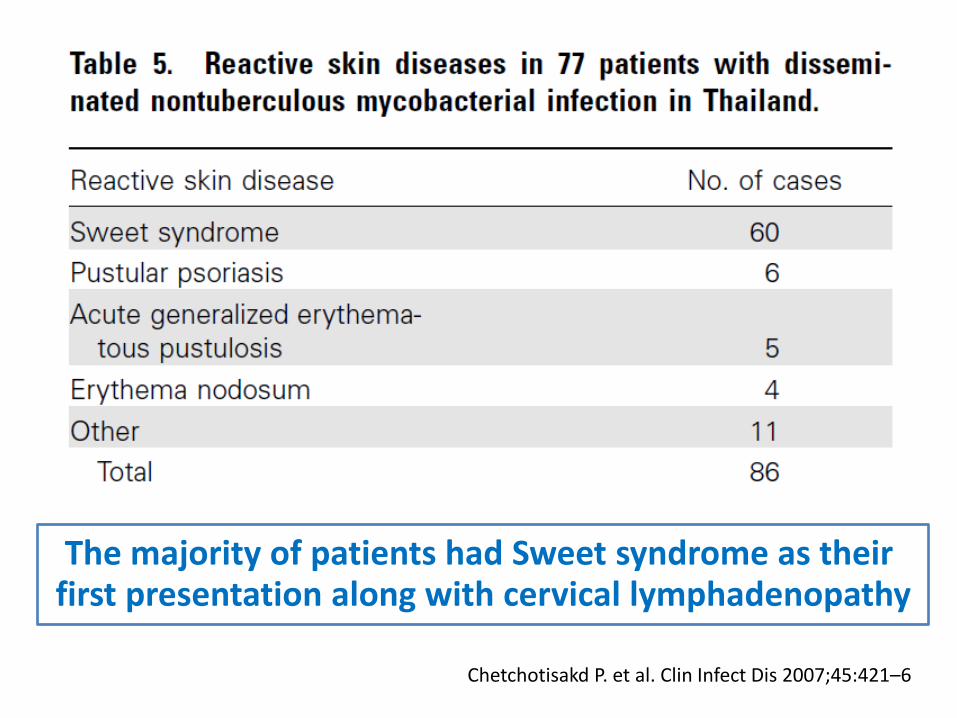
The majority of patients had Sweet syndrome as their first presentation along with cervical lymphadenopathy
Chetchotisakd P. et al. Clin Infect Dis 2007;45:421–6
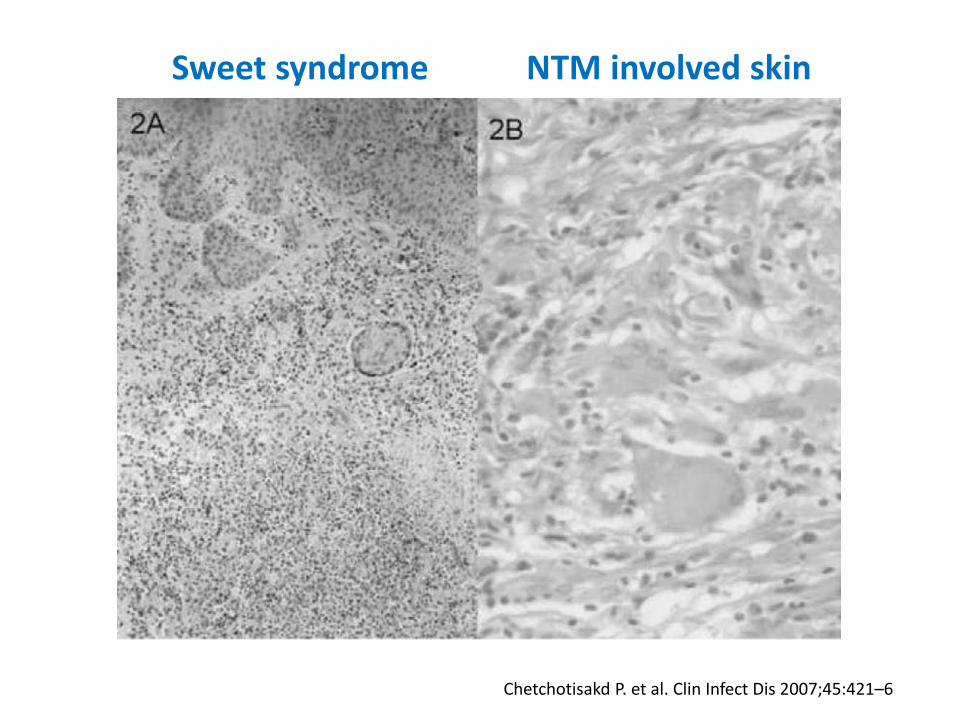
Sweet syndrome NTM involved skin
Chetchotisakd P. et al. Clin Infect Dis 2007;45:421–6
Anti–IFN- IgG autoantibodies were also present in 5 anonymous serum samples obtained
from the patients tested
Hoflich C. et al. Blood. 2004;103:673-5
A 25-year-old Thai woman, Anti – HIV – negative • Necrotizing lymphadenitis, tonsillitis, bilateral pneumonia, splenic and intracerebral abscesses, and osteomyelitis from Burkholderia cocovenenans (16S rDNA sequence)
• Fatal septic shock from Mycobacterium chelonae
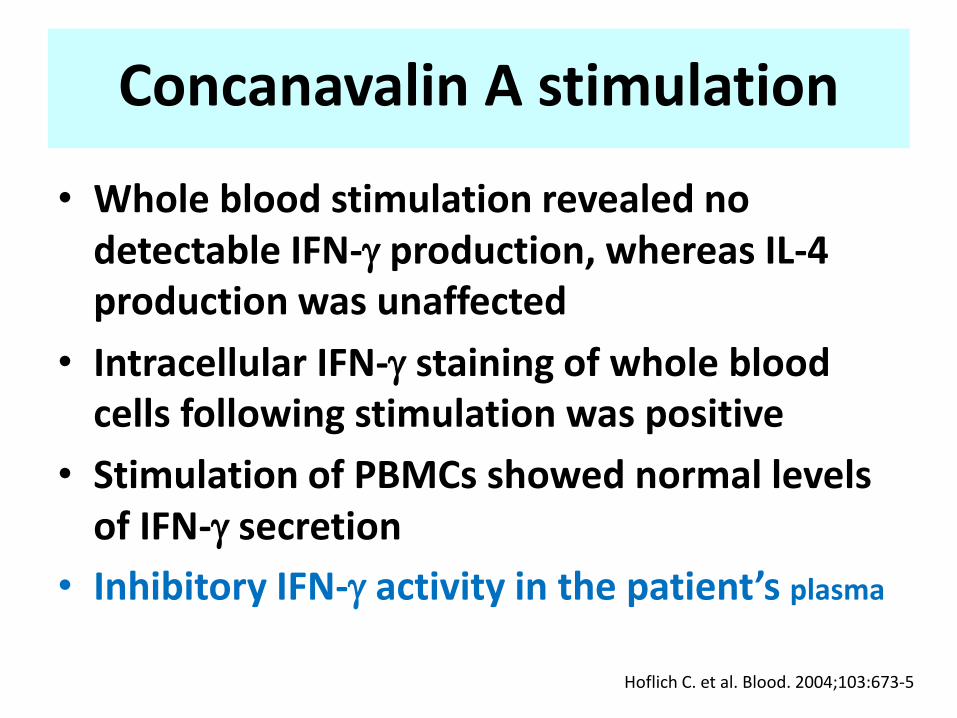
Concanavalin A stimulation
• Whole blood stimulation revealed no detectable IFN- production, whereas IL-4 production was unaffected
• Intracellular IFN- staining of whole blood cells following stimulation was positive
• Stimulation of PBMCs showed normal levels of IFN- secretion
• Inhibitory IFN- activity in the patient’s plasma
Hoflich C. et al. Blood. 2004;103:673-5
Hoflich C. et al. Blood. 2004;103:673-5
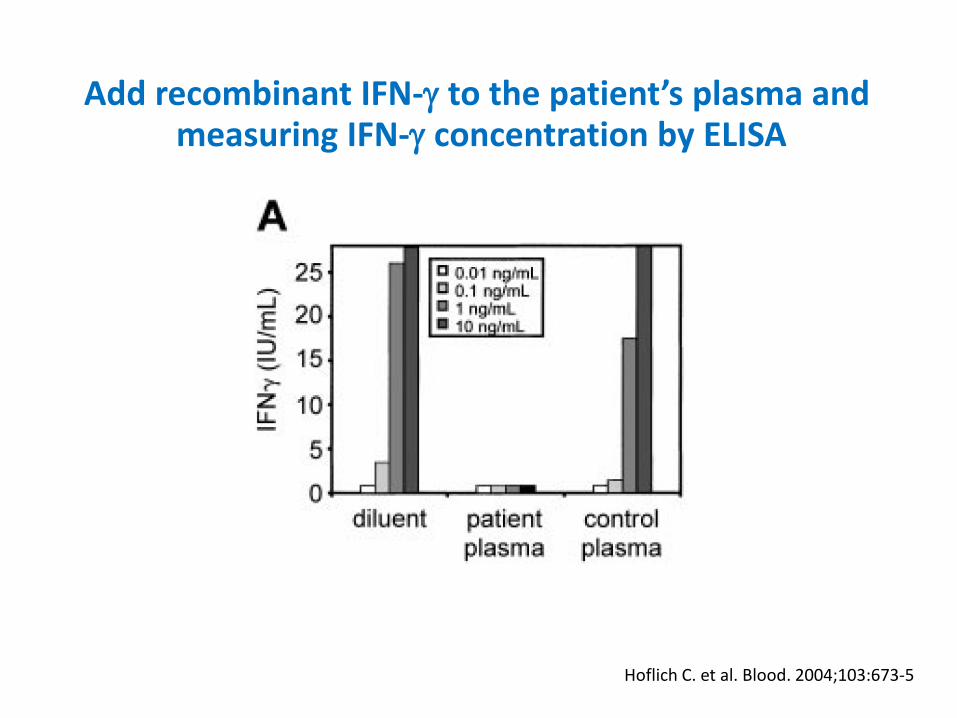
Add recombinant IFN- to the patient’s plasma and measuring IFN- concentration by ELISA
Hoflich C. et al. Blood. 2004;103:673-5
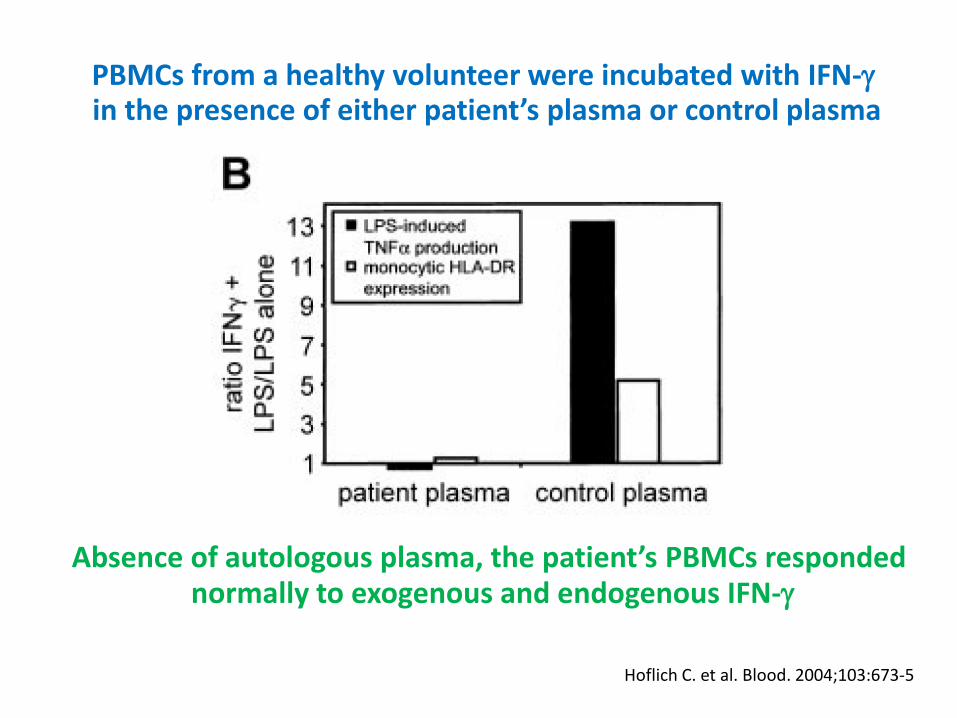
PBMCs from a healthy volunteer were incubated with IFN- in the presence of either patient’s plasma or control plasma
Absence of autologous plasma, the patient’s PBMCs responded normally to exogenous and endogenous IFN-
Hoflich C. et al. Blood. 2004;103:673-5
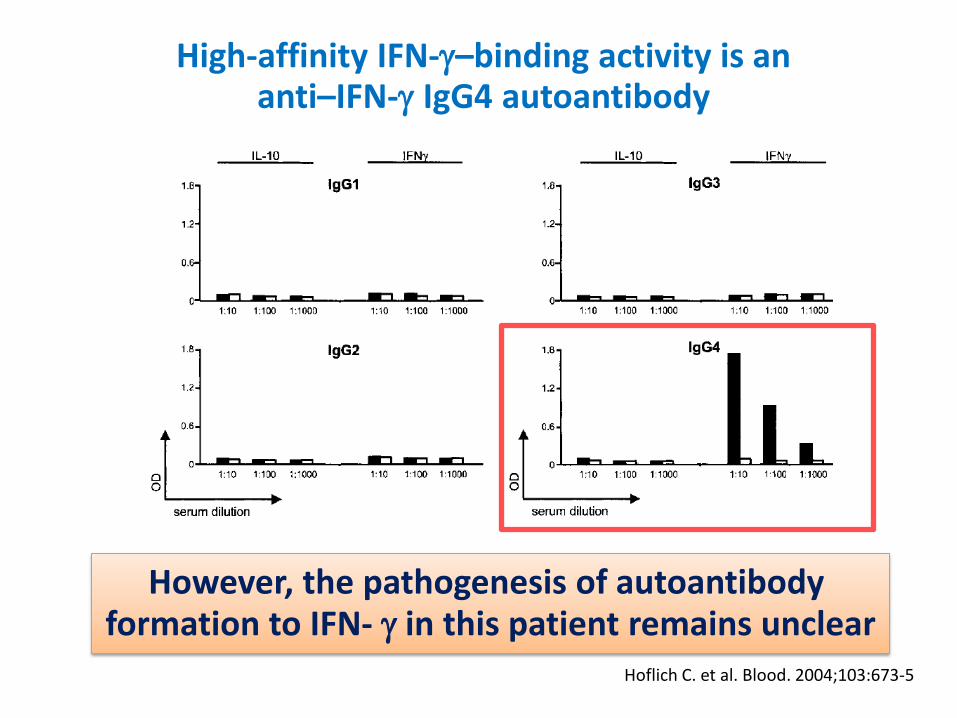
High-affinity IFN-–binding activity is an anti–IFN- IgG4 autoantibody
However, the pathogenesis of autoantibody formation to IFN- in this patient remains unclear

Doffinger R. et al. Clin Infect Dis 2004;38:e10-4
Autoantibodies to Interferon- in a Patient with Selective Susceptibility to Mycobacterial
Infection and Organ-Specific Autoimmunity
A 47-year-old, previously fit, Filipino man • Disseminated Mycobacterium tuberculosis • Disseminated Mycobacterium chelonae

Doffinger R. et al. Clin Infect Dis 2004;38:e10-4
Autoantibodies to Interferon- in a Patient with Selective Susceptibility to Mycobacterial
Infection and Organ-Specific Autoimmunity Anti–IFN- activity
Impaired IFN- and IL-12 secretion
PBMC + 5% autologous serum

Doffinger R. et al. Clin Infect Dis 2004;38:e10-4
Autoantibodies to Interferon- in a Patient with Selective Susceptibility to Mycobacterial
Infection and Organ-Specific Autoimmunity
Mendelian defects in IL-12–dependent INF- pathway were excluded by sequencing the IFNGR1, IFNGR2,
STAT1, IL12B, and IL-12RB1 genes
Doffinger R. et al. Clin Infect Dis 2004;38:e10-4
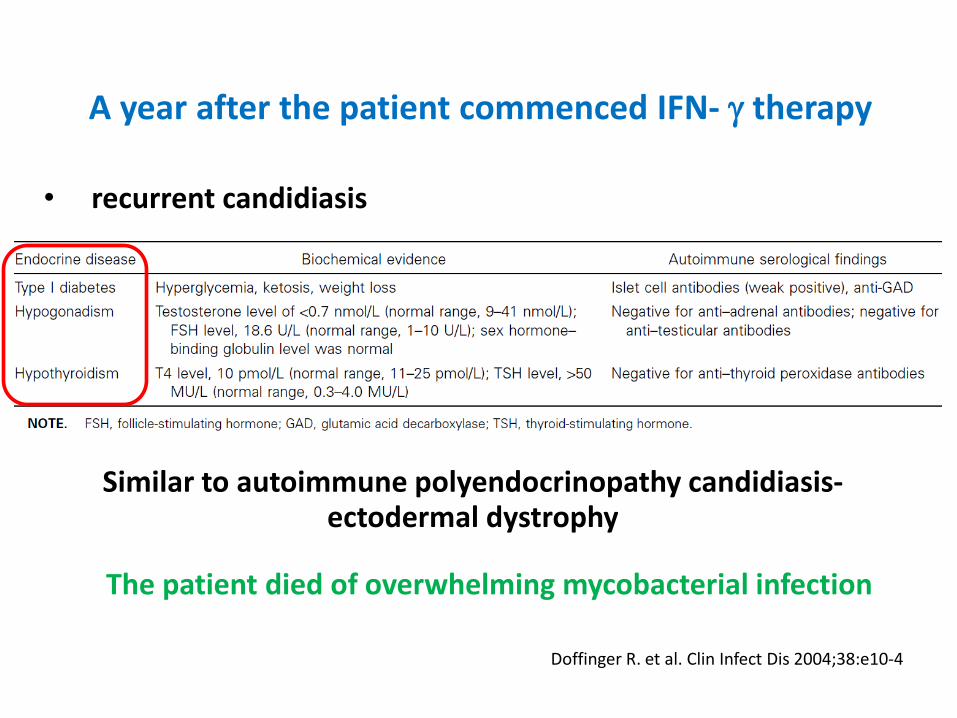
A year after the patient commenced IFN- therapy
• recurrent candidiasis
The patient died of overwhelming mycobacterial infection
Similar to autoimmune polyendocrinopathy candidiasis- ectodermal dystrophy
From 2004-2005 • 11 cases from 4 reports
• 8/11 were Asians
5 were Filipino
1 was Taiwanese
1 was Vietnamese
1 was Thai
Hoflich C. et al. Blood. 2004;103:673-5 Doffinger R. et al. Clin Infect Dis 2004;38:e10-4
Kampmann B. et al. J Clin Invest 2005;115:2480-8 Patel SY. et al. J Immunol 2005;175:4769-76
Interferon- and interleukin-12 pathways
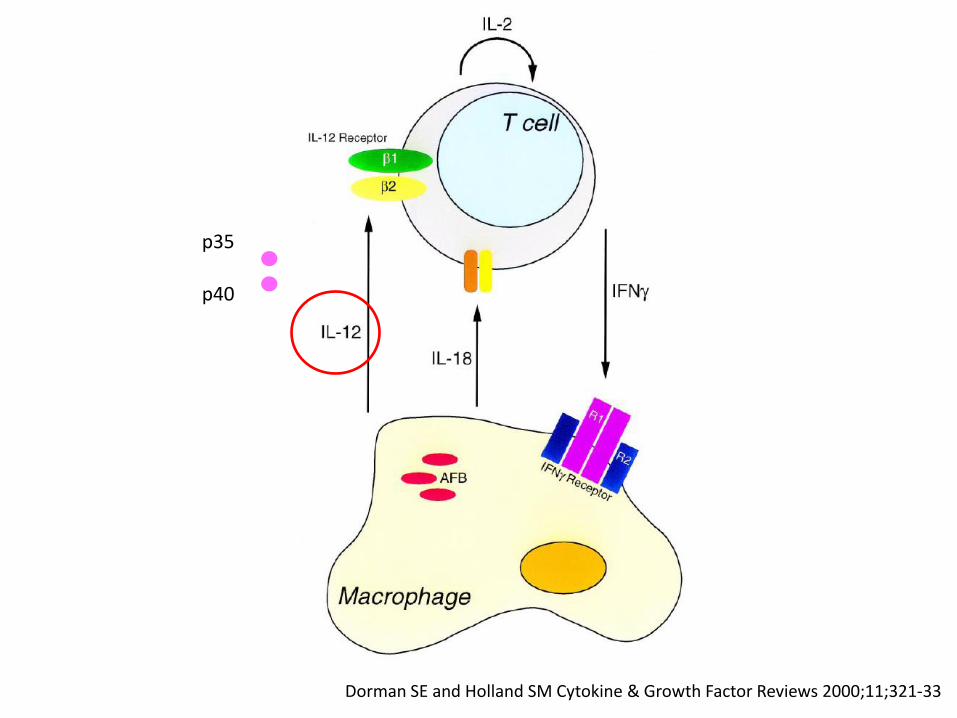
Dorman SE and Holland SM Cytokine & Growth Factor Reviews 2000;11;321-33
p35
p40
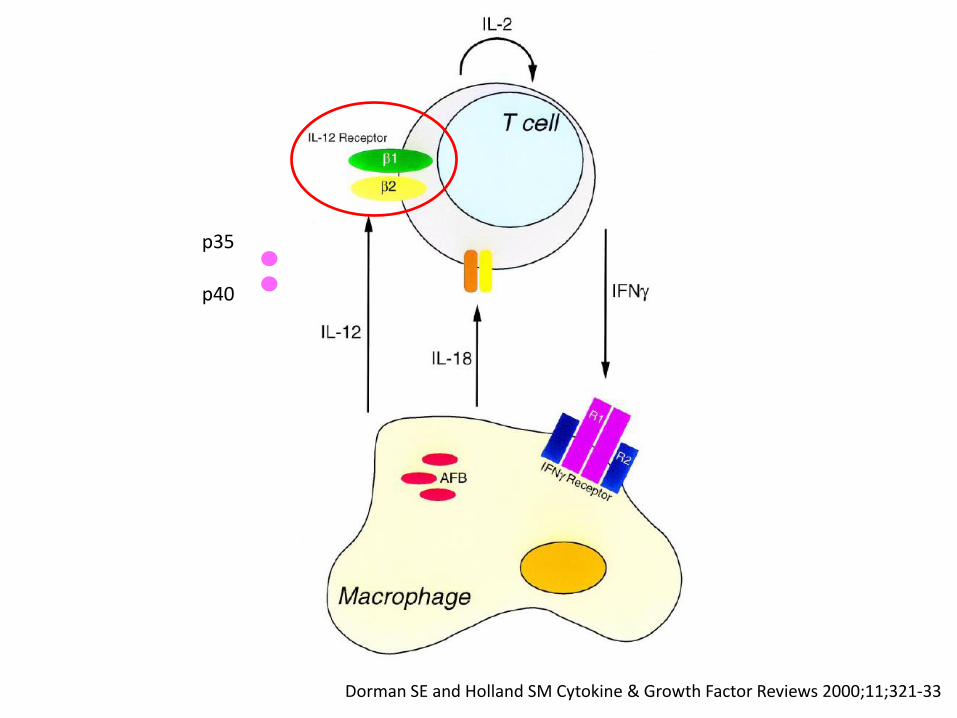
Dorman SE and Holland SM Cytokine & Growth Factor Reviews 2000;11;321-33
p35
p40
Dorman SE and Holland SM Cytokine & Growth Factor Reviews 2000;11;321-33
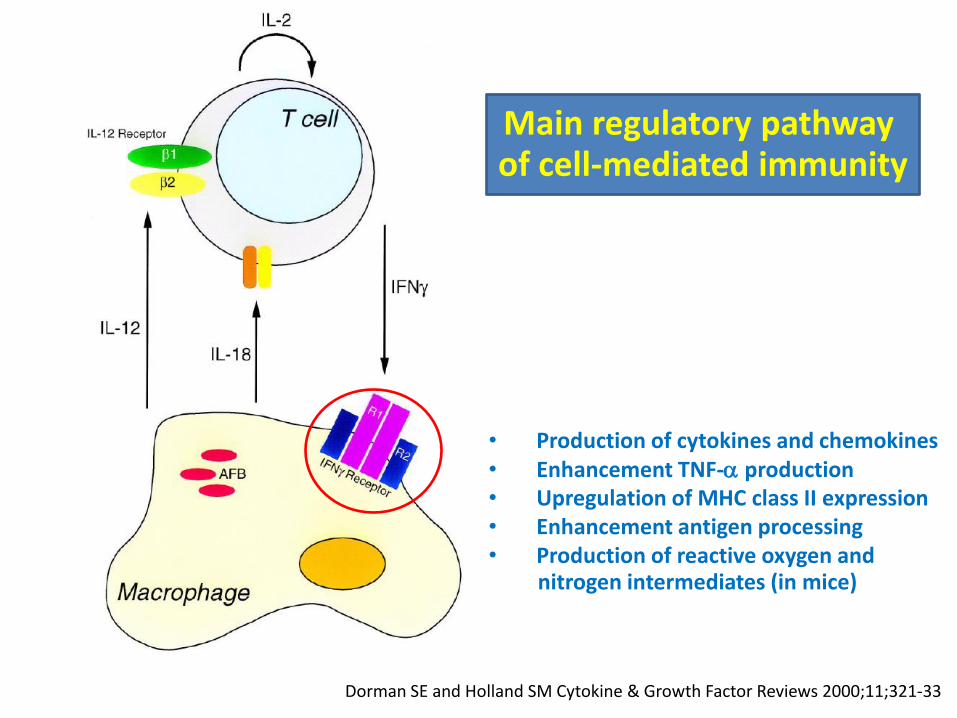
• Production of cytokines and chemokines • Enhancement TNF- production • Upregulation of MHC class II expression • Enhancement antigen processing • Production of reactive oxygen and nitrogen intermediates (in mice)
Main regulatory pathway of cell-mediated immunity
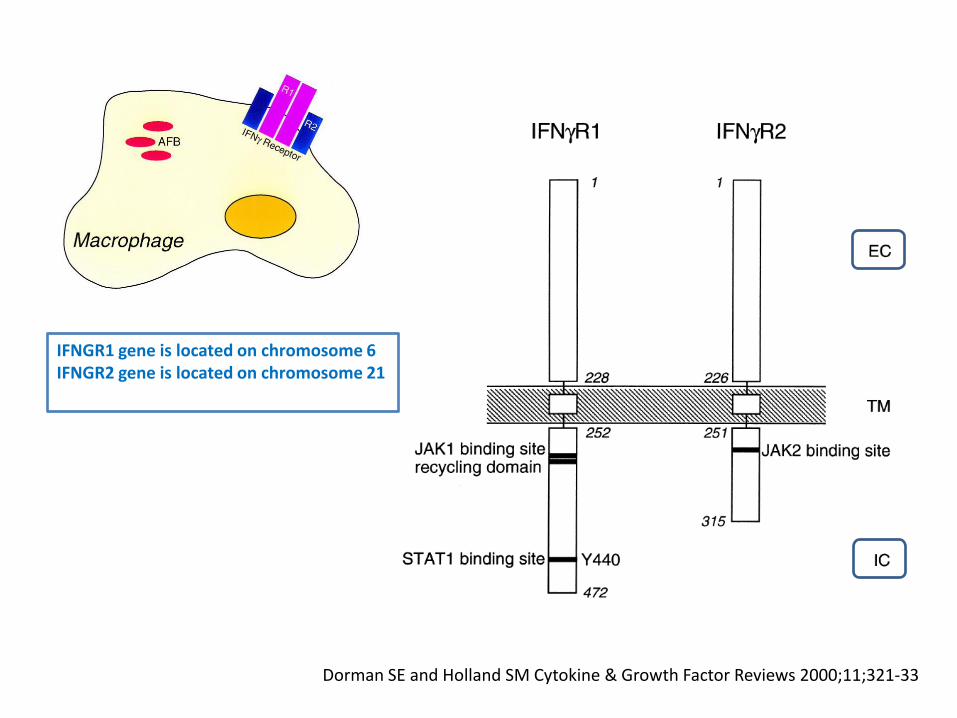
Dorman SE and Holland SM Cytokine & Growth Factor Reviews 2000;11;321-33
IFNGR1 gene is located on chromosome 6 IFNGR2 gene is located on chromosome 21
Dorman SE and Holland SM Cytokine & Growth Factor Reviews 2000;11;321-33
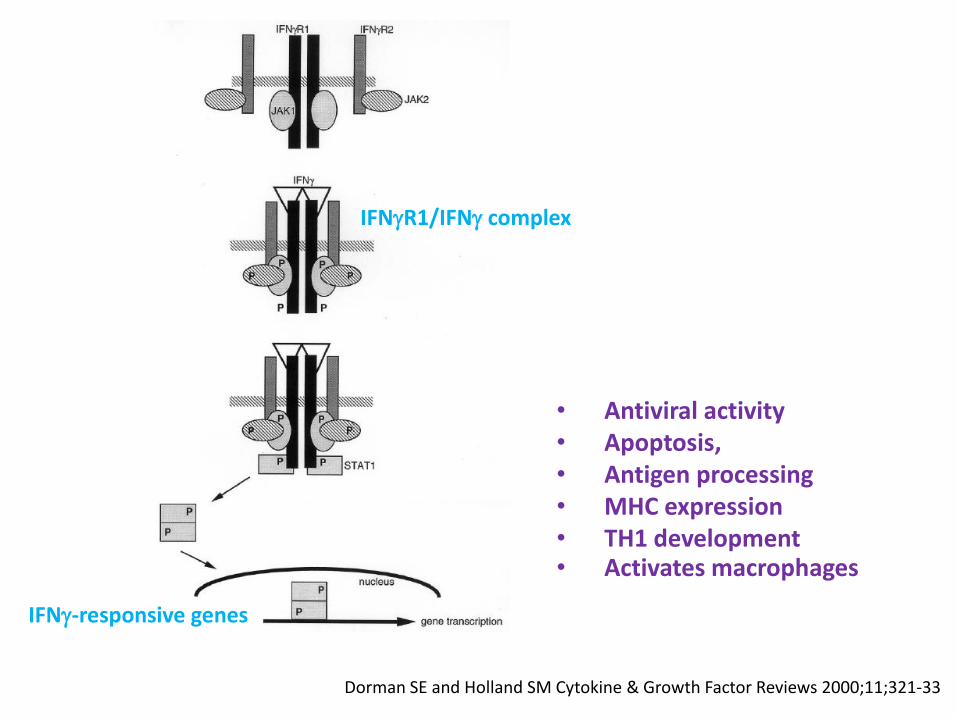
IFNR1/IFN complex
IFN-responsive genes
• Antiviral activity • Apoptosis, • Antigen processing • MHC expression • TH1 development • Activates macrophages
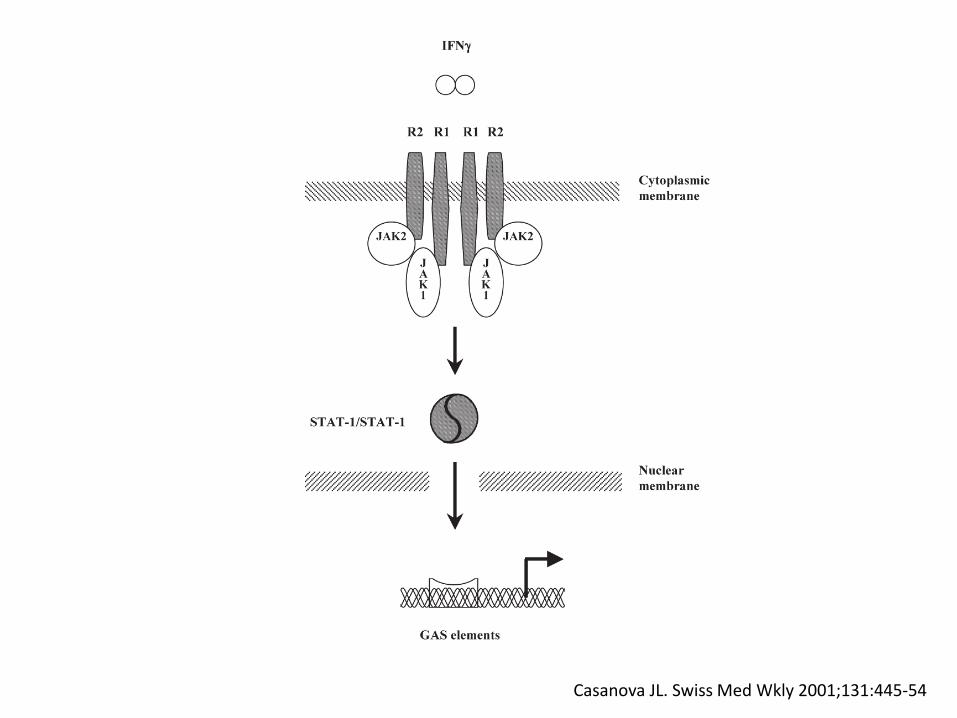
Casanova JL. Swiss Med Wkly 2001;131:445-54
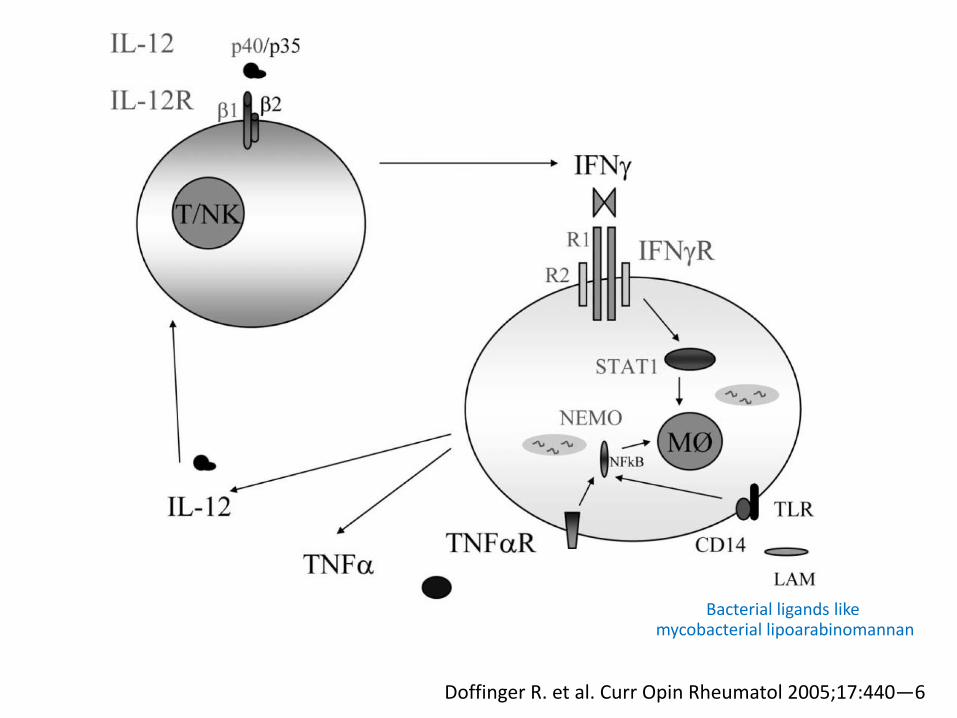
Doffinger R. et al. Curr Opin Rheumatol 2005;17:440—6
Bacterial ligands like mycobacterial lipoarabinomannan
Natural anti–INF- antibodies
Have been reported in patients with
• Tuberculosis
• Viral diseases
• Healthy subjects
• HIV-infected individuals
• Experimental African trypanosomiasis
Doffinger R. et al. Clin Infect Dis 2004;38:e10-4
But the potential pathogenic impact of these antibodies has not been established
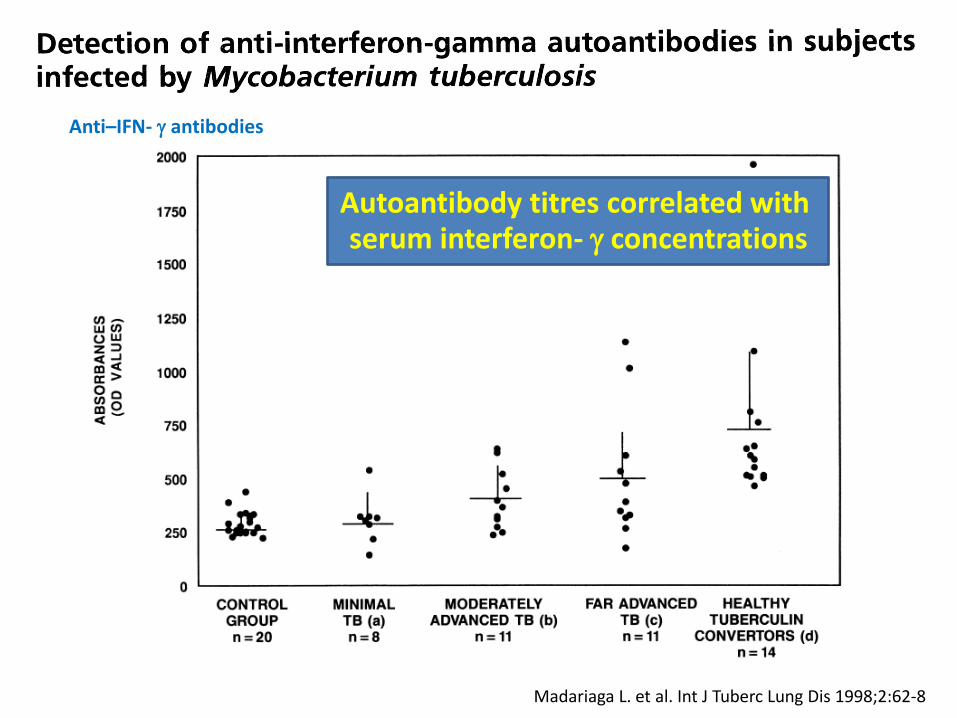
Madariaga L. et al. Int J Tuberc Lung Dis 1998;2:62-8
Anti–IFN- antibodies
Autoantibody titres correlated with serum interferon- concentrations
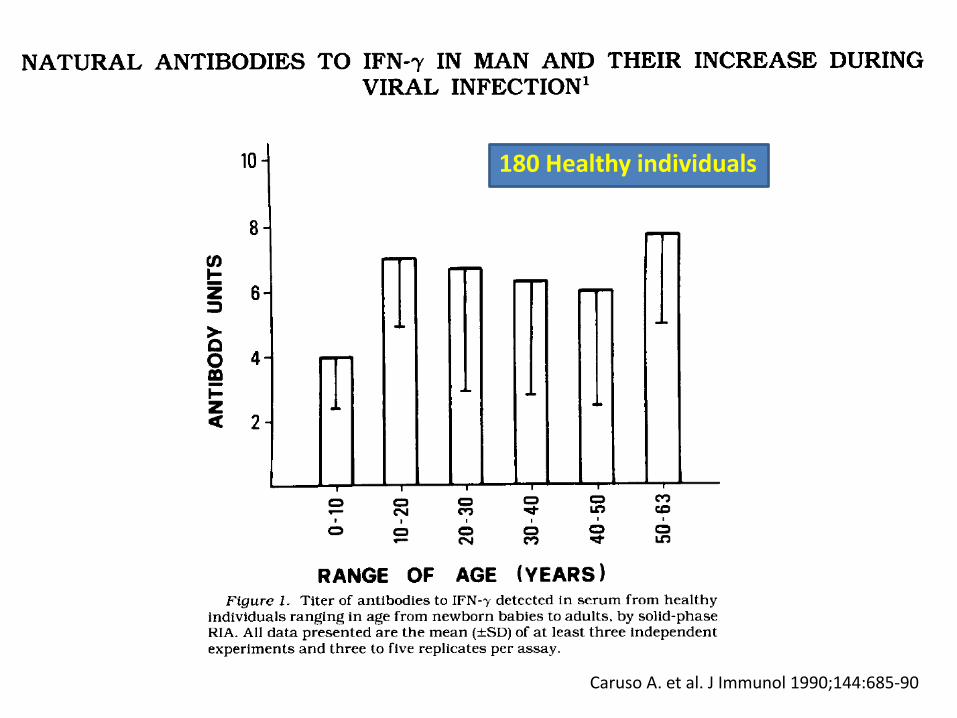
Caruso A. et al. J Immunol 1990;144:685-90
180 Healthy individuals
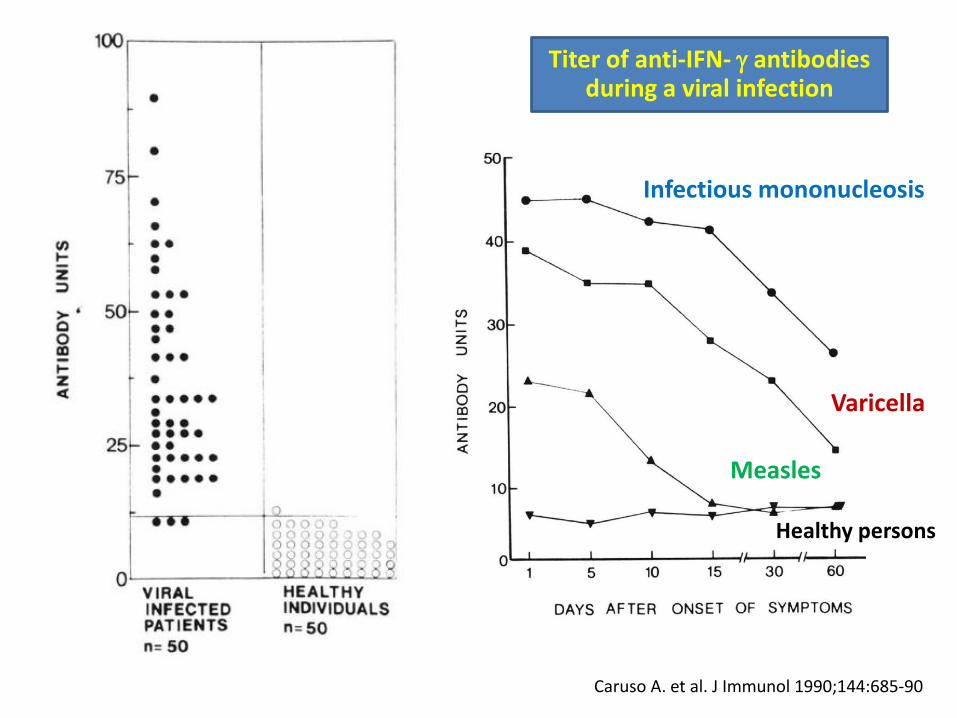
Caruso A. et al. J Immunol 1990;144:685-90
Titer of anti-IFN- antibodies during a viral infection
Infectious mononucleosis
Varicella
Measles
Healthy persons
Natural anti–INF- antibodies in healthy patients were detected in low titers and
been biologically inactive without antagonist activity against IFN- signaling
Lee WI. et al. Immunobiology 2013;218:762–71
Browne SK et al. N Engl J Med 2012;367:725-34
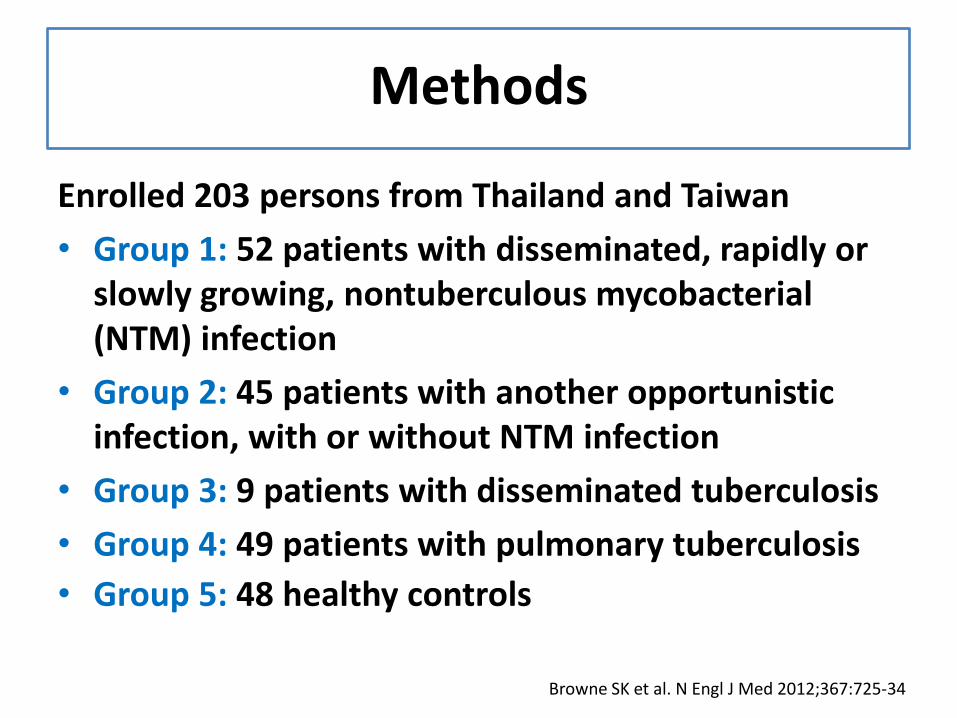
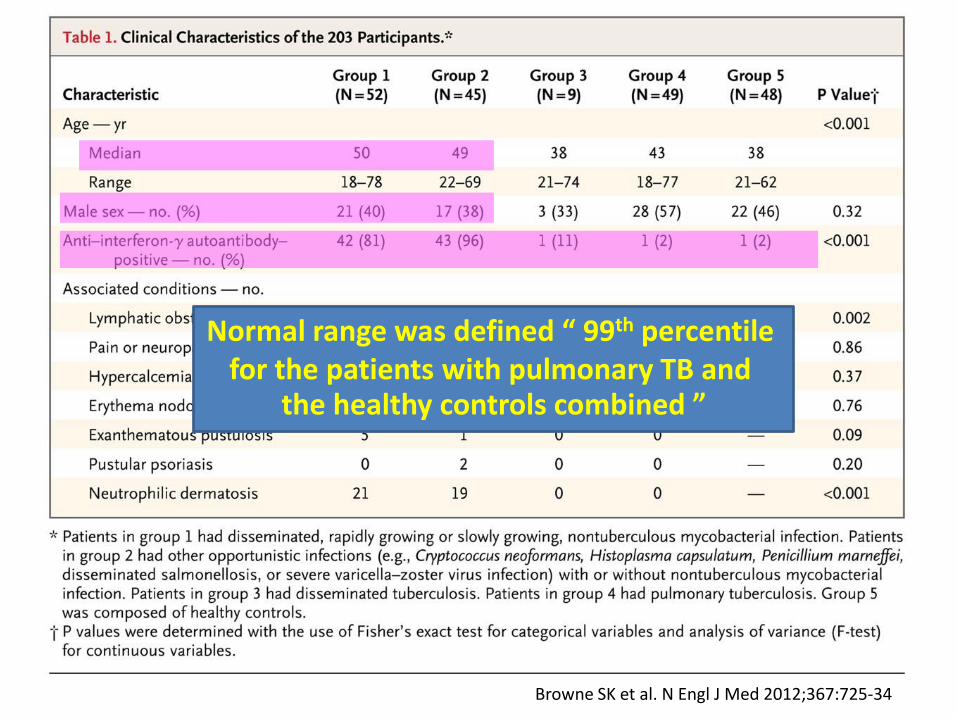
Methods
Enrolled 203 persons from Thailand and Taiwan
• Group 1: 52 patients with disseminated, rapidly or slowly growing, nontuberculous mycobacterial (NTM) infection
• Group 2: 45 patients with another opportunistic infection, with or without NTM infection
• Group 3: 9 patients with disseminated tuberculosis
• Group 4: 49 patients with pulmonary tuberculosis
• Group 5: 48 healthy controls
Browne SK et al. N Engl J Med 2012;367:725-34
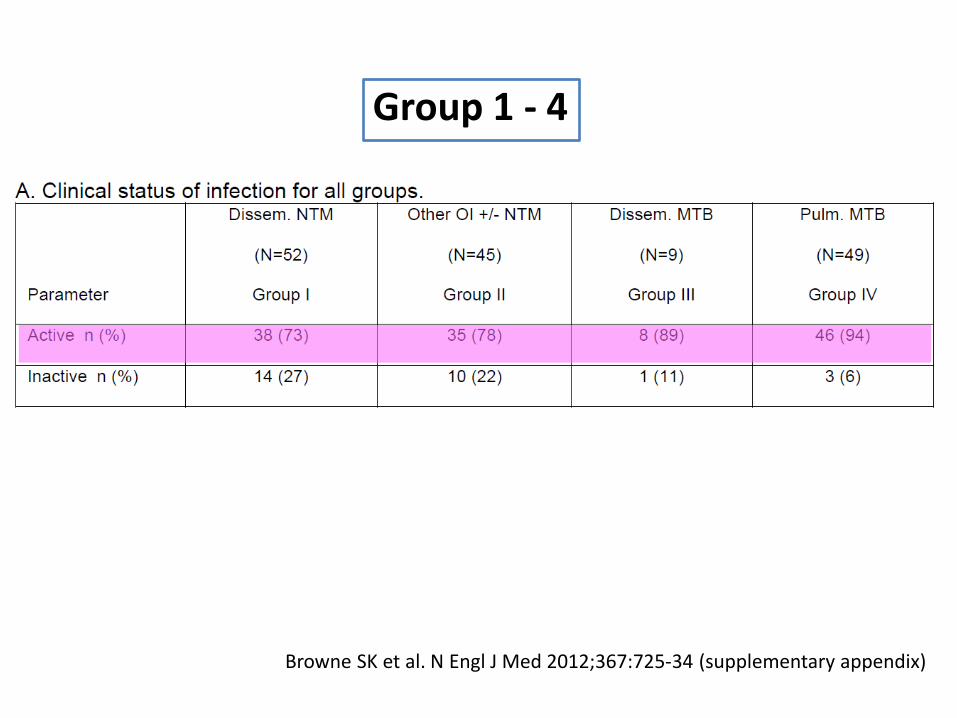
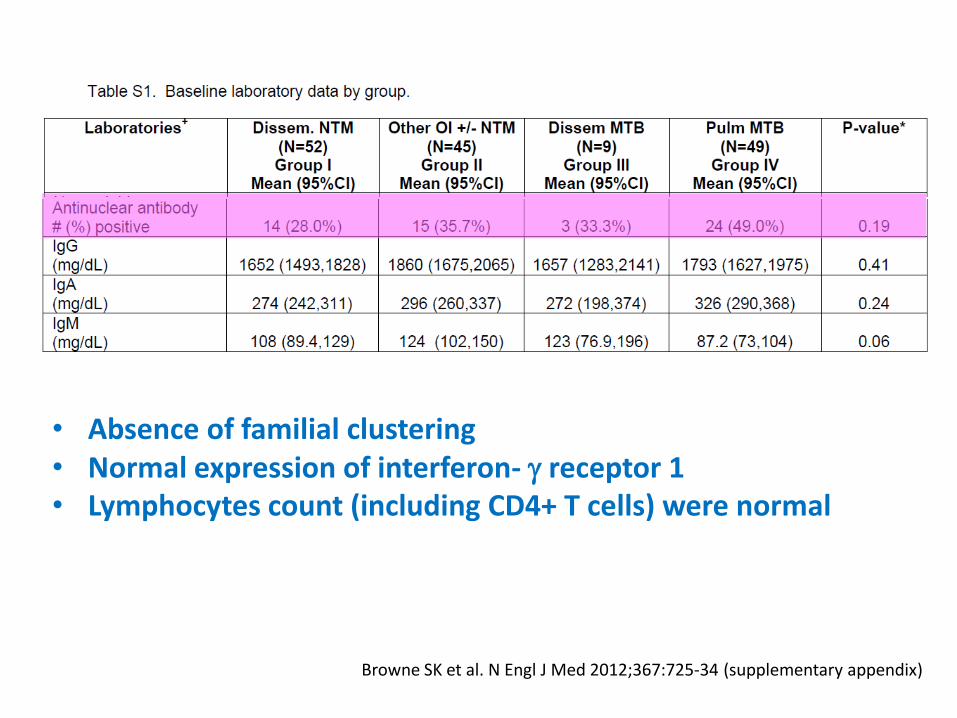
Browne SK et al. N Engl J Med 2012;367:725-34 (supplementary appendix)
Group 1 - 4
Browne SK et al. N Engl J Med 2012;367:725-34
Normal range was defined “ 99th percentile for the patients with pulmonary TB and
the healthy controls combined ”
Browne SK et al. N Engl J Med 2012;367:725-34
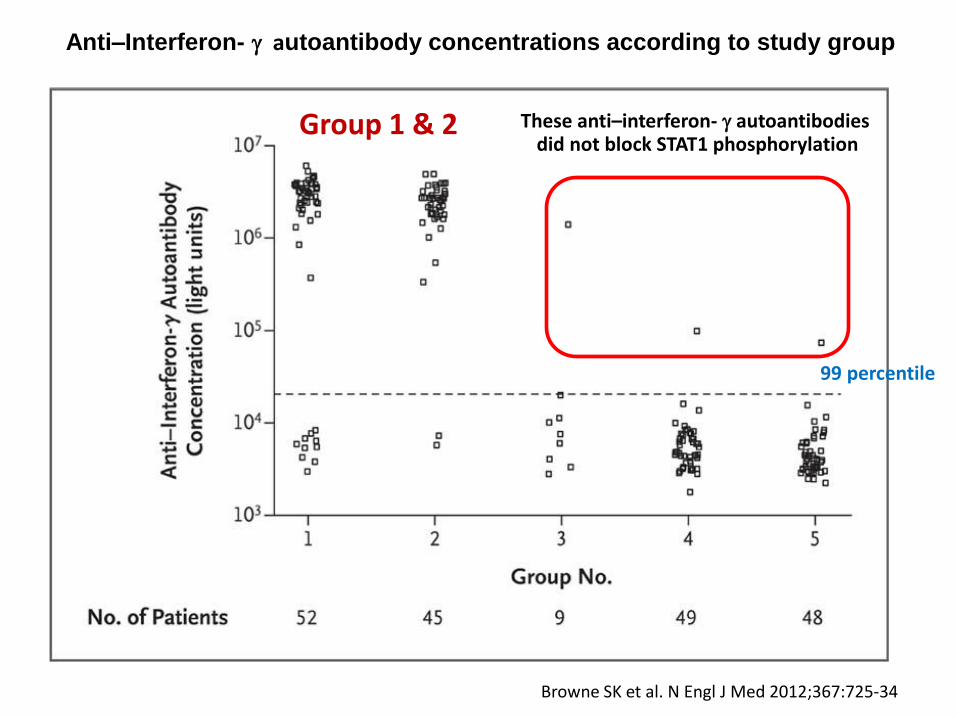
Anti–Interferon- autoantibody concentrations according to study group
Group 1 & 2
99 percentile
These anti–interferon- autoantibodies did not block STAT1 phosphorylation
Browne SK et al. N Engl J Med 2012;367:725-34 (supplementary appendix)
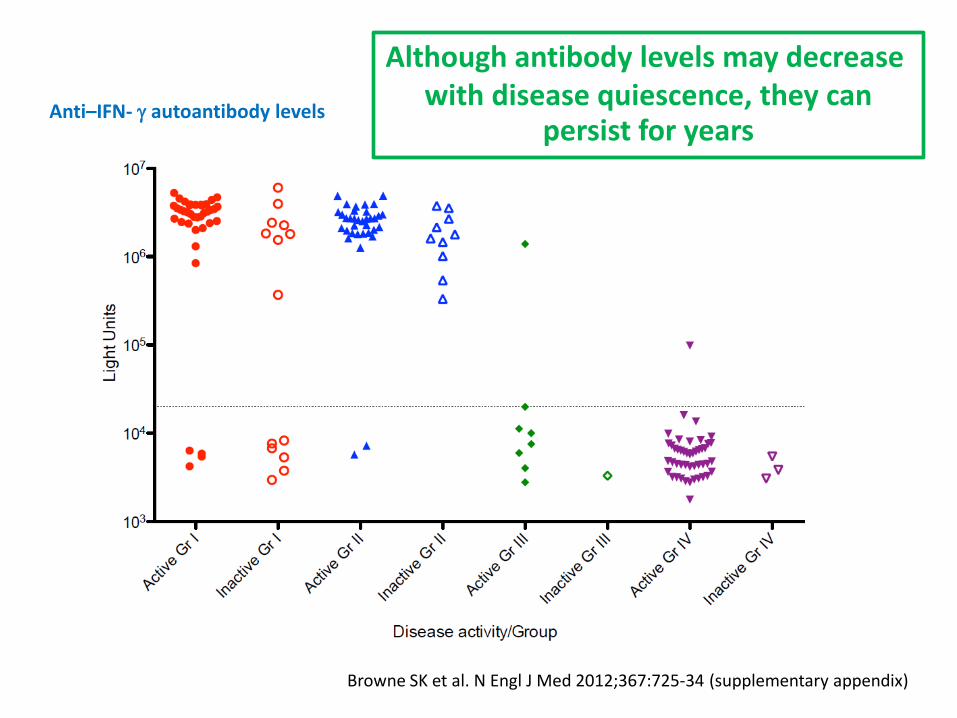
Anti–IFN- autoantibody levels
Although antibody levels may decrease with disease quiescence, they can
persist for years
Browne SK et al. N Engl J Med 2012;367:725-34 (supplementary appendix)
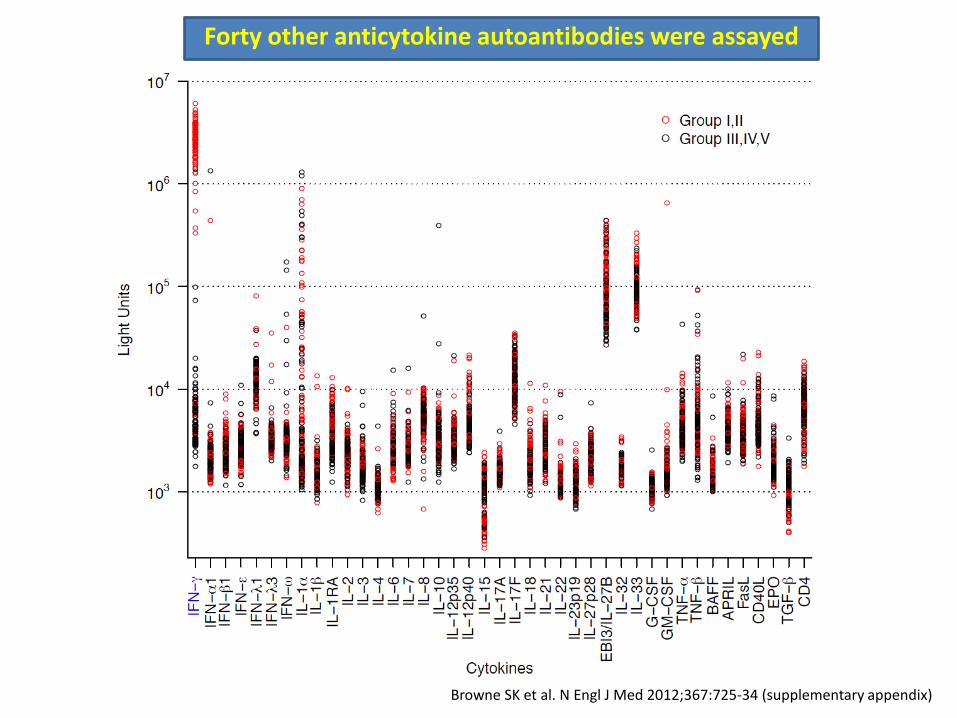
Forty other anticytokine autoantibodies were assayed

Browne SK et al. N Engl J Med 2012;367:725-34 (supplementary appendix)
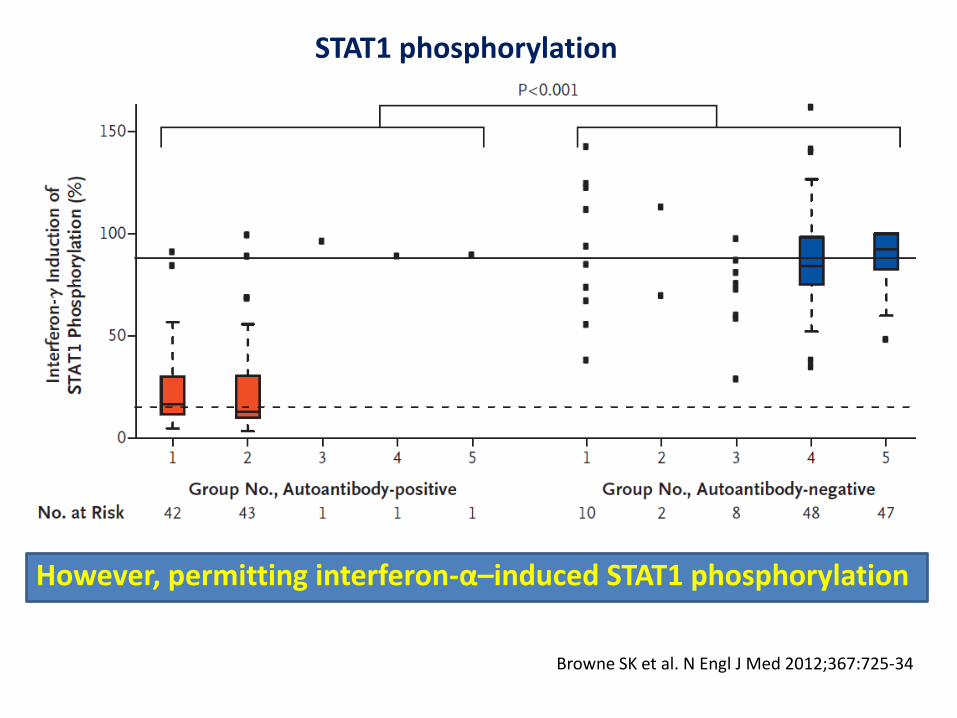
Browne SK et al. N Engl J Med 2012;367:725-34
STAT1 phosphorylation
However, permitting interferon-α–induced STAT1 phosphorylation
Browne SK et al. N Engl J Med 2012;367:725-34 (supplementary appendix)
• Absence of familial clustering • Normal expression of interferon- receptor 1 • Lymphocytes count (including CD4+ T cells) were normal
Remarks • Trigger for production of these
autoantibodies remains elusive
• Nearly all patients identified have been Asian-born Asians, implicates host genetic factors, environmental exposure, or both
Browne SK et al. N Engl J Med 2012;367:725-34
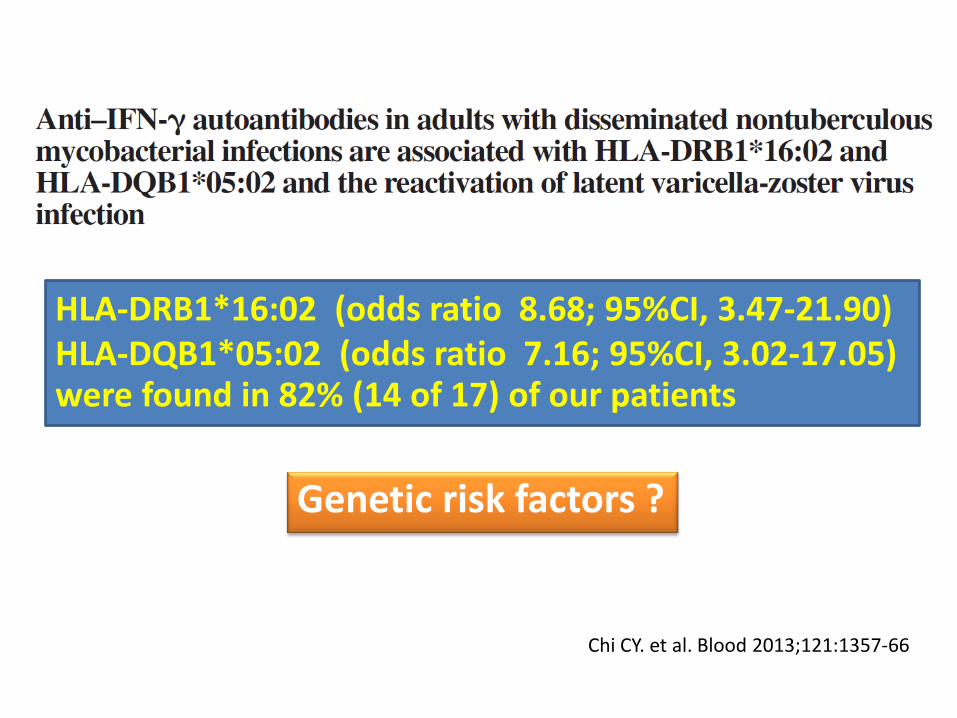
Chi CY. et al. Blood 2013;121:1357-66
HLA-DRB1*16:02 (odds ratio 8.68; 95%CI, 3.47-21.90) HLA-DQB1*05:02 (odds ratio 7.16; 95%CI, 3.02-17.05) were found in 82% (14 of 17) of our patients
Genetic risk factors ?
Genetic risk Factors ? Even the largest cohort of patients
• No familial clustering
• Few reported in Asians born outside of Asia
Browne SK. et al. Annu Rev Immunol 2014;32:635–57
Suggesting 1. Genetics are likely complex 2. Environmental factors, possibly early in life, may contribute to
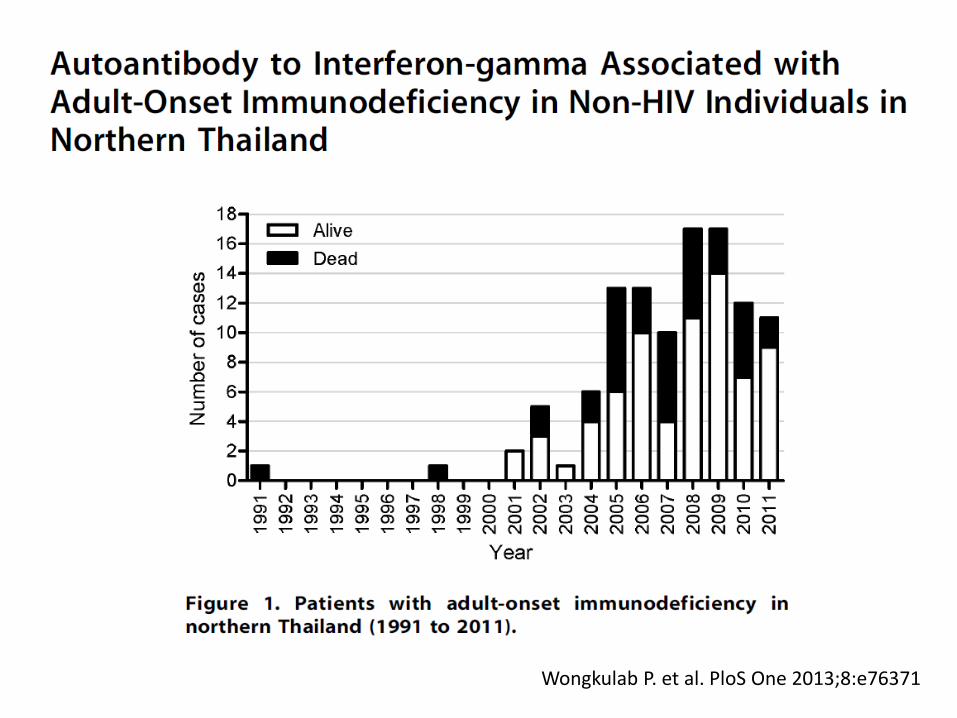
Wongkulab P. et al. PloS One 2013;8:e76371

Wongkulab P. et al. PloS One 2013;8:e76371
Mean 2.460 ± 1.309 O.D. among cases Mean 0.058 ± 0.004 O.D. among HIV Mean 0.059 ± 0.005 O.D. among controls
n 20 20 20
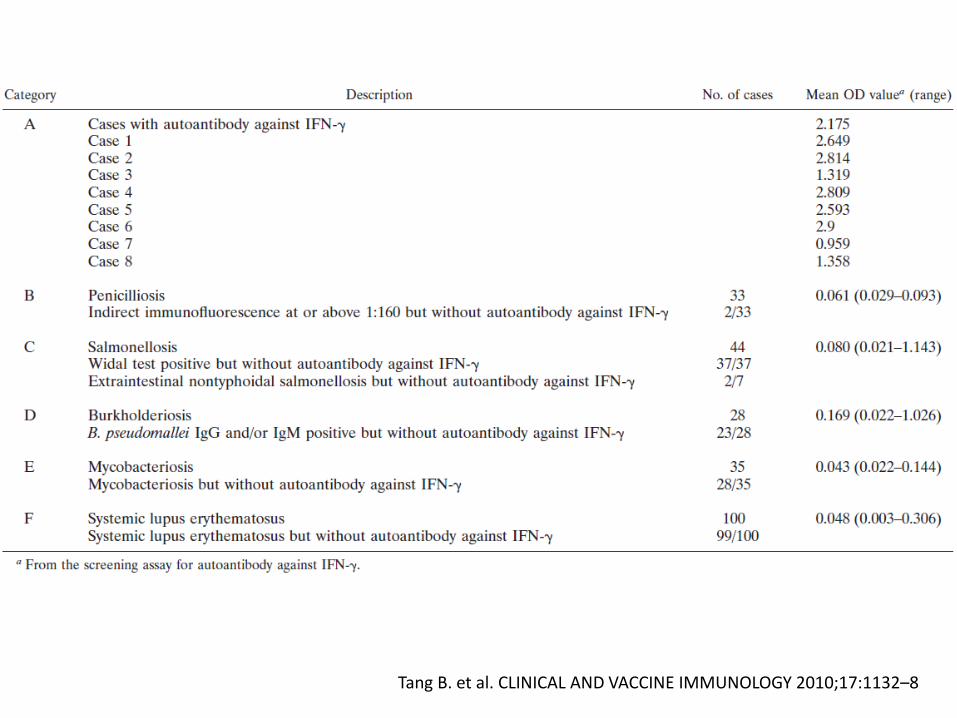
Tang B. et al. CLINICAL AND VACCINE IMMUNOLOGY 2010;17:1132–8
Subgroup analysis: • level of autoantibody in patients with active infections was relatively higher than those without (mean 3.279 ± 0.662 Vs 0.939 ± 0.630 O.D.) • level of autoantibody may have a role in monitoring disease activity or recurrence of the disease
Wongkulab P. et al. PloS One 2013;8:e76371
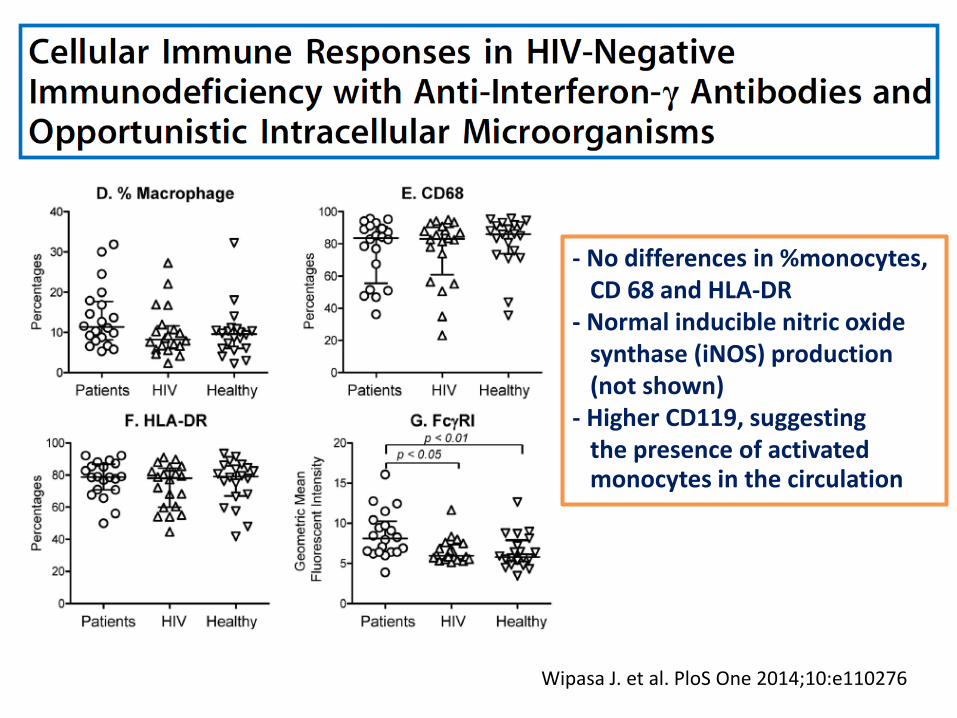
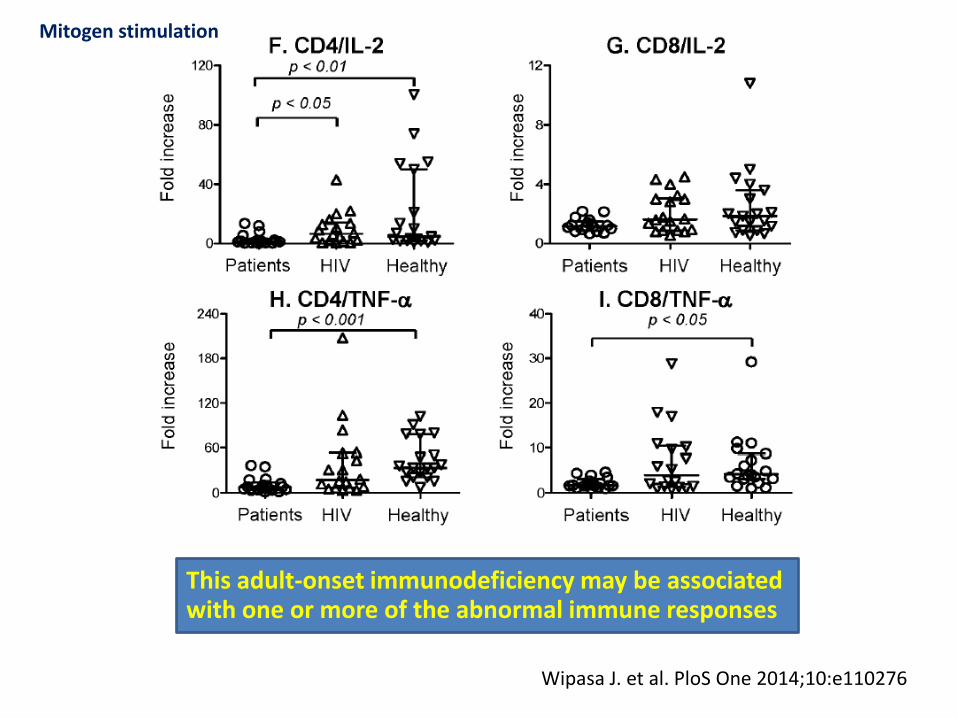
Wipasa J. et al. PloS One 2014;10:e110276
- No differences in %monocytes, CD 68 and HLA-DR - Normal inducible nitric oxide synthase (iNOS) production (not shown) - Higher CD119, suggesting the presence of activated monocytes in the circulation
Wipasa J. et al. PloS One 2014;10:e110276
This adult-onset immunodeficiency may be associated with one or more of the abnormal immune responses
Mitogen stimulation
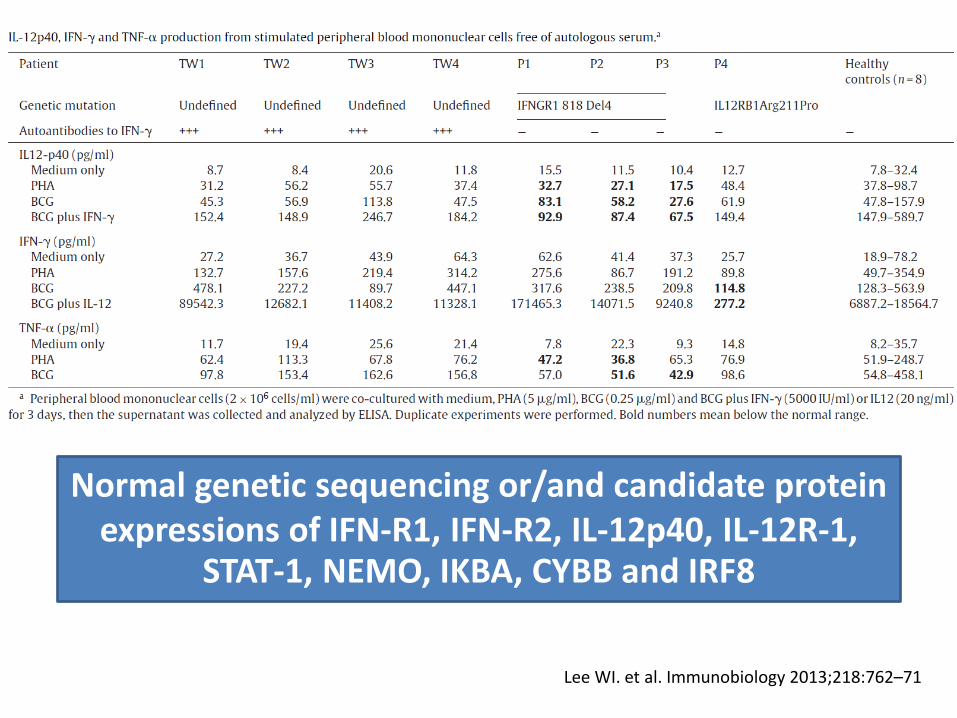
Lee WI. et al. Immunobiology 2013;218:762–71
Normal genetic sequencing or/and candidate protein expressions of IFN-R1, IFN-R2, IL-12p40, IL-12R-1,
STAT-1, NEMO, IKBA, CYBB and IRF8
Suggest including anti-IFN- autoantibodies
in the differential diagnosis of
• HIV-negative adult patients with unknown cell-mediated immunodeficiency
• Severe, persistent or recurrent infections caused by NTM
or Salmonella
• Especially in Asian patients
• Reactive skin lesions or autoimmune endocrinopathy
Kampitak T. et al. Infection 2011;39:65–71
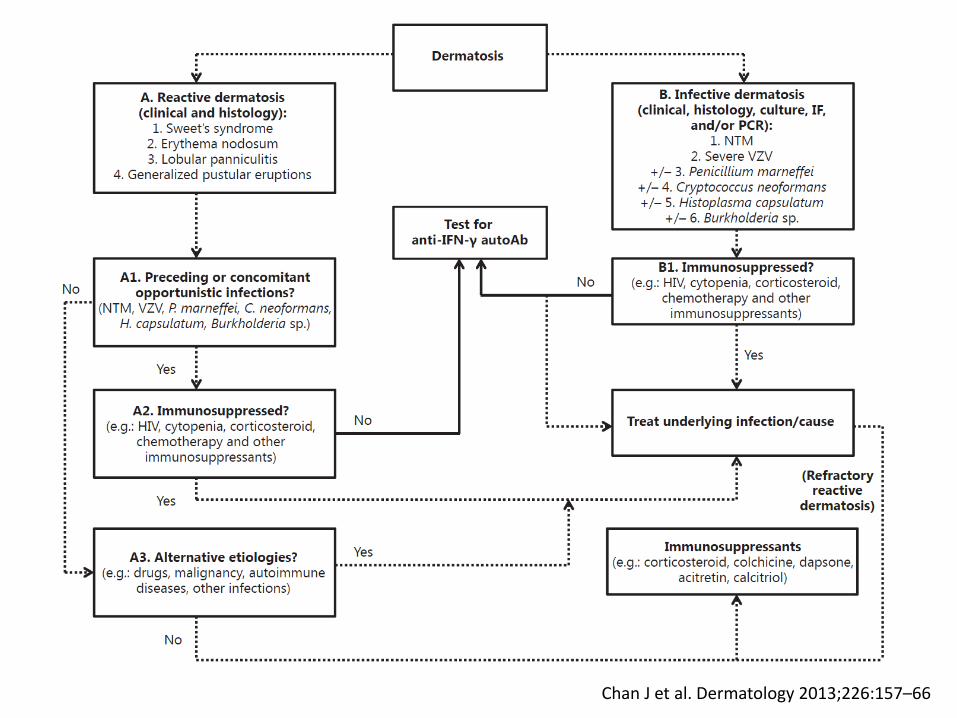
Chan J et al. Dermatology 2013;226:157–66

Chan J et al. Dermatology 2013;226:157–66
1. Progressive painful erythematous papules over 2 weeks
Chan J et al. Dermatology 2013;226:157–66
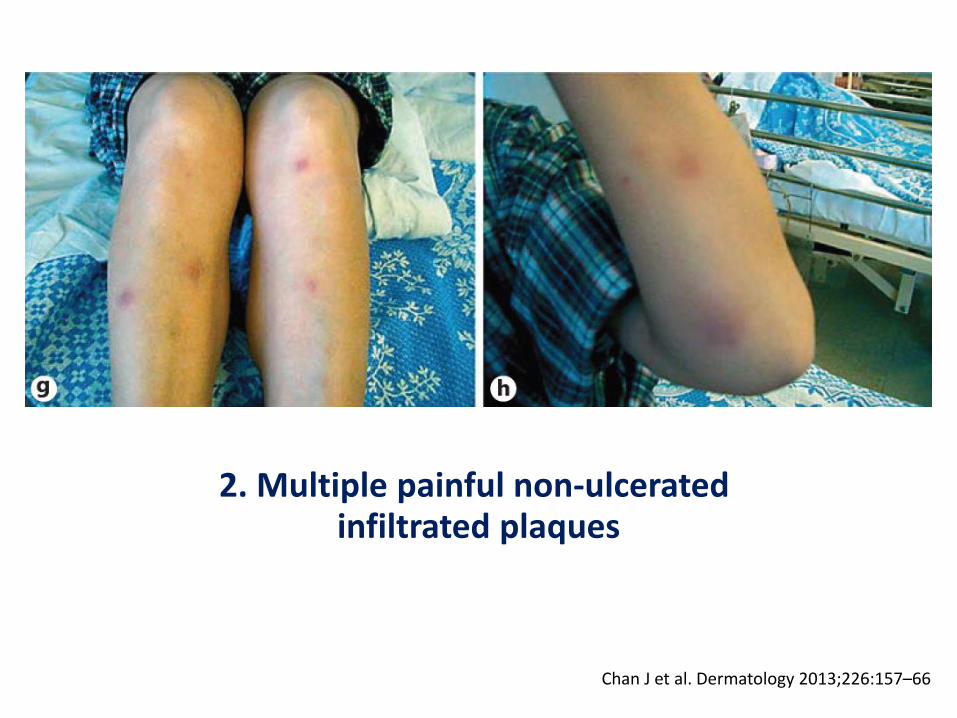
2. Multiple painful non-ulcerated infiltrated plaques
Chan J et al. Dermatology 2013;226:157–66
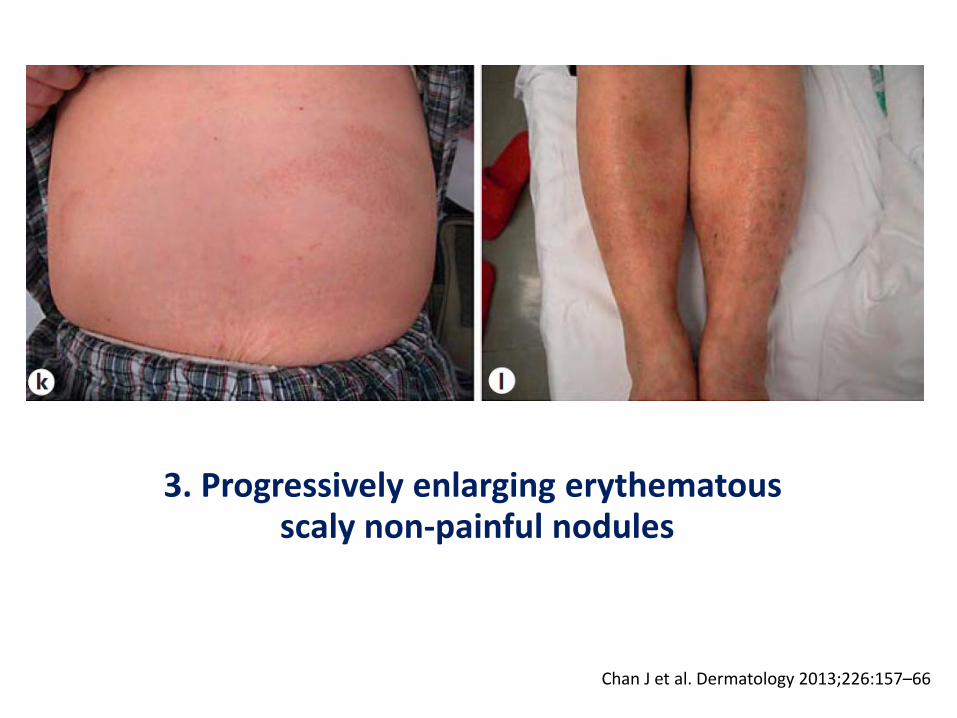
3. Progressively enlarging erythematous scaly non-painful nodules

Chan J et al. Dermatology 2013;226:157–66
1. Suppurative inflammation sparing the epidermis -> Sweet’s syndrome
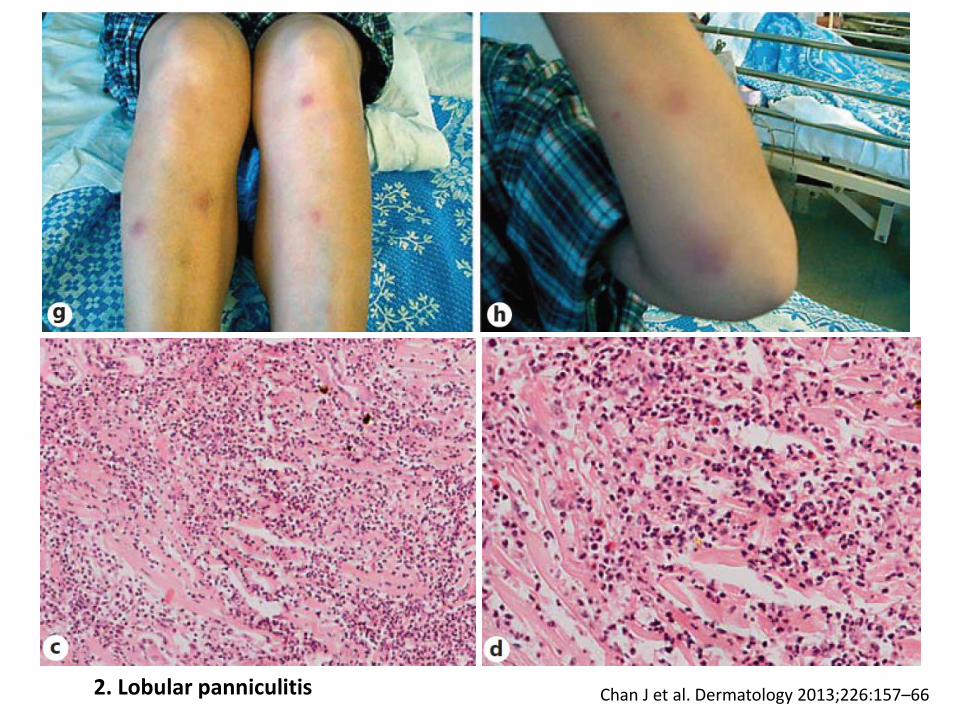
Chan J et al. Dermatology 2013;226:157–66 2. Lobular panniculitis
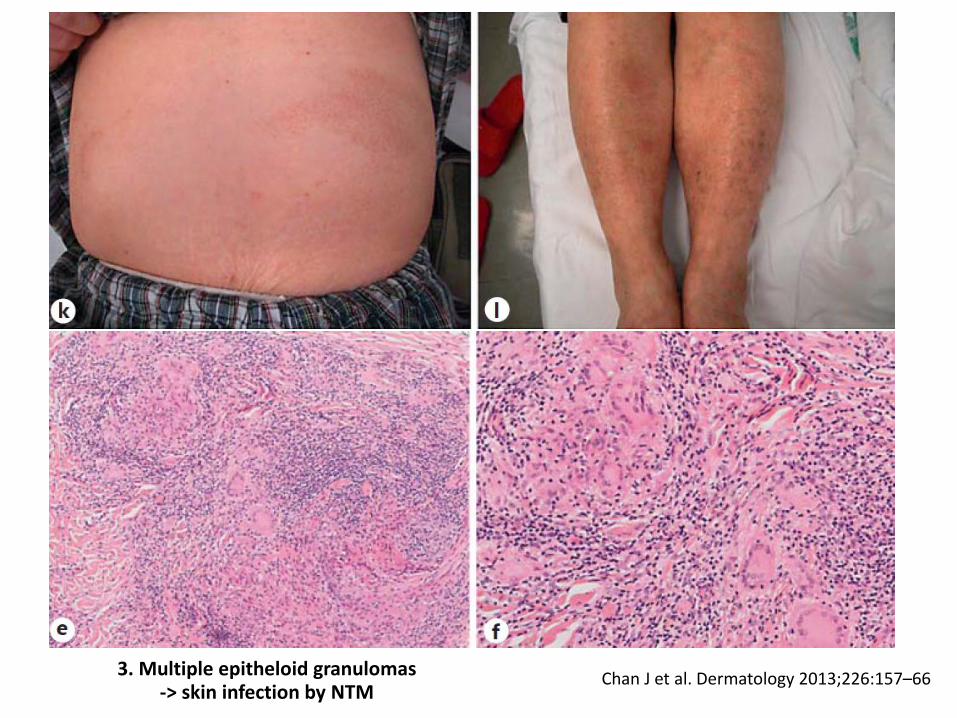
Chan J et al. Dermatology 2013;226:157–66 3. Multiple epitheloid granulomas -> skin infection by NTM
Different forms of dermatoses
Broadly classified into
• Reactive dermatoses
- Sweet’s syndrome
- Erythema nodosum
- Lobular panniculitis
- Generalized pustular eruptions (AGEP,
pustular psoriasis and subcorneal pustulosis)
• Direct invasion of the skin in disseminated infection
Chan J et al. Dermatology 2013;226:157–66
-> most common
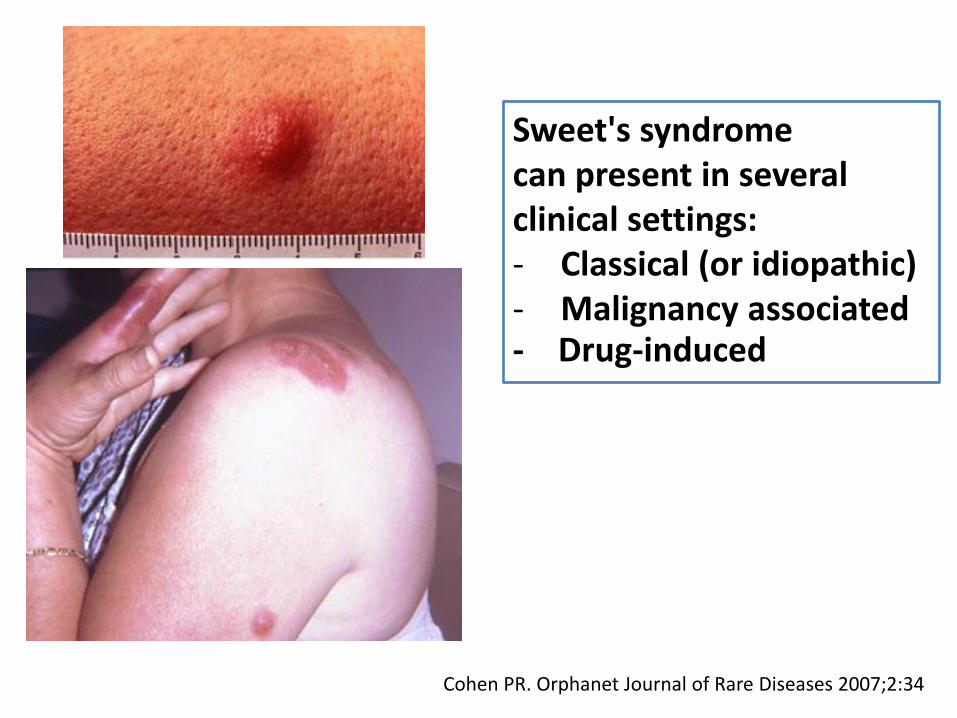
Cohen PR. Orphanet Journal of Rare Diseases 2007;2:34
Sweet's syndrome can present in several clinical settings: - Classical (or idiopathic) - Malignancy associated - Drug-induced
Cohen PR. Orphanet Journal of Rare Diseases 2007;2:34
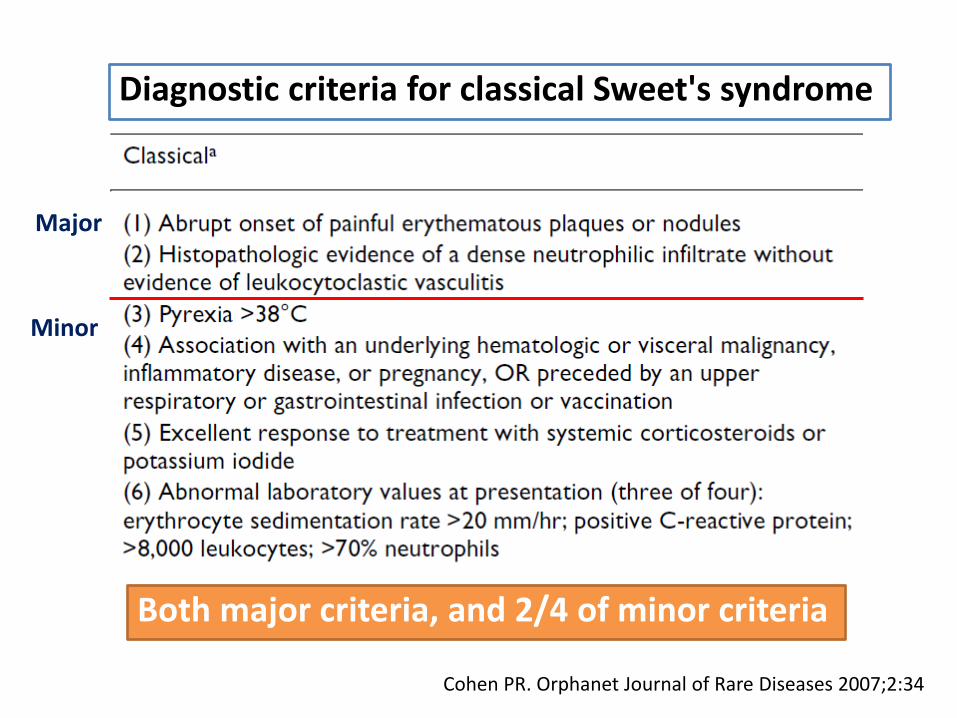
Diagnostic criteria for classical Sweet's syndrome
Major
Minor
Both major criteria, and 2/4 of minor criteria
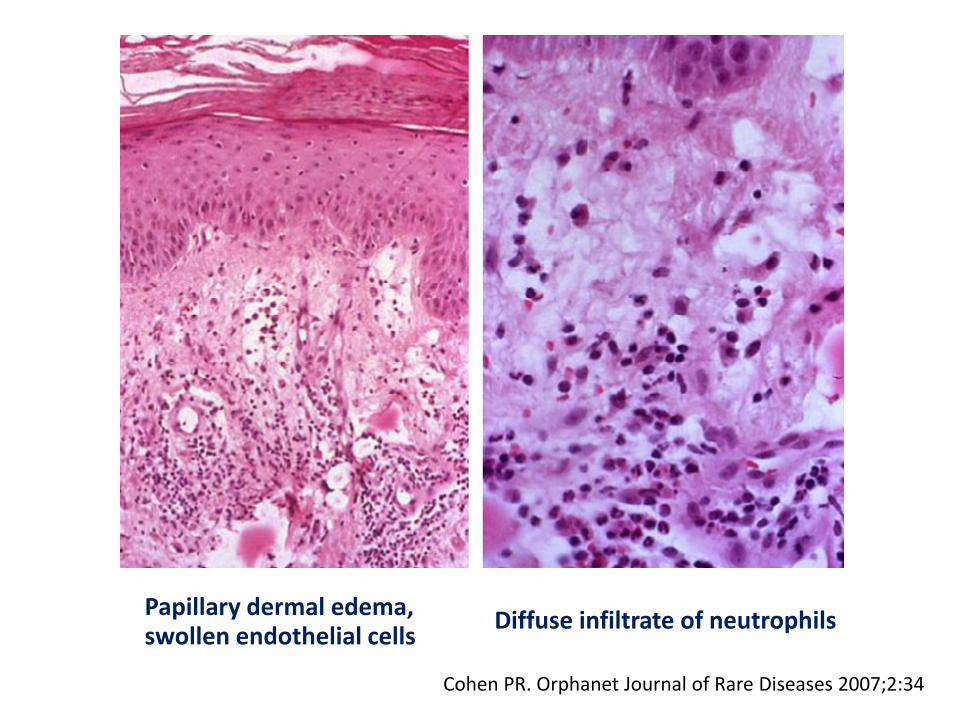
Cohen PR. Orphanet Journal of Rare Diseases 2007;2:34
Papillary dermal edema, swollen endothelial cells
Diffuse infiltrate of neutrophils
Chan J et al. Dermatology 2013;226:157–66

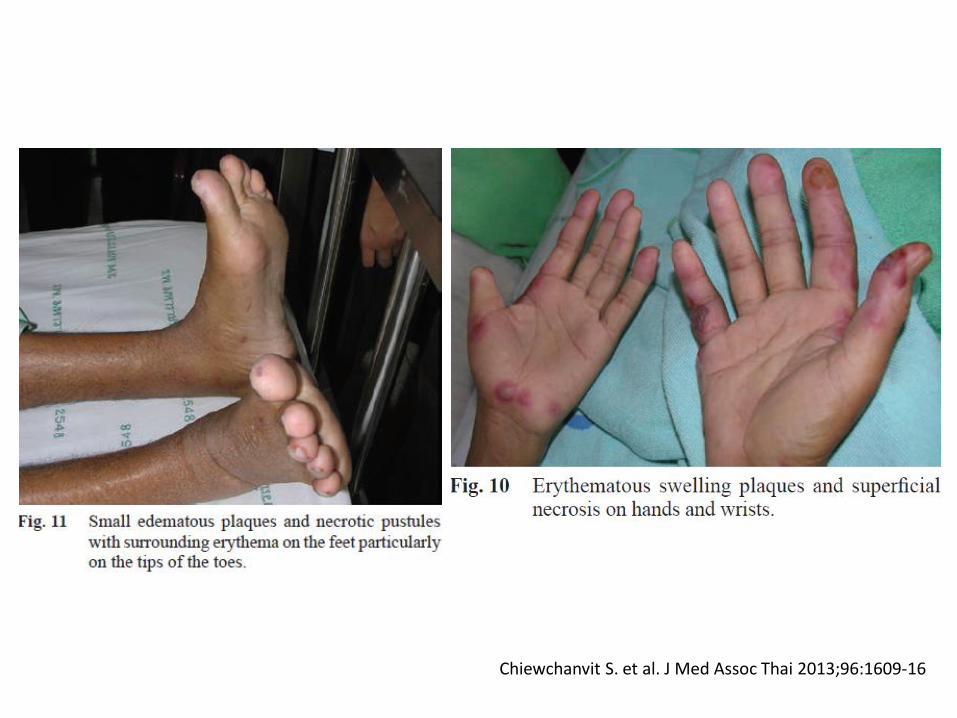
Chiewchanvit S. et al. J Med Assoc Thai 2013;96:1609-16
Acitretin, a second-generation retinoid, have been reported in the treatment of pustular diseases
including pustular psoriasis, subcorneal pustular dermatosis, eosinophilic pustular
folliculitis, and AGEP
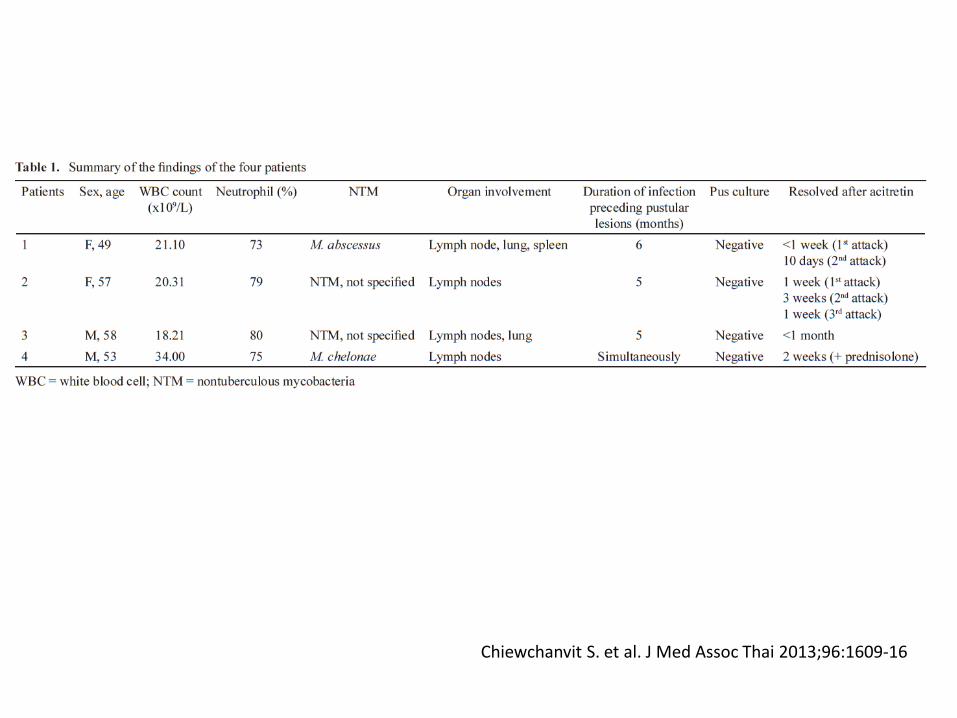
Chiewchanvit S. et al. J Med Assoc Thai 2013;96:1609-16

Chiewchanvit S. et al. J Med Assoc Thai 2013;96:1609-16
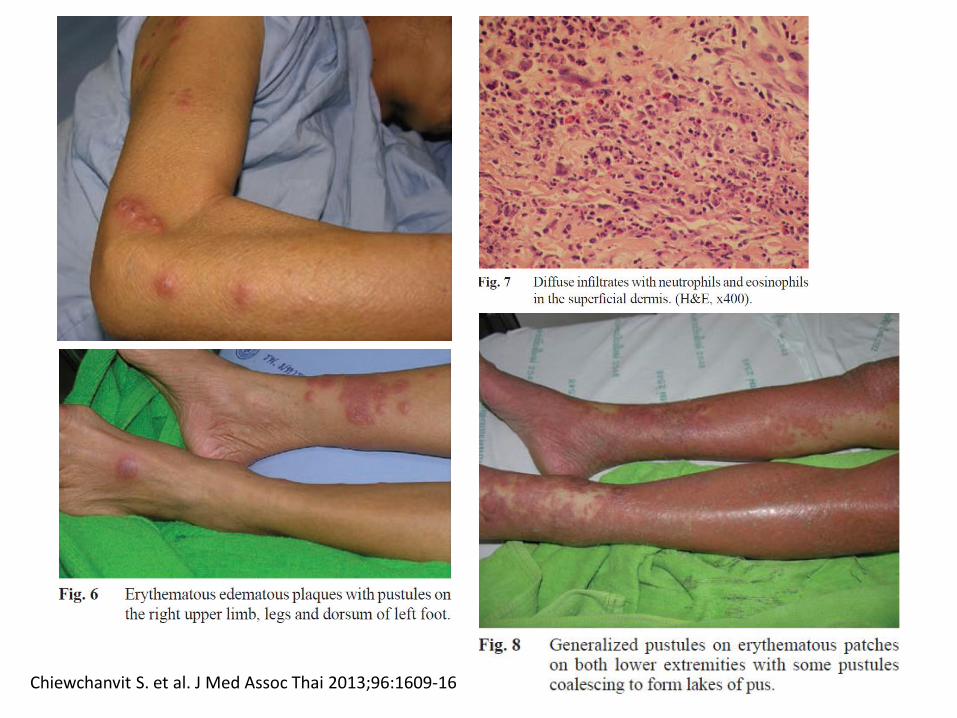
Chiewchanvit S. et al. J Med Assoc Thai 2013;96:1609-16
Chiewchanvit S. et al. J Med Assoc Thai 2013;96:1609-16

Chiewchanvit S. et al. J Med Assoc Thai 2013;96:1609-16

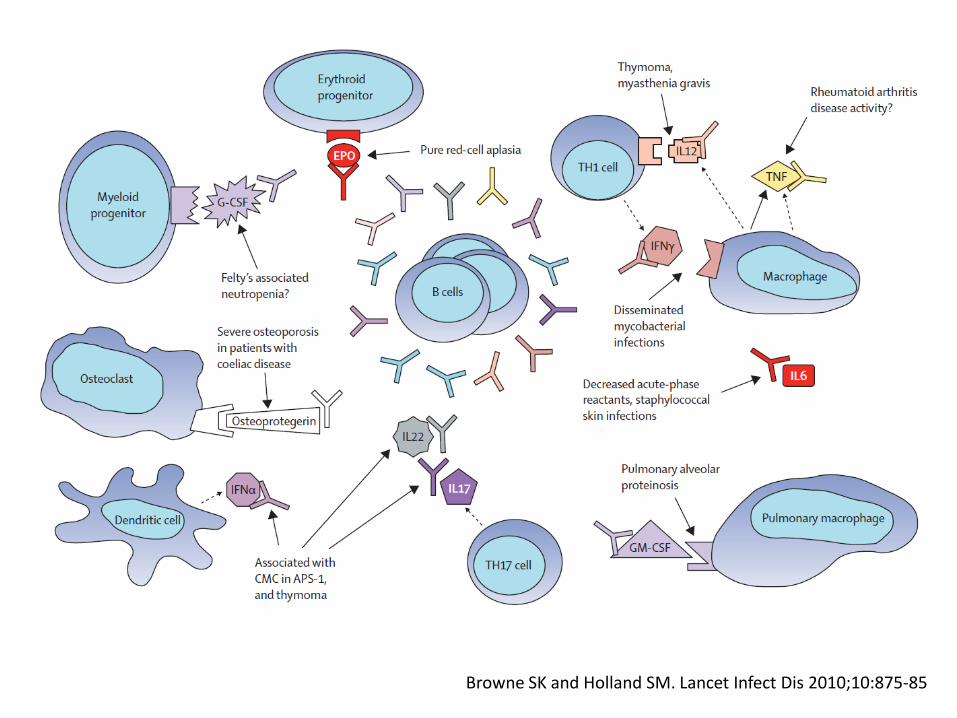
Autoantibodies to cytokines
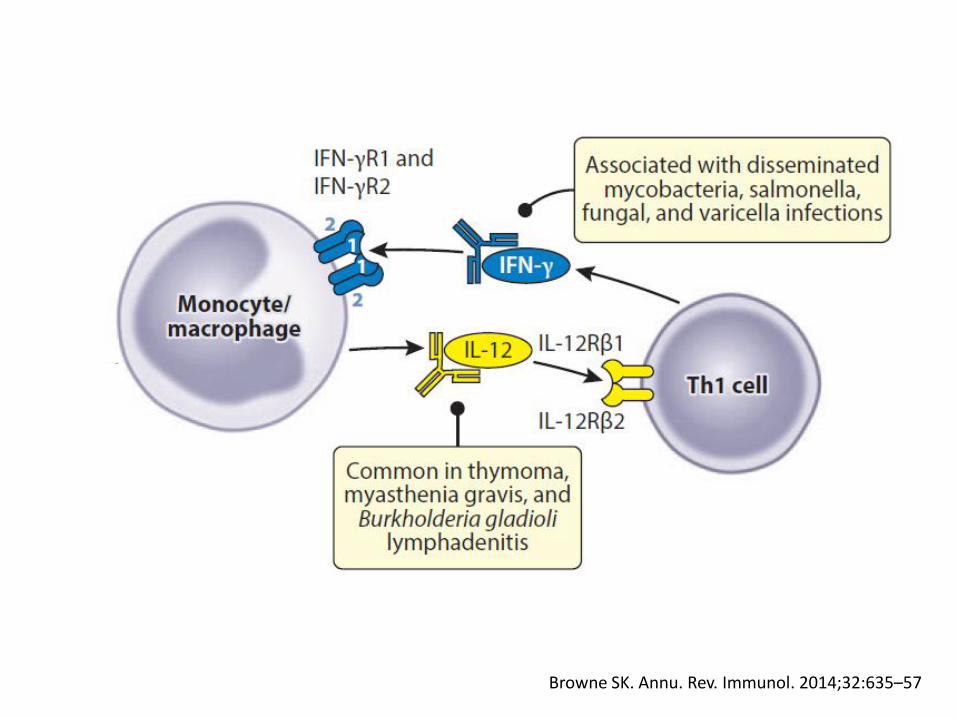
Browne SK. Annu. Rev. Immunol. 2014;32:635–57
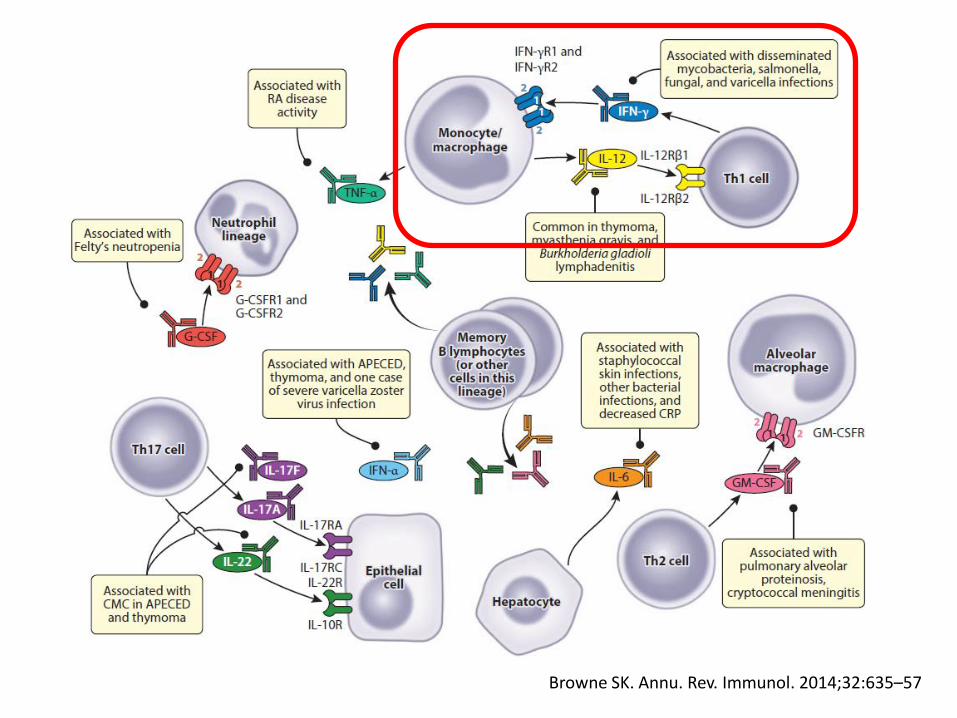
Browne SK. Annu. Rev. Immunol. 2014;32:635–57
Autoantibodies to cytokines
• Occur in many different conditions
• May also develop against exogenously cytokines
• Have been identified in health and disease, with their relationship ranging from none to directly causal
Browne SK and Holland SM. Lancet Infect Dis 2010;10:875-85
Browne SK and Holland SM. Lancet Infect Dis 2010;10:875-85
Mendelian susceptibility to mycobacterial infection (MSMD)

Mendelian susceptibility to mycobacterial infection
• Selective susceptibility to weakly pathogenic mycobacteria, such as BCG vaccine and environmental NTM causing idiopathic, disseminated infection, has long been suspected to be a Mendelian disorder
Casanova JL. Swiss Med Wkly 2001;131:445-54
Muhsen SA and Casanova JL. J Allergy Clin Immunol 2008;122:1043-51
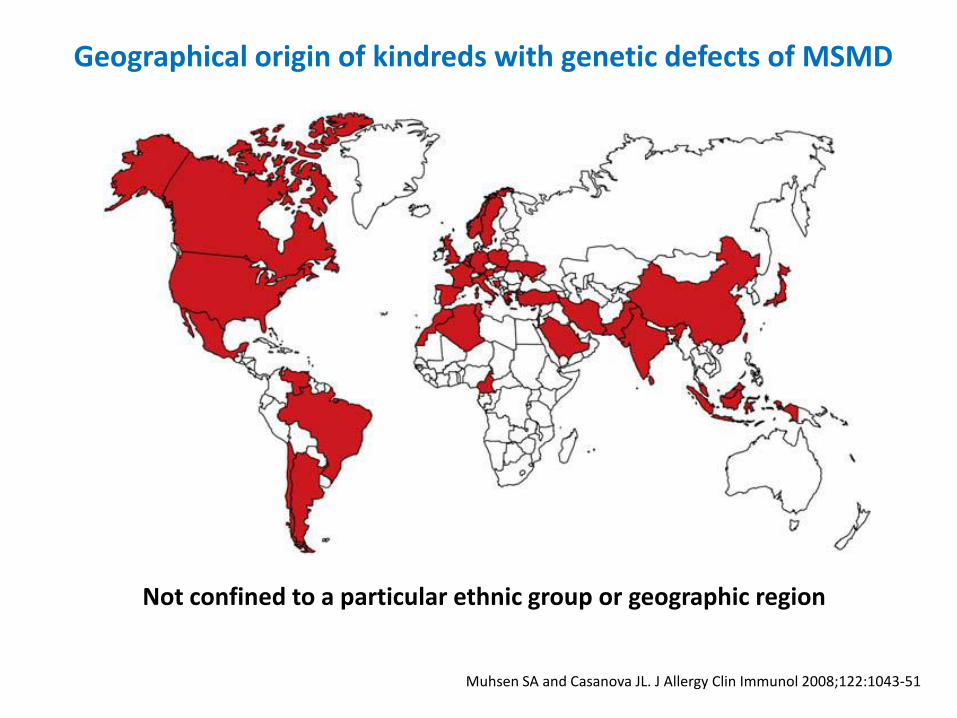
Geographical origin of kindreds with genetic defects of MSMD
Not confined to a particular ethnic group or geographic region
Vosse E. and Ottenhoff T. Microbes and Infection 2006;8:1167-73
Access January 8, 2015
Casanova JL. Swiss Med Wkly 2001;131:445-54 Muhsen SA and Casanova JL. J Allergy Clin Immunol 2008;122:1043-51
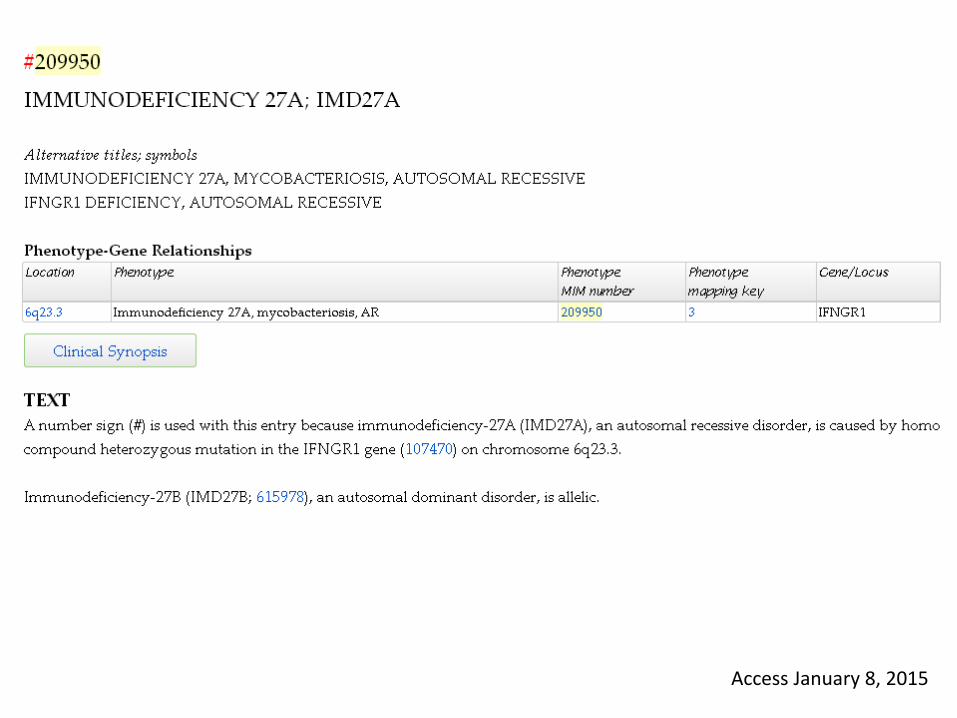
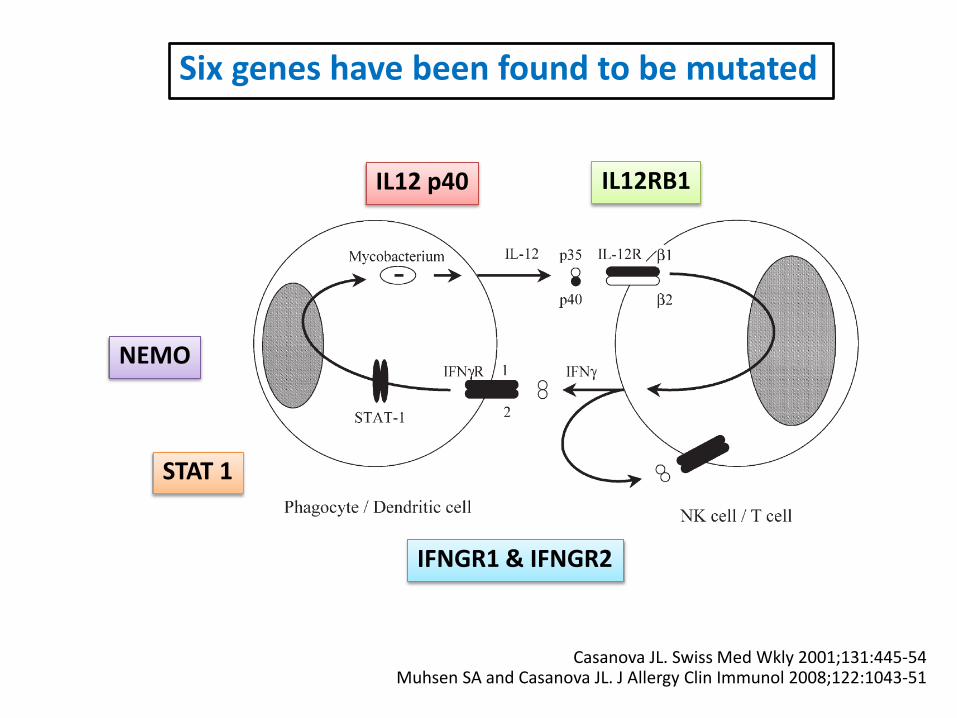
Six genes have been found to be mutated
IFNGR1 & IFNGR2
STAT 1
IL12 p40 IL12RB1
NEMO

Muhsen SA and Casanova JL. J Allergy Clin Immunol 2008;122:1043-51

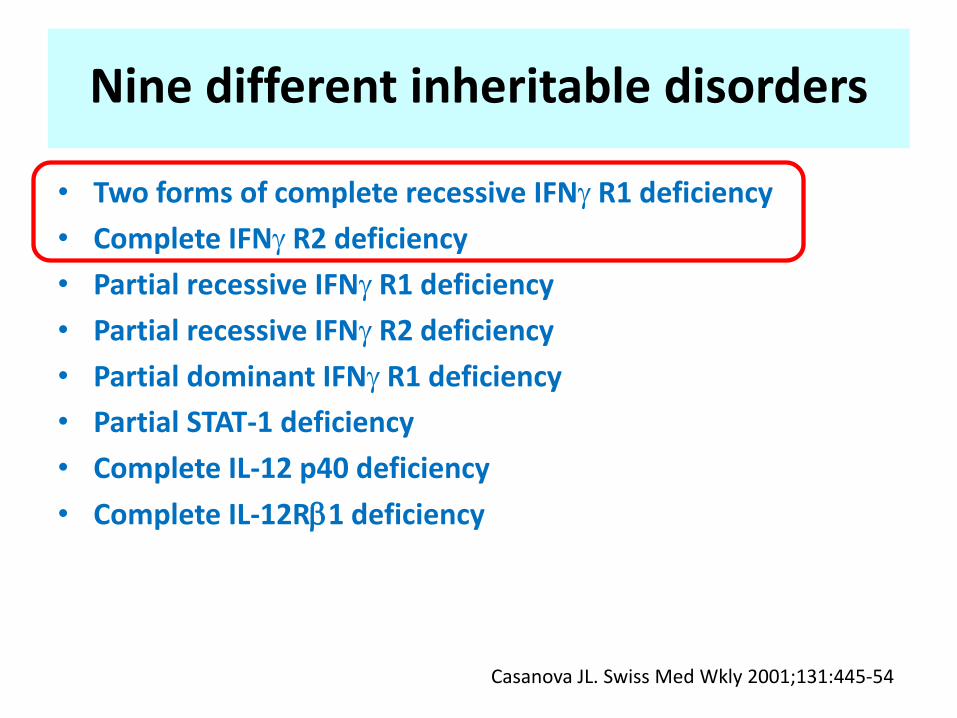
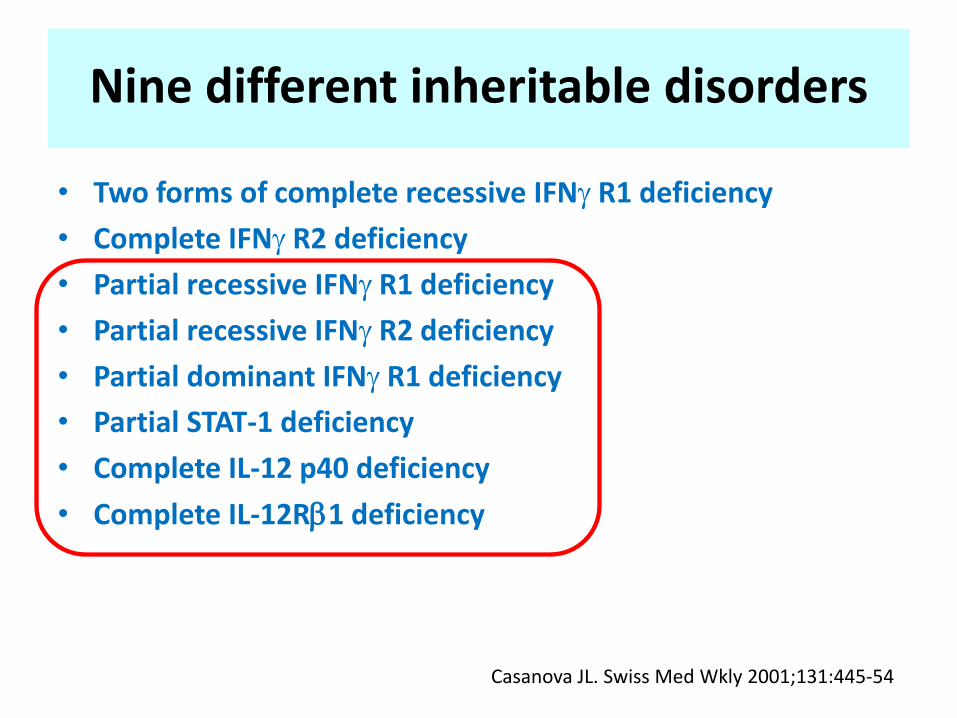
Nine different inheritable disorders
• Two forms of complete recessive IFN R1 deficiency
• Complete IFN R2 deficiency
• Partial recessive IFN R1 deficiency
• Partial recessive IFN R2 deficiency
• Partial dominant IFN R1 deficiency
• Partial STAT-1 deficiency
• Complete IL-12 p40 deficiency
• Complete IL-12R1 deficiency
Casanova JL. Swiss Med Wkly 2001;131:445-54
Nine different inheritable disorders
• Two forms of complete recessive IFN R1 deficiency
• Complete IFN R2 deficiency
• Partial recessive IFN R1 deficiency
• Partial recessive IFN R2 deficiency
• Partial dominant IFN R1 deficiency
• Partial STAT-1 deficiency
• Complete IL-12 p40 deficiency
• Complete IL-12R1 deficiency
Casanova JL. Swiss Med Wkly 2001;131:445-54
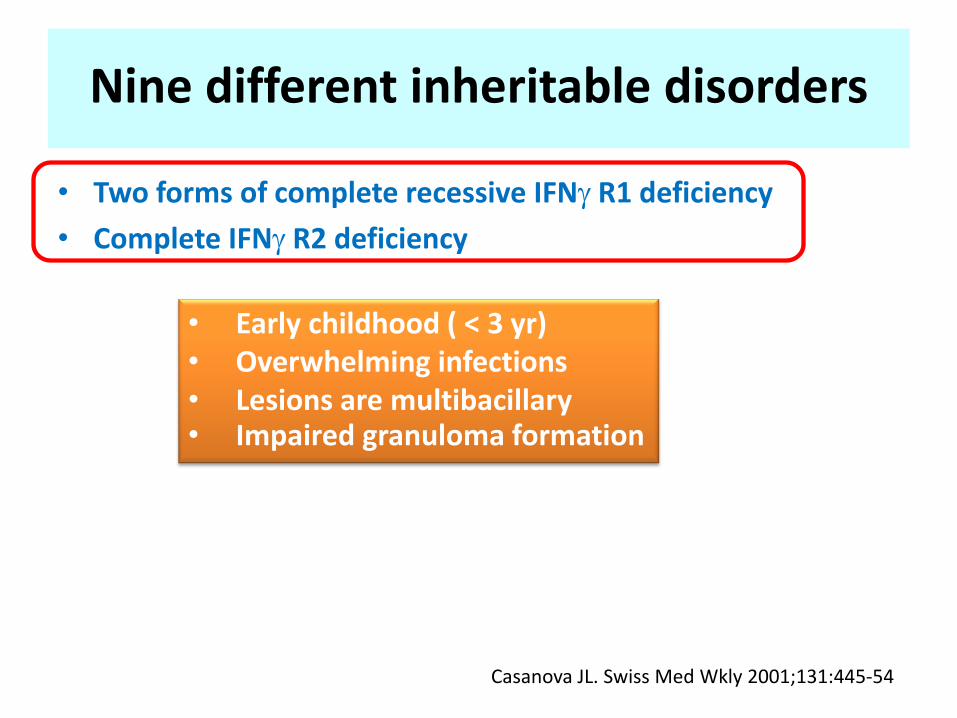
Nine different inheritable disorders
• Two forms of complete recessive IFN R1 deficiency
• Complete IFN R2 deficiency
Casanova JL. Swiss Med Wkly 2001;131:445-54
• Early childhood ( < 3 yr) • Overwhelming infections • Lesions are multibacillary • Impaired granuloma formation
Nine different inheritable disorders
• Two forms of complete recessive IFN R1 deficiency
• Complete IFN R2 deficiency
• Partial recessive IFN R1 deficiency
• Partial recessive IFN R2 deficiency
• Partial dominant IFN R1 deficiency
• Partial STAT-1 deficiency
• Complete IL-12 p40 deficiency
• Complete IL-12R1 deficiency
Casanova JL. Swiss Med Wkly 2001;131:445-54
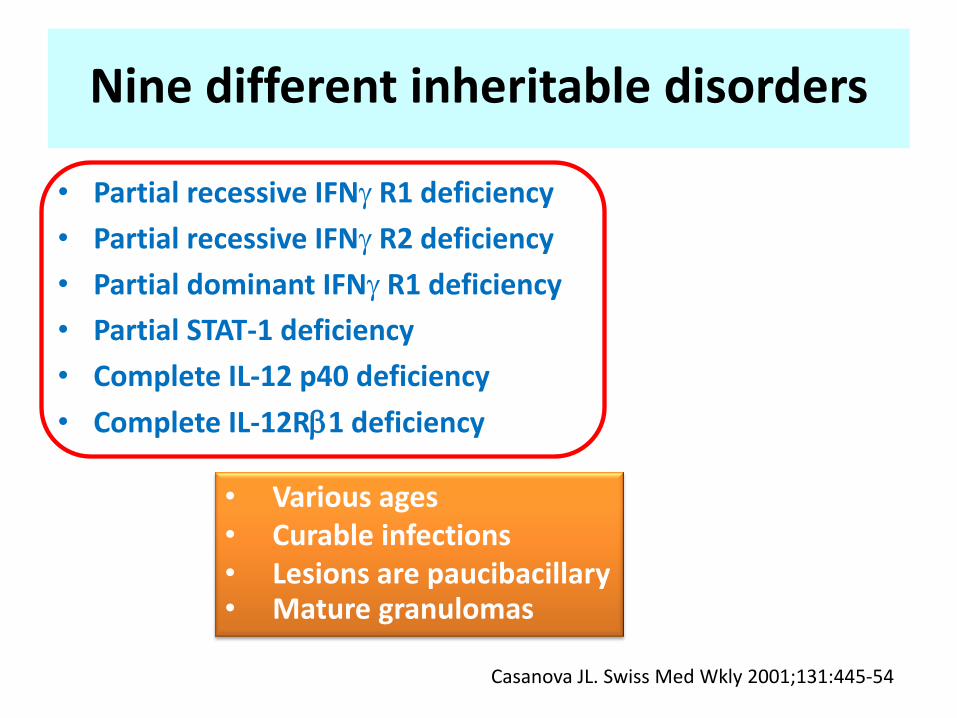
Nine different inheritable disorders
• Partial recessive IFN R1 deficiency
• Partial recessive IFN R2 deficiency
• Partial dominant IFN R1 deficiency
• Partial STAT-1 deficiency
• Complete IL-12 p40 deficiency
• Complete IL-12R1 deficiency
Casanova JL. Swiss Med Wkly 2001;131:445-54
• Various ages • Curable infections • Lesions are paucibacillary • Mature granulomas
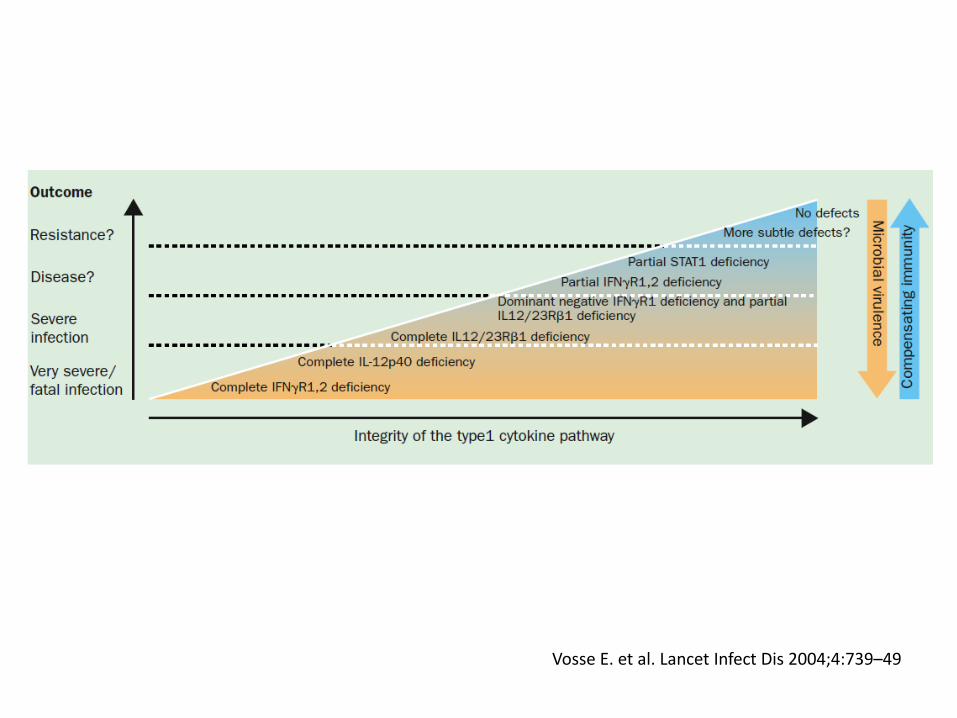
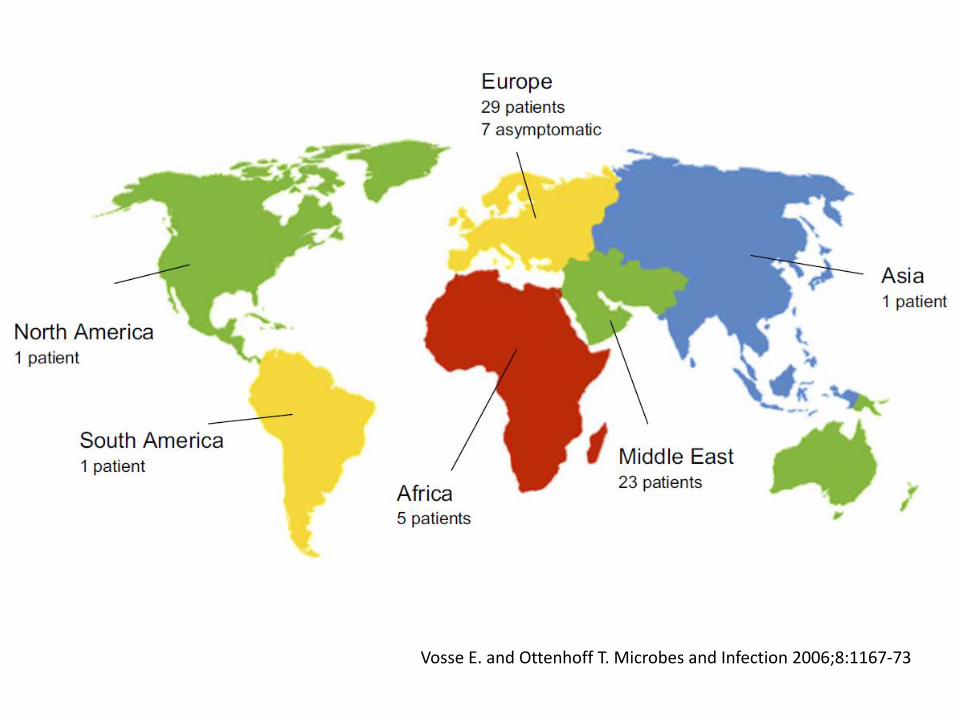
Vosse E. et al. Lancet Infect Dis 2004;4:739–49
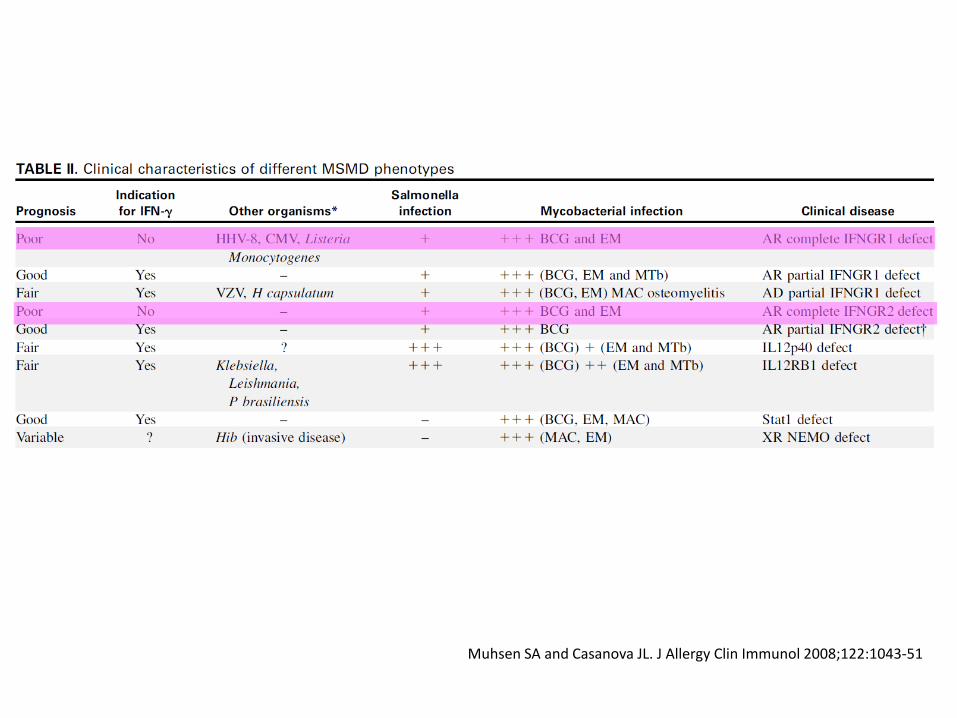
Muhsen SA and Casanova JL. J Allergy Clin Immunol 2008;122:1043-51
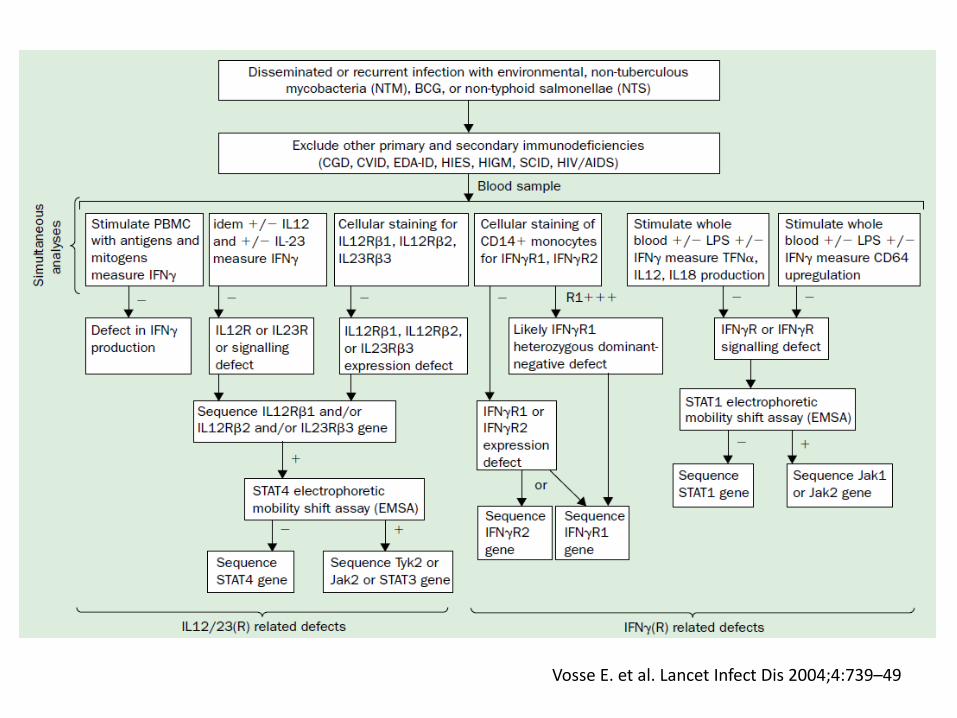
Vosse E. et al. Lancet Infect Dis 2004;4:739–49
Till…2013 25 reported cases from PubMed search
• Majority of cases were Asian (8 Chinese, 6 Filipino, 4 Thai, 4 Taiwanese, 2 Japanese, and 1 Vietnamese)
• Organs involved were the lymph nodes (22), lungs (19), bones (12), soft tissue (9), bone marrow (7), and skin (7)
Lee WI. et al. Immunobiology 2013;218:762–71
Till…2013 • Tissue cultures and pathology findings
rather than blood cultures provided evidence of NTM
• Both slow- and rapidly growing NTM were causative pathogens, with Mycobacterium avium complex (14) and M. chelonae (7)
• 6 patients were infected with multiple species of mycobacteria, including both NTM and M. tuberculosis
Lee WI. et al. Immunobiology 2013;218:762–71
Till…2013 • Co-infections with P. marneffei and
Salmonella spp. simultaneously developed in 11 and 7 patients
• Experience both dermatomal and disseminated varicella zoster reactivation at higher frequency
Lee WI. et al. Immunobiology 2013;218:762–71 Browne SK. et al. Annu Rev Immunol 2014;32:635–57
Till…2013 • Laboratory features often indicative of
chronic inflammation or infection, including anemia, leukocytosis, elevated ESR, CRP, and/or β2-microglobulin and polyclonal hypergammaglobulinemia
Browne SK. et al. Annu Rev Immunol 2014;32:635–57
Till…2013 • grossly normal immunologic
parameters, including CD4+ T lymphocytes, monocyte numbers, and IFNγR1 expression
Browne SK. et al. Annu Rev Immunol 2014;32:635–57
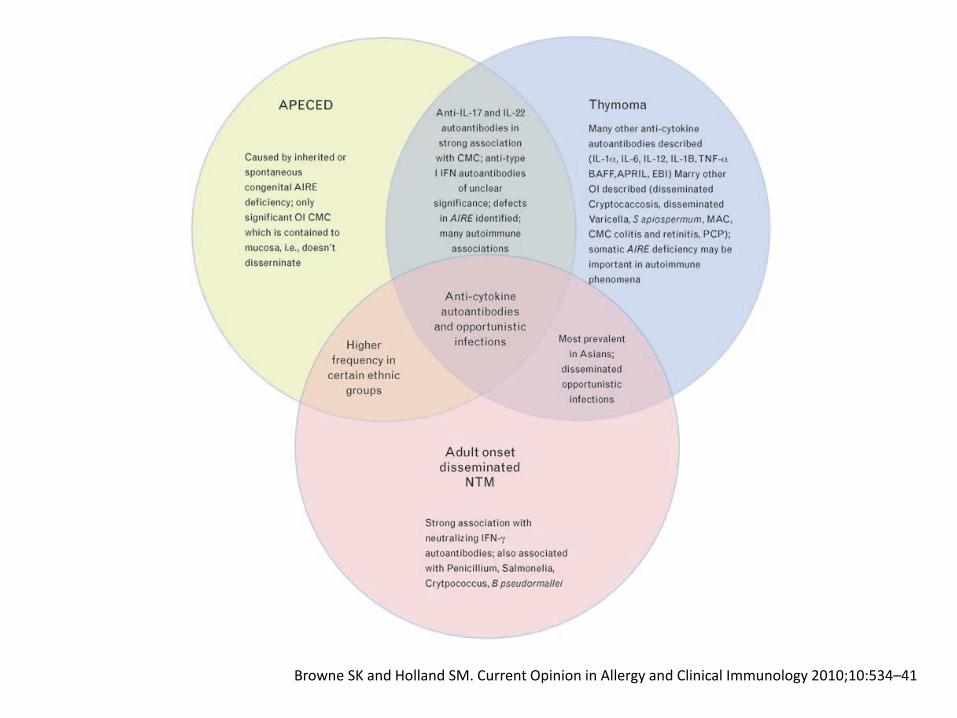
Browne SK and Holland SM. Current Opinion in Allergy and Clinical Immunology 2010;10:534–41
Prognosis • 32% mortality by a median of
25 months after diagnosis
Wongkulab P. et al. PloS One 2013;8:e76371

Treatment
Treatment
• Treating the disease consequences
• Targeting the autoantibody
Browne SK and Holland SM. Lancet Infect Dis 2010;10:875-85
Treatments • Majority fail to show a sustained
response to IFN- treatment
• IVIG for neutralizing and plasmapheresis to remove antibody, are not consistently effective
Lee WI. et al. Immunobiology 2013;218:762–71

Browne SK et al. Blood 2012;119:3933-9
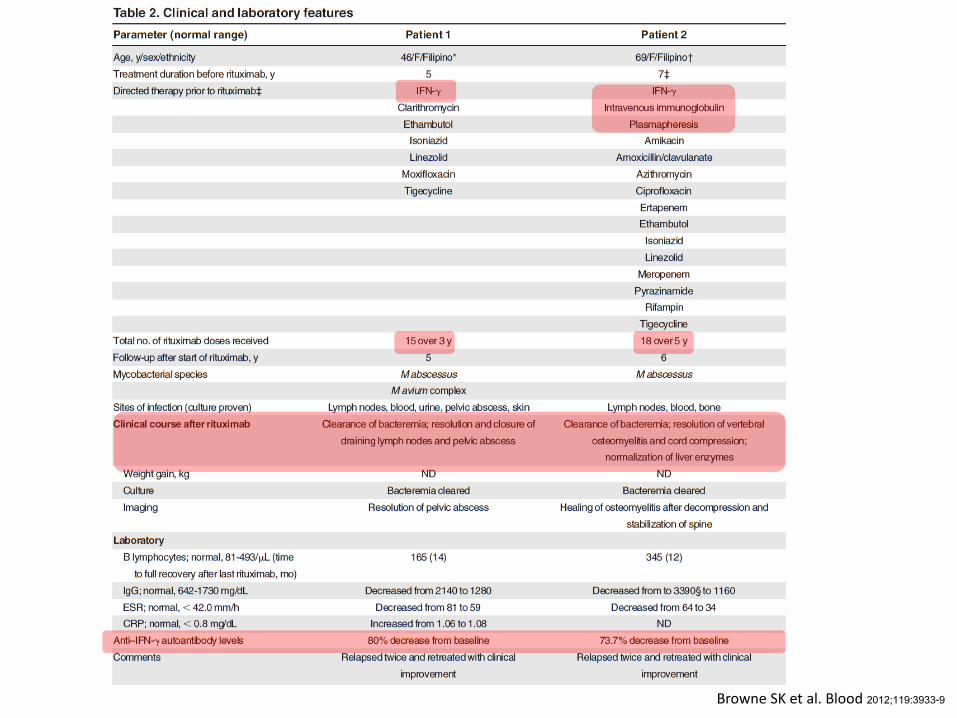
Rituximab was used in 4 patients with high-titer anti–IFN- autoantibodies who had progressive refractory NTM disease despite aggressive anti-infective treatment • Treat according to a lymphoma regimen, additional doses were given for persistence or relapse • Aim of depleting B cells • Other possible mechanisms; modulation cell surface receptors, modulation B-cell, elimination plasmablasts
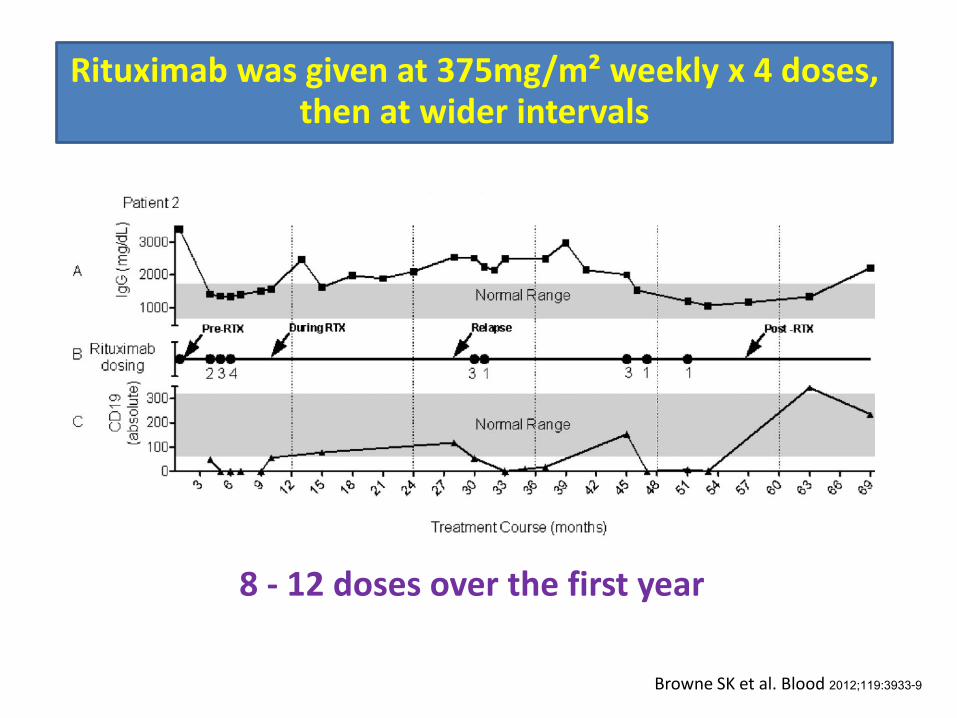
Browne SK et al. Blood 2012;119:3933-9
Rituximab was given at 375mg/m² weekly x 4 doses, then at wider intervals
8 - 12 doses over the first year
Browne SK et al. Blood 2012;119:3933-9
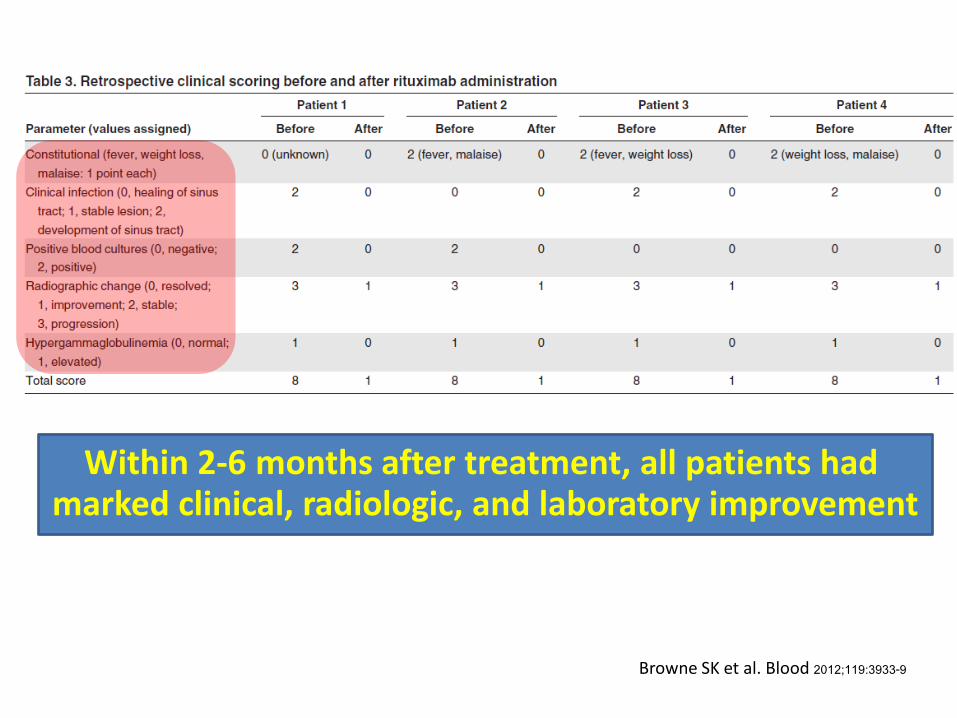
Browne SK et al. Blood 2012;119:3933-9
Within 2-6 months after treatment, all patients had marked clinical, radiologic, and laboratory improvement
Conclusion • Not all cases of anti–IFN- autoantibody-
mediated disseminated mycobacterial disease require rituximab
• Recommend for those with persistent, progressive, severe anti–IFN- autoantibody–associated infection
Browne SK et al. Blood 2012;119:3933-9
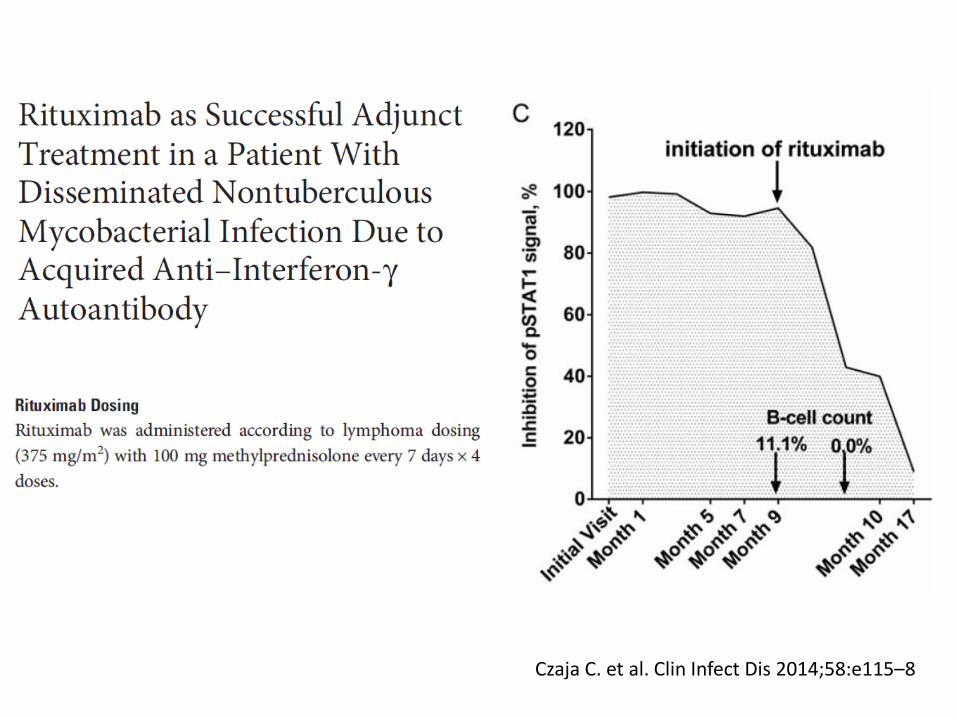
Czaja C. et al. Clin Infect Dis 2014;58:e115–8
Future well controlled studies are needed to
evaluate the safety and efficacy of this approach
Take home messages (1) Suggest including anti-IFN- autoantibodies
in the differential diagnosis of
• HIV-negative patients
• Severe, persistent or recurrent infections caused by NTM and other opportunistic infections
• Reactive skin dermatoses
• Especially in Asian patients
Take home messages (2) • Trigger for these autoantibodies
remains unknown
• Patients with genetic defects tend to present early in life, and often show familial clustering

Thank you for your attention