anemias. body contents of iron structure of hemoglobin
TRANSCRIPT
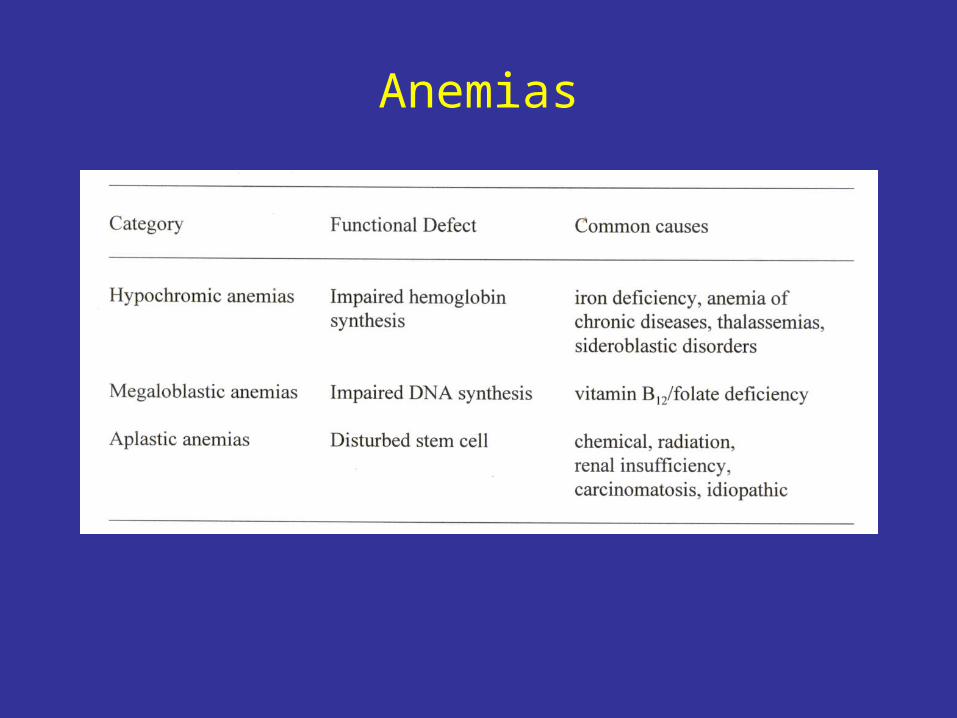
Anemias
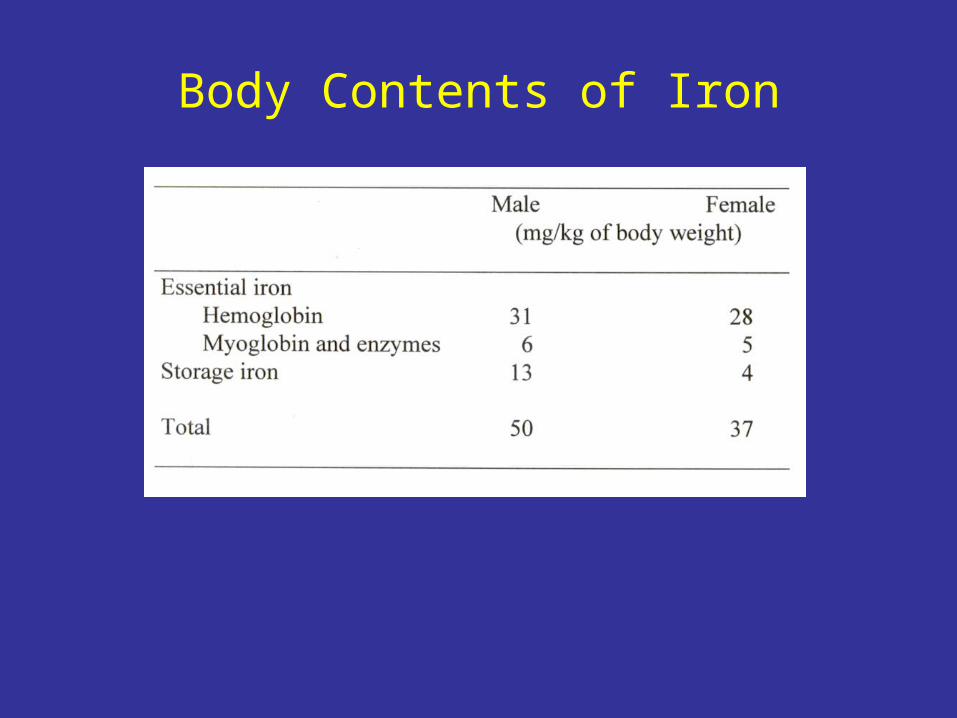
Body Contents of Iron
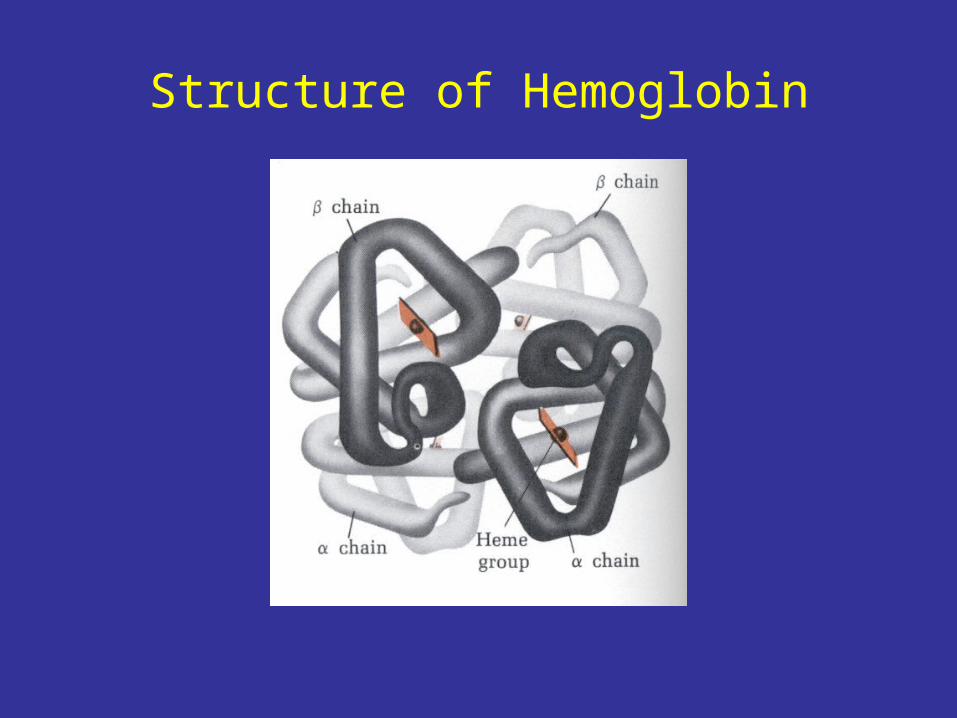
Structure of Hemoglobin
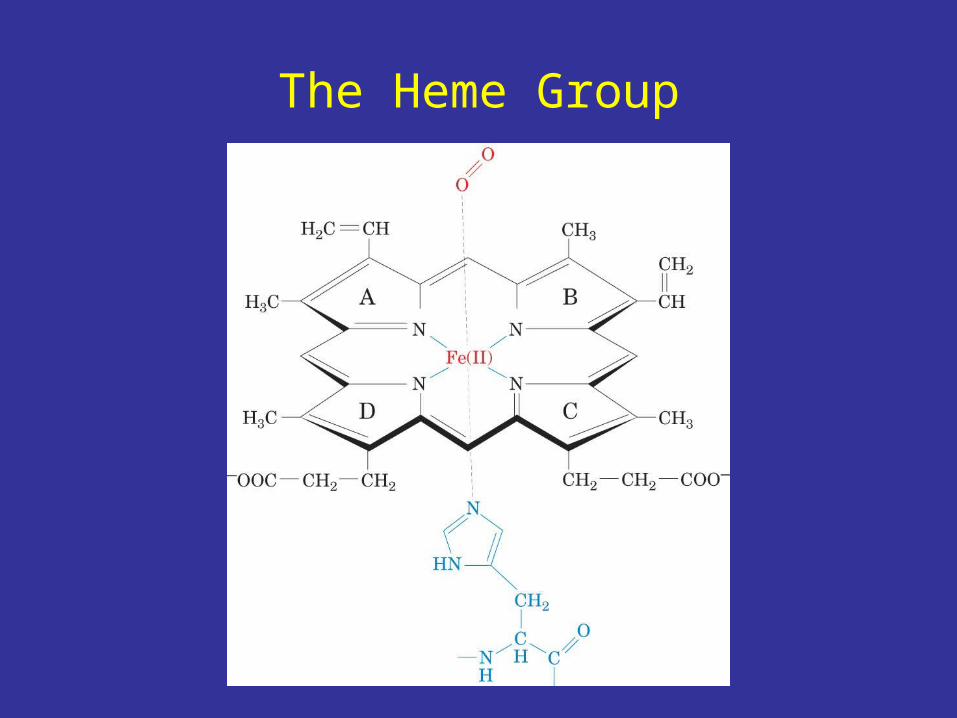
The Heme Group
Iron Absorption
• Ferritin – a large protein for iron storage• Hemosiderin – aggregated ferritin• Iron storage sites: hepatocytes
reticuloendothelial system
muscle (minor)
• Iron absorption – duodenum and jejunum
Ferrous (Fe2+) >>> Ferric (Fe3+)
• Transferrin – iron transport
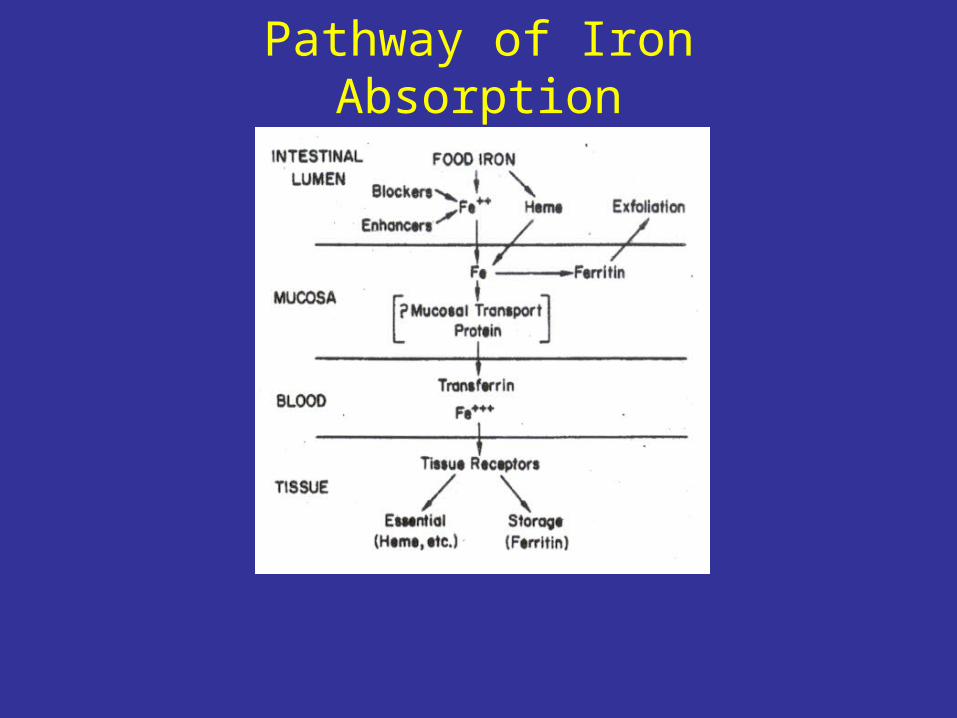
Pathway of Iron Absorption
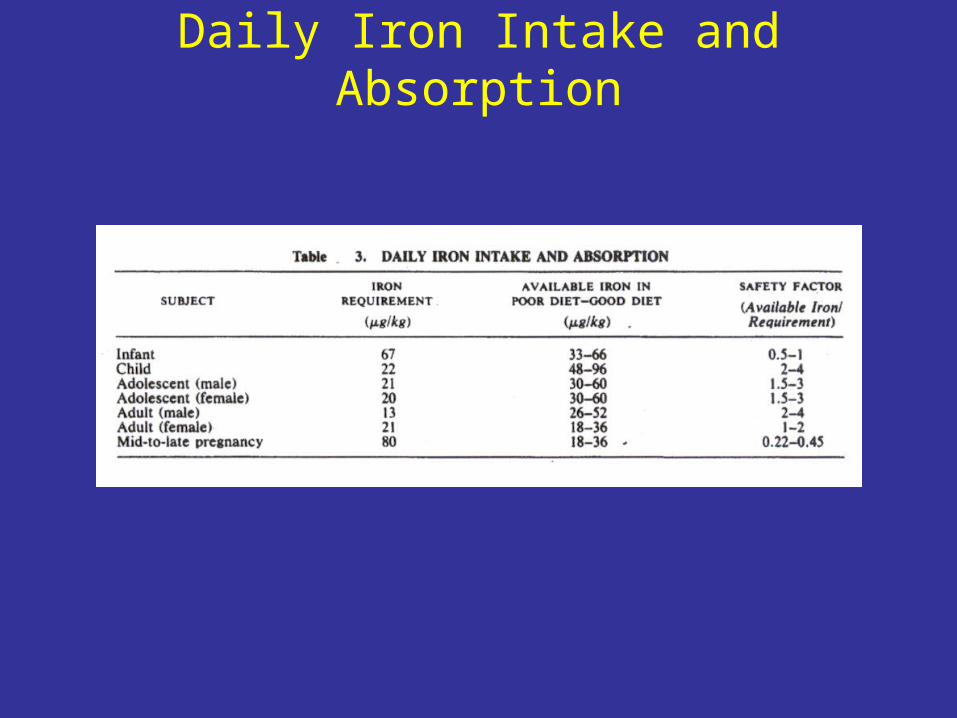
Daily Iron Intake and Absorption
Iron Deficiency
• Dietary intake of iron not adequate to meet normal requirements
• Conditions producing an increased requirements of iron because of iron loss
• Interference of iron absorption
Therapy for Iron Deficiency• Oral therapy
Drug of Choice – ferrous sulfate administered under fasting
Side effects – heart burn, nausea, upper gastric discomfort, constipation, diarrhea
antidote – deferoxamine• Parenteral therapy
Drug – iron dextran injection, im or iv
Side effects – im: long tern discomfort, local discoloration of skin, malignant changes
iv: serious anaphylactic reactions
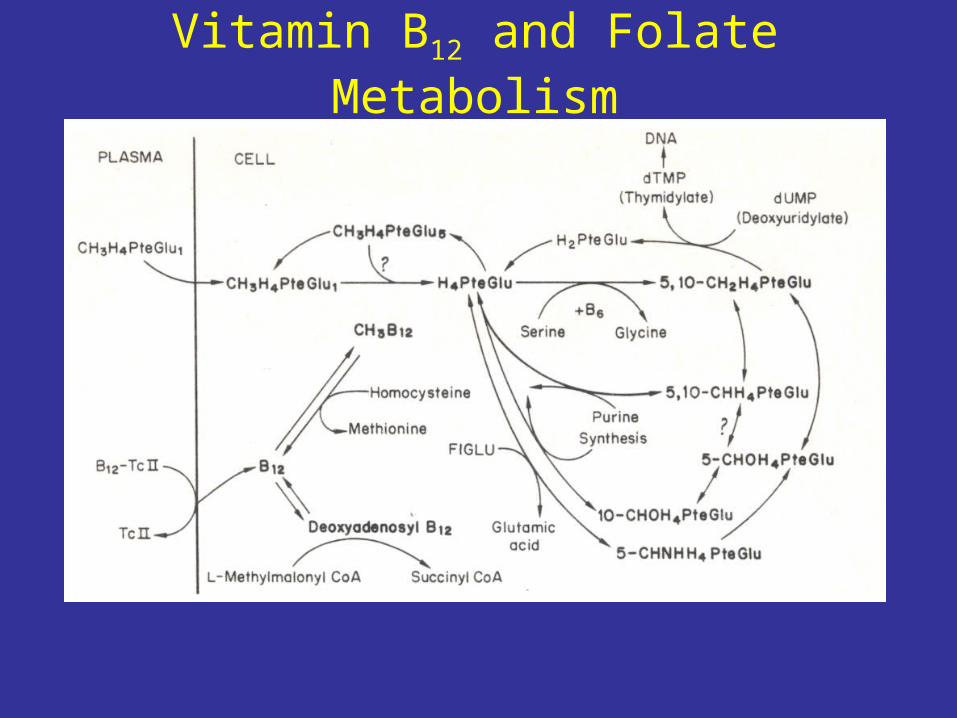
Vitamin B12 and Folate Metabolism
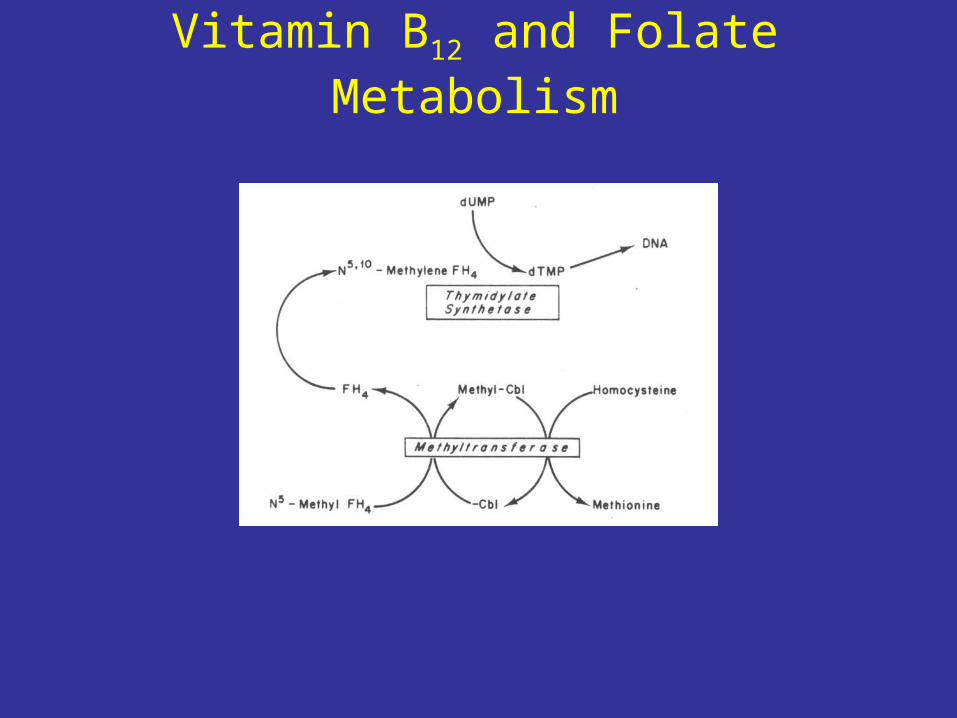
Vitamin B12 and Folate Metabolism

Hematological Responses ofVitamin B12 and Folate Therapy
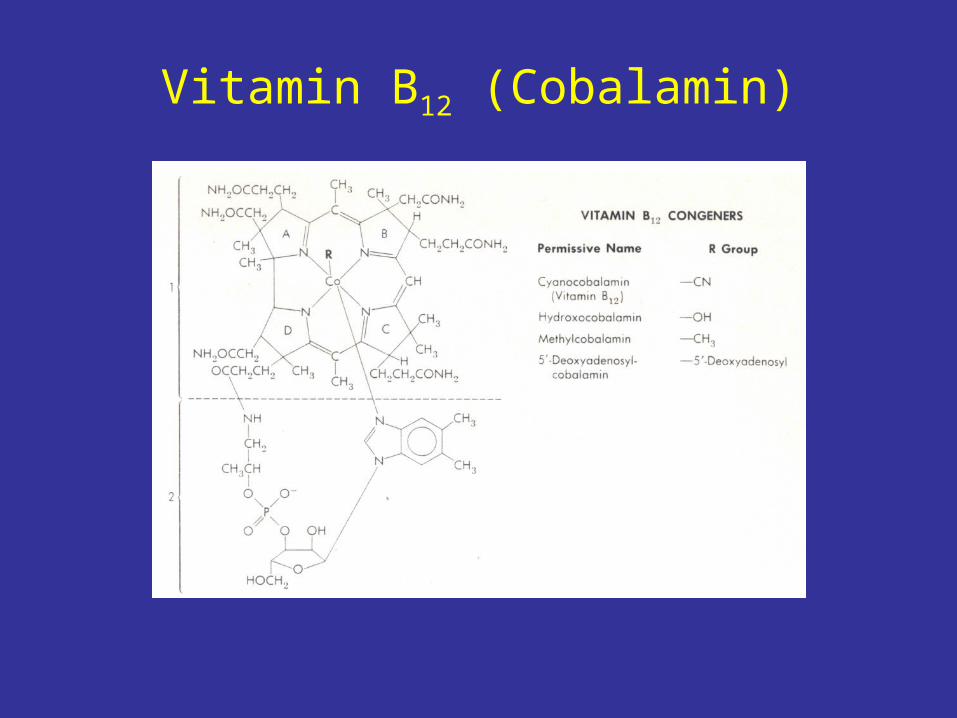
Vitamin B12 (Cobalamin)
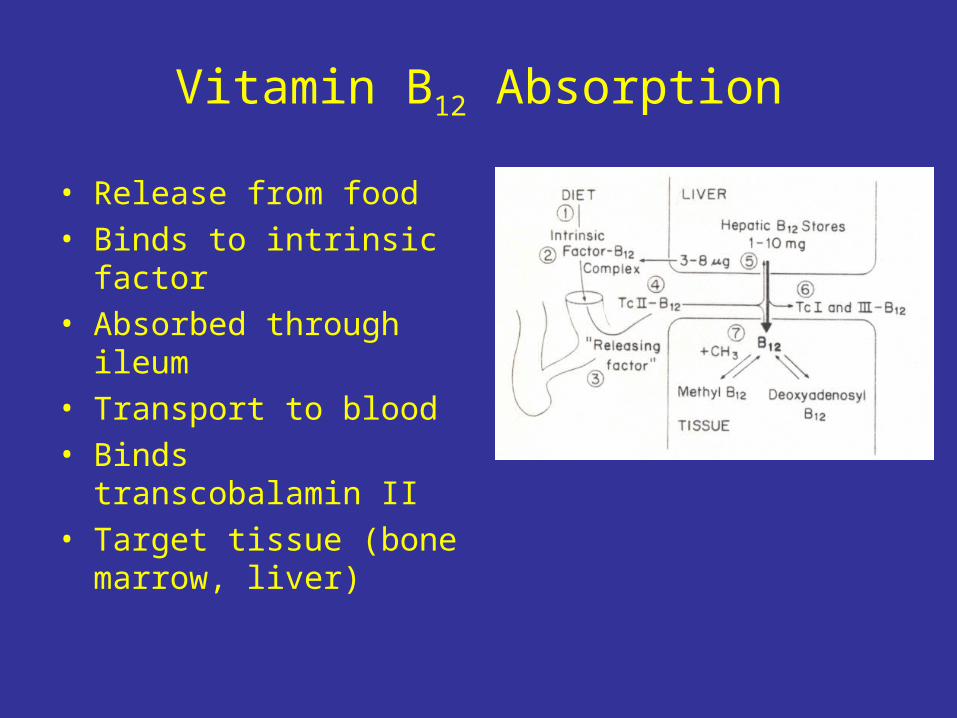
Vitamin B12 Absorption
• Release from food• Binds to intrinsic factor• Absorbed through ileum• Transport to blood• Binds transcobalamin II• Target tissue (bone
marrow, liver)
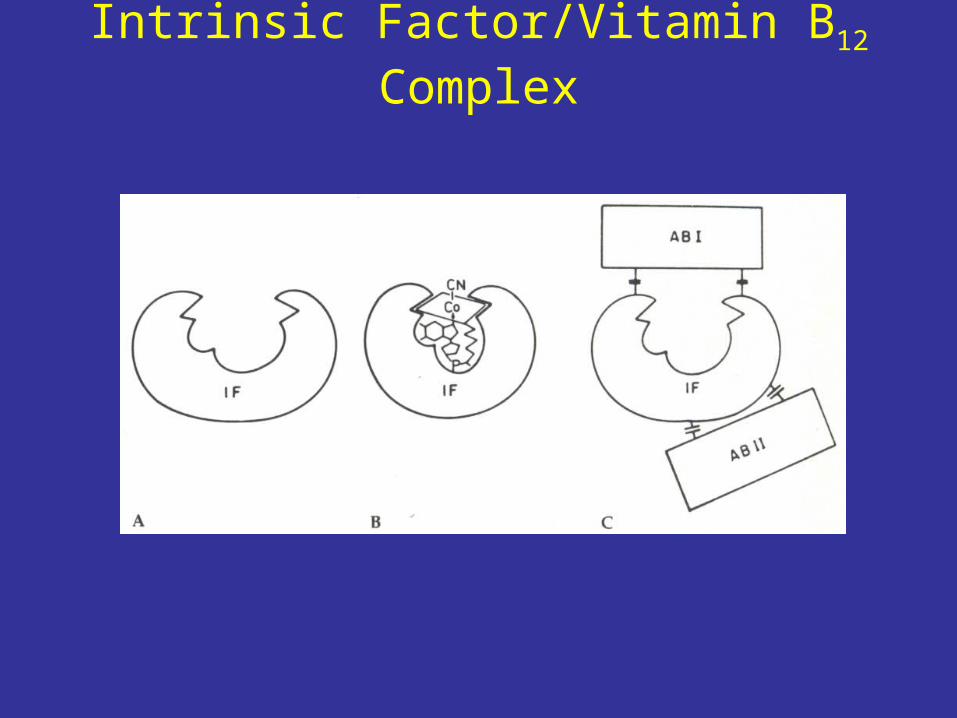
Intrinsic Factor/Vitamin B12 Complex
Vitamin B12 Deficiency
• Gastric achlorhydria and decreased intrinsic factor due to gastric atrophy and gastric surgery
• Panacreatic disorders
• Antibodies to intrinsic factor/vitamin B12 complex
• Bacterial overgrowth and intestinal parasites prevent vitamin B12 from reaching the ileum
• Damaged ileal mucosa• Congenital defects in transcobalamin II
Vitamin B12 Therapy
• Oral preparations
to supplement deficient diet
to prevent vitamin B12 deficiency
• Cyanocobalamin injection
given by intramuscular and subcutaneous routes, never intravenously
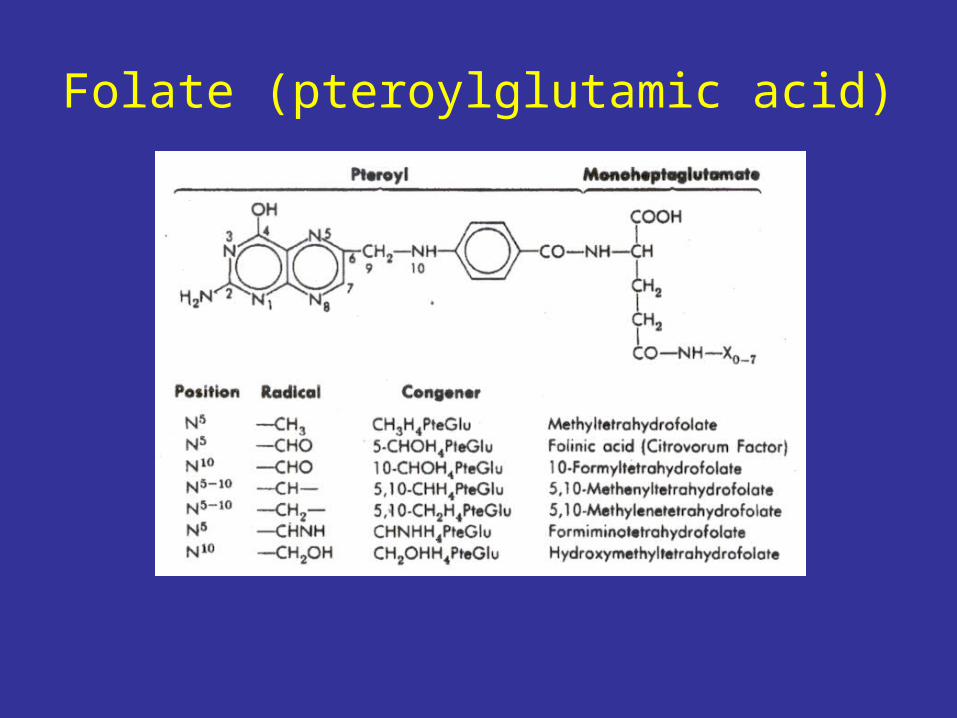
Folate (pteroylglutamic acid)
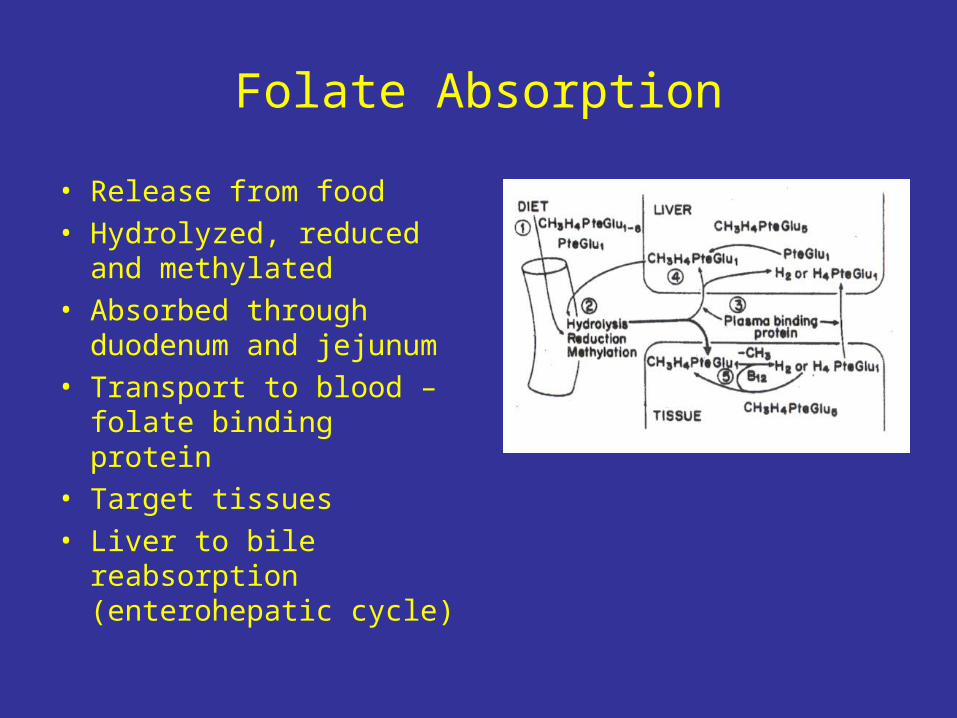
Folate Absorption
• Release from food• Hydrolyzed, reduced and
methylated• Absorbed through
duodenum and jejunum• Transport to blood –
folate binding protein• Target tissues• Liver to bile reabsorption
(enterohepatic cycle)
Folate Deficiency
• Malnutrition• Acute and chronic alcoholism• Defect in folate enterohepatic cycle• Small intestinal diseases• Defects in folate binding protein
• Vitamin B12 deficiency

Folate Therapy
• Oral preparations
Folic acid – drug of choice
• Folic acid injection
Problems with absorption
• Do NOT use folic acid to treat vitamin B12 deficiency
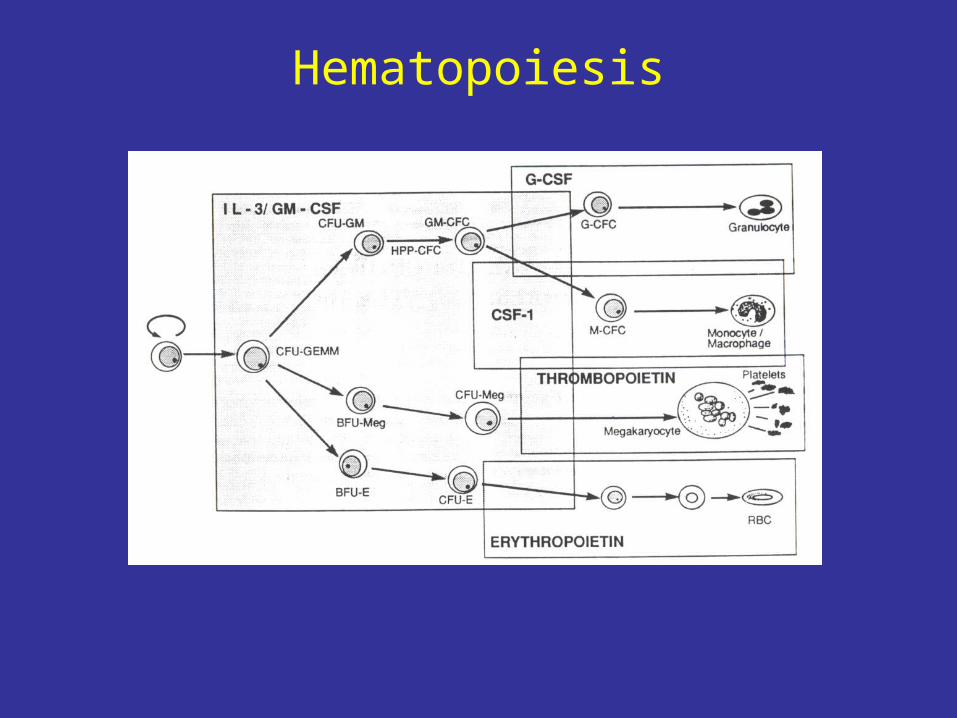
Hematopoiesis

Hematopoietic and LymphopoieticGrowth Factors
• Glycoproteins produced by marrow cells and peripheral tissues
• Active at low concentrations• Act on more than one committed stem cells• Synergism• Networking• Act on several points during cell proliferation and
differentiation
Erythropoietin
• Stimulates proliferation, maturation and hemoglobin formation by CFU-E
• Stimulates the release of reticulocytes• Acts synergistically with IL-3 and GM-CSF• A glycoprotein (34 kDa)• Binds to the erythropoietin receptor and
activates signal transduction processes• Produced primarily by the kidney• Deficiency in anephric patients
Erythropoietin Therapy
• Recombinant erythropoietin (epoetin alpha)• Administered parenterally; half-life ~10 h• 50-100 units/kg; 3 times weekly for patients with
chronic renal failure• Titrate dosage by hematocrit measurements• No significant allergic reactions• Mild adverse effects – lower dosage
• Iron, vitamin B12/folate deficiency
Myeloid Growth Factors(Colony-stimulating Factors)
• Glycoproteins that stimulate the proliferation of one or more myeloid cell lines
• Recombinant GM-CSF, G-CSF, IL-3, M-CSF (CSF-1), SCF, thrombopoietin are available
• GM-CSF and G-CSF are used for treatments of neutropenia
• Administered subcutaneously or intravenously• Short half-life• Adverse effects – bone pain, malaise, flulike
symptoms, more seriously vessel defects
Sickle Cell Anemia
• Hemoglobin
HbA (adult) – α2β2
HbF (fetal) – α2γ2
• Sickle Cell Hemoglobin – a single E6V mutation in the β chain
HbA (adult) – α2β2s

Normal vs Sickled Erythrocytes
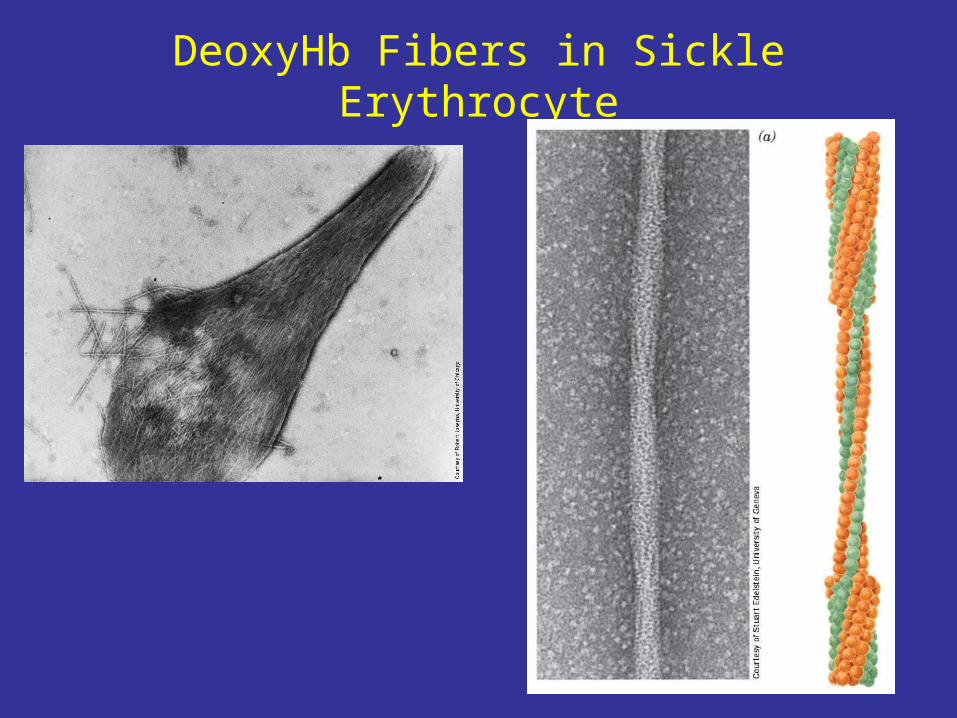
DeoxyHb Fibers in Sickle Erythrocyte
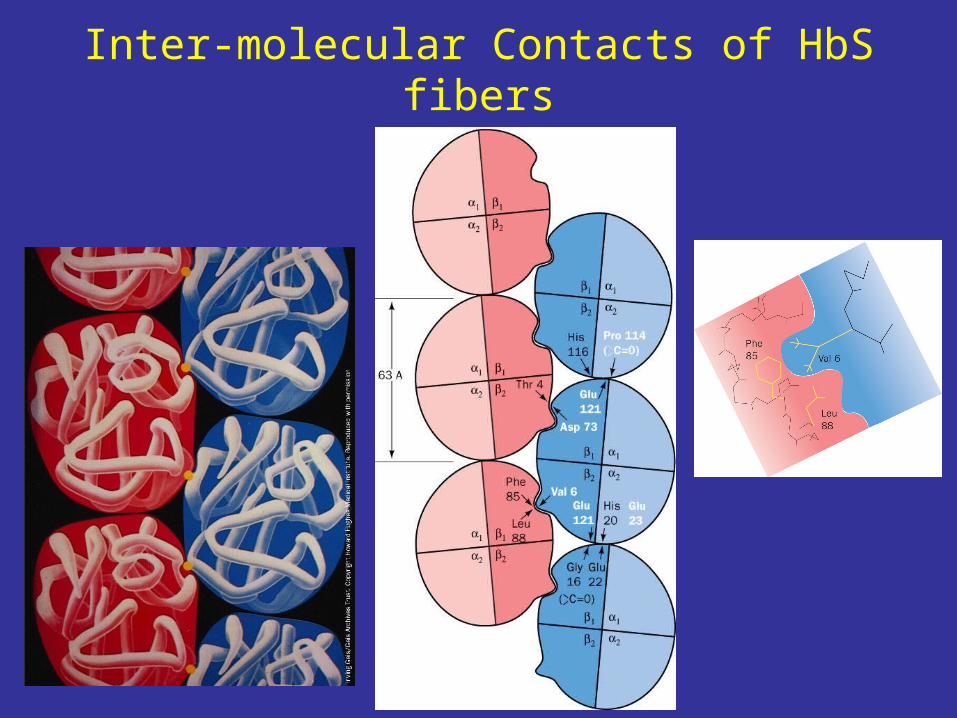
Inter-molecular Contacts of HbS fibers
Defects of Sickled Erythrocytes
• More rigid and adhesive – lodged in micro-vasculatures resulting in vascular occlusion
• Microinfarction – kidney, impaired its ability to concentrate urine and produce erythropoietin
• Altered ability to activate complement and defective granulocyte function - infections
• Splenic sequestration of sickled erythrocytes results in hemolytic anemia and splenomegaly
Treatments of Sickle Cell Disease
• Gene therapy• Prevention of infections - penicillin in children• Supportive managements of vaso-occlusive
crises – pain killers, chronic heparin therapy• Hydroxyurea increases HbF levels to 15-20%,
reducing frequency of vaso-occlusive crises• Prophylactic use, not for treatments of crises• Cytotoxic, side effects include GI effects (nausea,
vomiting, diarrhea), dermatologic effect (macular papular rash, pruritus) and risk of secondary neoplasm (leukemia) with prolonged use
• Hydroxyurea + Erythropoietin therapy?