anaphylaxis. rapid recognition and treatment
DESCRIPTION
Revisión actualizada 2015 UpToDateTRANSCRIPT

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 1/42
Official reprint from UpToDate www.uptodate.com ©2015 UpToDate
AuthorsF Estelle R Simons, MD,FRCPCCarlos A Camargo, Jr, MD,DrPH
Section EditorBruce S Bochner, MD
Deputy EditorAnna M Feldweg, MD
Anaphylaxis: Rapid recognition and treatment
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Dec 2014. | This topic last updated: Dec 18, 2014.
INTRODUCTION — Anaphylaxis is a potentially fatal disorder. In industrialized countries, the lifetime prevalencefrom all causes has been estimated to be between 0.05 and 2 percent in the general population and the rate ofoccurrence is increasing [16]. In the United States, the lifetime prevalence of anaphylaxis is reported to be 1.6percent, based on strict clinical diagnostic criteria [7]. Anaphylaxis is not always recognized as such because itcan mimic other conditions and is variable in its presentation.
This topic will review the recognition and treatment of anaphylaxis by healthcare professionals working in settingssuch as an emergency department (ED), surgical unit, hemodialysis facility, hospital ward, clinic, or clinician'soffice [812]. Unique features of anaphylaxis in pregnant women and infants are presented separately, as is thepathophysiology of anaphylaxis. (See "Anaphylaxis in pregnant and breastfeeding women" and "Anaphylaxis ininfants" and "Pathophysiology of anaphylaxis".)
DEFINITION AND DIAGNOSIS — Anaphylaxis is defined as a serious allergic or hypersensitivity reaction that israpid in onset and may cause death [13,14]. The diagnosis of anaphylaxis is based primarily upon clinicalsymptoms and signs, as well as a detailed description of the acute episode, including antecedent activities andevents occurring within the preceding minutes to hours.
Anaphylaxis is underrecognized and undertreated [13,5]. This may partly be due to failure to appreciate that it canpresent without obvious skin symptoms and signs and without shock. Anaphylaxis is a much broader syndromethan "anaphylactic shock," and the goal of therapy should be early recognition and treatment with epinephrine toprevent progression to lifethreatening respiratory and/or cardiovascular symptoms and signs, including shock.
Diagnostic criteria — Diagnostic criteria for anaphylaxis were published by a multidisciplinary group of experts in2005 and 2006 [13,14]. These criteria were intended to help clinicians recognize the full spectrum of symptomsand signs that comprise anaphylaxis. Recognition of the variable and atypical presentations of anaphylaxis iscritical to providing effective therapy in the form of epinephrine, as well as reducing overreliance on secondlinemedications such as antihistamines and glucocorticoids that are not lifesaving in anaphylaxis [15]. In aretrospective cohort study of 214 emergency department (ED) patients, these criteria were found to have asensitivity of 97 percent compared with an allergist's diagnosis upon review of the case, as well as a specificity of82 percent, a positivepredictive value of 69 percent, and a negativepredictive value of 98 percent [16].
There are three diagnostic criteria, each reflecting a different clinical presentation of anaphylaxis (table 1) [13].Anaphylaxis is highly likely when any ONE of the following three criteria is fulfilled:
Criterion 1 — Acute onset of an illness (minutes to several hours) involving the skin, mucosal tissue, or both(eg, generalized hives, pruritus or flushing, swollen lipstongueuvula) and at least one of the following:
®®
Respiratory compromise (eg, dyspnea, wheezebronchospasm, stridor, reduced peak expiratory flow,hypoxemia).
OR

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 2/42
Note: Skin symptoms and signs are present in up to 90 percent of anaphylactic episodes. This criterion willtherefore frequently be helpful in making the diagnosis.
Criterion 2 — Two or more of the following that occur rapidly after exposure to a LIKELY allergen for thatpatient (minutes to several hours):
Note: Skin symptoms or signs are absent or unrecognized in up to 20 percent of anaphylactic episodes. Criterion 2incorporates gastrointestinal symptoms in addition to skin symptoms, respiratory symptoms, and reduced BP. It isapplied to patients with exposure to a substance that is a likely allergen for them.
Criterion 3 — Reduced BP after exposure to a KNOWN allergen for that patient (minutes to several hours):
Note: Criterion 3 is intended to detect anaphylactic episodes in which only one organ system is involved and isapplied to patients who have been exposed to a substance to which they are known to be allergic, for example,hypotension or shock after an insect sting.
There will occasionally be patients who do not fulfill any of these criteria, but for whom the administration ofepinephrine is appropriate. As an example, it would be appropriate to administer epinephrine to a patient with ahistory of nearfatal anaphylaxis to peanut who presents with urticaria and flushing that developed within minutesof a known or suspected ingestion of peanut [14].
Symptoms and signs — Anaphylaxis may present with various combinations of approximately 40 potentialsymptoms and signs (table 2) [814,1725].
Common symptoms and signs of anaphylaxis include the following:
Reduced blood pressure (BP) or associated symptoms and signs of endorgan dysfunction (eg, hypotonia[collapse] syncope, incontinence). (See 'Criterion 3' below.)
Involvement of the skinmucosal tissue (eg, generalized hives, itchflush, swollen lipstongueuvula).
Respiratory compromise (eg, dyspnea, wheezebronchospasm, stridor, reduced peak expiratory flow,hypoxemia).
Reduced BP or associated symptoms and signs (eg, hypotonia [collapse], syncope, incontinence).
Persistent gastrointestinal symptoms and signs (eg, crampy abdominal pain, vomiting).
Reduced BP in adults is defined as a systolic BP of less than 90 mmHg or greater than 30 percent decreasefrom that person's baseline
In infants and children, reduced BP is defined as low systolic BP (age specific)* or greater than 30 percentdecrease in systolic BP
* Low systolic BP for children is defined as:
Less than 70 mmHg from 1 month up to 1 year•
Less than (70 mmHg + [2 x age]) from 1 to 10 years•
Less than 90 mmHg from 11 to 17 years•
Skin symptoms and signs, which occur in up to 90 percent of episodes, including generalized hives, itchingor flushing, swollen lipstongueuvula, periorbital edema, conjunctival swelling.
Respiratory symptoms and signs, which occur in up to 70 percent of episodes, including nasal discharge,nasal congestion, change in voice quality, sensation of throat closure or choking, stridor, shortness of breath,wheeze, cough.
Gastrointestinal symptoms and signs, which occur in up to 45 percent of episodes, including nausea,
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 3/42
Anaphylaxis may be mild and resolve spontaneously due to endogenous production of compensatory mediators(eg, epinephrine, angiotensin II, endothelin, and others) or it may be severe and progress within minutes torespiratory or cardiovascular compromise and death [19]. The factors that determine the course of anaphylaxis inan individual patient are not fully understood. At the onset of an anaphylactic episode, it is not possible to predicthow severe it will become, how rapidly it will progress, and whether it will resolve promptly and completely orbecome biphasic or protracted.
Death from anaphylaxis usually results from asphyxiation due to upper or lower airway obstruction or tocardiovascular collapse [15,2633]. (See "Fatal anaphylaxis".)
Unique aspects of the clinical manifestations of anaphylaxis in infants and in pregnant women during labor anddelivery are reviewed separately. (See "Anaphylaxis in infants" and "Anaphylaxis in pregnant and breastfeedingwomen".)
Time course — Anaphylaxis is usually characterized by a defined exposure to a potential trigger, followed byrapid onset, evolution, and resolution of symptoms and signs within minutes to hours.
Biphasic anaphylaxis — Biphasic anaphylaxis is defined as a recurrence of symptoms that developsfollowing the apparent resolution of the initial anaphylactic episode with no additional exposure to the trigger.Biphasic reactions have been reported to develop in 4.5 to 23 percent of anaphylactic episodes. Biphasic reactionswere reported in up to 11 percent of children with anaphylaxis [34,35]. They typically occur within 8 to 10 hoursafter resolution of the initial symptoms, although recurrences up to 72 hours later have been reported. (See"Biphasic and protracted anaphylaxis".)
Protracted anaphylaxis — Protracted anaphylaxis is defined as an anaphylactic reaction that lasts for hours,days, or even weeks in extreme cases [26].
Pitfalls in making the diagnosis — Anaphylaxis is not always easy to recognize clinically. The patterns of targetorgan involvement are variable and may differ among individuals, as well as among episodes in the sameindividual. Anaphylaxis is likely underdiagnosed and underreported for a variety of reasons [3,811,2024,36]:
vomiting, diarrhea, and crampy abdominal pain.
Cardiovascular symptoms and signs, which occur in up to 45 percent of episodes, including hypotonia(collapse), syncope, incontinence, dizziness, tachycardia, and hypotension.
Some healthcare professionals remain reluctant to diagnose anaphylaxis in the absence of hypotension orshock, even though changes in BP are not necessarily required for the diagnosis according to criterion 1 orcriterion 2 [13]. (See 'Diagnostic criteria' above.)
Hypotension may go undetected when the initial BP measurement is obtained after epinephrineadministration, or when an inappropriately small BP cuff is used. In infants and young children, BP is lowerthan it is in teenagers and adults.
Many of the dramatic physical signs associated with hypoxia and hypotension in anaphylaxis arenonspecific, such as dyspnea, stridor, wheeze, confusion, collapse, unconsciousness, and incontinence(table 2).
Skin symptoms and signs (such as hives, itching, flushing, and angioedema), which are helpful in making thediagnosis, are absent or unrecognized in up to 20 percent of all episodes. Skin symptoms and signs may beabsent if a patient has taken an H1 antihistamine. They may also be missed if an individual cannot describeitching or is not undressed and fully examined during the episode, or in patients who are draped duringsurgery [19]. (See "Perioperative anaphylaxis: Clinical manifestations, etiology, and diagnosis".)
Anaphylaxis may be difficult to recognize in certain clinical situations. For example, hemodialysis, surgery orchildbirth, when for other reasons patients may experience dramatic physiologic shifts with consequent
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 4/42
TRIGGERS AND MECHANISMS — Most anaphylaxis episodes are triggered through an immunologicmechanism involving immunoglobulin E (IgE). Foods are the most common trigger in children, while medicationsand insect stings are more common triggers in adults than in children. The table provides a more comprehensivelist of potential anaphylaxis triggers, categorized by causative mechanism (table 4) [13,14,17,2024].
In this review, the term anaphylaxis applies to all of the following:
The acute management of anaphylaxis is the same, regardless of the trigger or mechanism involved[13,14,17].
CONTRIBUTORY FACTORS — Comorbidities and concurrent medications may impact the severity ofsymptoms and signs and response to treatment in patients with anaphylaxis (table 5) [2024,38].
Comorbidities — Asthma and cardiovascular disease are the most important risk factors for a poor outcome fromanaphylaxis. Other disorders may also increase risk.
Concurrent medications — Concurrent administration of certain medications, such as betaadrenergic blockers,angiotensinconverting enzyme (ACE) inhibitors, and alphaadrenergic blockers may increase the likelihood of
changes in vital signs [812,19,36,37]. In addition, inability of the patient to communicate the presence ofearly symptoms (eg, if dysphonic, dyspneic, in shock, unconscious, or anesthetized) also impedes promptrecognition of anaphylaxis.
Anaphylaxis in a known asthmatic may be mistaken for an asthma exacerbation if accompanying skinsymptoms and signs such as itching and hives or dizziness suggestive of impending shock are overlooked[19].
Patients experiencing their first episode may not recognize the symptoms as anaphylaxis. As a result, theymay not report symptoms fully or may focus on one prominent symptom (eg, unless specifically asked, apatient presenting with vomiting may not report that the episode was preceded by diffuse itching).
The above factors are further compounded in patients with neurologic, psychiatric, or psychologic problems,or those who take medications or substances such as a sedating H1 antihistamine, ethanol, or recreationaldrugs that potentially impair cognition and judgment, making anaphylaxis symptoms difficult to recognize(table 3) [19,23].
Acute systemic reactions involving IgEdependent mechanisms.
Acute systemic reactions involving other immunologic mechanisms (formerly called anaphylactoid reactions).
Acute systemic reactions that occur independently of any immunologic mechanism due to direct release ofhistamine and other mediators from mast cells and basophils (eg, after exercise or exposure to cold orultraviolet light, ingestion of opioids, etc).
Acute systemic reactions without any obvious trigger or mechanism (idiopathic anaphylaxis).
Persistent asthma is a risk factor for anaphylaxis [39,40]. Asthma is also associated with increased risk ofdeath from anaphylaxis, especially in adolescents and young adults with poorlycontrolled disease [15,2630].
Cardiovascular disease is an important risk factor for death from anaphylaxis in middleaged and olderindividuals [31].
Other respiratory diseases, eg, chronic obstructive pulmonary disease (COPD), interstitial lung disease, orpneumonia are also risk factors for severe or fatal anaphylaxis in older adults [31,41].
Acute infection such as an upper respiratory tract infection, fever, emotional stress, exercise, disruption ofroutine, and premenstrual status may also increase the risk. With the exception of exercise, these amplifyingfactors have not been systematically studied in the context of anaphylaxis [21].
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 5/42
severe or fatal anaphylaxis, and may also interfere with the patient's ability to respond to treatment and with thepatient's compensatory physiologic responses (table 5) [4245].
LABORATORY TESTS — The clinical diagnosis of anaphylaxis can sometimes be supported by documentationof elevated concentrations of serum or plasma total tryptase or plasma histamine [38,4851]. It is critical to obtainblood samples for measurement of these mast cell and basophil mediators soon after the onset of symptomsbecause elevations are transient. Instructions for proper collection of samples are provided in the table (table 6).
Betaadrenergic blockers, administered orally, parenterally, or topically (eg, eye drops) are sometimesassociated with severe anaphylaxis and may also potentially make anaphylaxis more difficult to treat. Theycan cause unopposed alphaadrenergic effects, leading to paradoxical hypertension, as well as reduce thebronchodilator and cardiovascular responses to betaadrenergic stimulation by endogenous or exogenousepinephrine [46]. (See 'Glucagon for patients taking betablockers' below.)
Alphaadrenergic blockers may decrease the effects of endogenous or exogenous epinephrine at alphaadrenergic receptors, potentially making anaphylaxis less responsive to the alphaadrenergic effects ofepinephrine [44].
ACE inhibitors are of particular importance in regards to patients who have experienced anaphylaxis toHymenoptera venom [45,46]. They not only block the effect of angiotensin, a compensatory response, butalso block the degradation of kinins which are active in the production of symptoms and signs.
In an emergency department (ED) study, use of antihypertensive medications in aggregate (betablockers,ACE inhibitors, calcium channel blockers, angiotensinreceptor blockers, or diuretics) by patients withanaphylaxis was associated with increased organ system involvement and increased odds of hospitaladmission, independent of age, gender, suspected trigger, or preexisting lung disease [47].
Serum or plasma total tryptase – The standardized assay for measurement of total serum or plasmatryptase is widely available in clinical laboratories (normal range 1 to 11.4 ng/mL, Thermo Fisher Scientific).In infants under age six months, normal baseline total tryptase concentrations are higher than they are inolder infants, children, and adults [49,52]. Optimally, the blood sample for tryptase measurement needs to beobtained from 15 minutes to 3 hours of symptom onset.
Tryptase elevations are more likely to be detected in anaphylaxis from stinging insect venoms or medicationsand during reactions that involve hypotension [48].
A tryptase level that is within normal limits cannot be used to refute the clinical diagnosis of anaphylaxis[38]. The history trumps the test results. As an example, in individuals with foodinduced anaphylaxis, or inpatients who are normotensive, tryptase levels are seldom elevated, even in optimallytimed blood samplesobtained within 15 minutes to 3 hours of symptom onset [26].
Serial measurements of total tryptase in serum or plasma over several hours may increase the sensitivityand the specificity of the tests. In a prospective study, sequential serum tryptase concentrations weremeasured in 102 adults with anaphylaxis [53]. Tryptase levels one to two hours after onset of the episodewere significantly elevated (19.3 ± 15.4 mcg/L), compared with levels at four to six hours and at 12 to 24hours after the onset, and at baseline (all <11.4 mcg/L). However, tryptase was not elevated in 37 percent ofcases. (See "Laboratory tests to support the clinical diagnosis of anaphylaxis" and "Anaphylaxis: Confirmingthe diagnosis and determining the trigger(s)".)
If a tryptase level obtained 24 or more hours after resolution of clinical symptoms and signs is still elevated,the patient should be referred to an allergy/immunology specialist for evaluation of possible systemicmastocytosis or mast cell activation syndrome. (See "Mastocytosis (cutaneous and systemic):Epidemiology, pathogenesis, and clinical manifestations".)
Plasma histamine – Plasma histamine levels typically peak within 5 to 15 minutes of the onset of

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 6/42
DIFFERENTIAL DIAGNOSIS — Approximately 40 other diseases and conditions might need to be considered inthe differential diagnosis of anaphylaxis (table 7) [50,5763]. The most common disorders in the differentialdiagnosis include acute generalized urticaria and/or angioedema, acute asthma exacerbations, syncope/faint, andanxiety/panic attacks. These are reviewed in detail elsewhere. (See "Differential diagnosis of anaphylaxis inchildren and adults" and "Anaphylaxis in pregnant and breastfeeding women", section on 'Differential diagnosis'and "Anaphylaxis in infants", section on 'Differential diagnosis'.)
IMMEDIATE MANAGEMENT — The tables provide rapid overviews of the initial assessment and emergencymanagement of anaphylaxis in adults (table 8) and children (table 9).
Prompt assessment and treatment are critical in anaphylaxis, as respiratory or cardiac arrest and death can occurwithin minutes [15,2633]. The cornerstones of initial management are the following [6469]:
anaphylaxis symptoms, and then decline to baseline by 60 minutes due to rapid metabolism by Nmethyltransferase and diamine oxidase. Elevated plasma histamine levels correlate with anaphylaxissymptoms and signs and are more likely to be increased than are total serum tryptase levels [51]. (See"Laboratory tests to support the clinical diagnosis of anaphylaxis".)
Measurement of this mediator may be useful in cases of anaphylaxis occurring in a hospital setting in whichblood samples can be collected soon after the onset of symptoms. In many cases of anaphylaxis in thecommunity, however, it is not practical to measure histamine because typically by the time the patientreaches the emergency department (ED), levels have returned to baseline [38,48].
Histamine should be measured in plasma, not serum, because clotting may result in release of histaminethat is artifactual and only occurs ex vivo due to compromised basophil cell membranes. Blood samples forhistamine require special handling: draw blood through a widebore needle, keep it cold at all times,centrifuge it immediately, and freeze the plasma promptly [38]. (See "Laboratory tests to support the clinicaldiagnosis of anaphylaxis".)
Histamine and histamine metabolites can sometimes be detected in the urine following anaphylaxis andelevations are less fleeting than elevations in plasma histamine. However, a 24hour urine collection startedas soon as possible after the reaction begins is required. This is discussed separately. (See "Laboratorytests to support the clinical diagnosis of anaphylaxis", section on 'Histamine metabolites'.)
Potential future tests – The development of a rapid, sensitive, specific laboratory test or panel of tests thathelps clinicians to confirm the diagnosis of anaphylaxis in real time remains an important goal [17,38].
A laboratory test for mature betatryptase, a better marker of mast cell activation than total tryptase (whichmeasures constitutively secreted alphatryptase in addition to betatryptase) has been developed, although itis not widely available [17]. Testing for mature betatryptase is reviewed separately. (See "Laboratory teststo support the clinical diagnosis of anaphylaxis" and "Anaphylaxis: Confirming the diagnosis and determiningthe trigger(s)".)
Other potential markers of mast cell and/or basophil degranulation, such as plateletactivating factor, mastcell carboxypeptidase A3, chymase, and basogranulin are under investigation [38,51,5456].
Removal of the inciting antigen, if possible (eg, stop infusion of a suspect medication).
Call for help (summon a resuscitation team in a hospital setting, or call 911 or an equivalent emergencymedical services number in a community setting).
Intramuscular injection of epinephrine.
Placement of the patient in the supine position with the lower extremities elevated, or if dyspneic or vomiting,placement of the patient semirecumbent with lower extremities elevated.
Supplemental oxygen.

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 7/42
In a series of 164 fatalities due to anaphylaxis, the median time interval between onset of symptoms andrespiratory or cardiac arrest was 5 minutes in iatrogenic anaphylaxis, 15 minutes in stinging insect venominducedanaphylaxis, and 30 minutes in foodinduced anaphylaxis [15]. A more detailed review of fatal anaphylaxis ispresented elsewhere. (See "Fatal anaphylaxis".)
Initial assessment — A number of critical components in the initial management need to be institutedconcomitantly [2024]:
Airway management — As noted above, the initial steps in anaphylaxis management involve a rapid assessmentof the patient's airway [2024]:
Intubation may be difficult in individuals in whom edema distorts the upper airway anatomical landmarks. Failedattempts can lead to complete airway obstruction and fatality. Therefore, upper airway closure in the setting ofanaphylaxis should be managed by the most experienced clinician available. This may require immediatecollaboration between an emergency medicine specialist and an anesthesiologist, otolaryngologist, or intensivistwith training and experience in the management of the difficult airway. Hospitals and other healthcare facilitiesshould have clear written policies about how such situations will be handled.
Intravenous fluids — Intravenous access should be obtained in case fluid resuscitation is required. Massive fluidshifts can occur rapidly in anaphylaxis due to increased vascular permeability, with transfer of up to 35 percent of
Volume resuscitation with intravenous fluids.
Initially, attention should focus on airway, breathing, and circulation, as well as adequacy of mentation. Theskin should be examined.
Epinephrine should be injected intramuscularly into the midouter aspect of the thigh (table 8 and table 9) [6572]. If symptoms are severe, an intravenous epinephrine infusion should be prepared. (See 'Dosing andadministration' below.)
The patient should be placed in the recumbent position with the lower extremities elevated to maximizeperfusion of vital organs. This also helps prevent the "empty ventricle syndrome," in which severehypotension leads to inadequate cardiac filling and pulseless cardiac activity. In this syndrome, death canoccur within seconds [69]. Individuals with respiratory distress or vomiting may not tolerate the recumbentposition and should be placed in a position of comfort, with lower extremities elevated. Empty ventriclesyndrome is discussed in greater detail separately. (See "Fatal anaphylaxis".)
Supplemental oxygen, 8 to 10 liters by facemask, up to 100 percent, should be administered.
Two largebore intravenous catheters (ideally 14 to 16 gauges for most adults) should be inserted inpreparation for rapid administration of fluids and medications.
In normotensive adults, isotonic (0.9 percent) saline should be infused at a rate of 125 mL per hour tomaintain venous access. In normotensive children, isotonic saline should be infused at an appropriatemaintenance rate for weight in order to maintain venous access. (See "Maintenance fluid therapy inchildren".)
Continuous electronic monitoring of cardiopulmonary status, including blood pressure (BP), heart rate, andrespiratory rate, and monitoring of oxygen saturation by pulse oximetry is required for the duration of theepisode.
Intubation should be performed immediately if marked stridor or respiratory arrest is present.
Preparations for possible intubation should be made if there is any airway involvement or significant edemaof the tongue, facial, or neck tissues.
In a minority of cases, an emergency cricothyroidotomy may be required to secure the airway.

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 8/42
the intravascular volume into the extravascular space within minutes [65]. Any patient whose hypotension doesnot respond promptly and completely to injected epinephrine should be assumed to have intravascular volumedepletion causing persistent hypotension despite maximum vasoconstriction. These patients should receive largevolume fluid resuscitation [2024]. The following principles should guide therapy:
Fluid resuscitation should be initiated immediately in patients who present with orthostasis, hypotension, orincomplete response to intramuscular epinephrine.
Normal saline is preferred over other solutions in most situations because other solutions have potentialdisadvantages:
Patients should be monitored carefully and continuously for clinical response and for volume overload. (See"Treatment of severe hypovolemia or hypovolemic shock in adults" and "Hypovolemic shock in children: Initialevaluation and management".)
Pregnant women — Additional precautions and considerations are important in the management of anaphylaxis inpregnant women. For example, during labor and delivery, positioning of the patient on her left side, providing highflow supplemental oxygen, and maintaining a systolic BP of at least 90 mmHg, as well as continuous fetalmonitoring, are critically important [21]. (See "Anaphylaxis in pregnant and breastfeeding women", section on'Management'.)
PHARMACOLOGIC TREATMENTS — In humans experiencing anaphylaxis, randomized, placebocontrolledtrials that meet current standards have not yet been performed for any pharmacologic intervention. Epinephrine isthe best studied medication in anaphylaxis. The evidence for its use comes from observational studies duringanaphylaxis, randomized controlled clinical pharmacology studies at baseline, studies of anaphylaxis in animalmodels, and epidemiologic studies, including fatality studies. The evidence for use of H1 antihistamines inanaphylaxis is extrapolated from their use in urticaria. The evidence for the use of beta2 adrenergic agonists andglucocorticoids in anaphylaxis is extrapolated from their use in acute asthma.
In the future, it is possible that randomized controlled trials will be conducted in anaphylaxis with glucocorticoids,H1 antihistamines, or H2 antihistamines; however, placebocontrolled trials with epinephrine will never beperformed, due to ethical considerations. Anaphylaxis can kill within minutes [15,2631] and delayed epinephrineinjection is associated with fatalities [72,7478].
Epinephrine — Epinephrine is the drug of choice for anaphylaxis. The pharmacologic actions of this agentaddress the pathophysiologic changes that occur in anaphylaxis better than any other medication. It decreasesmediator release from mast cells [79]. Moreover, it is the only medication that prevents or reverses obstruction toairflow in the upper and lower respiratory tracts and prevents or reverses cardiovascular collapse (table 8 and table9).
Therapeutic actions and adverse effects — The therapeutic actions of epinephrine include the following (table10) [66,72,7578,80]:
Adults should receive 1 to 2 liters of normal saline at a rate of 5 to 10 mL/per kilogram in the first minutes oftreatment. Large volumes of fluid (eg, up to 7 liters) may be required.
Children should receive normal saline in boluses of 20 mL per kilogram, each over 5 to 10 minutes, andrepeated as needed. Large volumes of fluid (up to 100 mL per kilogram) may be required.
Lactated Ringer's solution can potentially contribute to metabolic acidosis.
Dextrose is rapidly extravasated from the circulation into the interstitial tissues.
Colloid solutions (eg, albumin or hydroxyethyl starch) confer no survival advantage in patients withdistributive shock and are more costly [73].
Alpha1 adrenergic agonist effects – Increased vasoconstriction, increased peripheral vascular resistance,

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source=… 9/42
In patients of all ages, epinephrine administered in therapeutic doses by any route often causes mild transientpharmacologic effects, such as anxiety, restlessness, headache, dizziness, palpitations, pallor, and tremor[66,77,78,80]. These symptoms and signs are similar to those occurring during the physiologic "fight or flight"response due to endogenous epinephrine that occurs normally in sudden frightening or lifethreatening situations.
Rarely, and especially after overdose, epinephrine may lead to ventricular arrhythmias, angina, myocardialinfarction, pulmonary edema, sudden sharp increase in blood pressure (BP), and intracranial hemorrhage. Seriousadverse effects occur most commonly after an intravenous bolus injection or an overly rapid intravenous infusionparticularly in patients who do not have continuous electronic monitoring of BP and heart rate and function. Theyalso occur after erroneous intravenous injection of a 1 mg/mL epinephrine solution instead of an appropriatelydiluted 0.1 mg/mL or 0.01 mg/mL epinephrine solution [72,77,81]. (See 'Situations requiring caution' below.)
Anaphylaxis itself can lead to angina, myocardial infarction, and cardiac arrhythmias in the absence of anyexogenous epinephrine or before exogenous epinephrine is administered [82].
Dosing and administration — Confusion persists among clinicians regarding the optimal epinephrine doseand route of administration for the initial treatment of anaphylaxis [81].
and decreased mucosal edema (eg, in the upper airway).
Beta1 adrenergic agonist effects – Increased inotropy and increased chronotropy.
Beta2 adrenergic agonist effects – Increased bronchodilation and decreased release of mediators ofinflammation from mast cells and basophils.
Intramuscular injection – Intramuscular injection is recommended over subcutaneous injection because itconsistently provides a more rapid increase in the plasma and tissue concentrations of epinephrine [67,68].Epinephrine is commercially available in several dilutions and great care must be taken to use the correctdilution [2024]. The epinephrine dilution for intramuscular injection contains 1 mg per mL and may also belabeled as 1:1000.
For adults, the recommended dose of epinephrine (1 mg per mL) is 0.3 to 0.5 mg per single dose, injectedintramuscularly into the midouter thigh (vastus lateralis muscle). Based on clinical experience andconsensus opinion, this dose may be repeated at 5 to 15 minute intervals [2123,80].
For infants and children, the recommended dose of epinephrine (1 mg per mL) is 0.01 mg per kilogram. Thedose should be drawn up using a 1 mL syringe. Large children weighing 50 kg or more can receive up to amaximum of 0.5 mg per dose. Epinephrine should be injected intramuscularly into the midouter thigh (vastuslateralis muscle). If there is no response or if the response is inadequate, the injection can be repeated in 5 to15 minutes [66,72,83].
Epinephrine can also be administered into the midouter thigh using an autoinjector. These are available onlyin 0.15 mg and 0.3 mg doses. Children weighing less than 25 kilograms should receive the 0.15 mg dose[66]:
The adult dose is AuviQ 0.3 mg, EpiPen 0.3 mg, Jext 0.3 mg, or other autoinjectors as available,including Emerade 0.5 mg and Adrenaclick. AuviQ is called Allerject in Canada.
•
The pediatric dose is AuviQ 0.15 mg, EpiPen Jr 0.15 mg, Jext 0.15 mg, or other, including Emerade0.15 mg or 0.3 mg and Adrenaclick.
•
The needle used in adults and children should be long enough to penetrate the subcutaneous adipose tissueover the vastus lateralis muscle. Realistically, however, intramuscular injection into the thigh may beimpossible in some patients, especially those who are overweight or obese [84,85]. Although the bestapproach in this situation has not been studied, we suggest as deep an injection as possible into the muscle.
Response to intramuscular epinephrine – Most patients respond to a single dose of intramuscular

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 10/42
Efficacy — Several case series have implicated the failure to administer epinephrine early in the course oftreatment as a consistent finding in anaphylaxis deaths [15,2631,89].
epinephrine, particularly if it is given promptly after the onset of symptoms. When additional intramusculardoses are required, typically one or rarely two additional doses are needed (eg, in patients with severeanaphylaxis and those who cannot access emergency care promptly) [86,87]. In patients who are notresponding to initial intramuscular epinephrine, intravascular fluid status should be assessed carefully beforeprogressing to intravenous epinephrine or other interventions.
Intravenous infusion and indications – Patients who do not respond to several intramuscular injections ofepinephrine and aggressive fluid resuscitation may not be adequately perfusing muscle tissues, as mostcommonly occurs in individuals presenting with profound hypotension or symptoms and signs suggestive ofimpending shock (dizziness, incontinence of urine and/or stool).
Such patients should receive epinephrine by SLOW intravenous infusion, with the rate titrated according toresponse and the presence of continuous electronic hemodynamic monitoring. Slow continuous infusion ispreferred over an intravenous bolus dose as the latter is associated with more dosing errors and moreadverse effects [22,72,88]. An intravenous infusion of epinephrine should preferably be given by clinicianswho are trained, skilled, and experienced in its use and can titrate the rate of infusion (and therefore theepinephrine dose) using continuous noninvasive monitoring of blood pressure (BP), heart rate, and function.
As noted above, epinephrine is commercially available in several dilutions. Great care must be taken to usethe correct dilution in order to avoid overdosing the patient [81]. To prepare an epinephrine intravenousmaintenance infusion for use in a perfusing patient, the commercially available epinephrine solution (eg,ampule, syringe) must be further diluted.
We use a dilution of 4 micrograms per mL in adults and adolescents (1 mg in 250 mL 5 percent dextrosewater) and 10 micrograms per mL in children and infants (1 mg in 100 mL 5 percent dextrose water). Note:Institutional protocols for dilution may vary.
Initial infusion rates:
For adults, the initial dose for intravenous epinephrine infusion is 2 to 10 micrograms per minute withuse of an infusion pump, titrated to effect on BP with continuous noninvasive monitoring [20].
•
For infants and children, the dose for intravenous infusion of epinephrine is 0.1 to 1 microgram perkilogram per minute with use of an infusion pump, titrated to effect on BP with continuous noninvasivemonitoring.
•
Epinephrine is a vesicant and central line administration is preferred. When a patient does not have acentral venous catheter, epinephrine can be temporarily administered through an appropriatelypositioned peripheral venous catheter until a central venous catheter is inserted. Closely monitorcatheter site throughout infusion to avoid extravasation injury.
To reduce the risk of making a medication error, we suggest that centers have available a protocol thatincludes steps on how to prepare and administer epinephrine infusion. Examples of adult (table 11) andpediatric infusions (table 12 and table 13) are provided.
In a series of 13 fatal and nearfatal foodinduced anaphylactic reactions in children and adolescents, the sixpatients who died had symptom onset within one to five minutes after ingestion of the culprit food, but did notreceive their first dose of epinephrine until 25, 60, 80, 90, 125, and 180 minutes after the food was ingested.The authors concluded that the failure to recognize severity of the reactions and to administer epinephrinepromptly increased the risk of a fatal outcome [26].
In a series of anaphylactic deaths occurring from 1992 to 1998, only 20 percent of 24 patients were givenepinephrine at any point in their treatment [27].
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 11/42
In addition, anaphylaxis occurring during evaluation of venom immunotherapy has been investigated prospectively.In one study, 68 patients with a history of anaphylaxis to insect stings were randomly assigned to venomimmunotherapy or placebo immunotherapy [65]. Following this, all were stung in a controlled, monitored settingand treated if needed with a standardized protocol of highflow oxygen, epinephrine infusion, and normal salinerapid infusion. Nineteen of the 21 patients in the placebo group developed anaphylaxis and received epinephrine.Symptoms responded within five minutes in all but one patient. In nine patients, an initial attempt to stop theepinephrine infusion was followed by a return of symptoms, which subsided again once the epinephrine infusionwas restarted.
Finally, there is extensive clinical experience among allergy practitioners with giving epinephrine to treatanaphylaxis occurring in response to immunotherapy. This is a unique situation, because allergy clinic staffobserve patients closely for the symptoms and signs of anaphylaxis and reactions are detected at very earlystages. Over the past few decades, consensus has been reached that even mild systemic reactions are besttreated immediately with epinephrine, as this appears to prevent progression to more severe symptoms moreeffectively than any other available therapies. As a result, successive guidelines for treatment of immunotherapyreactions have called for epinephrine to be given as soon as a systemic reaction of any severity is detected [90].In studies in which all or most patients who developed anaphylaxis after allergen immunotherapy were treatedpromptly with epinephrine injections, symptoms were mild and no additional injections of epinephrine were given,even in the 10 to 23 percent of reactions that were biphasic [91].
Situations requiring caution — There are NO absolute contraindications to epinephrine use in anaphylaxis[2024,72,7578,80].
Subgroups of patients might theoretically be at higher risk for adverse effects during epinephrine therapy. Formalriskbenefit analyses are not possible.
To reiterate, there are no absolute contraindications to the use of epinephrine in the treatment of anaphylaxis. Therisk of death or serious neurologic sequelae from hypoxicischemic encephalopathy due to inadequately treatedanaphylaxis usually outweighs other concerns [2024,72,7578,80]. Existing evidence clearly favors the benefit of
In the fatality series described previously, only 14 percent of the 164 patients dying from anaphylaxisreceived epinephrine before respiratory or cardiac arrest, although 62 percent of the 164 patients eventuallyreceived it before demise [15].
Patients with cardiovascular diseases: Reluctance to administer epinephrine due to fear of adverse cardiaceffects should be countered by the awareness that the heart is a target organ in anaphylaxis. In the healthyhuman heart, mast cells are present throughout the myocardium and in the intima of coronary arteries. Inpatients with coronary artery disease, mast cells are found in atherosclerotic lesions and contribute toatherogenesis. Anaphylaxis can unmask subclinical coronary artery disease, and myocardial infarction and/orarrhythmias can occur during anaphylaxis, even if epinephrine is not injected [43,92]. Moreover, anaphylaxisitself can cause vasospasm, arrhythmias, and myocardial infarction in patients, including children, withhealthy hearts as confirmed by normal electrocardiograms, echocardiograms, and coronary angiograms afterresolution of anaphylaxis [93].
Patients receiving monoamine oxidase inhibitors (which block epinephrine metabolism) or tricyclicantidepressants (which prolong epinephrine duration of action).
Patients with certain preexisting conditions, such as recent intracranial surgery, aortic aneurysm,uncontrolled hyperthyroidism or hypertension, or other conditions that might place them at higher risk foradverse effects related to epinephrine.
Patients receiving stimulant medications (eg, amphetamines or methylphenidate used in the treatment ofattention deficit hyperactivity disorder) or abusing cocaine that might place them at higher risk for adverseeffects from epinephrine.

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 12/42
epinephrine administration in anaphylaxis. Sound clinical judgment is essential.
Glucagon for patients taking betablockers — Patients receiving betablockers may be resistant to treatmentwith epinephrine and can develop refractory hypotension and bradycardia. In this situation, glucagon should beadministered because it has inotropic and chronotropic effects that are not mediated through betareceptors [94]. Adose of 1 to 5 mg in adults (in children, 20 to 30 micrograms per kilogram to a maximum of 1 mg) administeredintravenously over five minutes is recommended. This dose may be repeated or followed by an infusion of 5 to 15micrograms per minute. Rapid administration of glucagon can induce vomiting. Therefore, protection of the airway,for example, by placement in the lateral recumbent position, is important in drowsy or obtunded patients.
Adjunctive agents — Agents that may be given as adjunctive therapies to epinephrine in the treatment ofanaphylaxis include H1 antihistamines, H2 antihistamines, bronchodilators, and glucocorticoids. None of thesemedications should be used as initial treatment or as sole treatment because they do not relieve upper or lowerrespiratory tract obstruction, hypotension, or shock and are not lifesaving.
H1 antihistamines — Epinephrine is firstline treatment for anaphylaxis and there is no known equivalentsubstitute. A systematic review of the literature has failed to retrieve any randomized controlled trials that meetcurrent standards and support the use of H1 antihistamines in anaphylaxis [74].
Despite this, H1 antihistamines are the most commonly administered medications in the treatment of anaphylaxis.This suggests overreliance on these agents, which should be considered adjunctive to epinephrine for the purposeof relieving itching and hives [9598].
For parenteral treatment, only firstgeneration agents are available:
For oral treatment, secondgeneration H1 antihistamines (eg, cetirizine) offer certain advantages over firstgeneration agents (eg, diphenhydramine, chlorpheniramine, hydroxyzine, and promethazine). SecondgenerationH1 antihistamines are less likely to impair cognition or psychomotor performance (eg, the ability to drive safely), orto cause sedation [74,78,101]. Orallyadministered cetirizine acts within 30 to 40 minutes. However, secondgeneration H1 antihistamines are not available in parenteral formulations.
H2 antihistamines — An H2 antihistamine given with an H1 antihistamine may provide some additional reliefof itch and hives [102].
Although H2 antihistamines are sometimes administered in anaphylaxis treatment, a systematic review did notidentify any randomized controlled trials that support the use of these agents in anaphylaxis [103]. H2antihistamines DO NOT relieve upper or lower airway obstruction or shock. Moreover, a systematic review has notidentified randomized controlled trials that support the use of H2 antihistamines in urticaria [104].
If used, ranitidine (50 mg in adults) (12.5 to 50 mg [1 mg per kilogram] in children), may be diluted in 5 percentdextrose to a total volume of 20 mL and injected intravenously over five minutes. Rapid infusion of cimetidine can
H1 antihistamines relieve itch and hives. These medications DO NOT relieve upper or lower airwayobstruction, hypotension or shock, and in standard doses, do not inhibit mediator release from mast cells andbasophils. It is probable that the improvement in noncutaneous symptoms that is sometimes attributed toantihistamine treatment occurs instead because of endogenous production of epinephrine and othercompensatory mediators, including other catecholamines, angiotensin II, and endothelin I [19]. In addition,the onset of action of antihistamines such as cetirizine or diphenhydramine takes 30 to 40 minutes and is tooslow to provide any immediate benefit [99]. H1 antihistamines administered intravenously may increasehypotension [100].
For adults, consider diphenhydramine 25 to 50 mg intravenously, which may be repeated up to a maximumdaily dose of 400 mg per 24 hours.
For children weighing less than 40 kg, consider diphenhydramine 1 mg per kg (maximum 40 mg)intravenously, which may be repeated up to a maximum daily dose of 5 mg per kg or 200 mg per 24 hours.

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 13/42
cause hypotension.
Bronchodilators — For the treatment of bronchospasm not responsive to epinephrine, inhaled bronchodilators,such as albuterol should be administered by facemask and nebulizer/compressor as needed. They are adjunctivetreatment to epinephrine because they do not prevent or relieve mucosal edema in the upper airway or shock, forwhich the alpha1 adrenergic effects of epinephrine are required [2024].
Glucocorticoids — The onset of action of glucocorticoids takes several hours. Therefore, these medicationsdo not relieve the initial symptoms and signs of anaphylaxis. The rationale for giving them is to prevent thebiphasic or protracted reactions that occur in some cases of anaphylaxis. However, a systematic review of theliterature failed to retrieve any randomized controlled trials in anaphylaxis that confirmed the effectiveness ofglucocorticoids [105].
If given, a dose of methylprednisolone of 1 to 2 mg per kilogram per day is sufficient. If glucocorticoid treatment isinstituted, it can be stopped after one or two days without a taper, since all biphasic reactions reported to datehave occurred within 72 hours. (See 'Time course' above.)
Refractory anaphylaxis — Admission to an intensive care unit should occur without delay. There are no publishedprospective studies on the optimal management of refractory anaphylaxis.
Anaphylactic shock displays features of both distributive (vasodilatory) and hypovolemic shock. The managementof severe forms of these types of shock is discussed separately. (See "Systemic inflammatory responsesyndrome (SIRS) and sepsis in children: Definitions, epidemiology, clinical manifestations, and diagnosis" and"Hypovolemic shock in children: Initial evaluation and management" and "Evaluation and management of severesepsis and septic shock in adults", section on 'Vasopressors' and "Treatment of severe hypovolemia orhypovolemic shock in adults".)
One theory about the pathogenesis of refractory anaphylaxis proposes that the clinical manifestations maybecome refractory to further catecholamine administration, perhaps due to saturation or desensitization ofadrenergic receptors [106]. The use of nonadrenergic vasopressors, such as vasopressin, in the management ofanaphylaxis refractory to intravenous epinephrine in adults is discussed elsewhere. (See "Use of vasopressorsand inotropes", section on 'Vasopressin and analogs'.)
Vasoplegia (profound vasodilation) may be present in some cases of refractory anaphylaxis. A few case reportsand other publications support the use of methylene blue, an inhibitor of nitric oxide synthase and guanylatecyclase, in severe anaphylaxis [107,108]. The ideal dose of methylene blue is unknown, but a single bolus of 1 to2 mg/kg has been used. This drug should not be given to patients with pulmonary hypertension, underlyingglucose6phosphate dehydrogenase deficiency (G6PD), or acute lung injury. We also advise caution regardingpotential drug interactions with serotonergic agents. (See "Postoperative complications among patients undergoingcardiac surgery", section on 'Vasodilatory shock'.)
TREATMENT ERRORS — Important errors in the treatment of anaphylaxis include failure to administerepinephrine promptly and delay in epinephrine injection due to overreliance on antihistamines, albuterol(salbutamol), and glucocorticoids. (See 'Adjunctive agents' above.)
Epinephrine should be administered as soon as possible once anaphylaxis is recognized. Delayedadministration has been implicated in contributing to fatalities [15,2631,89]. As noted above, a study of 13fatal or nearfatal foodinduced anaphylactic reactions in children reported that six of the seven children whosurvived received epinephrine within 30 minutes of ingesting the allergen, whereas only two of the sixchildren who died received epinephrine within the first hour [26].
H1 antihistamines are useful for relieving itching and urticaria, as mentioned previously. They do NOT relievestridor, shortness of breath, wheezing, gastrointestinal symptoms and signs, hypotension or shock, andshould not be substituted for epinephrine [20,21,24,74,101].

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 14/42
CARE UPON RESOLUTION — To reduce the risk of recurrence, patients who have been successfully treated foranaphylaxis subsequently require confirmation of the anaphylaxis trigger as well as anaphylaxis education. (See"Anaphylaxis: Confirming the diagnosis and determining the trigger(s)" and "Longterm management of patientswith anaphylaxis".)
Observation — There is no consensus regarding the optimal observation period for a patient who has beensuccessfully treated for anaphylaxis in a healthcare facility. We suggest the following:
Discharge care — All patients who have experienced anaphylaxis should be sent home with an anaphylaxisemergency action plan, one or more epinephrine autoinjectors, a plan for arranging further evaluation, and printedinformation about anaphylaxis and its treatment.
Anaphylaxis emergency action plan — Before discharge, patients should be given a written personalizedanaphylaxis emergency action plan that lists the common symptoms and signs of anaphylaxis and containsinformation about prompt recognition of anaphylaxis and self injection of epinephrine (Anaphylaxis EmergencyAction Plan English) (Anaphylaxis Emergency Action Plan Spanish) [19].
Epinephrine autoinjector — Ideally, patients should be supplied with an epinephrine autoinjector directly.Instructions in the proper use of epinephrine autoinjectors should be reviewed verbally and they should be given aDVD and/or written material and directed to a manufacturer's website video providing relevant information (see'Information for patients' below). If this is not possible, they should be instructed in how to use an epinephrineautoinjector correctly, provided with a prescription for it, and advised to fill the prescription immediately. In asurvey of 1885 patients who survived anaphylaxis, 28 percent of those who did not inject epinephrine duringanaphylaxis reported that they had never received a prescription for an autoinjector [109].
Counseling — The mnemonic "SAFE" was developed to remind clinicians of the four basic action stepssuggested for patients with anaphylaxis who have been treated and are subsequently leaving the emergencydepartment (ED) or hospital [110,111]. These steps are: Seek support, Allergen identification and avoidance,Followup for specialty care, and Epinephrine for emergencies. The SAFE counseling is outlined below and hasbeen incorporated into printable patient information materials. (See 'Information for patients' below.)
Bronchodilator treatment with nebulized albuterol should be given in individuals with severe bronchospasm,as an adjunctive treatment to epinephrine. However, albuterol does NOT prevent or relieve upper airwayedema, hypotension, or shock, and should not be substituted for epinephrine in the treatment of anaphylaxis.
Glucocorticoids theoretically reduce the latephase response. However, they have not been proven to preventor reduce biphasic or protracted anaphylaxis. They do not relieve the initial symptoms of anaphylaxis.
Patients with moderate anaphylaxis who do not respond promptly to epinephrine and all patients with severeanaphylaxis should be admitted to an observation unit or to a hospital.
For patients with anaphylaxis that resolved promptly and completely with treatment, we suggest a minimumobservation period of a few hours, and prefer a period of 8 to 10 hours, if possible. We also suggest that ifpatients are sent home after only a few hours, they should be trained to use an epinephrine autoinjector andshould actually be supplied with one, rather than simply handed a prescription for one. As noted previously,from 4.5 percent to 23 percent of patients may experience a biphasic reaction [34]. (See 'Biphasicanaphylaxis' above.)
Seek support – Advise the patient that:
They have experienced anaphylaxis or "killer allergy," which is a lifethreatening condition.•
Symptoms of the current episode may recur (without further exposure to the trigger) up to three daysafter the initial onset of symptoms.
•
They should self inject epinephrine, and call emergency medical services or get to the nearest•

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 15/42
LONGTERM PROGNOSIS — Patients who have experienced anaphylaxis are at risk for recurrent episodesunless longterm risk reduction measures are implemented [20,21]. Specifically, the trigger for the anaphylacticepisode should be verified. In addition, anaphylaxis education is required in order to help patients successfullyavoid their confirmed trigger(s), and self inject epinephrine promptly and confidently in the event of a recurrentanaphylactic episode. For these reasons, patients with anaphylaxis benefit from referral to an allergy specialist.
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, "The Basics" and"Beyond the Basics." The Basics patient education pieces are written in plain language, at the 5 to 6 gradereading level, and they answer the four or five key questions a patient might have about a given condition. Thesearticles are best for patients who want a general overview and who prefer short, easytoread materials. Beyondthe Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are writtenat the 10 to 12 grade reading level and are best for patients who want indepth information and are comfortablewith some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or email thesetopics to your patients. (You can also locate patient education articles on a variety of subjects by searching on"patient info" and the keyword(s) of interest.)
emergency facility at the first sign of recurrence of symptoms.
They are at risk for repeat episodes of anaphylaxis in the future.•
Refer the patient to resources. (See 'Information for patients' below.)•
Allergen identification and avoidance – Before the patient is discharged, an effort should be made toconfirm the anaphylaxis trigger suspected from the patient's history (by measuring specific immunoglobulin E[IgE] to the allergen identified by the history). If the patient has received volume resuscitation, IgE levelsmight be falsely absent or undetectable due to the potential dilutional effects on circulating IgE, and it mightbe necessary to recheck the levels days or weeks after the anaphylactic episode.
Emphasize the importance of subsequent allergy skin testing to confirm the trigger, so that it can besuccessfully avoided in the future.
•
Followup for specialty care
Advise the patient to followup with his or her primary care clinician and obtain a referral to an allergistor to seek consultation directly with an allergist for testing and ongoing management.
•
Comorbidities such as asthma, other chronic pulmonary disease, and cardiovascular disease should beoptimally controlled.
•
Epinephrine for emergencies
Provide the patient with an epinephrine autoinjector or with a prescription for one and demonstrate properuse. In addition, give the patient written information about how to recognize anaphylaxis and how to use anepinephrine autoinjector, and provide directions to appropriate websites for video demonstrations ofautoinjector use. (See 'Information for patients' below.)
Explain the importance of carrying the epinephrine autoinjector at all times.•
Advise the patient to make sure that family and friends are aware of the risks of anaphylaxis, thetriggers, and how to administer epinephrine. The correct injection technique is important to avoidunintentional injection into fingers, thumbs, or other body parts [112].
•
th th
th th
Basics topics (see "Patient information: Anaphylaxis (The Basics)" and "Patient information: Epinephrineautoinjectors (The Basics)")
Beyond the Basics topics (see "Patient information: Anaphylaxis symptoms and diagnosis (Beyond the

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 16/42
Other sources of accurate patient information accessible through the internet include the American Academy ofAllergy, Asthma and Immunology (www.aaaai.org) and the American College of Allergy, Asthma and Immunology(www.acaai.org) [113,114].
SUMMARY AND RECOMMENDATIONS
Basics)" and "Patient information: Anaphylaxis treatment and prevention of recurrences (Beyond the Basics)"and "Patient information: Use of an epinephrine autoinjector (Beyond the Basics)")
Anaphylaxis is a serious allergic reaction that is rapid in onset and may cause death. (See 'Definition anddiagnosis' above.)
There are three clinical criteria for the diagnosis of anaphylaxis, which reflect the different ways in whichanaphylaxis may present (table 1). Anaphylaxis is highly likely when any ONE of the three criteria is fulfilled.(See 'Diagnostic criteria' above.)
Recognition is not always easy, because anaphylaxis can mimic many other disorders and can bevariable in its presentation. Anaphylaxis may present with various combinations of as many as 40potential symptoms and signs (table 2). (See 'Symptoms and signs' above.)
•
Patients and healthcare professionals commonly fail to recognize and diagnose anaphylaxis in its earlystages, when it is most responsive to treatment. In particular, there is a reluctance to diagnoseanaphylaxis in the absence of hypotension, even though this sign is not required for the diagnosis andis uncommon in children with anaphylaxis or in foodinduced anaphylaxis. (See 'Pitfalls in making thediagnosis' above.)
•
Anaphylaxis most often results from an immunoglobulin E (IgE)mediated allergic reaction. Common triggersinclude foods, insect stings, and medications. There is a rapidly expanding list of novel and/or unusualtriggers (table 4). (See 'Triggers and mechanisms' above.)
The diagnosis of anaphylaxis is based on clinical criteria, and the results of measurements of tryptase andother mediators are not available immediately (ie, STAT) at the point of care. However, detection of elevatedtotal tryptase (in serum or plasma) or histamine (in plasma) can be helpful in excluding other disorders that donot involve activation of mast cells and basophils. Of note, elevations in these mediators are transient. Theblood sample for tryptase should be obtained from 15 minutes to 3 hours of symptom onset (table 6). (See'Laboratory tests' above.)
Prompt recognition and treatment are critical in anaphylaxis. In fatal anaphylaxis, median times tocardiorespiratory arrest are 5 minutes in iatrogenic anaphylaxis, 15 minutes in stinging insect venominducedanaphylaxis, and 30 minutes in foodinduced anaphylaxis. (See 'Time course' above.)
Initial management is summarized in a rapid overview table for adults (table 8) and children (table 9). (See'Immediate management' above.)
Epinephrine is lifesaving in anaphylaxis. It should be injected as early as possible in the episode in order toprevent progression of symptoms and signs. There are no absolute contraindications to epinephrine useand it is the treatment of choice for anaphylaxis of any severity. We recommend epinephrine for patientswith apparently mild symptoms and signs (eg, a few hives and mild wheezing) (Grade 1B) and for patientswith moderate to severe symptoms and signs (Grade 1A).
The route of epinephrine administration depends upon the presenting symptoms. For patients who are notprofoundly hypotensive or in shock or cardiorespiratory arrest, intramuscular injection into the midouter thighas the initial route of administration is advised, in preference to subcutaneous administration or intravenousadministration:
For adults, the dose of epinephrine is 0.3 mg to 0.5 mg, injected intramuscularly into the midouter•

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 17/42
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Lieberman P, Camargo CA Jr, Bohlke K, et al. Epidemiology of anaphylaxis: findings of the AmericanCollege of Allergy, Asthma and Immunology Epidemiology of Anaphylaxis Working Group. Ann AllergyAsthma Immunol 2006; 97:596.
2. Decker WW, Campbell RL, Manivannan V, et al. The etiology and incidence of anaphylaxis in Rochester,Minnesota: a report from the Rochester Epidemiology Project. J Allergy Clin Immunol 2008; 122:1161.
3. Lin RY, Anderson AS, Shah SN, Nurruzzaman F. Increasing anaphylaxis hospitalizations in the first 2decades of life: New York State, 1990 2006. Ann Allergy Asthma Immunol 2008; 101:387.
4. Poulos LM, Waters AM, Correll PK, et al. Trends in hospitalizations for anaphylaxis, angioedema, andurticaria in Australia, 19931994 to 20042005. J Allergy Clin Immunol 2007; 120:878.
5. Sheikh A, HippisleyCox J, Newton J, Fenty J. Trends in national incidence, lifetime prevalence andadrenaline prescribing for anaphylaxis in England. J R Soc Med 2008; 101:139.
6. Liew WK, Williamson E, Tang ML. Anaphylaxis fatalities and admissions in Australia. J Allergy ClinImmunol 2009; 123:434.
7. Wood RA, Camargo CA Jr, Lieberman P, et al. Anaphylaxis in America: the prevalence and characteristicsof anaphylaxis in the United States. J Allergy Clin Immunol 2014; 133:461.
8. Ewan PW, Dugué P, Mirakian R, et al. BSACI guidelines for the investigation of suspected anaphylaxisduring general anaesthesia. Clin Exp Allergy 2010; 40:15.
9. Chacko T, Ledford D. Perianesthetic anaphylaxis. Immunol Allergy Clin North Am 2007; 27:213.10. Harboe T, Benson MD, Oi H, et al. Cardiopulmonary distress during obstetrical anaesthesia: attempts to
thigh. This treatment may be repeated at 5 to 15 minute intervals.
For infants and children, the dose of epinephrine is 0.01 mg per kilogram. Large children weighing 50 kgor can receive up to a maximum of 0.5 mg per dose, injected intramuscularly into the midouter thigh. Ifno response or inadequate response, this treatment can be repeated in 5 to 15 minutes.
•
Intravenous epinephrine is indicated for patients with profound hypotension or symptoms and signssuggestive of impending shock (dizziness, incontinence of urine or stool) or those who do not respond to aninitial intramuscular injection of epinephrine and fluid resuscitation. For these patients we suggest thatepinephrine be administered by continuous slow intravenous infusion rather than by intermittent intravenousbolus (Grade 2C). Patients receiving intravenous epinephrine should have continuous electronic monitoring ofblood pressure (BP), heart rate, and function. (See 'Epinephrine' above and 'Dosing and administration'above.)
Massive fluid shifts can occur in anaphylaxis, and all patients with orthostasis, hypotension, or incompleteresponse to epinephrine should receive large volume fluid resuscitation with normal saline. Normotensivepatients should receive normal saline to maintain venous access in case their status deteriorates. (See'Intravenous fluids' above.)
Supplemental oxygen should be administered. (See 'Initial assessment' above.)
Patients successfully treated for anaphylaxis should be discharged with a personalized written anaphylaxisemergency action plan (Anaphylaxis Emergency Action Plan English) (Anaphylaxis Emergency Action Plan Spanish), an epinephrine autoinjector, written information about anaphylaxis and its treatment, and a planfor further evaluation. (See 'Care upon resolution' above and 'Information for patients' above.)
It is critical that patients be evaluated further to confirm the trigger, as specific avoidance measures areuseful in reducing the risk of recurrence. Additionally, for some allergens, immunomodulation is also availableto reduce the risk. (See 'Care upon resolution' above and 'Longterm prognosis' above.)

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 18/42
diagnose amniotic fluid embolism in a case series of suspected allergic anaphylaxis. Acta AnaesthesiolScand 2006; 50:324.
11. Ebo DG, Bosmans JL, Couttenye MM, Stevens WJ. Haemodialysisassociated anaphylactic andanaphylactoid reactions. Allergy 2006; 61:211.
12. Oswalt ML, Kemp SF. Anaphylaxis: office management and prevention. Immunol Allergy Clin North Am2007; 27:177.
13. Sampson HA, MuñozFurlong A, Campbell RL, et al. Second symposium on the definition and managementof anaphylaxis: summary reportSecond National Institute of Allergy and Infectious Disease/Food Allergyand Anaphylaxis Network symposium. J Allergy Clin Immunol 2006; 117:391.
14. Sampson HA, MuñozFurlong A, Bock SA, et al. Symposium on the definition and management ofanaphylaxis: summary report. J Allergy Clin Immunol 2005; 115:584.
15. Pumphrey RS. Lessons for management of anaphylaxis from a study of fatal reactions. Clin Exp Allergy2000; 30:1144.
16. Campbell RL, Hagan JB, Manivannan V, et al. Evaluation of national institute of allergy and infectiousdiseases/food allergy and anaphylaxis network criteria for the diagnosis of anaphylaxis in emergencydepartment patients. J Allergy Clin Immunol 2012; 129:748.
17. Simons FE. Anaphylaxis. J Allergy Clin Immunol 2010; 125:S161.18. Kemp SF, Lockey RF. Anaphylaxis: a review of causes and mechanisms. J Allergy Clin Immunol 2002;
110:341.19. Simons FE. Anaphylaxis, killer allergy: longterm management in the community. J Allergy Clin Immunol
2006; 117:367.20. Lieberman P, Nicklas RA, Oppenheimer J, et al. The diagnosis and management of anaphylaxis practice
parameter: 2010 update. J Allergy Clin Immunol 2010; 126:477.21. Simons FE, Ardusso LR, Bilò MB, et al. World Allergy Organization anaphylaxis guidelines: summary. J
Allergy Clin Immunol 2011; 127:587.22. Soar J, Pumphrey R, Cant A, et al. Emergency treatment of anaphylactic reactionsguidelines for
healthcare providers. Resuscitation 2008; 77:157.23. Brown SG, Mullins RJ, Gold MS. Anaphylaxis: diagnosis and management. Med J Aust 2006; 185:283.24. Muraro A, Roberts G, Clark A, et al. The management of anaphylaxis in childhood: position paper of the
European academy of allergology and clinical immunology. Allergy 2007; 62:857.25. Muraro A, Roberts G, Worm M, et al. Anaphylaxis: Guidelines from the European Academy of Allergy and
Clinical Immunology (in preparation). Allergy 2014.26. Sampson HA, Mendelson L, Rosen JP. Fatal and nearfatal anaphylactic reactions to food in children and
adolescents. N Engl J Med 1992; 327:380.27. Bock SA, MuñozFurlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin
Immunol 2001; 107:191.28. Bock SA, MuñozFurlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001
2006. J Allergy Clin Immunol 2007; 119:1016.29. Pumphrey R. Anaphylaxis: can we tell who is at risk of a fatal reaction? Curr Opin Allergy Clin Immunol
2004; 4:285.30. Pumphrey RS, Gowland MH. Further fatal allergic reactions to food in the United Kingdom, 19992006. J
Allergy Clin Immunol 2007; 119:1018.31. Greenberger PA, Rotskoff BD, Lifschultz B. Fatal anaphylaxis: postmortem findings and associated
comorbid diseases. Ann Allergy Asthma Immunol 2007; 98:252.32. Shen Y, Li L, Grant J, et al. Anaphylactic deaths in Maryland (United States) and Shanghai (China): a review
of forensic autopsy cases from 2004 to 2006. Forensic Sci Int 2009; 186:1.33. Yilmaz R, Yuksekbas O, Erkol Z, et al. Postmortem findings after anaphylactic reactions to drugs in Turkey.
Am J Forensic Med Pathol 2009; 30:346.34. Rohacek M, Edenhofer H, Bircher A, Bingisser R. Biphasic anaphylactic reactions: occurrence and
mortality. Allergy 2014; 69:791.35. Mehr S, Liew WK, Tey D, Tang ML. Clinical predictors for biphasic reactions in children presenting with

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 19/42
anaphylaxis. Clin Exp Allergy 2009; 39:1390.36. Simons FE. Anaphylaxis in infants: can recognition and management be improved? J Allergy Clin Immunol
2007; 120:537.37. Simons FE, Schatz M. Anaphylaxis during pregnancy. J Allergy Clin Immunol 2012; 130:597.38. Simons FER, Frew AJ, Ansotegui IJ, et al. Risk assessment in anaphylaxis: current and future approaches.
J Allergy Clin Immunol 2007; 120:S2.39. GonzálezPérez A, Aponte Z, Vidaurre CF, Rodríguez LA. Anaphylaxis epidemiology in patients with and
patients without asthma: a United Kingdom database review. J Allergy Clin Immunol 2010; 125:1098.40. Iribarren C, Tolstykh IV, Miller MK, Eisner MD. Asthma and the prospective risk of anaphylactic shock and
other allergy diagnoses in a large integrated health care delivery system. Ann Allergy Asthma Immunol 2010;104:371.
41. Mulla ZD, Simons FE. Concomitant chronic pulmonary diseases and their association with hospitaloutcomes in patients with anaphylaxis and other allergic conditions: a cohort study. BMJ Open 2013; 3.
42. Westfall TC, Westfall DP. Adrenergic agonists and antagonists. In: Goodman and Gilman's thepharmacological basis of therapeutics, 11th ed, Brunton LL (Ed), McGrawHill, New York 2006. p.215.
43. Triggiani M, Patella V, Staiano RI, et al. Allergy and the cardiovascular system. Clin Exp Immunol 2008; 153Suppl 1:7.
44. Watson A. Alpha adrenergic blockers and adrenaline. A mysterious collapse. Aust Fam Physician 1998;27:714.
45. Ruëff F, Przybilla B, Biló MB, et al. Predictors of severe systemic anaphylactic reactions in patients withHymenoptera venom allergy: importance of baseline serum tryptasea study of the European Academy ofAllergology and Clinical Immunology Interest Group on Insect Venom Hypersensitivity. J Allergy ClinImmunol 2009; 124:1047.
46. Mueller UR. Cardiovascular disease and anaphylaxis. Curr Opin Allergy Clin Immunol 2007; 7:337.47. Lee S, Hess EP, Nestler DM, et al. Antihypertensive medication use is associated with increased organ
system involvement and hospitalization in emergency department patients with anaphylaxis. J Allergy ClinImmunol 2013; 131:1103.
48. Schwartz LB. Diagnostic value of tryptase in anaphylaxis and mastocytosis. Immunol Allergy Clin North Am2006; 26:451.
49. Komarow HD, Hu Z, Brittain E, et al. Serum tryptase levels in atopic and nonatopic children. J Allergy ClinImmunol 2009; 124:845.
50. Lieberman PL. Anaphylaxis. In: Middleton's allergy: Principles and practice, 7th ed, Adkinson NF Jr,Bochner BS, Busse WW, et al (Eds), St. Louis 2009. p.1027.
51. Vadas P, Perelman B, Liss G. Plateletactivating factor, histamine, and tryptase levels in humananaphylaxis. J Allergy Clin Immunol 2013; 131:144.
52. Belhocine W, Ibrahim Z, Grandné V, et al. Total serum tryptase levels are higher in young infants. PediatrAllergy Immunol 2011; 22:600.
53. SalaCunill A, Cardona V, LabradorHorrillo M, et al. Usefulness and limitations of sequential serum tryptasefor the diagnosis of anaphylaxis in 102 patients. Int Arch Allergy Immunol 2013; 160:192.
54. Summers CW, Pumphrey RS, Woods CN, et al. Factors predicting anaphylaxis to peanuts and tree nuts inpatients referred to a specialist center. J Allergy Clin Immunol 2008; 121:632.
55. Vadas P, Gold M, Perelman B, et al. Plateletactivating factor, PAF acetylhydrolase, and severeanaphylaxis. N Engl J Med 2008; 358:28.
56. Mochizuki A, McEuen AR, Buckley MG, Walls AF. The release of basogranulin in response to IgEdependent and IgEindependent stimuli: validity of basogranulin measurement as an indicator of basophilactivation. J Allergy Clin Immunol 2003; 112:102.
57. Izikson L, English JC 3rd, Zirwas MJ. The flushing patient: differential diagnosis, workup, and treatment. JAm Acad Dermatol 2006; 55:193.
58. Erem C, Kocak M, Onder Ersoz H, et al. Epinephrinesecreting cystic pheochromocytoma presenting withan incidental adrenal mass: a case report and a review of the literature. Endocrine 2005; 28:225.
59. Ueda T, Oka N, Matsumoto A, et al. Pheochromocytoma presenting as recurrent hypotension and syncope.
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 20/42
Intern Med 2005; 44:222.60. Becker K, Southwick K, Reardon J, et al. Histamine poisoning associated with eating tuna burgers. JAMA
2001; 285:1327.61. Daschner A, AlonsoGómez A, Cabañas R, et al. Gastroallergic anisakiasis: borderline between food allergy
and parasitic diseaseclinical and allergologic evaluation of 20 patients with confirmed acute parasitism byAnisakis simplex. J Allergy Clin Immunol 2000; 105:176.
62. Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1INHdeficiency. J Allergy Clin Immunol 2012; 130:692.
63. Greenberger PA. Idiopathic anaphylaxis. Immunol Allergy Clin North Am 2007; 27:273.64. Brown SG. Cardiovascular aspects of anaphylaxis: implications for treatment and diagnosis. Curr Opin
Allergy Clin Immunol 2005; 5:359.65. Brown SG, Blackman KE, Stenlake V, Heddle RJ. Insect sting anaphylaxis; prospective evaluation of
treatment with intravenous adrenaline and volume resuscitation. Emerg Med J 2004; 21:149.66. Simons FE. Firstaid treatment of anaphylaxis to food: focus on epinephrine. J Allergy Clin Immunol 2004;
113:837.67. Simons FE, Gu X, Simons KJ. Epinephrine absorption in adults: intramuscular versus subcutaneous
injection. J Allergy Clin Immunol 2001; 108:871.68. Simons FE, Roberts JR, Gu X, Simons KJ. Epinephrine absorption in children with a history of anaphylaxis.
J Allergy Clin Immunol 1998; 101:33.69. Pumphrey RS. Fatal posture in anaphylactic shock. J Allergy Clin Immunol 2003; 112:451.70. Brown SG. The pathophysiology of shock in anaphylaxis. Immunol Allergy Clin North Am 2007; 27:165.71. Brown SG. Anaphylaxis: clinical concepts and research priorities. Emerg Med Australas 2006; 18:155.72. Simons KJ, Simons FE. Epinephrine and its use in anaphylaxis: current issues. Curr Opin Allergy Clin
Immunol 2010; 10:354.73. Perel P, Roberts I, Ker K. Colloids versus crystalloids for fluid resuscitation in critically ill patients.
Cochrane Database Syst Rev 2013; 2:CD000567.74. Sheikh A, Ten Broek V, Brown SG, Simons FE. H1antihistamines for the treatment of anaphylaxis:
Cochrane systematic review. Allergy 2007; 62:830.75. Sheikh A, Shehata YA, Brown SG, Simons FE. Adrenaline for the treatment of anaphylaxis: cochrane
systematic review. Allergy 2009; 64:204.76. Simons FE. Emergency treatment of anaphylaxis. BMJ 2008; 336:1141.77. McLeanTooke AP, Bethune CA, Fay AC, Spickett GP. Adrenaline in the treatment of anaphylaxis: what is
the evidence? BMJ 2003; 327:1332.78. Simons FE. Pharmacologic treatment of anaphylaxis: can the evidence base be strengthened? Curr Opin
Allergy Clin Immunol 2010; 10:384.79. Vadas P, Perelman B. Effect of epinephrine on plateletactivating factorstimulated human vascular smooth
muscle cells. J Allergy Clin Immunol 2012; 129:1329.80. Kemp SF, Lockey RF, Simons FE, World Allergy Organization ad hoc Committee on Epinephrine in
Anaphylaxis. Epinephrine: the drug of choice for anaphylaxis. A statement of the World Allergy Organization.Allergy 2008; 63:1061.
81. Kanwar M, Irvin CB, Frank JJ, et al. Confusion about epinephrine dosing leading to iatrogenic overdose: alifethreatening problem with a potential solution. Ann Emerg Med 2010; 55:341.
82. Kounis NG. Coronary hypersensitivity disorder: the Kounis syndrome. Clin Ther 2013; 35:563.83. Hegenbarth MA, American Academy of Pediatrics Committee on Drugs. Preparing for pediatric
emergencies: drugs to consider. Pediatrics 2008; 121:433.84. Song TT, Nelson MR, Chang JH, et al. Adequacy of the epinephrine autoinjector needle length in delivering
epinephrine to the intramuscular tissues. Ann Allergy Asthma Immunol 2005; 94:539.85. Stecher D, Bulloch B, Sales J, et al. Epinephrine autoinjectors: is needle length adequate for delivery of
epinephrine intramuscularly? Pediatrics 2009; 124:65.86. Brown SG, Stone SF, Fatovich DM, et al. Anaphylaxis: clinical patterns, mediator release, and severity. J

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 21/42
Allergy Clin Immunol 2013; 132:1141.87. BenShoshan M, La Vieille S, Eisman H, et al. Anaphylaxis treated in a Canadian pediatric hospital:
Incidence, clinical characteristics, triggers, and management. J Allergy Clin Immunol 2013; 132:739.88. Wheeler DW, Carter JJ, Murray LJ, et al. The effect of drug concentration expression on epinephrine dosing
errors: a randomized trial. Ann Intern Med 2008; 148:11.89. Anchor J, Settipane RA. Appropriate use of epinephrine in anaphylaxis. Am J Emerg Med 2004; 22:488.90. Cox L, Nelson H, Lockey R, et al. Allergen immunotherapy: a practice parameter third update. J Allergy Clin
Immunol 2011; 127:S1.91. Scranton SE, Gonzalez EG, Waibel KH. Incidence and characteristics of biphasic reactions after allergen
immunotherapy. J Allergy Clin Immunol 2009; 123:493.92. Ridella M, Bagdure S, Nugent K, Cevik C. Kounis syndrome following betalactam antibiotic use: review of
literature. Inflamm Allergy Drug Targets 2009; 8:11.93. Biteker M, Duran NE, Biteker FS, et al. Allergic myocardial infarction in childhood: Kounis syndrome. Eur J
Pediatr 2010; 169:27.94. Thomas M, Crawford I. Best evidence topic report. Glucagon infusion in refractory anaphylactic shock in
patients on betablockers. Emerg Med J 2005; 22:272.95. Clark S, Bock SA, Gaeta TJ, et al. Multicenter study of emergency department visits for food allergies. J
Allergy Clin Immunol 2004; 113:347.96. Clark S, Long AA, Gaeta TJ, Camargo CA Jr. Multicenter study of emergency department visits for insect
sting allergies. J Allergy Clin Immunol 2005; 116:643.97. Gaeta TJ, Clark S, Pelletier AJ, Camargo CA. National study of US emergency department visits for acute
allergic reactions, 1993 to 2004. Ann Allergy Asthma Immunol 2007; 98:360.98. Banerji A, Long AA, Camargo CA Jr. Diphenhydramine versus nonsedating antihistamines for acute allergic
reactions: a literature review. Allergy Asthma Proc 2007; 28:418.99. Park HJ, Kim JH, Kim JE, et al. Diagnostic value of the serumspecific IgE ratio of ω5 gliadin to wheat in
adult patients with wheatinduced anaphylaxis. Int Arch Allergy Immunol 2012; 157:147.100. Ellis BC, Brown SG. Parenteral antihistamines cause hypotension in anaphylaxis. Emerg Med Australas
2013; 25:92.101. Simons FE, Simons KJ. Histamine and H1antihistamines: celebrating a century of progress. J Allergy Clin
Immunol 2011; 128:1139.102. Lin RY, Curry A, Pesola GR, et al. Improved outcomes in patients with acute allergic syndromes who are
treated with combined H1 and H2 antagonists. Ann Emerg Med 2000; 36:462.103. Nurmatov UB, Rhatigan E, Simons FE, Sheikh A. H2antihistamines for the treatment of anaphylaxis with
and without shock: a systematic review. Ann Allergy Asthma Immunol 2014; 112:126.104. Fedorowicz Z, van Zuuren EJ, Hu N. Histamine H2receptor antagonists for urticaria. Cochrane Database
Syst Rev 2012; 3:CD008596.105. Choo KJ, Simons FE, Sheikh A. Glucocorticoids for the treatment of anaphylaxis. Cochrane Database Syst
Rev 2012; 4:CD007596.106. Dewachter P, MoutonFaivre C, Emala CW. Anaphylaxis and anesthesia: controversies and new insights.
Anesthesiology 2009; 111:1141.107. Jang DH, Nelson LS, Hoffman RS. Methylene blue for distributive shock: a potential new use of an old
antidote. J Med Toxicol 2013; 9:242.108. Puttgen HA, Mirski MA. The level of evidence 5 blues: investigating medicine when experience trumps
equipoise. Crit Care Med 2013; 41:359.109. Simons FE, Clark S, Camargo CA Jr. Anaphylaxis in the community: learning from the survivors. J Allergy
Clin Immunol 2009; 124:301.110. The Be S.A.F.E. campaign is discussed on the website of the American College of Allergy, Asthma and
Immunology. http://www.acaai.org/allergist/allergies/Anaphylaxis/Pages/safeawarenessanaphylaxis.aspx(Accessed on May 09, 2014).
111. Lieberman P, Decker W, Camargo CA Jr, et al. SAFE: a multidisciplinary approach to anaphylaxiseducation in the emergency department. Ann Allergy Asthma Immunol 2007; 98:519.

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 22/42
112. Simons FE, Edwards ES, Read EJ Jr, et al. Voluntarily reported unintentional injections from epinephrineautoinjectors. J Allergy Clin Immunol 2010; 125:419.
113. The American College of Allergy, Asthma and Immunology. www.acaai.org (Accessed on August 13, 2009).114. The American Academy of Allergy, Asthma and Immunology. www.aaaai.org (Accessed on August 13,
2009).
Topic 392 Version 21.0

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 23/42
GRAPHICS
Diagnostic criteria for anaphylaxis
Anaphylaxis is highly likely when any ONE of the following three criteriais fulfilled:
1. Acute onset of an illness (minutes to several hours) with involvement of the skin,mucosal tissue, or both (eg, generalized hives, pruritus or flushing, swollen lipstongueuvula)
AND AT LEAST ONE OF THE FOLLOWING:
A. Respiratory compromise (eg, dyspnea, wheezebronchospasm, stridor, hypoxemia)
B. Reduced BP* or associated symptoms of endorgan dysfunction (eg, hypotonia, collapse,syncope, incontinence)
2. TWO OR MORE OF THE FOLLOWING that occur rapidly after exposure to a LIKELYallergen for that patient (minutes to several hours):
A. Involvement of the skinmucosal tissue (eg, generalized hives, itchflush, swollen lipstongueuvula)
B. Respiratory compromise (eg, dyspnea, wheezebronchospasm, stridor, hypoxemia)
C. Reduced BP* or associated symptoms (eg, hypotonia, collapse, syncope, incontinence)
D. Persistent gastrointestinal symptoms (eg, crampy abdominal pain, vomiting)
3. Reduced BP* after exposure to a KNOWN allergen for that patient (minutes toseveral hours):
A. Infants and children Low systolic BP (age specific)* or greater than 30 percent decreasein systolic BP
B. Adults Systolic BP of less than 90 mmHg or greater than 30 percent decrease from thatperson's baseline
BP: blood pressure. * Low systolic blood pressure for children is defined as:
Less than 70 mmHg from one month to one year,Less than (70 mmHg + [2 x age]) from 1 to 10 years, andLess than 90 mmHg from 11 to 17 years
Adapted with permission from: Sampson HA, MunozFurlong A, Campbell RL, et al. Second symposium onthe definition and management of anaphylaxis: summary reportSecond National Institute of Allergy andInfectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol 2006;117:391. Copyright © 2006 The American Academy of Allergy, Asthma, and Immunology.
Graphic 72225 Version 11.0
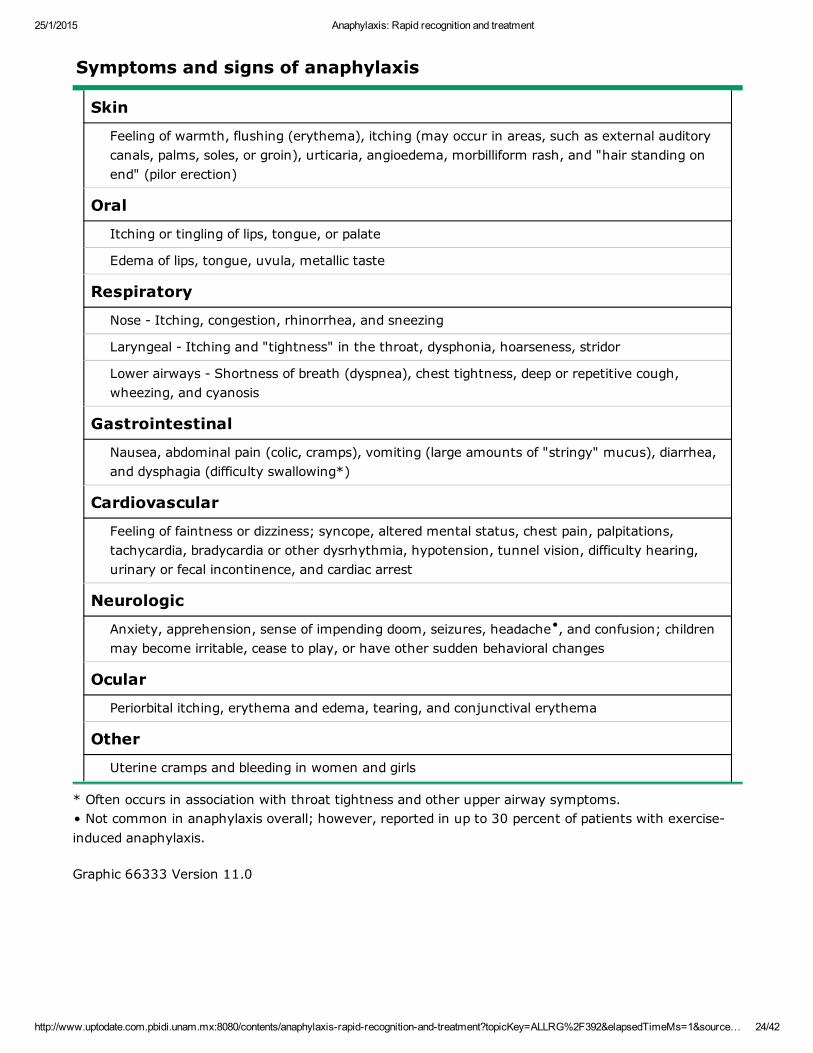
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 24/42
Symptoms and signs of anaphylaxis
Skin
Feeling of warmth, flushing (erythema), itching (may occur in areas, such as external auditorycanals, palms, soles, or groin), urticaria, angioedema, morbilliform rash, and "hair standing onend" (pilor erection)
Oral
Itching or tingling of lips, tongue, or palate
Edema of lips, tongue, uvula, metallic taste
Respiratory
Nose Itching, congestion, rhinorrhea, and sneezing
Laryngeal Itching and "tightness" in the throat, dysphonia, hoarseness, stridor
Lower airways Shortness of breath (dyspnea), chest tightness, deep or repetitive cough,wheezing, and cyanosis
Gastrointestinal
Nausea, abdominal pain (colic, cramps), vomiting (large amounts of "stringy" mucus), diarrhea,and dysphagia (difficulty swallowing*)
Cardiovascular
Feeling of faintness or dizziness; syncope, altered mental status, chest pain, palpitations,tachycardia, bradycardia or other dysrhythmia, hypotension, tunnel vision, difficulty hearing,urinary or fecal incontinence, and cardiac arrest
Neurologic
Anxiety, apprehension, sense of impending doom, seizures, headache , and confusion; childrenmay become irritable, cease to play, or have other sudden behavioral changes
Ocular
Periorbital itching, erythema and edema, tearing, and conjunctival erythema
Other
Uterine cramps and bleeding in women and girls
* Often occurs in association with throat tightness and other upper airway symptoms.• Not common in anaphylaxis overall; however, reported in up to 30 percent of patients with exerciseinduced anaphylaxis.
Graphic 66333 Version 11.0
•
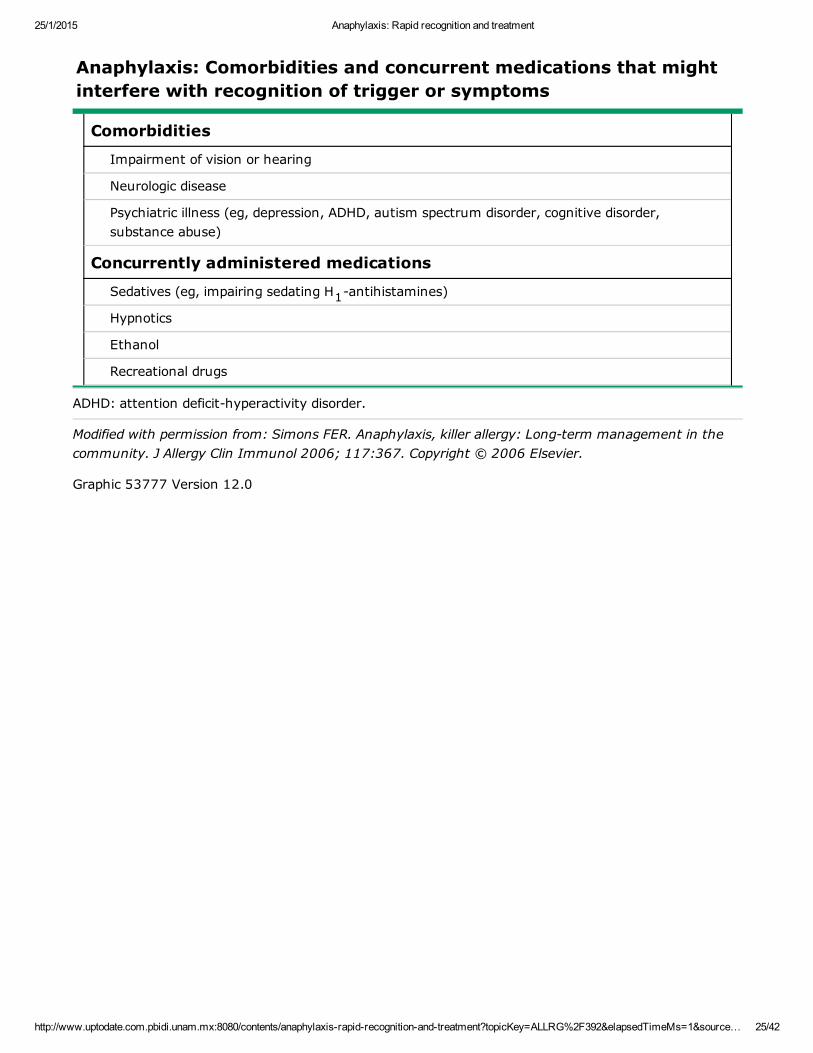
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 25/42
Anaphylaxis: Comorbidities and concurrent medications that mightinterfere with recognition of trigger or symptoms
Comorbidities
Impairment of vision or hearing
Neurologic disease
Psychiatric illness (eg, depression, ADHD, autism spectrum disorder, cognitive disorder,substance abuse)
Concurrently administered medications
Sedatives (eg, impairing sedating H antihistamines)
Hypnotics
Ethanol
Recreational drugs
ADHD: attention deficithyperactivity disorder.
Modified with permission from: Simons FER. Anaphylaxis, killer allergy: Longterm management in thecommunity. J Allergy Clin Immunol 2006; 117:367. Copyright © 2006 Elsevier.
Graphic 53777 Version 12.0
1

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 26/42
Triggers of anaphylaxis
Allergen triggers (IgEdependent immunologic mechanism)
Foods, especially peanut, tree nut, crustacean shellfish, finned fish, milk, egg
Insect stings (eg, hymenoptera venom) and insect bites (eg, kissing bugs, mosquitoes)
Medications (eg, betalactam antibiotics, some NSAIDs)
Biological materials, including allergens, allergen immunotherapy, monoclonal antibodies,vaccines to prevent infectious disease*, and hormones (eg, progesterone)
Natural rubber latex
Food additives, including spices, insectderived colorants (eg, carmine), and vegetable gums
Inhalants (rare) (eg, horse dander, cat dander, grass pollen)
Human seminal fluid (rare trigger of anaphylaxis in women)
Occupational allergens (eg, stinging insects, natural rubber latex)
Immunologic triggers (IgEindependent mechanism)
IgGdependent (rare) (eg, to highmolecular weight dextran, infliximab)
Coagulation system activation (eg, heparin contaminated with oversulfated chondroitin sulfate)
Idiopathic anaphylaxis
Consider the possibility of a hidden or previously unrecognized trigger
Consider the possibility of a mast cell activation syndrome, including systemic mastocytosis
Nonimmunologic triggers (direct activation of mast cells and basophils)
Physical factors (eg, exercise , cold, heat, sunlight/ultraviolet radiation)
Medications (eg, opioids, some NSAIDs)
Alcohol (ethanol) (may augment, rarely induces)
Any food, insect sting or bite, or medication or biological, can potentially trigger anaphylaxis.Novel or unusual allergen triggers include foods, such as vegetables, lupin flour, bird's nestsoup, seal, whale, and kangaroo meats, and storage mitecontaminated flour. They alsoinclude saliva from kissing bugs, mosquitoes, pigeon ticks, green ants, and pharaoh ants, andvenoms from jellyfish, scorpions, and snakes. Medications include taxanes, platins, and otherchemotherapy drugs; biologic agents, including monoclonal antibodies, such as rituximab,cetuximab, infliximab, and uncommonly, omalizumab. Other injectants and ingestants,including Botox, bee products, and herbal formulations are also implicated.Some triggers, such as radiocontrast media, insect venoms, and medications (such asNSAIDs), can act through more than one mechanism.
IgE: immunoglobulin E; NSAIDs: nonsteroidal antiinflammatory drugs; IgG: immunoglobulin G.* Reactions to vaccines are rare and typically involve an excipient such as dextran or gelatin rather thanmicrobial content.•Usually involves a cotrigger, such as a food, medication (eg, an NSAID), or exposure to cold air or water.
Graphic 70667 Version 16.0
•

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 27/42
Comorbidities and concurrent medications that might impact theseverity and treatment of anaphylaxis
Comorbidities
Asthma
Other pulmonary diseases (eg, COPD, interstitial lung disease)
Cardiovascular diseases (eg, ischemic heart disease, hypertensive vascular disease,cardiomyopathy)
Mastocytosis and clonal mast cell disorders
Concurrently administered medications
Betaadrenergic blockers*
Alphaadrenergic blockers
Angiotensinconverting enzyme inhibitors
Angiotensin II receptor blockers
Tricyclic antidepressants
Monoamine oxidase inhibitors
ADHD medications (eg, stimulants such as methylphenidate and amphetamines)
Recreational use of cocaine
COPD: chronic obstructive pulmonary disease; ADHD: attention deficithyperactivity disorder. * Betaadrenergic blockers, administered orally or topically (eg, eye drops) may be associated withsevere anaphylaxis and may also make anaphylaxis more difficult to treat by causing unopposed alphaadrenergic effects, hypertension, and reduced bronchodilator response to the betaadrenergic effects ofendogenous or exogenous epinephrine.• Alphaadrenergic blockers may decrease the effects of endogenous or exogenous epinephrine at alphaadrenergic receptors, potentially making patients less response to the alphaadrenergic effects ofepinephrine. Δ Potential interference with endogenous compensatory responses.◊ Potential increase in adverse effects of epinephrine because of prevention of epinephrine uptake atadrenergic receptors. § Potentiate epinephrine's effects by inhibiting its metabolism by monoamine oxidase. ¥ Side effects are similar to those of epinephrine. ‡ Potentiates epinephrine's effects, especially cardiovascular effects, by preventing its reuptake intoadrenergic neurons.
Modified with permission from: Simons FER. Anaphylaxis, killer allergy: Longterm management in thecommunity. J Allergy Clin Immunol 2006; 117:367. Copyright © 2006 Elsevier.
Graphic 65161 Version 14.0
•
Δ
Δ
◊
§
¥
‡

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 28/42
Instructions for optimal collection and handling of blood samples formeasurement of tryptase and histamine following suspectedanaphylaxis
Tryptase* (serum or plasma)
When to collect the sample:
Blood should be collected between 15 minutes and 3 hours after symptom onset wheneverpossible. Samples collected <15 minutes or >3 hours after symptom onset are less likely to beinformative.
How to collect the sample:
Blood can be drawn using standard technique. Collect blood for serum (red top tube) or plasma(tube with heparin, citrate, or EDTA). A minimum of 1 mL is recommended.
For postmortem samples, collect blood from the femoral artery or vein, not the heart.
How to process the sample:
Serum or plasma should be placed on ice and frozen as soon as possible. Samples should beshipped frozen by overnight courier if the assay cannot be performed on site.
Histamine (plasma)
When to collect the sample:
Plasma for histamine levels should be collected between 5 and 15 minutes after symptomonset. Samples collected <5 minutes or >15 minutes after symptom onset are less likely to beinformative.
How to collect the sample:
Pull blood manually (DO NOT use vacuum tubes) under gentle pressure through a 20 gauge orlarger needle into a syringe containing either citrate or EDTA.
How to process the sample:
Anticoagulated blood should be placed on ice and centrifuged to separate plasma from cells assoon as possible, and then the plasma should be frozen until ready to be analyzed.
The assay for total tryptase is standardized. The assay for histamine is not.
EDTA: ethylenediaminetetraacetic acid.* Normal reference range is similar in adults and in infants, children, and teens ages 6 months to 18years. Komarow HD, Hu Z, Brittain E, et al. Serum tryptase levels in atopic and nonatopic children. JAllergy Clin Immunol 2009; 124:845. The normal reference range is higher in infants less than threemonths. Belhocine W, Ibrahim Z, Grandne V, et al. Total serum tryptase levels are higher in infantsyounger than 3 months of age, particularly in atopic infants. Pediatr Allergy Immunol 2011; 22:600.¶ Plasma is used to avoid the artifactual release of histamine from basophils that can occur during bloodclotting.
Graphic 72041 Version 22.0
¶
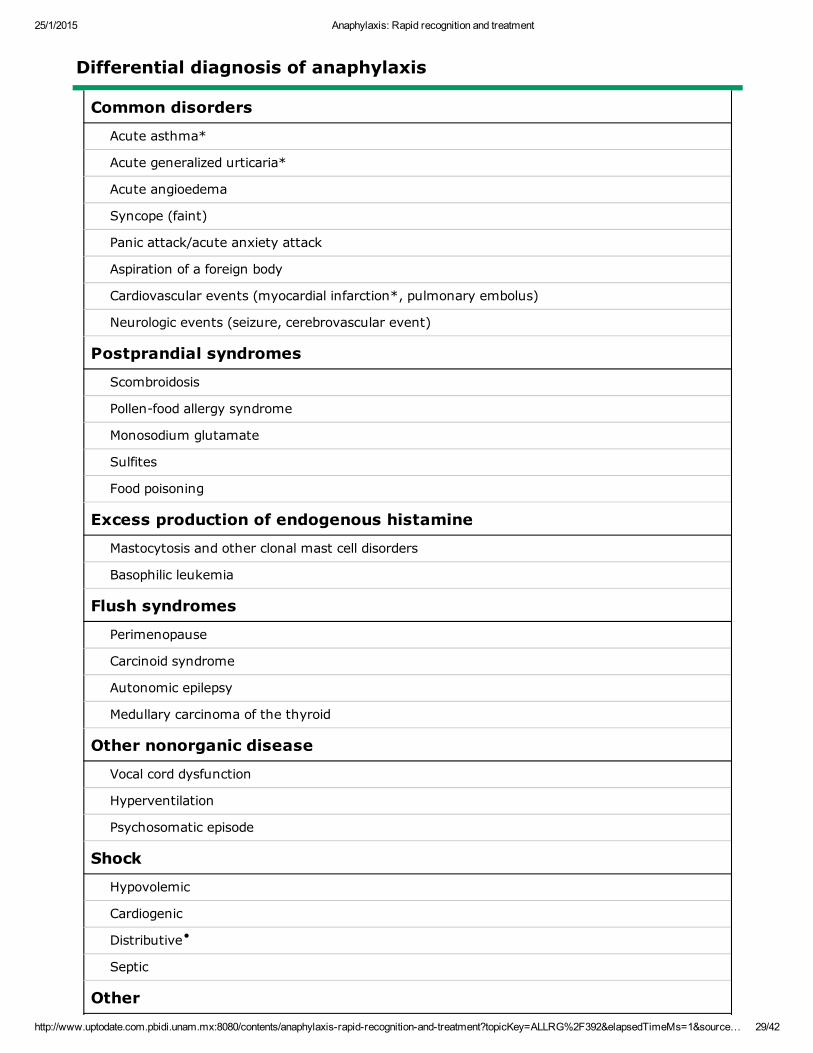
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 29/42
Differential diagnosis of anaphylaxis
Common disorders
Acute asthma*
Acute generalized urticaria*
Acute angioedema
Syncope (faint)
Panic attack/acute anxiety attack
Aspiration of a foreign body
Cardiovascular events (myocardial infarction*, pulmonary embolus)
Neurologic events (seizure, cerebrovascular event)
Postprandial syndromes
Scombroidosis
Pollenfood allergy syndrome
Monosodium glutamate
Sulfites
Food poisoning
Excess production of endogenous histamine
Mastocytosis and other clonal mast cell disorders
Basophilic leukemia
Flush syndromes
Perimenopause
Carcinoid syndrome
Autonomic epilepsy
Medullary carcinoma of the thyroid
Other nonorganic disease
Vocal cord dysfunction
Hyperventilation
Psychosomatic episode
Shock
Hypovolemic
Cardiogenic
Distributive
Septic
Other
•

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 30/42
Nonallergic angioedema (hereditary angioedema types I, II, and III, ACE inhibitorassociatedangioedema)
Systemic capillary leak syndrome
Red man syndrome (vancomycin)
Pheochromocytoma (paradoxical response)
The differential diagnosis in children and adults is shown. In infants, the differential diagnosisof anaphylaxis is unique.
ACE inhibitors: angiotensinconverting enzyme inhibitors. * Acute asthma symptoms, acute generalized urticaria, or myocardial infarction symptoms can alsooccur during an anaphylactic episode.• In anaphylaxis, shock is distributive and hypovolemic. Distributive shock may be due to anaphylaxis orto spinal cord injury.
Graphic 65677 Version 14.0

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 31/42
Rapid overview: Emergent management of anaphylaxis in adults
Diagnosis is made clinically:
The most common signs and symptoms are cutaneous (eg, sudden onset of generalized urticaria,angioedema, flushing, pruritus). However, 10 to 20 percent of patients have no skin findings.
Danger signs: Rapid progression of symptoms, respiratory distress (eg, stridor,wheezing, dyspnea, increased work of breathing, persistent cough, cyanosis),abdominal pain, hypotension, dysrhythmia, chest pain, collapse.
Acute management:
The first and most important treatment in anaphylaxis is epinephrine. There are NO absolutecontraindications to epinephrine in the setting of anaphylaxis.
Airway: Immediate intubation if evidence of impending airway obstruction from angioedema.Delay may lead to complete obstruction. Intubation can be difficult and should be performed by themost experienced clinician available. Cricothyrotomy may be necessary.
Promptly and simultaneously, give:
IM epinephrine (1 mg/mL preparation): Give epinephrine 0.3 to 0.5 mg intramuscularly,preferably in the midouter thigh. Can repeat every 5 to 15 minutes as needed. If epinephrine isinjected promptly IM, most patients respond to one, two, or at most, three doses. If symptomsare not responding to epinephrine injections, prepare IV epinephrine for infusion (see below).
Place patient in recumbent position, if tolerated, and elevate lower extremities.
Oxygen: Give 8 to 10 liters per minute via facemask, or up to 100 percent oxygen as needed.
Normal saline rapid bolus: Treat hypotension with rapid infusion of 1 to 2 liters IV. Repeat asneeded. Massive fluid shifts with severe loss of intravascular volume can occur.
Consider administration of:
Albuterol (salbutamol): For bronchospasm resistant to IM epinephrine, give 2.5 to 5 mg in 3mL saline via nebulizer. Repeat as needed.
H1 antihistamine*: Consider giving diphenhydramine 25 to 50 mg IV (for relief of urticariaand itching only).
H2 antihistamine*: Consider giving ranitidine 50 mg IV.
Glucocorticoid*: Consider giving methylprednisolone 125 mg IV.
Monitoring: Continuous noninvasive hemodynamic monitoring and pulse oximetry monitoringshould be performed. Urine output should be monitored in patients receiving IV fluid resuscitationfor severe hypotension or shock.
Treatment of refractory symptoms:
Epinephrine infusion : For patients with inadequate response to IM epinephrine and IV saline,give epinephrine continuous infusion, 2 to 10 micrograms per minute by infusion pump. Titrate thedose continuously according to blood pressure, cardiac rate and function, and oxygenation.
Vasopressors : Some patients may require a second vasopressor (in addition to epinephrine). Allvasopressors should be given by infusion pump, with the doses titrated continuously according toblood pressure and cardiac rate and function monitored continuously, and oxygenation monitoredby pulse oximetry.
¶
¶

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 32/42
Glucagon: Patients on betablockers may not respond to epinephrine and can be given glucagon 1to 5 mg IV over five minutes, followed by infusion of 5 to 15 micrograms per minute. Rapidadministration of glucagon can cause vomiting.
IM: intramuscular; IV: intravenous.* These medications should not be used as initial or sole treatment.¶ All patients receiving an infusion of epinephrine and another vasopressor require continuousnoninvasive monitoring of blood pressure, heart rate and function, and oxygen saturation.
Adapted from: Simons FER. Anaphylaxis. J Allergy Clin Immunol 2010; 125:S161.
Graphic 58346 Version 20.0

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 33/42
Rapid overview: Emergent management of anaphylaxis in infantsand children*
Diagnosis is made clinically:
The most common signs and symptoms are cutaneous (eg, sudden onset of generalizedurticaria, angioedema, flushing, pruritus). However, 10 to 20 percent of patients have no skinfindings.
Danger signs: Rapid progression of symptoms, evidence of respiratory distress (eg,stridor, wheezing, dyspnea, increased work of breathing, retractions, persistentcough, cyanosis), signs of poor perfusion, abdominal pain, dysrhythmia, hypotension,collapse.
Acute management:
The first and most important therapy in anaphylaxis is epinephrine. There are NO absolutecontraindications to epinephrine in the setting of anaphylaxis.
Airway: Immediate intubation if evidence of impending airway obstruction from angioedema;delay may lead to complete obstruction; intubation can be difficult and should be performed bythe most experienced clinician available; cricothyrotomy may be necessary.
IM epinephrine (1 mg/mL preparation): Epinephrine 0.01 mg per kilogram should beinjected intramuscularly in the midouter thigh. For large children (>50 kilograms), themaximum is 0.5 mg per dose. If there is no response or the response is inadequate, theinjection can be repeated in 5 to 15 minutes. If epinephrine is injected promptly IM, patientsrespond to one, two, or at most, three injections. If signs of poor perfusion are present orsymptoms are not responding to epinephrine injections, prepare IV epinephrine for infusion (seebelow).
Place patient in recumbent position, if tolerated, and elevate lower extremities.
Oxygen: Give 8 to 10 liters per minute via facemask, or up to 100 percent oxygen as needed.
Normal saline rapid bolus: Treat poor perfusion with rapid infusion of 20 mL per kilogram;reevaluate and repeat fluid boluses (20 mL per kilogram) as needed; massive fluid shifts withsevere loss of intravascular volume can occur; monitor urine output.
Albuterol: For bronchospasm resistant to IM epinephrine, give albuterol 0.15 mg per kilogram(minimum dose: 2.5 mg) in 3 mL saline inhaled via nebulizer; repeat as needed.
H1 antihistamine: Consider giving diphenhydramine 1 mg per kilogram (max 40 mg) IV.
H2 antihistamine: Consider giving ranitidine 1 mg per kilogram (max 50 mg) IV.
Glucocorticoid: Consider giving methylprednisolone 1 mg per kilogram (max 125 mg) IV.
Monitoring: Continuous noninvasive hemodynamic monitoring and pulse oximetry monitoringshould be performed; urine output should be monitored in patients receiving IV fluidresuscitation for severe hypotension or shock.
Treatment of refractory symptoms:
Epinephrine infusion : Patients with inadequate response to IM epinephrine and IV saline,give epinephrine continuous infusion at 0.1 to 1 microgram per kilogram per minute, titrated toeffect.
Vasopressors : Patients may require large amounts of IV crystalloid to maintain blood
•
•

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 34/42
pressure; if response to epinephrine and saline is inadequate, dopamine (5 to 20 microgramsper kilogram per minute) can be given with the dose titrated to effect on continuouslymonitored blood pressure, cardiac rate, and function.
IM: intramuscular; IV: intravenous. * A child is defined as a prepubertal patient weighing less than 40 kg.• All patients receiving an infusion of epinephrine and/or another vasopressor require continuousnoninvasive monitoring of blood pressure, heart rate and function, and oxygen saturation. We suggestthat pediatric centers provide instructions for preparation of standard concentrations and also providecharts for established infusion rate for epinephrine and other vasopressors in infants and children.
Graphic 74242 Version 22.0

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 35/42
Beneficial effects and adverse effects of epinephrine in thetreatment of anaphylaxis
Beneficial effects
At alpha1 receptor:
Increased vasoconstriction (at low doses)
Increased peripheral vascular resistance
Increased blood pressure
Decreased mucosal edema (eg, in larynx)
At beta1 receptor:
Increased heart rate (chronotropy)
Increased force of cardiac contraction (inotropy)
At beta2 receptor:
Decreased mediator release from mast cells and basophils
Increased bronchodilation
Increased vasodilation
Adverse effects*
Common andtransient
Anxiety, palpitations, pallor, tremor, fear, restlessness, dizziness,headache
Uncommon(typically occur afteroverdose)
Ventricular arrhythmias, angina, myocardial infarction, pulmonaryedema, sudden sharp increase in blood pressure, intracranial hemorrhage
* Risk of adverse effects may be increased in the following conditions: Use of tricyclic antidepressants, monoamine oxidase inhibitors, or cocaine. Some preexisting cardiovascular, central nervous system, or thyroid diseases. Examples includeintracranial surgery, acute aneurysm, or untreated hyperthyroidism.• Serious adverse effects such as those listed in the table potentially occur when epinephrine is given inoverdose by any route, most commonly after an intravenous bolus injection, an overly rapid intravenousinfusion, or an erroneous intravenous injection of a 1 mg/mL (1:1000) epinephrine solution instead ofan appropriately diluted 0.1 mg/mL (1:10,000) or a 0.01 mg/mL epinephrine solution. Δ Anaphylaxis can present as an acute coronary syndrome (ACS), arrhythmias, myocardial infarction, orangina, before or in the absence of epinephrine injection. This potentially occurs in patients with knowncoronary artery disease, patients in whom subclinical coronary artery disease is unmasked, and patients(including children) with transient coronary artery vasospasm in whom no cardiovascular abnormalitiescan be detected by electrocardiogram or echocardiography after recovery from anaphylaxis.
Graphic 65684 Version 10.0
•Δ

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 36/42
Example of epinephrine infusion Adult
Example of preparation of epinephrine infusion for refractory symptomsof anaphylaxis (adult patient) for emergency/critical care units
Epinephrine 4 micrograms/mL (0.004 mg/mL)
Add 1 mg (1000 micrograms) of epinephrine to 250 mL of 5 percent dextrose water(D5W).
Resulting concentration is 4 micrograms per milliliter (mL).
Preparation
1. CHECK vial strength.
2. To prepare epinephrine infusion for a final concentration of 4 micrograms per mL, dilute 10mL of 0.1 mg/mL epinephrine (also labeled 1:10,000) OR 1 mL of 1 mg/mL epinephrine (alsolabeled 1:1000) in 250 mL of D5W.*
Administration
Infuse an initial dose of 2 to 10 micrograms per minute using a programmable infusion pumpand titrate as needed while continuously monitoring the patient's cardiac rhythm and bloodpressure.
Adult dose
Administration rate
1 milligram epinephrine diluted in 250 mL D5W
4 micrograms per milliliter
Micrograms per minute mL per minute mL per hour
1 0.25 15
2 0.5 30
3 0.75 45
4 1 60
5 1.25 75
6 1.5 90
7 1.75 105
8 2 120
9 2.25 135
10 2.5 150
11 2.75 165
12 3 180
13 3.25 195
14 3.5 210
15 3.75 225
16 4 240
To reduce the risk of making a medication error, we suggest that centers have available an
Δ

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 37/42
institutionally approved protocol for epinephrine infusion that includes steps on how to prepareand administer the infusion and standard concentration(s).The above table is provided as an example. There are other acceptable concentrations.
Intravenous epinephrine, like all vasopressors, can cause lifethreateninghypertension, cardiac ischemia, and ventricular arrhythmias. It should beadministered ONLY by clinicians trained and experienced in dose titration ofintravenous epinephrine using continuous noninvasive electronic monitoring ofheart rate and blood pressure.Epinephrine is an ischemia causing agent and vesicant. Monitor infusion site for extravasation.See Lexicomp drug reference for information on managing extravasation including infiltration ofphentolamine. Central line administration is preferred when available.
* Unused diluted solutions should be discarded within 24 hours or less of preparation depending on localstandards. Δ To calculate the adult dose based on body weight, initial dose range is 0.03 micrograms/kg of bodyweight per minute to up to 0.14 micrograms/kg of body weight per minute.
References:1. Gahart BL, Nazareno AR. Intravenous Medications 31st ed. ElsevierMosby © 2014 St. Louis, MO.2. Lieberman P, et al. J Allergy Clin Immunol 2010; 126(3):477.
Graphic 75682 Version 7.0

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 38/42
Example of epinephrine infusion Pediatric 10 kg
Example of preparation of epinephrine infusion for refractory symptomsof anaphylaxis for pediatric patient of 10 kg body weight for
emergency/critical care units
Epinephrine 10 micrograms/mL (0.01 mg/mL)
Add 1 mg (1000 micrograms) of epinephrine to 100 mL of 5 percent dextrose water(D5W).
Resulting concentration is 10 micrograms per milliliter (mL).
Preparation
1. CHECK vial strength.
2. To prepare epinephrine infusion for a final concentration of 10 micrograms per mL, dilute 10mL of 0.1 mg/mL epinephrine (also labeled 1:10,000) in 100 mL of D5W OR 1 mL of 1mg/mL epinephrine (also labeled 1:1000) in 100 mL of D5W.*
Administration
Infuse an initial dose of 0.1 micrograms per kg per minute using a programmable infusion pumpand titrate as needed while continuously monitoring the patient's cardiac rhythm and bloodpressure.
Pediatric dose for 10 kg child
Administration rate
1 milligram epinephrine diluted in 100 mLD5W
10 micrograms per milliliter
Microgramsper kg perminute
Multiply bypatientweight(10 kg)
Microgramsper minute
mL perminute for 10kg child
Multiply by 60minutes
mL per hourfor 10 kgchild
0.05 0.5 0.05 3
0.1 1 0.1 6
0.2 2 0.2 12
0.3 3 0.3 18
0.4 4 0.4 24
0.5 5 0.5 30
0.6 6 0.6 36
0.7 7 0.7 42
0.8 8 0.8 48
0.9 9 0.9 54
1 10 1 60
To reduce the risk of making a medication error, we suggest that centers have available aninstitutionally approved protocol for epinephrine infusion that includes steps on how to prepareand administer the infusion and standard concentration(s).The above table is provided as an example; there are other acceptable concentrations.

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 39/42
Intravenous epinephrine, like all vasopressors, can cause lifethreateninghypertension, cardiac ischemia, and ventricular arrhythmias. It should beadministered ONLY by clinicians trained and experienced in dose titration ofintravenous epinephrine using continuous noninvasive electronic monitoring ofheart rate and blood pressure.Epinephrine is an ischemia causing agent and vesicant. Monitor infusion site for extravasation.See Lexicomp drug reference for information on managing extravasation including infiltration ofphentolamine. Central line administration is preferred when available.
* Unused diluted solutions should be discarded within 24 hours or less of preparation depending on localstandards.
References:1. Gahart BL, Nazareno AR. Intravenous Medications 31st ed. ElsevierMosby © 2014 St. Louis, MO.2. Lieberman P, et al. J Allergy Clin Immunol 2010; 126(3):477.
Graphic 56049 Version 7.0
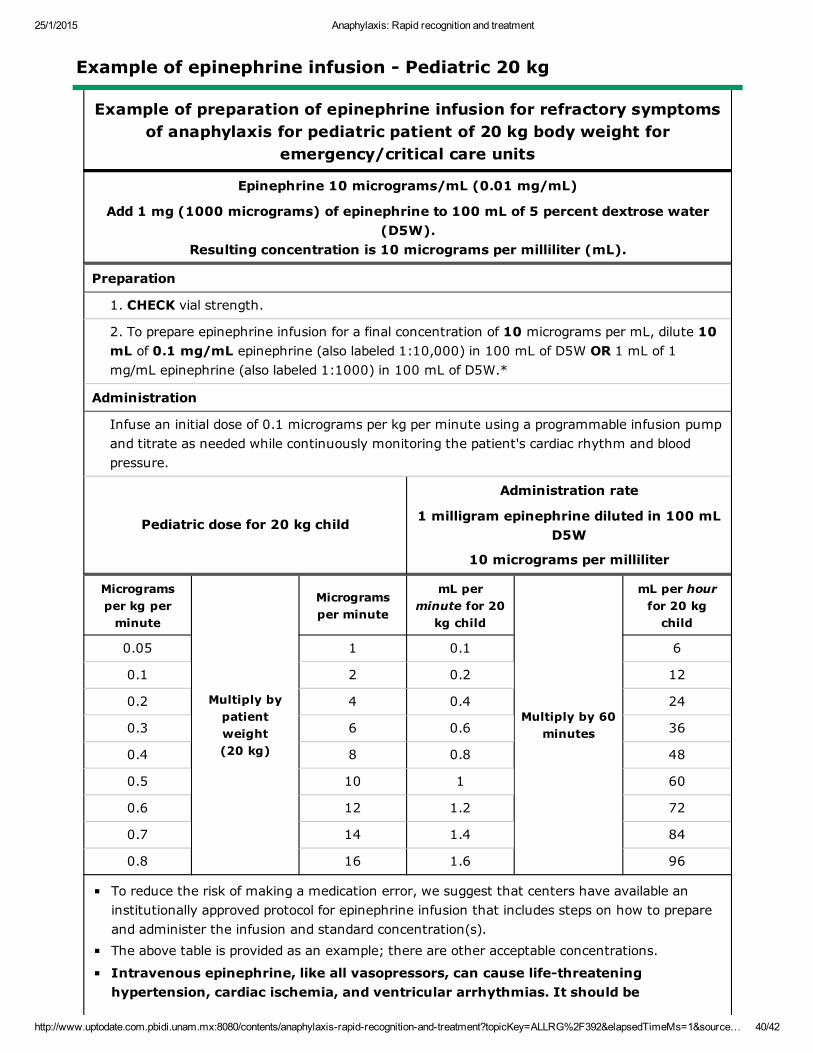
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 40/42
Example of epinephrine infusion Pediatric 20 kg
Example of preparation of epinephrine infusion for refractory symptomsof anaphylaxis for pediatric patient of 20 kg body weight for
emergency/critical care units
Epinephrine 10 micrograms/mL (0.01 mg/mL)
Add 1 mg (1000 micrograms) of epinephrine to 100 mL of 5 percent dextrose water(D5W).
Resulting concentration is 10 micrograms per milliliter (mL).
Preparation
1. CHECK vial strength.
2. To prepare epinephrine infusion for a final concentration of 10 micrograms per mL, dilute 10mL of 0.1 mg/mL epinephrine (also labeled 1:10,000) in 100 mL of D5W OR 1 mL of 1mg/mL epinephrine (also labeled 1:1000) in 100 mL of D5W.*
Administration
Infuse an initial dose of 0.1 micrograms per kg per minute using a programmable infusion pumpand titrate as needed while continuously monitoring the patient's cardiac rhythm and bloodpressure.
Pediatric dose for 20 kg child
Administration rate
1 milligram epinephrine diluted in 100 mLD5W
10 micrograms per milliliter
Microgramsper kg perminute
Multiply bypatientweight(20 kg)
Microgramsper minute
mL perminute for 20kg child
Multiply by 60minutes
mL per hourfor 20 kgchild
0.05 1 0.1 6
0.1 2 0.2 12
0.2 4 0.4 24
0.3 6 0.6 36
0.4 8 0.8 48
0.5 10 1 60
0.6 12 1.2 72
0.7 14 1.4 84
0.8 16 1.6 96
To reduce the risk of making a medication error, we suggest that centers have available aninstitutionally approved protocol for epinephrine infusion that includes steps on how to prepareand administer the infusion and standard concentration(s).The above table is provided as an example; there are other acceptable concentrations.
Intravenous epinephrine, like all vasopressors, can cause lifethreateninghypertension, cardiac ischemia, and ventricular arrhythmias. It should be
25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 41/42
administered ONLY by clinicians trained and experienced in dose titration ofintravenous epinephrine using continuous noninvasive electronic monitoring ofheart rate and blood pressure.Epinephrine is an ischemia causing agent and vesicant. Monitor infusion site for extravasation.See Lexicomp drug reference for information on managing extravasation including infiltration ofphentolamine. Central line administration is preferred when available.
* Unused diluted solutions should be discarded within 24 hours or less of preparation depending on localstandards.
References:1. Gahart BL, Nazareno AR. Intravenous Medications 31st ed. ElsevierMosby © 2014 St. Louis, MO.2. Lieberman P, et al. J Allergy Clin Immunol 2010; 126(3):477.
Graphic 66791 Version 8.0

25/1/2015 Anaphylaxis: Rapid recognition and treatment
http://www.uptodate.com.pbidi.unam.mx:8080/contents/anaphylaxisrapidrecognitionandtreatment?topicKey=ALLRG%2F392&elapsedTimeMs=1&source… 42/42
Disclosures: F Estelle R Simons, MD, FRCPC Consultant/Advisory Boards: Sanofi Canada[Anaphylaxis]. Carlos A Camargo, Jr, MD, DrPH Grant/Research/Clinical Trial Support: GSK; Novartis[asthma]. Consultant/Advisory Boards: GSK; Merck; Novartis; Teva [asthma]. Bruce S Bochner, MDGrant/Research/Clinical Trial Support: NIAID; NHLBI; GSK [Siglec8, Siglec9, asthma, COPD,anaphylaxis, imaging; eosinophilic granulomatosis with polyangiitis (Mepolizumab)]. Consultant/AdvisoryBoards: TEVA; Sanofi; Merck; Glycomimetics; Allakos; Biogen Idec; Svelte Medical Systems. PatentHolder: Siglec8 and its ligand; antiSiglec8 antibodies [held by Johns Hopkins University]. Employment:Northwestern University Feinberg School of Medicine. Equity Ownership/Stock Options: Glycomimetics;Allakos. Other Financial Interest: Elsevier [publication royalties]. Anna M Feldweg, MD Employee ofUpToDate, Inc.Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these areaddressed by vetting through a multilevel review process, and through requirements for references to beprovided to support the content. Appropriately referenced content is required of all authors and mustconform to UpToDate standards of evidence.Conflict of interest policy
Disclosures