an introduction to laboratory tests
DESCRIPTION
AN INTRODUCTION TO LABORATORY TESTS. AN INTRODUCTION TO LABORATORY TESTS. Aim - introduction to laboratory tests of clinical and diagnostic importance - biochemistry and haematology Use? Assist doctor in making a diagnosis and monitoring treatment - PowerPoint PPT PresentationTRANSCRIPT
AN INTRODUCTION TO AN INTRODUCTION TO LABORATORY TESTSLABORATORY TESTS
AN INTRODUCTION TO AN INTRODUCTION TO LABORATORY TESTSLABORATORY TESTS
Aim - introduction to laboratory tests of clinical and diagnostic Aim - introduction to laboratory tests of clinical and diagnostic importance - biochemistry and haematologyimportance - biochemistry and haematology
Use?Use? Assist doctor in making a diagnosis and monitoring Assist doctor in making a diagnosis and monitoring
treatmenttreatment Assist pharmacist in assessing and monitoring drug Assist pharmacist in assessing and monitoring drug
treatmenttreatment
Individual tests may provide insufficient information - consider Individual tests may provide insufficient information - consider
pattern of testspattern of tests within a groupwithin a group Single tests are of less value than a series - show trendsSingle tests are of less value than a series - show trends Expressed as a reference range - based on the assumption that Expressed as a reference range - based on the assumption that
95% of the population are normal95% of the population are normal
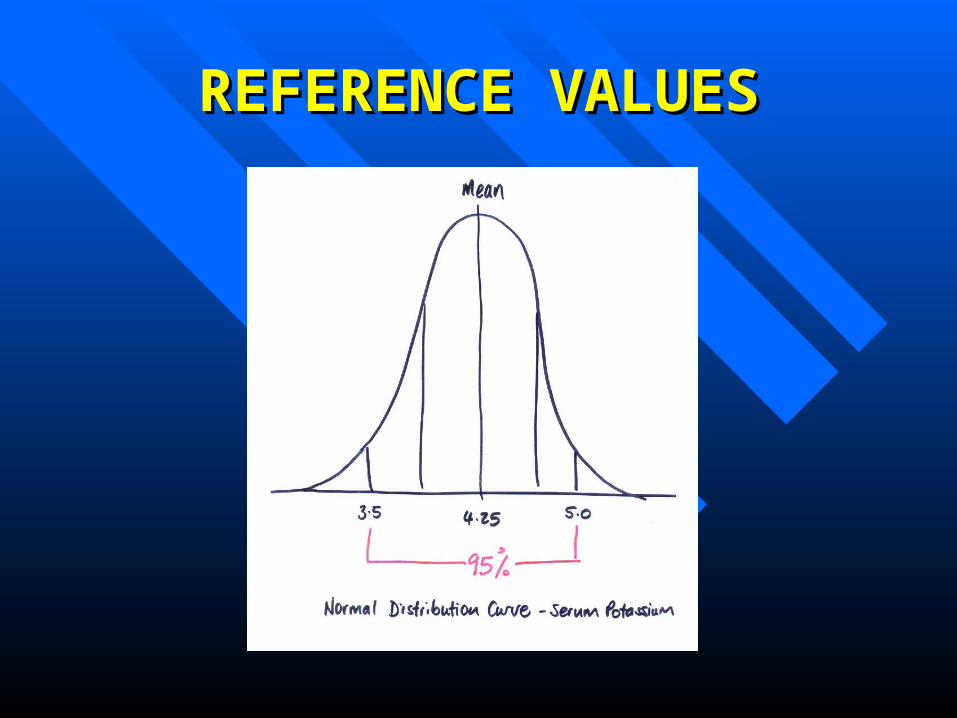
REFERENCE VALUESREFERENCE VALUES
1. RENAL FUNCTION TESTS1. RENAL FUNCTION TESTS
Serum Creatinine, Creatinine Clearance, Serum Creatinine, Creatinine Clearance, UreaUrea– Used to give an estimate of glomerular filtration Used to give an estimate of glomerular filtration
rate (GFR)rate (GFR)– GFR gives an indication of the efficiency of the GFR gives an indication of the efficiency of the
kidney and is decreased in renal impairmentkidney and is decreased in renal impairment– In practice, this is crucial information to determine In practice, this is crucial information to determine
drug handling. Renally cleared drugs and drug handling. Renally cleared drugs and metabolites will accumulate in renal impairmentmetabolites will accumulate in renal impairment
– Some drugs may reduce GFR e.g. NSAIDs and Some drugs may reduce GFR e.g. NSAIDs and aminoglycosidesaminoglycosides
1. RENAL FUNCTION TESTS1. RENAL FUNCTION TESTS
Serum CreatinineSerum Creatinine (Cr)(Cr)– Reference range 80 -150 micromoles/LReference range 80 -150 micromoles/L– Creatinine is a major metabolite of creatine phosphate, Creatinine is a major metabolite of creatine phosphate,
a major constituent of muscle.a major constituent of muscle.– Excreted almost exclusively by glomerular filtration – Excreted almost exclusively by glomerular filtration –
freely filtered.freely filtered.– GFR results in creatinineGFR results in creatinine
Creatinine ClearanceCreatinine Clearance (CrCl) (CrCl)– Renal impairment if< 50ml/min Renal impairment if< 50ml/min – Serum creatinine can be used in the Serum creatinine can be used in the
Cockroft-Gault equation to estimate creatinine Cockroft-Gault equation to estimate creatinine clearance. GFR approximates to CrClclearance. GFR approximates to CrCl
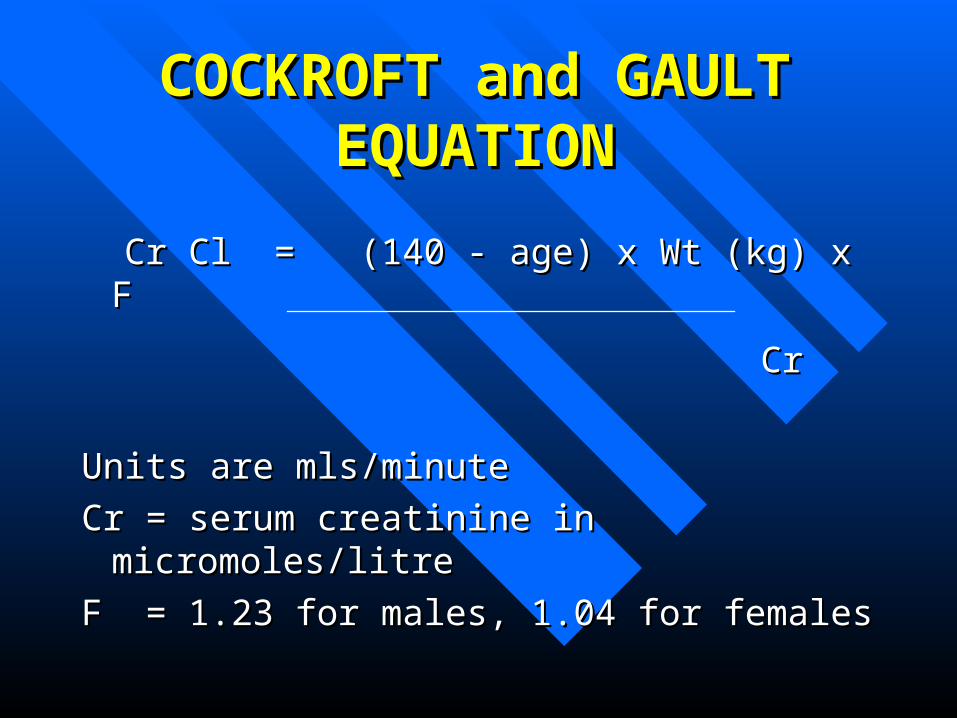
COCKROFT and GAULT COCKROFT and GAULT EQUATIONEQUATION
Cr Cl = (140 - age) x Wt (kg) x FCr Cl = (140 - age) x Wt (kg) x F
CrCr
Units are mls/minuteUnits are mls/minute
Cr = serum creatinine in micromoles/litreCr = serum creatinine in micromoles/litre
F = 1.23 for males, 1.04 for femalesF = 1.23 for males, 1.04 for females
1. RENAL FUNCTION TESTS1. RENAL FUNCTION TESTS
UreaUrea (4.2-6.4mmol/L) (4.2-6.4mmol/L)– Also known as blood urea nitrogen, BUN.Also known as blood urea nitrogen, BUN.– Used to estimate renal function, but poor Used to estimate renal function, but poor
measure of minor degrees of renal measure of minor degrees of renal impairment as it is influenced by other impairment as it is influenced by other factors.factors.
– End product of protein metabolism. (High End product of protein metabolism. (High protein diet increases urea)protein diet increases urea)
– Usually measured as urea and electrolytes Usually measured as urea and electrolytes (U&Es)(U&Es)

1. RENAL FUNCTION TESTS1. RENAL FUNCTION TESTS
HIGH SERUM CREATININE HIGH SERUM CREATININE
signifiessignifies
GFRGFR Renal impairmentRenal impairment

RENAL IMPAIRMENTRENAL IMPAIRMENT
Renal impairment is arbitrarily divided into 3 grades ( see BNF) Renal impairment is arbitrarily divided into 3 grades ( see BNF) Glomerular Filtration rate, measured by creatinine clearance Glomerular Filtration rate, measured by creatinine clearance Note - definitions vary. Consult product literature for specific Note - definitions vary. Consult product literature for specific
drugsdrugs
GradeGrade GFRGFR(Creatinine Clearance)(Creatinine Clearance)
ml/minml/min
SerumSerum
CreatinineCreatininemicromoles/Lmicromoles/L
MildMild 20-5020-50 150-300150-300
ModerateModerate 10-2010-20 300-700300-700
SevereSevere <10<10 >700>700
2. ELECTROLYTES2. ELECTROLYTES
Sodium, potassium, calcium, phosphate,Sodium, potassium, calcium, phosphate,glucoseglucose
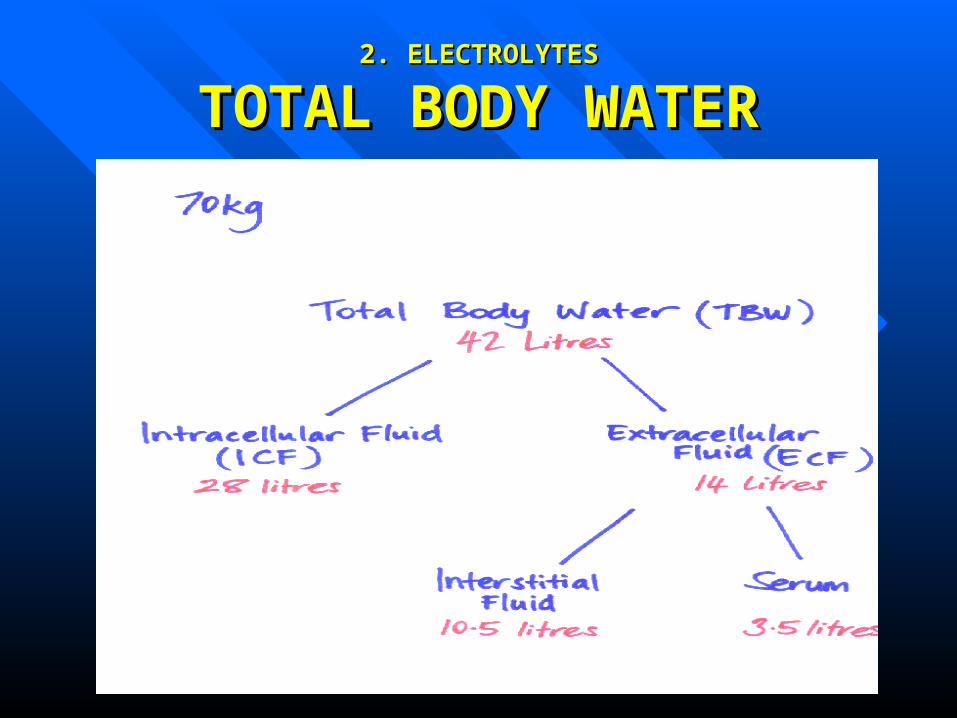
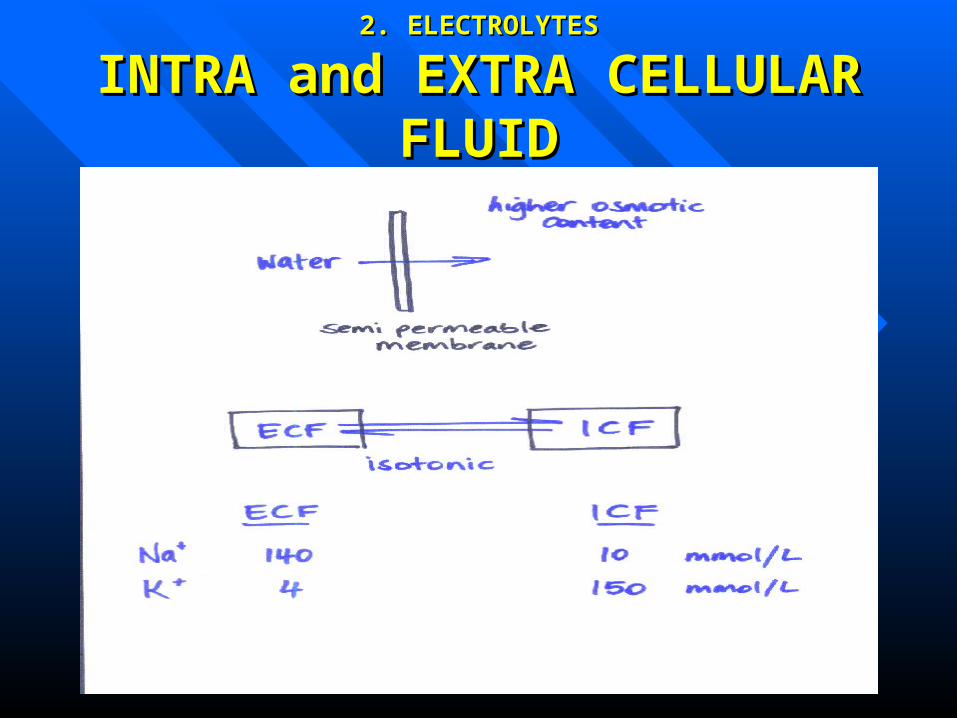
SodiumSodium– Main extracellular cation. Osmolality of ECF is Main extracellular cation. Osmolality of ECF is
largely determined by sodium and associated anionslargely determined by sodium and associated anions– Intimately linked with distribution of water between Intimately linked with distribution of water between
intra and extracellular compartments (ICF and ECF). intra and extracellular compartments (ICF and ECF). Reflects fluid status of patientReflects fluid status of patient
– Changes in body sodium content result in changes Changes in body sodium content result in changes in ECF volumein ECF volume
– Reference value 133-144mmol/LReference value 133-144mmol/L
2. ELECTROLYTES2. ELECTROLYTES
TOTAL BODY WATERTOTAL BODY WATER
2. ELECTROLYTES2. ELECTROLYTES
INTRA and EXTRA CELLULAR INTRA and EXTRA CELLULAR FLUIDFLUID
2. ELECTROLYTES2. ELECTROLYTES
HyponatraemiaHyponatraemia Indicates an increase in free water in Indicates an increase in free water in
ECFECF Caused byCaused by
– Sodium (and water) loss e.g.diureticsSodium (and water) loss e.g.diuretics– Water retention in excess of sodium e.g. Water retention in excess of sodium e.g.
carbamazepine, tricylclicscarbamazepine, tricylclics– Symptoms if Na<120mmol/L – headache, Symptoms if Na<120mmol/L – headache,
nausea, cramps, confusion nausea, cramps, confusion
2. ELECTROLYTES2. ELECTROLYTES
HypernatraemiaHypernatraemia Indicates a loss of free water and an increase Indicates a loss of free water and an increase
in sodiumin sodium Caused byCaused by
– Excessive water loss, or combined loss of water Excessive water loss, or combined loss of water and sodium with predominant water loss e.g. and sodium with predominant water loss e.g. diarrhoea in infantsdiarrhoea in infants
– Unlikely to be caused by sodium excess - thirst Unlikely to be caused by sodium excess - thirst compensatescompensates
Symptoms at Na>160mmol/L - thirst, mental Symptoms at Na>160mmol/L - thirst, mental confusion comaconfusion coma
2. ELECTROLYTES2. ELECTROLYTES PotassiumPotassium
– Principal intracellular cation (<2-3% in Principal intracellular cation (<2-3% in ECF)ECF)
– Involved in muscle excitation and cardiac Involved in muscle excitation and cardiac function. Body sensitive to changes in function. Body sensitive to changes in serum potassium.serum potassium.
– Reference values 3.5 - 5 mmol/LReference values 3.5 - 5 mmol/L– Hypo - reduced muscle activity, Hypo - reduced muscle activity,
arrhythmias, mental slowing.arrhythmias, mental slowing.– Hyper - ventricular fibrillation and cardiac Hyper - ventricular fibrillation and cardiac
arrest.arrest.

2. ELECTROLYTES2. ELECTROLYTES
HypokalaemiaHypokalaemia Decreased potassiumDecreased potassium Serious at <2.5mmol/LSerious at <2.5mmol/L
(reference range 3.5-5)(reference range 3.5-5) Caused byCaused by
– Diuretics (loop and thiazide)Diuretics (loop and thiazide)– Loss from GI tract (diarrhoea, vomiting)Loss from GI tract (diarrhoea, vomiting)– Shift into cells (insulin, salbutamol)Shift into cells (insulin, salbutamol)
2. ELECTROLYTES2. ELECTROLYTES
HyperkalaemiaHyperkalaemia Increased potassiumIncreased potassium Serious at >6.5 mmol/LSerious at >6.5 mmol/L
(reference range 3.5-5)(reference range 3.5-5) Caused byCaused by
– Potassium sparing diureticsPotassium sparing diuretics– Acute renal failureAcute renal failure– Catabolic states e.g. diabetic ketoacidosisCatabolic states e.g. diabetic ketoacidosis– Vast intracellular damage – cell lysis, release of KVast intracellular damage – cell lysis, release of K
3. LIVER FUNCTION TESTS3. LIVER FUNCTION TESTS
No specific test to determine degree of No specific test to determine degree of liver impairmentliver impairment
Important to look for a pattern using the Important to look for a pattern using the following testsfollowing tests– ALPALP– AST and ALTAST and ALT– GGTGGT– BilirubinBilirubin
3. LIVER FUNCTION TESTS3. LIVER FUNCTION TESTS
Alkaline Phosphatase (ALP)Alkaline Phosphatase (ALP)– Found in cells lining the bile duct – rise usually signifies Found in cells lining the bile duct – rise usually signifies
cholestasis [c] (obstruction to flow in bile duct)cholestasis [c] (obstruction to flow in bile duct) Aspartate aminotransferase (AST)Aspartate aminotransferase (AST) and and Alanine aminotransferase (ALT)Alanine aminotransferase (ALT)
– Found in hepatocytes – rise usually signifies Found in hepatocytes – rise usually signifies hepatocellular damage [h]hepatocellular damage [h]
Gamma-glutamyl transferase (GGT)Gamma-glutamyl transferase (GGT)– Synthesis of the enzyme induced by alcohol and drugs. Synthesis of the enzyme induced by alcohol and drugs.
Rise usually signifies hepatobiliary disease [hb]Rise usually signifies hepatobiliary disease [hb]
3. LIVER FUNCTION TESTS3. LIVER FUNCTION TESTS BilirubinBilirubin
Breakdown product of haemoglobin Breakdown product of haemoglobin
Rise in Rise in UNCONJUGATEDUNCONJUGATED form usually signifies form usually signifies» haemolysis (increased RBC destruction), or haemolysis (increased RBC destruction), or » direct hepatocellualr damage.direct hepatocellualr damage.
Rise in Rise in CONGUGATEDCONGUGATED form usually signifies form usually signifies» cholestasis - obstruction to bile flow cholestasis - obstruction to bile flow
A rise in both A rise in both CONJUGATED & UNCONJUGATEDCONJUGATED & UNCONJUGATED bilirubin suggests bilirubin suggests » mixed hepatocellular damage and cholestasis.mixed hepatocellular damage and cholestasis.
Changes in LFTs may be due to disease process Changes in LFTs may be due to disease process (e.g. gallstones, hepatitis) or due to drugs (e.g. gallstones, hepatitis) or due to drugs (e.g. chlorpromazine [h,c], flucloxacillin [c]).(e.g. chlorpromazine [h,c], flucloxacillin [c]).
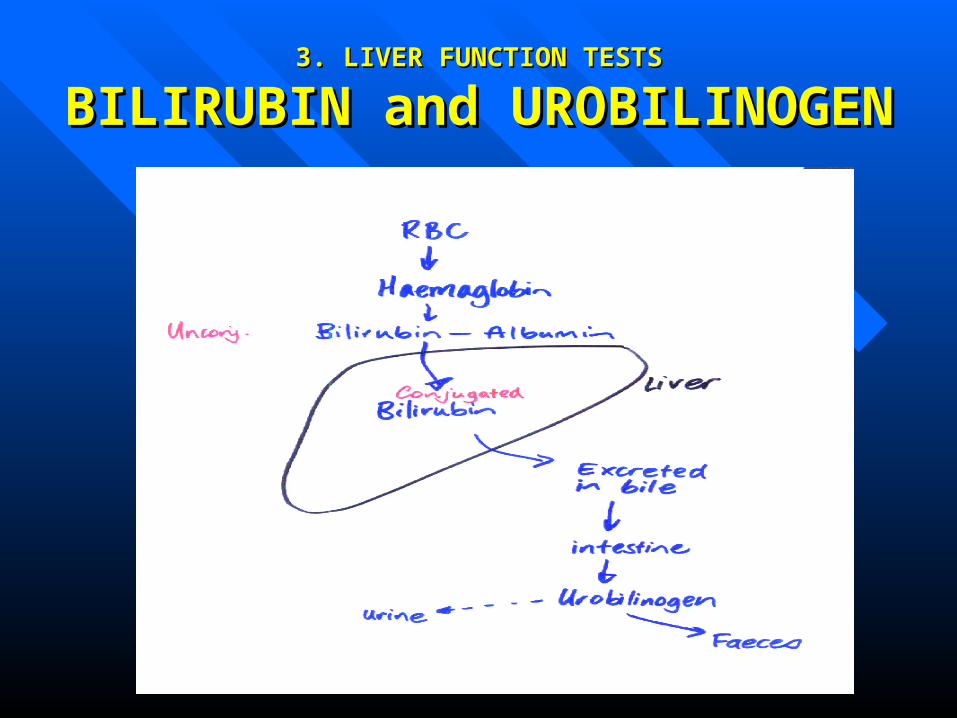
3. LIVER FUNCTION TESTS3. LIVER FUNCTION TESTS
BILIRUBIN and UROBILINOGENBILIRUBIN and UROBILINOGEN