an integrative research review: effective school-based childhood overweight interventions
TRANSCRIPT

166 JSPN Vol. 11, No. 3, July, 2006
Accepted for publication January 31, 2006.
Blackwell Publishing, Ltd.Oxford, UKJSPNJournal for Specialists in Pediatric Nursing1539-0136© 2006 Blackwell Publishing, Inc.July 2006113
ORIGINAL ARTICLE
An Integrative Research Review: Effective School-Based Childhood Overweight Interventions
An Integrative Research Review: Effective School-Based Childhood Overweight Interventions
Kristen Cole, Julee Waldrop, Jennifer D’Auria, and Heather Garner
PURPOSE.
To describe theoretical and
methodological characteristics of effective school-
based interventions that used healthy lifestyle
education, dietary habits, and/or physical activity
in children ages 4 to 14.
DESIGN.
Integrative research review.
METHODS.
Stetler’s model of research utilization.
RESULTS.
Social Cognitive Theory was the stated
or implied theory in eight of the 10 studies.
Healthy lifestyle education was initiated in nine
studies, dietary habits in four, and physical activity
in eight. Four of the 10 studies used a combination of
all three interventions; three used a combination of
two interventions; and three used only one intervention.
PRACTICE IMPLICATIONS.
Social Cognitive Theory
and the role of social learning are useful when
designing interventions for preventing and
treating childhood overweight.
Search terms:
BMI, childhood overweight, food
habits, nutrition education, physical activity,
school-based programs, social cognitive theory
Kristen Cole, RN, MS, PNP, is a primary care provider, Village Pediatrics of Chapel Hill, Chapel Hill, NC; Julee Waldrop, RN, MS, FNP, PNP, is a Clinical Associate Professor, School of Nursing and School of Medicine, University of North Carolina Chapel Hill; Jennifer D’Auria, RN, PhD, PNP, is Associate Professor, School of Nursing, University of North Carolina Chapel Hill, Chapel Hill, NC; and Heather Garner, RN, MS, PNP, is a primary care provider, Forsyth Pediatrics, Kernersville, NC.
Accepted for publication January 31, 2006.
Introduction
Childhood overweight has become a major publichealth concern in the United States. The prevalence ofchildhood overweight is increasing at such a dramaticrate throughout the country that it has been describedas a pandemic (Kimm & Obarzenek, 2002). The NationalHealth and Nutrition Examination Survey (NHANES)data from 1999 to 2002, which includes all U.S. race andethnic groups, indicates that 31% of children ages 6–19years are either overweight with a body mass index(BMI) greater than the 95th percentile of the referencepopulation or at risk for overweight with a BMIbetween the 85th and 95th percentiles (U.S. Departmentof Health and Human Services [USDHHS], 2004a).Compared to the 1965–1970 NHANES II data, thenumber of overweight children has nearly quadrupledin the last three to four decades (Hedley et al., 2004).Furthermore, findings from the 2001–2002 NHANESreport indicate that the incidence of overweightchildren continues to be on the rise (USDHHS, 2004a).
Overweight places youth at a much higher risk fordeveloping type 2 diabetes, obstructive sleep apnea,orthopedic complications, renal disease, and metabolicsyndrome (Amschler, 2002; Sabin, Crowne, & Shield,2002). Overweight children also have a greater riskof developing cardiovascular diseases, such ashypercholesterolemia, hypertension, and hyperlipi-demia (Freeman, Dietz, Srinivasan, & Berenson,1999). Furthermore, Morgan et al. (2002) demonstratedthat being overweight has a negative impact on

JSPN Vol. 11, No. 3, July, 2006 167
children’s psychological state, which is often reflectedin body dissatisfaction and binge-eating behaviors.Considering the increasing prevalence and negativehealth consequences associated with childhood over-weight, healthcare providers urgently need to focus onproviding and supporting prevention and treatmentprograms to address this problem.
The nursing profession has been highly influencedby theoretical frameworks that are used as practicemodels to guide nursing assessment, diagnosis, andintervention (Friedman, Bowden, & Jones, 2003). Nursesalso have a unique opportunity to use the nursing modelof health promotion and disease prevention to helpreverse the current trend of increasing incidence ofchildhood overweight. Nurses can encourage healthylifestyle habits early in childhood and promote appro-priate theoretical approaches and interventive strate-gies specific to the pediatric population.
Purpose
The purpose of this paper is to describe the theoreticaland methodological characteristics of effectiveschool-based interventions that used healthy lifestyleeducation, dietary habits, and/or physical activityinterventions. This review will provide valuableinformation for the practicing clinician about promis-ing theoretical and implementation approaches thathave been used in studies demonstrating weight lossor BMI reduction outcomes for children 4–14 years ofage.
Background
While childhood overweight and the importance ofdiet and exercise are often discussed as treatment withinboth medical and public circles, it is essential thatevidence-based practice and theoretical frameworksguide nursing education and research in childhoodoverweight. The purpose of theories used in theprofession of nursing is to identify, explain, or predictevents and outcomes present in the discipline of
nursing (Friedman et al., 2003). Theories and frameworksfoster advancement in the nursing profession andhave enormous implications in reversing the growingtrend of childhood overweight (Friedman et al.).
It is essential that child-based interventions be guidedby theoretical perspectives that consider the child’ssocial context. Schools have been identified as idealenvironments for the initiation of healthy lifestyleeducation for youth in the United States as well asinternationally. School settings provide the opportunityto carry out educational programs in stable andestablished settings (Hayman et al., 2004). In school,children may have the following opportunities notavailable in other settings: (a) one to two meals eachday, (b) physical activity instruction in a safe environ-ment, and (c) educators who can be trained inhealthy behavior curriculum (Davis, Davis, Northing-ton, Moll, & Kolar, 2002). In addition, school settingshave the potential to reach the majority of our nation’syouth.
Healthy lifestyle education, dietary habits, andphysical activity have been identified as modifiablevariables that influence childhood overweight and at-risk for overweight (American Academy of Pediatrics[AAP], 2003; Barlow & Dietz, 1998; Hayman et al.,2004). Healthy lifestyle education should emphasizephysical activity and nutritional knowledge to encour-age positive behavioral changes (Story, 1999). Dietarygoals set forth by the pediatric expert committeeare well-balanced, healthy meals that adhere to theFood Guide Pyramid developed by the USDHHS(Barlow & Dietz, 1998).
Decreased physical activity is strongly associatedwith an increase in incidence of overweight and itsassociated adverse health effects (AAP, 2003). Onesurvey indicated that the proportion of childrenattending physical education classes in school decreasedfrom 41.6% in 1991 to 29.1% in 1999 (Grunbaum et al.,2002). The amount of physical activity recommendedby the Surgeon General’s report involves at least30 min of moderate to vigorous activity on most days(USDHHS, 2004b).

168 JSPN Vol. 11, No. 3, July, 2006
An Integrative Research Review: Effective School-Based Childhood Overweight
Definitions
The term
theoretical perspective
refers to theunderlying theoretical or conceptual foundation astudy is built upon (Polit & Beck, 2004). Theoreticalperspectives are often stated clearly in sections ofresearch papers under such headings as “theoreticalframeworks” or “conceptual frameworks” (Polit &Beck). Theoretical perspectives can also be implied,challenging readers to extract common methodologiesthat fall under established theories and models (Polit& Beck). Theoretical and conceptual frameworks weredesigned to make research findings more measurableand meaningful, thus advancing knowledge andevidence-based practice (Polit & Beck).
Healthy lifestyle education, dietary habits,
and physical activity have been identified as
modifiable variables that influence childhood
overweight and at-risk for overweight.
The definition of effective school-based interven-tions that is used in this review refers to thoseinterventions that resulted in a significant reductionin BMI or weight in children ages 4–14 years. Beginningin 1998, the expert committee on pediatrics recom-mended BMI as a preferred method of measuringadiposity across age groups (Barlow & Dietz, 1998).BMI has been found to accurately correlate with bodyfatness, using height and weight, measurements thatare easily attainable and readily available in everypractice setting (Pietrobelli et al., 1998). In 2000, theCenters for Disease Control and Prevention (CDC)added BMI in children (ages 2–20) as part of thestandard growth assessment tool used in pediatriccare settings (Kuczmarski, Ogden, & Guo, 2002). Prior
to 2000, height and weight measurements were usedfor standard overweight assessment in pediatrics(Barlow & Dietz). Consequently, studies publishedprior to 2000 that found a significant reduction inweight from their school-based interventions werealso included in this literature review.
The definition of healthy lifestyle education used inthis review is based on the “Blueprint for Our Nation’sHealth and Prevention,” Healthy People 2010,released by the USDHHS (2000). Healthy lifestyleeducation includes providing youth with “the capacityto obtain, interpret, and understand basic healthinformation and services and the competence to usesuch information and services to enhance health”(USDHHS, 2004b).
Dietary habits refer to a prescribed course of eatingand drinking in which the amount and kind of foodand time at which one eats and drinks are regulated(Stedman, 2002). This review includes studies thatdirectly influenced children’s daily dietary consumption,whether by restricting caloric intake or controlling theactual food choices available to them while in theschool setting. Physical activity is defined as “any bodilymovement produced by skeletal muscles and resultingin energy expenditure” (Bourchard, Shephard, Stephens,& Sutton, 1990, p. 6).
Methods
The model of research utilization developed byStetler et al. (1998) was the guiding framework for thisintegrative research review. Stetler’s model includesfive phases: preparation, validation, comparativeevaluation/decision making, translation/application,and evaluation.
The sampling frame for the study was effectiveschool-based intervention studies that used healthylifestyle education, dietary habits, and/or physicalactivity interventions in children ages 4–14. Theinclusion criteria for the study were (a) school-basedstudies published prior to February 5, 2005; (b) studiesthat involved children ages 4 to 14; a manipulation of

JSPN Vol. 11, No. 3, July, 2006 169
at least one of the variables of healthy lifestyle education,dietary habits, and/or physical activity; and (c) studieswith a statistically significant decrease in BMI orweight. Studies that did not meet the above criteriawere excluded from this review.
Tools used in this literature review includedcomputer search engines accessed from the libraryfacilities of a southeastern major research institution.The majority of the studies for this review wereobtained from the search engines PubMed and CINAHL.The search engine terms used were “school andchildhood obesity,” “school-based intervention andobesity,” “obesity and school,” “school-aged childrenand obesity intervention,” “school-based interventions,”“obesity and children,” “nutrition and school,” “physicalactivity and obesity and children,” “diets and obesityand children,” and “childhood obesity or overweight.”
The ancestry approach, as defined by Cooper (1982),was also used. The ancestry approach involves gatheringinformation by pursuing articles cited in others’reference lists. Two integrative research reviews werelocated and their reference lists examined to identifyadditional relevant studies (Moyer et al., 2000; Story,1999). After an exhaustive investigation with theassistance of a university librarian, 10 studies that metinclusion criteria comprised the study sample.
Research synthesis tables were developed duringthe validation and comparative phases. The tablesprovided visualization and comparison of ages andnumber of subjects, research design and level, inter-ventions, and outcomes (Stetler, 2001). There are sixdifferent levels of research described by Stetler et al.(1998). Level I describes the strongest type of research—meta-analysis of multiple controlled studies. Level IIdescribes individual experimental studies. Level IIIindicates a quasi-experimental study, and a nonexperi-mental study is classified as Level IV. Level Vdescribes a case report or program evaluation data.Finally, Level VI indicates reviewed evidence basedupon the opinions of respected authorities. Thetranslation/application and evaluation phases arepresented in the discussion section.
Results
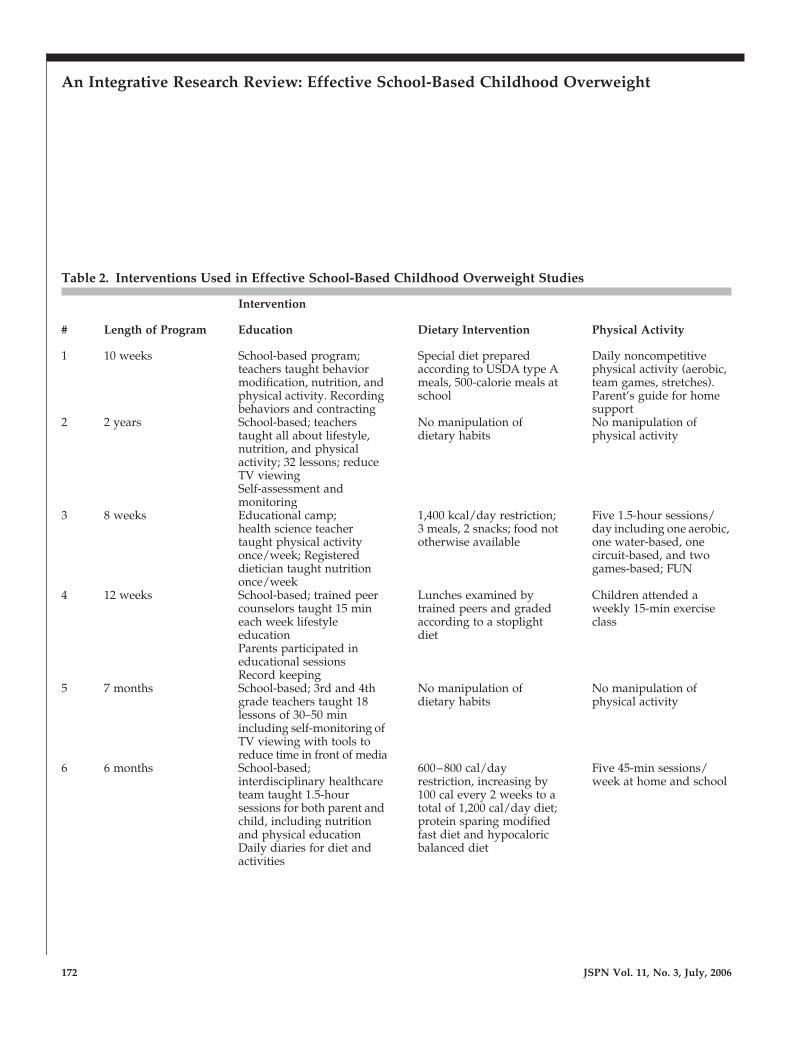
The research synthesis tables are displayed in Tables1 and 2. Table 1 provides an overview of the studies,including publication citation, sample characteristics,research design, theoretical perspective, and outcomes.Table 2 provides an overview of the specific interven-tions and length of time each was implemented.
Theoretical Perspective
Three of the studies included Social CognitiveTheory (SCT) by name in their description of theoreticalframeworks (Gately, Cooke, Butterly, Knight, & Carroll,2000; Gortmaker et al., 1999; Robinson, 1999). Charac-teristics of the social-cognitive perspective include self-evaluation and self-monitoring, peer support, socialsetting, modeling, observational learning, and inclu-sive participation (Bandura, 1986). These conceptswere mentioned under sections “Treatment Program,”“Methods,” “Behavior Modification,” and “Interven-tions” in five other studies (Brownell & Kaye,1982; Figueroa-Colon, Franklin, Lee, von Almen, &Suskind, 1996; Foster, Wadden, & Brownell, 1985;Manios, Moschandreas, Hatzis, & Kafatos, 1999;Muller, Asbeck, Mast, Langnase, & Grund, 2001). Twoof the studies (Flores, 1995; Mo-suwan, Pongprapai,Junjana, & Puetpaiboon, 1998) did not specificallymention concepts commonly associated with SCT.However, their study interventions were conducted infun, noncompetitive social settings among classmates.
Research Design
Investigators in 9 out of the 10 studies reportedusing an experimental research design. They wereassigned levels according to Stetler’s model of research(see Table 1). Of those nine, six were reported as indi-vidual, experimental studies. Brownell and Kaye(1982) and Figueroa-Colon et al. (1996) conductedquasi-experimental studies. The study by Muller et al.(2001) was reported in two phases: one phase was

170JSPN
Vol. 11, N
o. 3, July, 2006
An Integrative R
esearch Review
: Effective School-Based C
hildhood Overw
eight
Table 1. Effective School-Based Childhood Overweight Studies
Project #
Authors/citation/year
Sample Age/grade
# Subjects Research Design
Level Theory SCT
Outcome BMI/weight
1 Brownell & Kaye
American Journal of Clinical Nutrition
1982
5–12 years 77 total; 63 intervention,14 control (no gender described)
experimental III + *95% lost weight, 99% reduced % overweight, 71% control gained weight
2 Gortmaker et al.
Archives of Pediatric and Adolescent Medicine
1999
Grades 6–7 1,295 surveyed; 627 girls, 668 boys
experimental II + Decreased in girls, especially African American, but no change in boys
3 Gately et al.
Pediatric Exercise Science
2000
12.6
±
2.5 years 194; 64 boys, 130 girls
prospective nonexperimental
IV + Decreased in whole group, 12%
4 Foster et al.
Journal of Consulting and Clinical Psychology
1985
Grades 2–5 48 students; 24 boys, 24 girls enrolled
experimental II + *Treatment group lost 0.15 kg, control gained 1.3 kg; at 18 month follow-up, program children gained more weight
5 Robinson
Journal of the American Medical Association
1999
Grades 3–4 192 students; 100 in intervention (45 girls, 55 boys), 92 in control (44 girls, 48 boys)
experimental II + Significant decrease in intervention group compared with control
6 Figueroa- Colon et al.
Obesity Research
1996
Grades 3–5 19 students; 12 in intervention, 7 control, 11 girls, 7 boys
experimental III + Significant decrease in intervention group compared with control
7 Muller et al.
International Journal of Obesity
2001
5–7 years 1,640 total students in 6 schools; 847 girls, 793 boys
experimental II/III + †Significant increase in control vs. intervention at 1-year follow-up
8 Mo-suwan et al.
American Journal of Clinical Nutrition
1998
4 years, Kindergarten
292 students; 147 intervention and 145 control; 170 boys, 122 girls
experimental II – ‡Significant decrease in probability of increase in BMI slope in girls; no significant change in boys

JSPN V
ol. 11, No. 3, July, 2006
171
9 Manios et al.
Preventive Medicine
1999
Grade 1 471 total; 288 students in 24 intervention schools; 183 students in 16 control schools (no gender described)
experimental II + †Significant increase in control vs. intervention at 3-year follow-up
10 Flores
Public Health Report
1995
Grade 7 81 total students; 43 intervention students, 38 control students 44 boys, 37 girls
experimental II – Significant decrease in girls only; decrease in boys (not significant)
*Before BMI standard recommended, accepted loss of weight in kg.†Studies showing an increase in BMI in control vs. intervention.‡Studies using BMI slope, or rate of change of BMI.
Project #
Authors/citation/year
Sample Age/grade
# Subjects Research Design
Level Theory SCT
Outcome BMI/weight
Table 1.
Continued
172 JSPN Vol. 11, No. 3, July, 2006
An Integrative Research Review: Effective School-Based Childhood Overweight
Table 2. Interventions Used in Effective School-Based Childhood Overweight Studies
Intervention
# Length of Program Education Dietary Intervention Physical Activity
1 10 weeks School-based program; teachers taught behavior modification, nutrition, and physical activity. Recording behaviors and contracting
Special diet prepared according to USDA type A meals, 500-calorie meals at school
Daily noncompetitive physical activity (aerobic, team games, stretches). Parent’s guide for home support
2 2 years School-based; teachers taught all about lifestyle, nutrition, and physical activity; 32 lessons; reduce TV viewing Self-assessment and monitoring
No manipulation of dietary habits
No manipulation of physical activity
3 8 weeks Educational camp; health science teacher taught physical activity once/week; Registered dietician taught nutrition once/week
1,400 kcal/day restriction; 3 meals, 2 snacks; food not otherwise available
Five 1.5-hour sessions/day including one aerobic, one water-based, one circuit-based, and two games-based; FUN
4 12 weeks School-based; trained peer counselors taught 15 min each week lifestyle education Parents participated in educational sessions Record keeping
Lunches examined by trained peers and graded according to a stoplight diet
Children attended a weekly 15-min exercise class
5 7 months School-based; 3rd and 4th grade teachers taught 18 lessons of 30–50 min including self-monitoring of TV viewing with tools to reduce time in front of media
No manipulation of dietary habits
No manipulation of physical activity
6 6 months School-based; interdisciplinary healthcare team taught 1.5-hour sessions for both parent and child, including nutrition and physical education Daily diaries for diet and activities
600–800 cal/day restriction, increasing by 100 cal every 2 weeks to a total of 1,200 cal/day diet; protein sparing modified fast diet and hypocaloric balanced diet
Five 45-min sessions/week at home and school

JSPN Vol. 11, No. 3, July, 2006 173
7 1 school year School-based; school teachers and nutritionists taught 8 hours total nutrition and health promotion, self-monitoring 3 home visits by registered dietician with family
No manipulation of dietary habits
6-month sports program offered only to overweight children and parents (twice weekly)
8 30 weeks School-based; no manipulation of healthy lifestyle education
No manipulation of dietary habits
15-min walk each day before class taught by physical education teachers; 20-min aerobic dance session 3
×
/week taught by research personnel
9 1 school year evaluated 3 years post study
School-based; school teachers taught health promotion program 13–17 hours of in-class learning; physical activity education 4–6 hours total Parental education
No manipulation of dietary habits
Physical activity two 45-min sessions/week, about 60 classes/year
10 12 weeks School-based; school teachers taught health education curriculum 30 min twice weekly for total of 25 lessons
No manipulation of dietary habits
3
×
/week dance class (50 min long)
Intervention
# Length of Program Education Dietary Intervention Physical Activity
Table 2.
Continued
considered an individual, experimental study and theother was quasi-experimental. The study by Gatelyet al. (2000) was classified as nonexperimental.
Sample Characteristics
The geographical location for 7 of the 10 studieswas the United States, with the remaining three takingplace in Germany, Crete, and Thailand (Muller et al.,2001; Manios et al., 1999; Mo-suwan et al., 1998).Sample size in the studies ranged from 19 to 1,560students, and length of the programs ranged from8 weeks to 2 years (see Table 2). Nine of the studiesreported equal representation of both gender and
ethnicity, while Flores’ “Dance for Health” (1995)study sampled only African American and Hispanicstudents (see Table 2). The study by Gately et al. (2000)included only children from families with high socio-economic status in their educational summer camp.Four of the studies included only overweight childrenin their samples (Brownell & Kaye, 1982; Figueroa-Colon et al., 1996; Foster et al., 1985; Gately et al.).
Outcomes
The outcomes of each study are found in Table 1.Only 2 of the 10 studies reported follow-up outcomes.Muller et al. (2001) reported significant findings at

174 JSPN Vol. 11, No. 3, July, 2006
An Integrative Research Review: Effective School-Based Childhood Overweight
1-year follow-up, and Manios et al. (1999) reported asignificant increase in BMI in the control versusintervention group at the 3-year follow-up.
Healthy Lifestyle Education
Healthy lifestyle education was implemented in 9of the 10 studies reviewed (see Table 2). As stated bythe authors, the purpose of including healthy lifestyleeducation was to encourage lifelong benefits bychanging existing behaviors. In these nine studies, thehealthy lifestyle education interventions focused onappropriate nutrition and physical activity behaviorsfor children. Education was delivered via classroomlessons, discussions, and printed materials. In six ofthe nine studies, teachers taught the curriculum to thechildren. In the remaining three studies, schoolteach-ers and nutritionists shared in the teaching (Mulleret al., 2001), an interdisciplinary healthcare team deliv-ered the intervention (Figueroa-Colon et al., 1996), andpeers trained by the researchers taught the educationalsessions (Foster et al., 1985).
Healthy lifestyle education included specific lessons,concentrating on the importance of slowing the rate ofeating, increasing fruit and vegetable intake, decreasinghigh-fat foods in diets, and increasing daily physicalactivity. The programs described in 6 of the 10 studies(see Table 2) stressed the impact that self-evaluationand self-monitoring have on changing unhealthybehavior. Additional emphasis was placed on reducingtelevision viewing and video game use.
Dietary Habits
Four of the 10 studies manipulated dietary habits ofoverweight children (Brownell & Kaye, 1982; Figueroa-Colon et al., 1996; Foster et al., 1985; Gately et al., 2000).Interventions included restricting calories to 1,200–1,400/day, limiting lunches to USDA Type A 500calorie meals, holding lunch box inspections, providingvitamin/mineral supplements, and controlling avail-ability of foods. Two of these four studies used hypocaloric
dietary interventions (Figueroa-Colon et al.; Gatelyet al.). The studies provided each participant in theexperimental groups with equally restrictive caloricdiets meant to reduce BMI or weight rather thanindividually designed diets.
Physical Activity
Physical activity interventions were implemented in8 of the 10 studies (Brownell & Kaye, 1982; Figueroa-Colon et al., 1996; Flores, 1995; Foster et al., 1985; Gatelyet al, 2000; Manios et al., 1999; Mo-suwan et al., 1998;Muller et al., 2001). Physical activity interventionsvaried from a simple walk (Mo-suwan et al.), tononcompetitive sports (Brownell & Kaye), to choreo-graphed dance routines (Flores). Evidence of a social-cognitive perspective was seen in the design of theinterventions, such as the inclusion of parents andpeers, as well as noncompetitive and fun physical activitycurricula (see Table 2).
Number of Intervention Approaches
Four of the 10 studies focused on overweight childrenand used a combination of all three interventionapproaches (Brownell & Kaye, 1982; Figueroa-Colonet al., 1996; Foster et al., 1985; Gately et al., 2000). Twoof the 10 studies used a healthy lifestyle educationintervention only (Gortmaker et al., 1999; Robinson,1999), and one of the studies used a physical activityintervention only (Mo-suwan et al., 1998). Three of the10 studies used healthy lifestyle education and physicalactivity treatment approaches, but they did not includea dietary habits intervention (Flores, 1995; Manioset al., 1999; Muller et al., 2001).
Discussion
Social Cognitive Theory or the theoretical under-pinnings of this theory was found in the theoretical per-spective or research methods in 8 of the 10 studiesin this review. This theory is based on observational

JSPN Vol. 11, No. 3, July, 2006 175
learning and modeling and highlights the impact ofsocial and/or peer acceptability on human behavior(Bandura, 1986). Self-empowerment and ownership ofone’s learning and capabilities are highly valued inSCT. When using this theoretical perspective, thefacilitator’s role is to actively include student participa-tion, using innovative strategies to implement positivechanges. This provides students with fundamentalknowledge and skills that encourage lifelong change inthe context of their everyday lives (Bandura).
Social Cognitive Theory or the theoretical
underpinnings of this theory was found in
the theoretical perspective or research
methods in 8 of the 10 studies in this review.
The findings of this review support the fact that themajority of school-based interventions used multipletreatment modalities to address childhood overweight(AAP, 2003). Four of the 10 studies used a combinationof healthy lifestyle education, dietary intervention,and physical activity. Three of the 10 studies includeda healthy lifestyle component and a physical activitycomponent. However, 2 of the 10 studies used only ahealthy lifestyle education approach, while one studyused a physical activity intervention only.
Interventions must consider the powerful influencesof the child’s social context on treatment approachesand the theoretical basis for their use. Healthy lifestyleeducation was delivered to students in structured,educational settings with peer support and teacherguidance. Teachers were commonly responsible forthe teaching of the healthy lifestyle curriculum. Theyare important role models in the school setting forchildren. As such, they represent an importantcommunity partner for nurses who work with
childhood overweight in primary care clinics andspecialty outpatient clinics.
Unlike dietary habits and physical activity interven-tions that could be manipulated only during schoolhours, healthy lifestyle education had the potential toimpact the behavior of children at a cognitive level atschool and across other settings. In some cases, parentswere also included in the study participant’s educa-tion. Providing education in a nonthreatening, familiarsetting with a supportive network of friends andfamily is an effective educational strategy for targetingchildhood overweight. This approach was successfulin contributing to the desired outcome in thesestudies. In addition, interventions in the majority ofthese studies provided incentives to promote positivechanges in children’s dietary intake and habits, particu-larly in younger children. Self-regulatory mechanisms,such as diaries to document food intake or televisionconsumption, challenged children to take ownershipof their behaviors.
No attempt was made in this review to evaluate thequality of the studies, including sample size andpower. Sample sizes and sample characteristics variedgreatly across studies. The time frames for interven-tions in these studies were highly variable or inade-quately described. Thus, recommendations regardingthe ideal time frame for an interventive approachcannot be determined. Finally, effective interventionswere used as a means to answer the research questionand identify the study sample. No conclusion aboutthe actual effectiveness of the interventions can bedrawn from this integrative review.
How Do I Apply This Information to Nursing Practice?
Social Cognitive Theory is a sound theoreticalperspective for designing and implementing successfulinterventions with children. SCT emphasizes thecritical importance of social contexts on the beha-vior of children. It is within the school setting that

176 JSPN Vol. 11, No. 3, July, 2006
An Integrative Research Review: Effective School-Based Childhood Overweight
children are socialized to accept the standards andvalues of their society. As the values and standards ofhealth change, the school is an ideal setting for pro-motion of new health behaviors. Specialists inpediatric nursing should work collaboratively withteachers and other educators in the community toachieve positive outcomes related to childhoodoverweight.
Successful interventions for childhood overweight
should
consider the principles of SCT. Modeling isone of the primary techniques that should be encour-aged when designing interventions for children in theschool setting. Demonstration of and the opportunityto rehearse behaviors that improve overweight inchildren by teachers, peers, and students themselvesshould be highlighted. Self-monitoring is an SCTtechnique that incorporates self-reflection andself-evaluation of behaviors. Additionally, the use ofcontracts with goals and rewards can regulate andreinforce newly minted behaviors and improveself-efficacy. Self-efficacy, or the belief in one’s abilityto achieve a goal or be successful, is an importantcomponent of SCT and behavioral change. Moreimportantly, the SCT stresses assessment of thecognitive skills of children and the need to providechildren with the opportunity to rehearse, organize,and recall new behaviors. Many examples of ways touse SCT in designing interventions in school-based programs are provided by the studies in thisreview and can be used by those specializing in thewell-being of children to improve their futurehealth.
Author contact: [email protected], with a copy to theEditor: [email protected]
References
American Academy of Pediatrics: Committee on Nutrition. (2003).Prevention of pediatric overweight and obesity.
Pediatrics
,
112
(2),424–428.
Amschler, D. (2002). The alarming increase of type 2 diabetes in chil-dren.
Journal of School Health
,
72
(1), 39–41.Bandura, A. (1986).
Social foundations of thought in action. A social cog-nitive theory.
Englewood Cliffs, NJ: Prentice Hall.Barlow, S.E., & Dietz, W.H. (1998). Obesity evaluation and treat-
ment: Expert committee recommendations.
Pediatrics
,
102
(3), 1–11.Bourchard, C., Shephard, R.J., Stephens, T., & Sutton, J.R. (1990).
Exercise, fitness and health: A consensus of current knowledge
. Cham-paign, IL: Human Kinetics Books.
Brownell, K.D., & Kaye, F.S. (1982). A school-based behaviormodification, nutrition education, and physical activity programfor obese children.
American Journal of Clinical Nutrition
,
35
, 277–283.
Cooper, H.M. (1982). Scientific guidelines for conducting integrativeresearch reviews.
Review of Educational Research
,
52
(2), 291–302.Davis, S.P., Davis, M., Northington, L., Moll, G., & Kolar, K. (2002).
Childhood obesity reduction by school based programs.
TheABNF Journal
,
6
, 145–149.Figueroa-Colon, R., Franklin, F.A., Lee, J.Y., von Almen, T.K., &
Suskind, R.M. (1996). Feasibility of a clinic-based hypocaloricdietary intervention implemented in a school setting for obesechildren.
Obesity Research
,
4
, 419–429.Flores, R. (1995). Dance for health: Improving fitness in African
American and Hispanic adolescents.
Public Health Report
,
110
(2),189–193.
Foster, G.D., Wadden, T.A., & Brownell, K.D. (1985). Peer-ledprogram for the treatment and prevention of obesity in theschools.
Journal of Consulting and Clinical Psychology
,
53
(4), 538–540.Freeman, D., Dietz, W., Srinivasan, S., & Berenson, G. (1999). The
relation of overweight to cardiovascular risk factors amongchildren and adolescents: The Bogalusa Heart Study.
Pediatrics
,
103
(6), 1175–1182.Friedman, M., Bowden, V., & Jones, E. (2003).
Family nursing:Research, theory and practice
(5th ed.). Englewood Cliffs, NJ:Prentice Hall.
Gately, P.J., Cooke, C.B., Butterly, R.J., Knight, C., & Carroll, S.(2000). The acute effects of an 8-week diet, exercise and educationalcamp program on obese children.
Pediatric Exercise Science
,
12
,413–423.
Gortmaker, S.L., Peterson, K., Wiecha, J., Sobol, A.M., Dixit, S., Fox,M.K., & Laird, N. (1999). Reducing obesity via a school-basedinterdisciplinary intervention among youth.
Archives of Pediatricsand Adolescent Medicine
,
153
, 409–417.Grunbaum, J.A., Kann, L., Kinschen, S.A., Williams, B., Ross, J.G.,
Lowry, R., & Kolbe, L. (2002). Youth risk behavior surveillance-United States 2001.
Morbidity and Mortality Weekly ReportSurveillance Summary
,
51
, 1–62.Hayman, L.L., Williams, C.L., Daniels, S.R., Steinberger, J., Paridon,
S., Dennison, B.A., & McCrindle, B.W. (2004). Cardiovascularhealth promotion in the schools: A statement for health andeducation professionals and child health advocates from thecommittee on atherosclerosis, hypertension, and obesity in youthof the council on cardiovascular disease in the young, AmericanHeart Association.
Circulation
,
110
, 2266–2275.Hedley, A.A., Ogden, C.L., Johnson, C.L., Carroll, M.D., Curtin, L.R.,
& Flegal, K.M. (2004). Prevalence of overweight and obesity

JSPN Vol. 11, No. 3, July, 2006 177
among U.S. children, adolescents, and adults, 1999–2002.
Journalof the American Medical Association
,
291
(23), 2847–2851.Kimm, S.Y., & Obarzenek, E. (2002). Childhood obesity: A new
pandemic of the new millennium.
Pediatrics
,
110
(5), 1003–1007.Kuczmarski, R.J., Ogden, C.L., & Guo, S.S. (2002). 2000 CDC growth
charts for the United States: Methods and development.
NationalCenter for Health Statistics, Vital Health Statistics
,
11
(246).Manios, Y., Moschandreas, J., Hatzis, C., & Kafatos, A. (1999). Evalua-
tion of a health and nutrition program in primary school childrenof Crete over a three-year period.
Preventative Medicine
,
28
, 149–159.Morgan, C., Yanovski, S., Ngyen, T., McDuffie, J., Sebring, N., Jorge,
M., Keil, M., & Yanovski, J.A. (2002). Loss of control over eating,adiposity, and psychopathology in overweight children.
International Journal of Eating Disorders
,
31
(4), 430–441.Mo-suwan, L., Pongprapai, S., Junjana, C., & Puetpaiboon, A. (1998).
Effects of a controlled trial of a school-based exercise program onthe obesity indexes of preschool children.
American Journal ofClinical Nutrition
,
68
, 1006–1011.Moyer, V.A., Elliott, E.J., Davis, R.L., Gilbert, R., Klassen, T., Logan,
S., Mellis, C., & Williams, K. (2000).
Evidence-based pediatrics andchild health.
London: BMJ Books.Muller, M.J., Asbeck, I., Mast, M., Langnase, K., & Grund, A. (2001).
Prevention of obesity—More than an intention. Concepts andfirst results of the Kiel Obesity Prevention Study (KOPS).
International Journal of Obesity
,
25
(S1), S66–S74.Pietrobelli, A., Faith, M.S., Allison, D.B., Gallagher, D., Chiumello,
G., & Heymsfield S. (1998). Body mass index as a measure ofadiposity among children and adolescents: A validation study.
Journal of Pediatrics
,
132
, 204–210.
Polit, D., & Beck, C. (2004).
Nursing research principles and methods
(7th ed.). Philadelphia: Lippincott Williams & Wilkins.Robinson, T.N. (1999). Reducing children’s television viewing to
prevent obesity: A randomized controlled trial.
Journal of theAmerican Medical Association
,
282
(16), 1561–1567.Sabin, M., Crowne, E., & Shield, J. (2002). Childhood obesity and
type 2 diabetes.
Nursing Times
,
98
(19), 49–50.Stedman, T. (Ed.). (2002).
The American heritage Stedman’s medical dic-tionary
(28th ed.). Boston: Houghton Mifflin Company.Stetler, C.B., Morsi, D., Rucki, S., Broughton, S., Corrigan, B.,
Fitzgerald, J., Giuliano, K., Havener, P., & Sheridan, E.A. (1998).Utilization-focused integrative reviews in a nursing service.
Applied Nursing Research
,
11
(4), 195–206.Stetler, C.B. (2001). Updating the Stetler model of research utilization
to facilitate evidence-based practice.
Nursing Outlook
,
49
(6), 272–279.
Story, M. (1999). School-based approaches for preventing and treatingobesity.
International Journal of Obesity
,
23
(S2), S43–S51.U.S. Department of Health and Human Services. (2000).
Healthy people2010: Conference edition
. Washington, DC. Retrieved November 17,2004 from http://web.health.gov/healthypeople/Document/default.htm.
U.S. Department of Health and Human Services. (2004a).
Health,United States, 2004
. Retrieved February 5, 2005, from http://www.cdc.gov/nchs/data/hus/hus04trend.pdf#070.
U.S. Department of Health and Human Services. (2004b).
The SurgeonGeneral’s call to action to prevent and decrease overweight and obesity.
Retrieved January 11, 2005, from http://www.surgeongeneral.gov/topics/obesity/calltoaction/fact_adolescents.htm.