a.m. staiano - etouches · outline 1. differenza tra reflusso gastroesofageo e malattia da reflusso...
TRANSCRIPT

La patologia respiratoria e il
reflusso gastro-esofageo
A.M. Staiano

La patologia respiratoria e
il reflusso gastro-esofageo
ANNAMARIA STAIANO
Dipartimento di Scienze Mediche Traslazionali
Sezione di Pediatria
Università di Napoli “Federico II”
Outline
1. Differenza tra reflusso gastroesofageo e malattia da
reflusso gastroesofageo (MRGE)
2. Le manifestazioni respiratorie della MRGE
3. Eccessivo uso di farmaci acido-soppressori
La patologia respiratoria e il reflusso gastro-esofageo

NASPGHAN-ESPGHAN Guidelines for Evaluation and Treatment
of Gastro-Esophageal Reflux in Infants and Children Y. Vandenplas, C. Rudolph, G. Liptak, M. Lynette, C. Di Lorenzo, E. Hassall,
J. Sondheimer, M. Thomson, A. Staiano, G. Veereman, T. Wenzl
J Pediatr Gastroentoerol Nutr 2009;49:498-547
11/28/2014
Gastroesophageal reflux: management guidance for the pediatrician. Lightdale JR, Gremse DA; Section on Gastroenterology, Hepatology, and Nutrition.
Pediatrics. 2013;131:e1684-95
This clinical report endorses the rigorously developed,
well-referenced North American Society for Pediatric
Gastroenterology, Hepatology, and Nutrition guidelines and
likewise emphasizes important concepts for the general
pediatrician.

• Il reflusso gastroesofageo (RGE) è un
fenomeno fisiologico che si verifica in
lattanti, bambini e adulti.
• Il reflusso fisiologico si presenta
solitamente in circa il 70% dei lattanti
di 4 mesi di età.
• Nella maggior parte dei lattanti il RGE
non causa alcun sintomo.
Il Reflusso Gastroesofageo

Sherman PM et al. Am J Gastroenterol 2009
La Malattia da Reflusso Gastroesofageo (MRGE) è
presente quando il reflusso del contenuto gastrico è
causa di sintomi fastidiosi e/o di complicanze.
Definizione

• A detailed questionnaire was completed by 59 primary care pediatricians .
• 2642 patients (0-12 months) were prospectively enrolled during a 3-month period.
• Follow-up at 6, 12, 18 and 24 months of age
“PREVALENCE AND NATURAL HISTORY OF
GASTROESOPHAGEAL REFLUX:
PEDIATRIC PROSPECTIVE SURVEY” (1/2)
Campanozzi A. Pediatrics 2009

• 313 infants (12%; 147 girls) affected by infant regurgitation.
• Vomiting in 34/313 patients (10.9%).
• Follow-up in 210/313: regurgitation disappeared
• 56 (27%) at 6 months
• 128 (61%) at 12 months
• 23 (11%) at 18 months
• 3 (1%) at 24 months
• Organic disease in 2/210 (0.1%)
Campanozzi A. Pediatrics 2009
“PREVALENCE AND NATURAL HISTORY OF
GASTROESOPHAGEAL REFLUX:
PEDIATRIC PROSPECTIVE SURVEY” (2/2)

Sherman PM, et al. Am J Gastroenterol 2009
La patologia respiratoria e il reflusso gastro-esofageo

La patologia respiratoria e il reflusso gastro-esofageo
• POLMONITI RICORRENTI
• PATOLOGIA LARINGEA
• SINUSITE
• OTITE MEDIA E OTALGIA
• APNEA
• ASMA E TOSSE CRONICA

Vantaggi
• Rileva sia reflussi acidi che alcalini
•Determina l’associazione temporale tra
MRGE e sintomi
•Può essere eseguita in pazienti in terapia
anti-acida
•Può definire l’altezza e la composizione del
reflusso (gas, liquido, misto)
Limiti
•I valori normali in età pediatrica non sono
stati ancora definiti
•L’analisi dei tracciati richiede tempo (2-5 ore
per paziente)
Impedance
channels
t
pH IMPEDENZOMETRIA
J Pediatr Gastroenterol Nutr 2009; 49:498-547
La patologia respiratoria e il reflusso gastro-esofageo: DIAGNOSI

Respiratory Medicine (2011) 105, 972e978
Interobserver agreement in combined pH-multichannel intraluminal
impedance analysis in experts is moderate; only 42% of GER episodes
were detected by the majority of observers.
Considering these poor outcomes, automated analysis (AA) seems
favorable compared with manual analysis because of its reproducibility.
However, the lower specificity rate suggests the need for refinement of
AA before widespread use can be advocated.
J Pediatr 2012;160:441-6

Vandenplas Y. Expert Opin Med Diagn. 2013;7:289-98
Challenges in the diagnosis of GERD in infants
and children.
Although evidence for a "relation" between GER and extra-
esophageal symptoms is demonstrated, the "causality" between both
is not proven.
MII measures non-acid or weakly acid reflux.
However, as long as medical therapeutic options are limited to anti-
acid medications, MII lacks therapeutic implications, and therefore
clinical impact.

At present,
no single diagnostic test can prove or
exclude extraesophageal presentations of
GERD in pediatrics.
Pediatric Gastroesophageal Reflux Clinical Practice Guidelines:
Joint Recommendations of NASPGHAN and ESPGHAN
Co-Chairs: Yvan Vandenplas and Colin D. Rudolph
J Pediatr Gastroentoerol Nutr 2009;49:498-547

In children with reflux-related cough, dilated intercellular
space diameter appears to be an objective and useful marker
of oesophageal mucosal injury regardless of acid exposure,
and its evaluation should be considered for those patients
where the diagnosis is uncertain.
Dilated intercellular space diameter as marker of
reflux-related mucosal injury in children with chronic
cough and gastro-oesophageal reflux didease
O. Borrelli et al. Aliment Pharmacol Ther 2014; 39: 733–742
Extraesophageal Presentations of GER: Where is the
Science?
• Suspected extraesophageal manifestations of GERD, such as
asthma, chronich cough and laryngitis, are commonly encountered in
gastroenterology practices.
• Otolaryngologists and gastroenterologists commonly disagree with
the underlying cause for the complaints in patients with one of the
suspected extraesophageal reflux syndromes.
• The accuracy of diagnostic tests ( laryngoscopy, endoscopy, and pH-
or pH-impedance monitoring) for patients with suspected
extraesophageal manifestations of GERD is suboptimal.
• An empiric trial of PPIsin patients without alarm features can help
some patients, but the response to therapy can be quite variable.
Gastroenterol Clin North Am. 2014 Mar;42(1):71-91

•162 infants with crying, regurgitation, refuse feed, coughing
•Treatment with lansoprazole or placebo for 4 weeks
•44/81 infants (54%) in each group were responders, identical for
lansoprazole and placebo
•Serious adverse events, expecially lower respiratory tract infections,
more frequently in the lansoprazole group compared with the placebo
group
Orenstein SR et al. J Pediatr 2009; 154: 514-20

PPI over-prescription: US report
Despite a lack of evidence to support
their effectiveness, PPI use in pediatric
patients has increased over time. In US
infants, there was an 11-fold increase in
the number of new prescriptions
dispensed between 2002 and 2009.
Food and Drug Administration: National database online. Years 2002-2009
Trends of Outpatient Prescription Drug Utilization in US Children
Pediatrics 2012;130; 23

Prevalence and Natural History of Infant
Regurgitation
Prevalence and Natural History of Infant Regurgitation
PPI over-prescription: European survey
results
Untrained pediatricians
Trained pediatricians
45.2 % 3.7 % 4.5 % 37.1 %
Infants with
unexplained crying
and/or distressed
behaviour who were
prescribed PPIs
Infants with
uncomplicated recurrent
regurgitation and
vomiting who were
prescribed PPIs
Quitadamo P et al. J Pediatr Gastroenterol Nutr. 2014 Apr;58(4):505-9

PPI over-prescription: European survey results
Quitadamo P et al. J Pediatr Gastroenterol Nutr. 2014;59: 356–359
Rates of PPIs over-prescription
(according to the guidelines indications for prescription)
Untrained
pediatricians
Trained
pediatricians
Do pediatricians apply the 2009 NASPGHAN-ESPGHAN guidelines for the
diagnosis and management of gastroesophageal reflux after being trained?

POTENZIALI RISCHI DEGLI
INIBITORI DI POMPA PROTONICA (IPP)
• Gli effetti collaterali attribuibili agli IPP tra cui cefalea, diarrea,
costipazione, nausea si verificano negli adulti fino al 14% dei casi
• Aumento del rischio di polmonite acquisita in comunità e gastroenterite
acuta nei bambini e negli adulti trattati con IPP
• Aumento del rischio di candidemia e di NEC nei neonati prematuri
trattati con terapia acido-soppressiva
• Nefrite interstiziale
• Possibile aumento del rischio di infezione da C. Difficile e di fratture
dell'anca negli adulti trattati cronicamente con IPP

Development of food allergies in patients with GERD
treated with gastric acid suppressive medications.
Children with GERD who were treated with GAS were more likely to be diagnosed
with a food allergy (Hazard ratio (HR): 3.67, 95% CI 2.15-6.27),
as were children with GERD diagnosis but who were not treated
with GAS medications (HR: 2.15, 95% CI: 1.21-3.81).
A direct comparison of the two GERD cohorts showed that children with GERD
who were treated with GAS had a greater risk of food allergy than those with
GERD who were untreated (HR, 1.68, 95%CI, 1.15-2.46).
Trikha A. Pediatr Allergy Immunol. 2013;24:582-8
Potential Mechanisms Linking Reflux to Respiratory Disorders
Reflux events potentially trigger coughing through three main mechanisms:
Microaspiration of refluxate into the airways
Extension of reflux into the larynx and pharynx (laryngo-pharyngeal reflux)
An ‘esophageal bronchial reflex’ Lung 2014; 192: 39-46
- Le polmoniti ricorrenti e le interstiziopatie possono essere
complicanze del reflusso dovute all’aspirazione del contenuto
gastrico. Tuttavia, nessun test è in grado di determinare se il
reflusso sia la causa delle polmoniti ricorrenti nel singolo paziente.
La positività di un esame pH-impedenzometrico può aumentare
la probabilità che il reflusso sia responsabile ma non fornisce la
certezza.
- L’aspirazione durante la deglutizione è più comune
dell’aspirazione del materiale refluito.
Vandenplas Y et al. J Pediatr Gastroenterol Nutr 2009;49:498-547
Polmoniti ricorrenti
La patologia respiratoria e il reflusso gastro-esofageo

PATOLOGIA LARINGEA
I dati che collegano il reflusso alla raucedine, tosse cronica, sinusite, otite cronica, eritema, e noduli laringei derivano principalmente da case reports e case series.
A B C
D E

• In children, based on current data, PPIs should not be used empirically.
• The single relatively large high quality study on the utility of PPI for cough
associated with GORD found no beneficial effect in infants and those on
lansoprazole had significantly increased serious adverse events, in
particular lower respiratory infections.
• Data on milk modification for infants and cough with GORD is insufficient
to make specific recommendations.
• Until more evidence is available in the form of well-designed RCTs, other
causes of cough should be considered in children with cough and GORD,
prior to any consideration of empiric treatment with a prolonged course of
GORD medications/interventions.
Cochrane Database of Systematic Reviews 2011, Issue 1. Art. No.: CD004823. DOI: 10.1002/14651858.CD004823.pub4.

• There is a possible association between GERD and asthma
in pediatric patients seen with asthma in referral settings.
• However, because of methodologic limitations of existing
studies, the paucity of population-based studies, and a lack
of longitudinal studies, several aspects of this association
are unclear.
Pediatrics 2010;125: e925–e930

Prevalence of Gastroesophageal Reflux Identified by
Esophageal pH-monitoring in Children with Asthma

Gastroesophageal reflux disease and childhood asthma.
Clinical studies show that GERD is highly prevalent in children with asthma, with
estimates as high as 80%, but nearly half of the children are asymptomatic.
However, there is no conclusive evidence per se that asymptomatic GERD
informs asthma control, and treatment of GERD in the few controlled trials
available for review does not substantively improve asthma outcomes.
In a recent large controlled clinical trial, treatment with a PPI was not
only ineffective, but adverse effects were common, including an
increased prevalence of symptomatic respiratory infections.
Current evidence does not support
the routine use of anti-GERD medication
in the treatment of poorly controlled asthma of childhood.
Blake K. Curr Opin Pulm Med. 2013;19:24-9

31 28-11-2014
Lansoprazole for children with poorly controlled asthma: a RCT (2) Writing Committee for the American Lung Association Asthma Clinical Research Centers.
JAMA.2012;307:373-81
…
115 children with pH metries: prevalence of GER was 43%
In the subgroup with a positive pH study,
no treatment effect for lansoprazole vs placebo
was observed for any asthma outcome.
Children treated with lansoprazole reported more respiratory infections
(relative risk, 1.3 [95% CI, 1.1-1.6]).
Children with poorly controlled asthma without symptoms of GER
who were using inhaled corticosteroids,
the addition of lansoprazole, compared with placebo,
improved neither symptoms nor lung function
but was associated with increased adverse events.
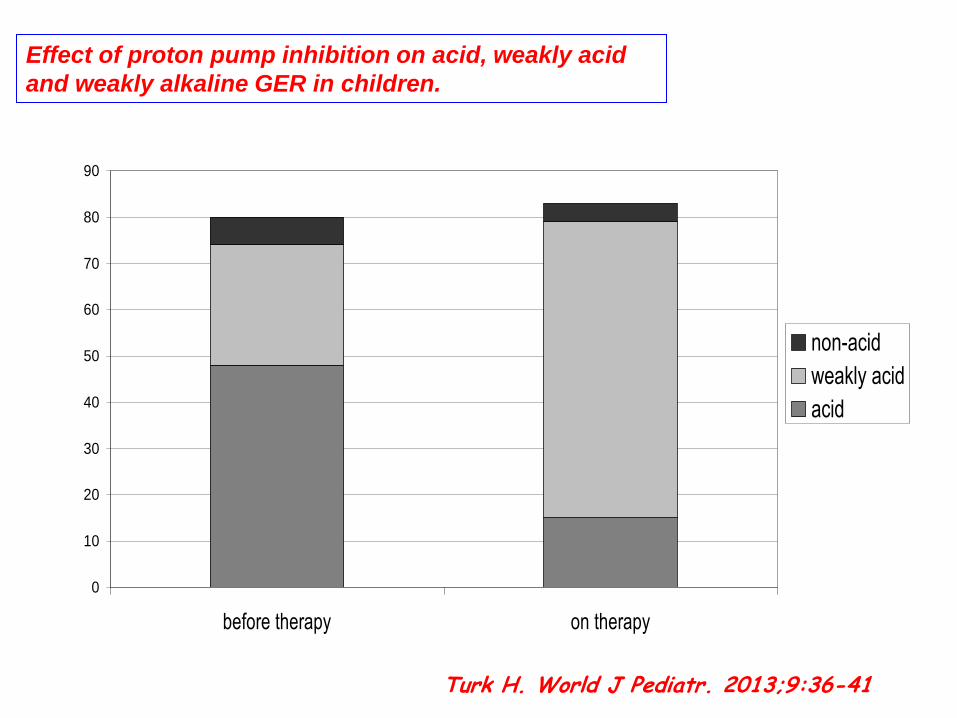
Turk H. World J Pediatr. 2013;9:36-41
0
10
20
30
40
50
60
70
80
90
before therapy on therapy
non-acid
weakly acid
acid
Effect of proton pump inhibition on acid, weakly acid
and weakly alkaline GER in children.
J Pediatr. 2011; 159(3): 504–506
• Do children with chronic cough or wheezing and with
more full-column, nonacid reflux have a higher likelihood
of a positive BAL fluid culture.
• 46 children with cough who had a positive culture had
significantly more full-column, nonacid GER than those
who had a negative culture.
PPI ? pos culture BAL
Higher Rate Of Bronchoalveolar Lavage Culture
Positivity In Children With Nonacid Reflux And
Respiratory Disorders.

Changes in gastric and lung microflora with Acid suppression: Acid suppression and bacterial growth.
• Acid-suppression use results in gastric bacterial overgrowth of genera including Staphylococcus and Streptococcus.
• Full-column nonacid reflux is associated with greater concentrations of bacteria in the lung.
• Additional studies are needed to determine if acid suppression-related microflora changes predict clinical infection risk.
Rosen R et al. JAMA Pediatr. 2014 Oct 1;168(10):932-7.
Conclusions and Relevance:
Evidence to support the efficacy and safety of H2RAs
in infants and children is limited and of poor quality.
Well-designed placebo-controlled trials are needed
before thorough conclusions can be drawn
JAMA Pediatr August 18, 2014
Efficacy and Safety of Histamine-2 Receptor Antagonists

C.-T. Chiu et al. Aliment Pharmacol Ther 2013; 38: 1054–1064

• Recent observations of an alginate / antacid combination using MRI show formation of a raft at the air – meal interface after a liquid meal and formation of a clot between the EGJ and solid meal, exactly where the acid pocket would be located.
P J. Kahrilas et al. Am J Gastroenterol 2013; 108:1058–1064;

Ummarino D et al. J Pediatr Gastroenterol Nutr. 2014 Jul 30. [Epub ahead of print]
Mg-alginate plus simethicone seems to be more efficacious on GER symptom scores than thickened formula and reassurance with lifestyle changes alone.
Effect of Magnesium Alginate Plus Simethicone
on Gastroesophageal Reflux in Infants

Current evidence supports a possible association between GERD and respiratory symptoms, but casuality or temporal associations have not be established
Acid-reducing agents in infants and children: friend or foe? • Emerging data suggest acid reduction carried increasing risk of both
respiratory and gastrointestinal infections in children, possibly related to a change in microbiome.
If needed, other drugs, with less side effects, should be
considered
Take Home Messages
Menchise AN, Cohen MB. JAMA Pediatr. 2014 Oct 1;168(10):888-90.


• Allo stato attuale, in pediatria, nessun test diagnostico in
grado di dimostrare o escludere manifestazioni
respiratorie di MRGE.
• In presenza di sintomi respiratori e sintomi gastrointestinali
e’ giustificato un trial terapeutico
• In presenza di sintomi respiratori resistenti alle terapie
convenzionali, in assenza di sintomi GI, praticare pH-
impedenzometria.
• In caso di pH-impedenzometria negativa, in assenza di
sintomi GI, altre cause, differenti dalla MRGE, debbono
essere ricercate.
………..in sintesi
