alveolar corticotomies in orthodontic tooth movement ... · the use of corticotomy to correct...
TRANSCRIPT
International Journal of Advanced Health Sciences • Vol 1 Issue 11 • March 2015 12
Alveolar Corticotomies in Orthodontic Tooth Movement: Review Literature and Case ReportJay Sureshbhai Soni1, Avinash P Nawathe2, Hemal R Brahmkshatriya3, Lajja B Jha4
1Post Graduate Student, Department of Orthodontic and Dentofacial Orthopedics, KM Shah Dental College & Hospital, Vadodara, Gujarat, India, 2Professor, Department of Orthodontic and Dentofacial Orthopedics, KM Shah Dental College & Hospital, Vadodara, Gujarat, India, 3Post Graduate Student, Department of Oral and Maxillofacial Surgery, KM Shah Dental College & Hospital, Vadodara, Gujarat, India, 4Post Graduate Student, Department of Conservative Dentistry & Endodontics, Karnavati School of Dentistry And Hospital, Gandhinagar, Gujarat, India
Case Report
corticotomy to resolve malocclusion. He performed interdental alveolar corticotomy surgery, leaving the medullary bone intact, combined with a through and through osteotomy above the apex of the teeth.4 Generson et al.,5 in 1978, modified the Kole method by eliminating the subapical osteotomy and described treatment of open-bite malocclusion using selective alveolar decortication and orthodontics. Subsequently, multiple authors reported rapid tooth movement after alveolar decortication and explained the changes as “bony block” movement.6,7
In 2001, Wilcko et al.8 claimed that the decortication combined with augmentation grafting created greater alveolar volume, which eliminated bony dehiscences and fenestrations under most circumstances and likely enhanced the stability of the orthodontic treatment result. In the Wilcko protocol, fixed orthodontic appliances were placed and tooth movement was initiated during the week prior to the decortication surgery, and the orthodontic appliances were activated approximately every 2 weeks thereafter until orthodontic treatment was completed.9
Corticotomy-facilitated orthodontics has been indicated for non-extraction treatment of crowding, shortening
INTRODUCTION
Orthodontic treatment of late adolescent or adult patients can be challenging; often these patients request short treatments.1 If growth modification is no longer possible, surgical procedures might be necessary to attain treatment goals.2 With an osteotomy, both the cortical and trabecular bone is cut, followed by repositioning of the segments by the surgeon. Damage to the nerves and blood supply is a possible complication. For patients with mild dentoskeletal discrepancies, orthognathic surgery might not be a feasible option. To address these issues, other surgical techniques have been proposed. With a corticotomy, shallow perforations or cuts are made on the cortical alveolar bone only; the trabecular bone is left intact, in contrast to an osteotomy. Orthodontic force is applied shortly after surgery to produce the desired tooth movement and optimal bone remodeling. It has been claimed that orthodontic treatment progresses faster and that the results were more stable after a corticotomy, with minimal risk of complications.1,2
The use of corticotomy to correct malocclusion was first described by Bryan in 1892 and Cummingham in 18933, but it was Kole4 in 1959 who re-introduced alveolar
Corresponding Author: Dr. Jay Sureshbhai Soni, 11, Shyam Society, Tasiya Road, Mahavirnagar, Himmatnagar - 383 001, Gujarat, India. Phone: +91-9998222880, E-mail: [email protected]
ABSTRACT
Corticotomy and dental distraction provide an effective and short period to shorten the orthodontics movement especially in adolescent and adult patients. There are so many techniques provide corticotomy. The basic concept for corticotomy is to remove the cortical buccal bone to provide the osteoclastic activity that will start to resorb the bone periphery. The osteoclastic activity followed by the osteoblastic activity by new collagen fi bers formation at the site and converted into the immature bone. This will facilitate the rapid movement of the tooth. Here, we are presenting the case of corticotomy in the lower right back tooth region that was done by creating the wedge shape osteotomy.
Keywords: Alveolar remodeling, Corticotomy, Orthodontic tooth movement, Rapid Orthodontics, Regional acceleratory phenomenon
Alveolar Corticotomy Soni, et al.
13 International Journal of Advanced Health Sciences • Vol 1 Issue 11 • March 2015
treatment duration, borderline orthognathic surgery patients, extrusion of ankylosed teeth, intrusion of posterior teeth to close anterior open bites, faster canine retraction in extraction patients and impacted canines.1,2,7,9,10
The aim of this study was to surgically facilitated orthodontic treatment significantly increase the velocity of tooth movement of 47 and shorten treatment duration in healthy orthodontic patients, compared with conventional orthodontics.
CASE REPORT
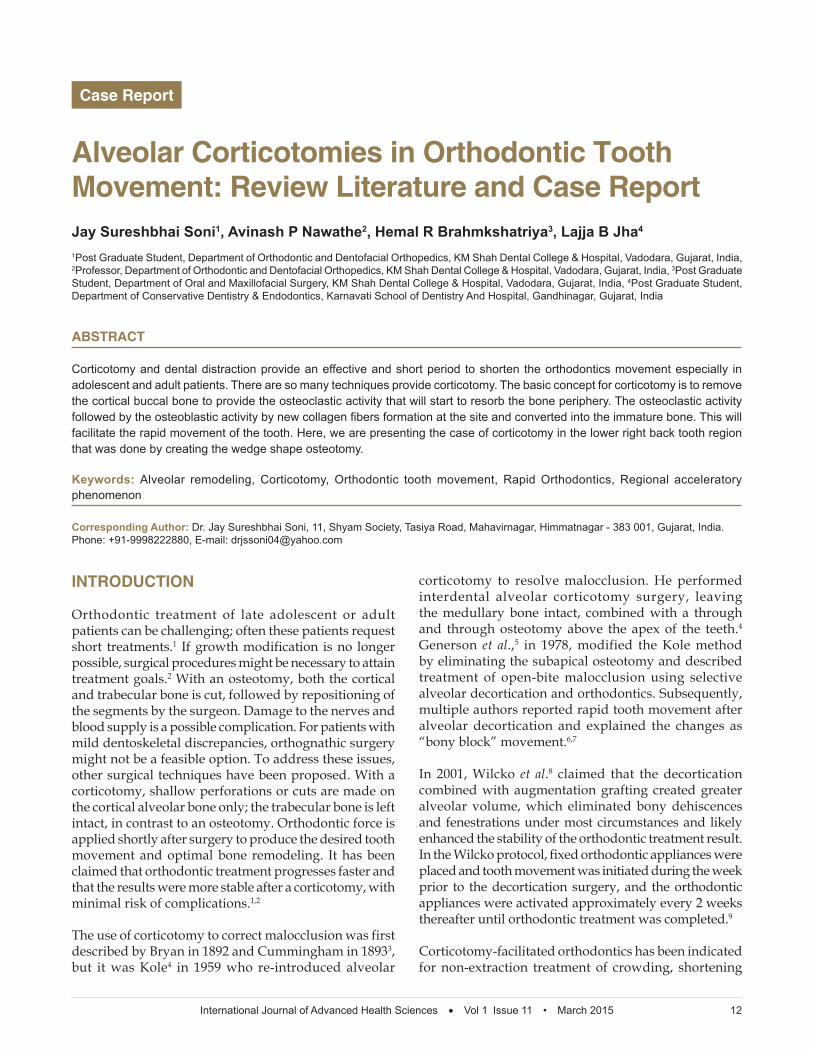
A 20-year-old female patient came to the department with the chief complaint of the crooked teeth. We found that the patient was undergone for extraction of lower right first molar (46) at the age of the 14 years as the tooth was not preserved with the endodontic treatment. We planned for orthodontic tooth movement of the second molar (47) at the site of the 46. We started with the orthodontic movement of all the other teeth to align them and to make them upright. By the end of the 1 year, we finished with all the other movements except 47. When we stared with the movement of 47, we found the soft tissue and bony interference over 46 alveolar ridge region (Figure 1). We preferred for the corticotomy over 46 tooth region for rapid orthodontic tooth movement.
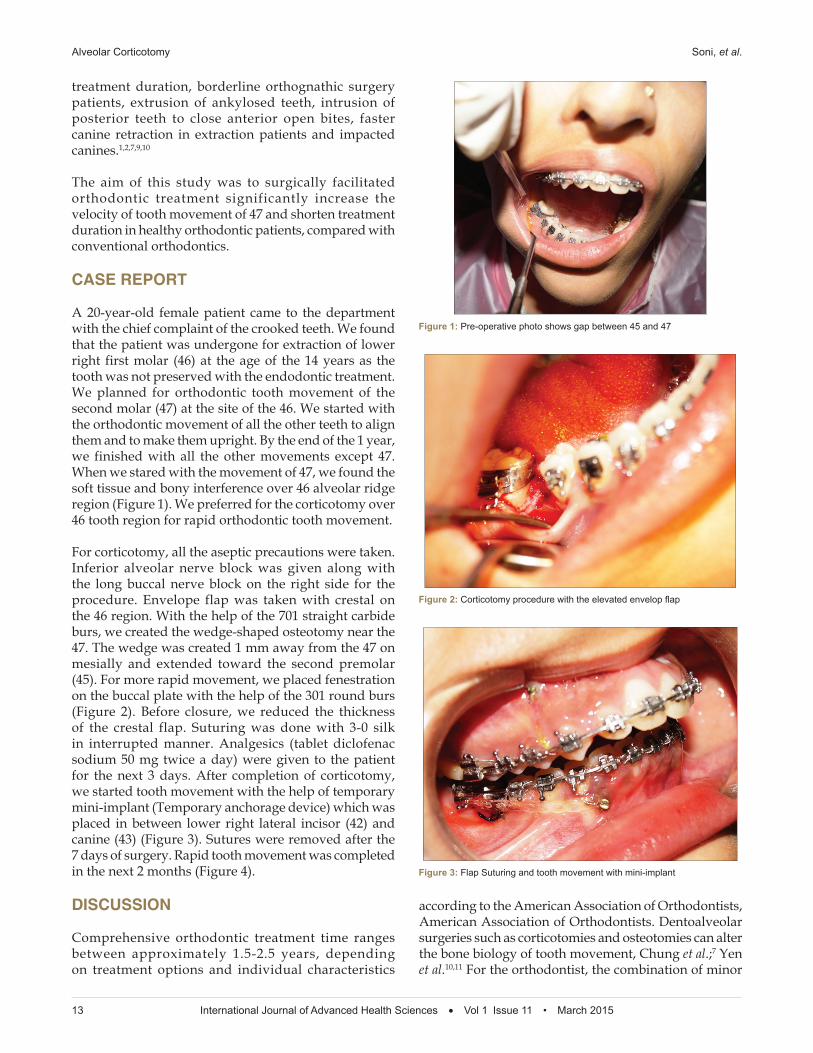
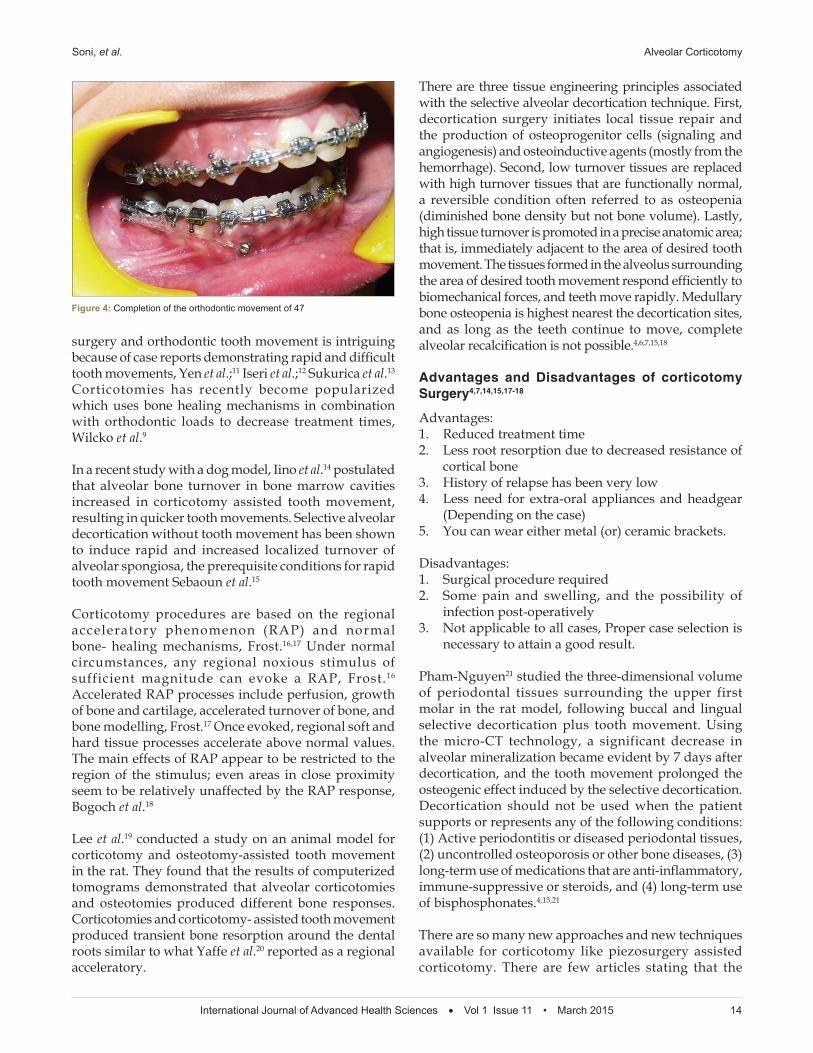
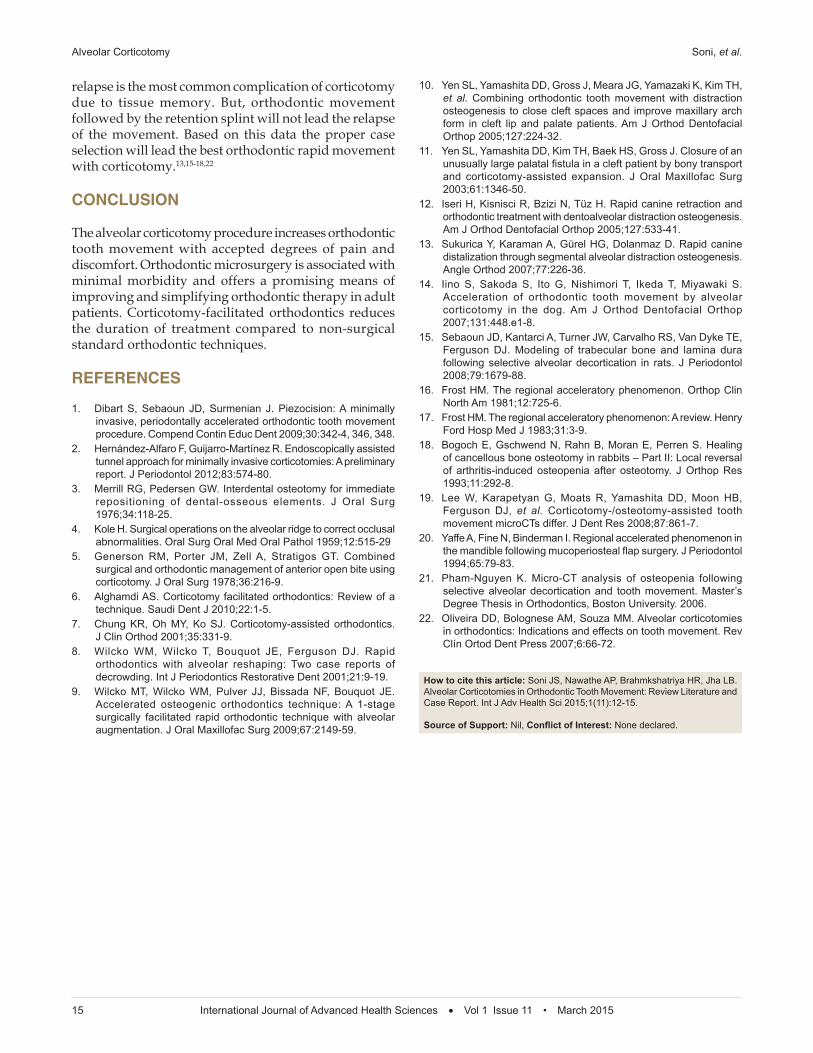
For corticotomy, all the aseptic precautions were taken. Inferior alveolar nerve block was given along with the long buccal nerve block on the right side for the procedure. Envelope flap was taken with crestal on the 46 region. With the help of the 701 straight carbide burs, we created the wedge-shaped osteotomy near the 47. The wedge was created 1 mm away from the 47 on mesially and extended toward the second premolar (45). For more rapid movement, we placed fenestration on the buccal plate with the help of the 301 round burs (Figure 2). Before closure, we reduced the thickness of the crestal flap. Suturing was done with 3-0 silk in interrupted manner. Analgesics (tablet diclofenac sodium 50 mg twice a day) were given to the patient for the next 3 days. After completion of corticotomy, we started tooth movement with the help of temporary mini-implant (Temporary anchorage device) which was placed in between lower right lateral incisor (42) and canine (43) (Figure 3). Sutures were removed after the 7 days of surgery. Rapid tooth movement was completed in the next 2 months (Figure 4).
DISCUSSION
Comprehensive orthodontic treatment time ranges between approximately 1.5-2.5 years, depending on treatment options and individual characteristics
according to the American Association of Orthodontists, American Association of Orthodontists. Dentoalveolar surgeries such as corticotomies and osteotomies can alter the bone biology of tooth movement, Chung et al.;7 Yen et al.10,11 For the orthodontist, the combination of minor
Figure 1: Pre-operative photo shows gap between 45 and 47
Figure 2: Corticotomy procedure with the elevated envelop fl ap
Figure 3: Flap Suturing and tooth movement with mini-implant
Soni, et al. Alveolar Corticotomy
International Journal of Advanced Health Sciences • Vol 1 Issue 11 • March 2015 14
surgery and orthodontic tooth movement is intriguing because of case reports demonstrating rapid and difficult tooth movements, Yen et al.;11 Iseri et al.;12 Sukurica et al.13 Corticotomies has recently become popularized which uses bone healing mechanisms in combination with orthodontic loads to decrease treatment times, Wilcko et al.9
In a recent study with a dog model, Iino et al.14 postulated that alveolar bone turnover in bone marrow cavities increased in corticotomy assisted tooth movement, resulting in quicker tooth movements. Selective alveolar decortication without tooth movement has been shown to induce rapid and increased localized turnover of alveolar spongiosa, the prerequisite conditions for rapid tooth movement Sebaoun et al.15
Corticotomy procedures are based on the regional acceleratory phenomenon (RAP) and normal bone- healing mechanisms, Frost.16,17 Under normal circumstances, any regional noxious stimulus of sufficient magnitude can evoke a RAP, Frost.16 Accelerated RAP processes include perfusion, growth of bone and cartilage, accelerated turnover of bone, and bone modelling, Frost.17 Once evoked, regional soft and hard tissue processes accelerate above normal values. The main effects of RAP appear to be restricted to the region of the stimulus; even areas in close proximity seem to be relatively unaffected by the RAP response, Bogoch et al.18
Lee et al.19 conducted a study on an animal model for corticotomy and osteotomy-assisted tooth movement in the rat. They found that the results of computerized tomograms demonstrated that alveolar corticotomies and osteotomies produced different bone responses. Corticotomies and corticotomy- assisted tooth movement produced transient bone resorption around the dental roots similar to what Yaffe et al.20 reported as a regional acceleratory.
There are three tissue engineering principles associated with the selective alveolar decortication technique. First, decortication surgery initiates local tissue repair and the production of osteoprogenitor cells (signaling and angiogenesis) and osteoinductive agents (mostly from the hemorrhage). Second, low turnover tissues are replaced with high turnover tissues that are functionally normal, a reversible condition often referred to as osteopenia (diminished bone density but not bone volume). Lastly, high tissue turnover is promoted in a precise anatomic area; that is, immediately adjacent to the area of desired tooth movement. The tissues formed in the alveolus surrounding the area of desired tooth movement respond efficiently to biomechanical forces, and teeth move rapidly. Medullary bone osteopenia is highest nearest the decortication sites, and as long as the teeth continue to move, complete alveolar recalcification is not possible.4,6,7,15,18
Advantages and Disadvantages of corticotomy Surgery4,7,14,15,17-18
Advantages:1. Reduced treatment time2. Less root resorption due to decreased resistance of
cortical bone3. History of relapse has been very low4. Less need for extra-oral appliances and headgear
(Depending on the case)5. You can wear either metal (or) ceramic brackets.
Disadvantages:1. Surgical procedure required2. Some pain and swelling, and the possibility of
infection post-operatively3. Not applicable to all cases, Proper case selection is
necessary to attain a good result.
Pham-Nguyen21 studied the three-dimensional volume of periodontal tissues surrounding the upper first molar in the rat model, following buccal and lingual selective decortication plus tooth movement. Using the micro-CT technology, a significant decrease in alveolar mineralization became evident by 7 days after decortication, and the tooth movement prolonged the osteogenic effect induced by the selective decortication. Decortication should not be used when the patient supports or represents any of the following conditions: (1) Active periodontitis or diseased periodontal tissues, (2) uncontrolled osteoporosis or other bone diseases, (3) long-term use of medications that are anti-inflammatory, immune-suppressive or steroids, and (4) long-term use of bisphosphonates.4,13,21
There are so many new approaches and new techniques available for corticotomy like piezosurgery assisted corticotomy. There are few articles stating that the
Figure 4: Completion of the orthodontic movement of 47
Alveolar Corticotomy Soni, et al.
15 International Journal of Advanced Health Sciences • Vol 1 Issue 11 • March 2015
relapse is the most common complication of corticotomy due to tissue memory. But, orthodontic movement followed by the retention splint will not lead the relapse of the movement. Based on this data the proper case selection will lead the best orthodontic rapid movement with corticotomy.13,15-18,22
CONCLUSION
The alveolar corticotomy procedure increases orthodontic tooth movement with accepted degrees of pain and discomfort. Orthodontic microsurgery is associated with minimal morbidity and offers a promising means of improving and simplifying orthodontic therapy in adult patients. Corticotomy-facilitated orthodontics reduces the duration of treatment compared to non-surgical standard orthodontic techniques.
REFERENCES
1. Dibart S, Sebaoun JD, Surmenian J. Piezocision: A minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend Contin Educ Dent 2009;30:342-4, 346, 348.
2. Hernández-Alfaro F, Guijarro-Martínez R. Endoscopically assisted tunnel approach for minimally invasive corticotomies: A preliminary report. J Periodontol 2012;83:574-80.
3. Merrill RG, Pedersen GW. Interdental osteotomy for immediate repositioning of dental-osseous elements. J Oral Surg 1976;34:118-25.
4. Kole H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral Surg Oral Med Oral Pathol 1959;12:515-29
5. Generson RM, Porter JM, Zell A, Stratigos GT. Combined surgical and orthodontic management of anterior open bite using corticotomy. J Oral Surg 1978;36:216-9.
6. Alghamdi AS. Corticotomy facilitated orthodontics: Review of a technique. Saudi Dent J 2010;22:1-5.
7. Chung KR, Oh MY, Ko SJ. Corticotomy-assisted orthodontics. J Clin Orthod 2001;35:331-9.
8. Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: Two case reports of decrowding. Int J Periodontics Restorative Dent 2001;21:9-19.
9. Wilcko MT, Wilcko WM, Pulver JJ, Bissada NF, Bouquot JE. Accelerated osteogenic orthodontics technique: A 1-stage surgically facilitated rapid orthodontic technique with alveolar augmentation. J Oral Maxillofac Surg 2009;67:2149-59.
10. Yen SL, Yamashita DD, Gross J, Meara JG, Yamazaki K, Kim TH, et al. Combining orthodontic tooth movement with distraction osteogenesis to close cleft spaces and improve maxillary arch form in cleft lip and palate patients. Am J Orthod Dentofacial Orthop 2005;127:224-32.
11. Yen SL, Yamashita DD, Kim TH, Baek HS, Gross J. Closure of an unusually large palatal fi stula in a cleft patient by bony transport and corticotomy-assisted expansion. J Oral Maxillofac Surg 2003;61:1346-50.
12. Iseri H, Kisnisci R, Bzizi N, Tüz H. Rapid canine retraction and orthodontic treatment with dentoalveolar distraction osteogenesis. Am J Orthod Dentofacial Orthop 2005;127:533-41.
13. Sukurica Y, Karaman A, Gürel HG, Dolanmaz D. Rapid canine distalization through segmental alveolar distraction osteogenesis. Angle Orthod 2007;77:226-36.
14. Iino S, Sakoda S, Ito G, Nishimori T, Ikeda T, Miyawaki S. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am J Orthod Dentofacial Orthop 2007;131:448.e1-8.
15. Sebaoun JD, Kantarci A, Turner JW, Carvalho RS, Van Dyke TE, Ferguson DJ. Modeling of trabecular bone and lamina dura following selective alveolar decortication in rats. J Periodontol 2008;79:1679-88.
16. Frost HM. The regional acceleratory phenomenon. Orthop Clin North Am 1981;12:725-6.
17. Frost HM. The regional acceleratory phenomenon: A review. Henry Ford Hosp Med J 1983;31:3-9.
18. Bogoch E, Gschwend N, Rahn B, Moran E, Perren S. Healing of cancellous bone osteotomy in rabbits – Part II: Local reversal of arthritis-induced osteopenia after osteotomy. J Orthop Res 1993;11:292-8.
19. Lee W, Karapetyan G, Moats R, Yamashita DD, Moon HB, Ferguson DJ, et al. Corticotomy-/osteotomy-assisted tooth movement microCTs differ. J Dent Res 2008;87:861-7.
20. Yaffe A, Fine N, Binderman I. Regional accelerated phenomenon in the mandible following mucoperiosteal fl ap surgery. J Periodontol 1994;65:79-83.
21. Pham-Nguyen K. Micro-CT analysis of osteopenia following selective alveolar decortication and tooth movement. Master’s Degree Thesis in Orthodontics, Boston University. 2006.
22. Oliveira DD, Bolognese AM, Souza MM. Alveolar corticotomies in orthodontics: Indications and effects on tooth movement. Rev Clín Ortod Dent Press 2007;6:66-72.
How to cite this article: Soni JS, Nawathe AP, Brahmkshatriya HR, Jha LB. Alveolar Corticotomies in Orthodontic Tooth Movement: Review Literature and Case Report. Int J Adv Health Sci 2015;1(11):12-15.
Source of Support: Nil, Confl ict of Interest: None declared.