aldose reductase inhibitors and diabetic complications
TRANSCRIPT

Aldose Reductase Inhibitors and Diabetic Complications
PHILIP RASKIN, M.D. JULIO ROSENSTOCK, M.D.
Dallas, Texas
From the Department of Medicine, University of Texas Health Science Center at Dallas, South- western Medical School, Dallas, Texas. Re- quests for repritns should be addressed to Dr. Philip Raskin, Department of Internal Medicine, University of Texas Health Science Center at Dallas, 5323 Harry Hines Boulevard, Dallas, Tex- as 75235. Manuscript submitted December 17, 1988, and accepted February 17, 1987.
A new series of compounds, the aldose reductase inhibitors, has recently been viewed as potentially useful in the area of medicine. These com- pounds, which are still only experimental and in various stages of development, may play an important role in the management of the complications related to diabetes mellitus. Furthermore, the financial impact of the possible widespread use of these agents in most diabetic subjects has prompted very active research by the drug industry. As of this date, there are at least five pharmaceutical companies in the process of investigating the efficacy and safety of different aldose reductase inhibitor drugs. The product that gets to the marketplace first will result in high profits for that company.
Although the idea of using aldose reductase inhibitors in patients with diabetes is a relatively recent one, interest in the polyol pathway is not. it was Mann [I] in 1946 who discovered that the main sugar in seminal fluid was fructose and that the fructose in seminal fluid was derived from blood glucose. Furthermore, there was a relationship between the level of blood glucose and the seminal fluid fructose concentration [2]. Hers [3] was the first to demonstrate that seminal fructose was formed via the polyol pathway.
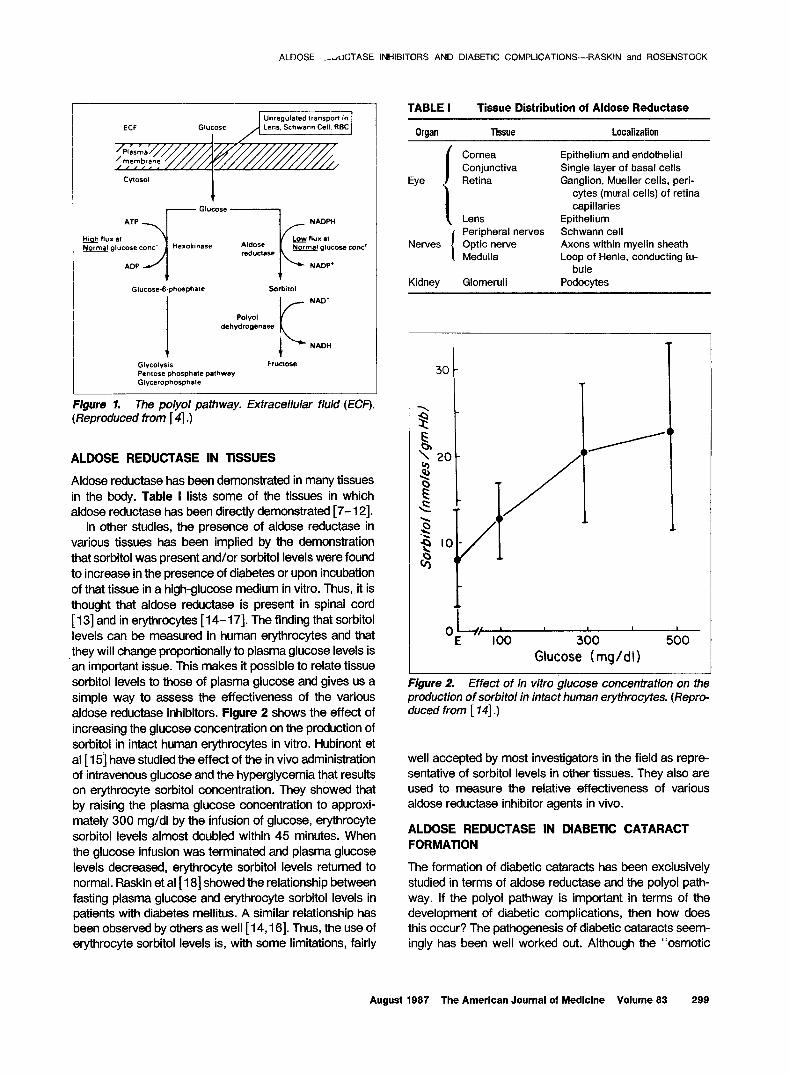
Figure 1 shows the polyol pathway [4]. Aldose reductase (alditol: NADPH oxidoreductase, EC 1.1.1.2.1) is the rate-limiting enzyme of this pathway. It catalyzes the reduction of hexoses to their respective sugar alcohol (e.g., glucose to sorbitol and galactose to galactitol or its other name, dulcitol); sorbitol is then oxidized by the second enzyme of this pathway, polyol (sorbitol) dehydrogenase (i-iditol dehydrogenase EC 1-I. 1.14). Sorbitol dehydrogenase has broad substrate specificities for many sugar alcohols, additionally converting xylitol to ~xylulose and ribitol to D-ribulose. However, it has limited ability to further metabolize dulcitol, leading to enhanced accumulation of this sugar alcohol in galactosemia [5]. Generally, hexoses including glucose are poor sub- strates for aldose reductase. Aldose reductase has a high Michaelis constant (70 to 150 mM) for glucose and galactose; thus, when levels of the hexose are elevated, as in diabetes with hyperglycemia or in hyperga- lactosemia, significant polyol formation can occur [5].
Over the past decade, there has been considerable interest in the relationship between the polyol pathway and the small blood vessel complications of diabetes mellitus [5]. If this enzymatic pathway does serve as some pathogenic mechanism in all or some of the diabetic complications, then the inhibition of aldose reductase may represent a direct pharmacologic approach in the treatment of certain diabetic com- plications. This approach is distinct and separate from treatments de- signed to improve blood glucose levels [S].
298 August 1987 The American Journal of Medicine Volume 83
ALDOSE .-YuCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
Unregulated transpon in Lens. Schwenn Cell. RBC
Figure 1. The polyol pathway. Extracellular fluid (ECF). (Reproduced from [ 41.)
ALDOSE REDUCTASE IN TlSSUES
Aldose reductase has been demonstrated in many tissues in the body. Table I lists some of the tissues in which aldose reductase has been directly demonstrated [7-l 21.
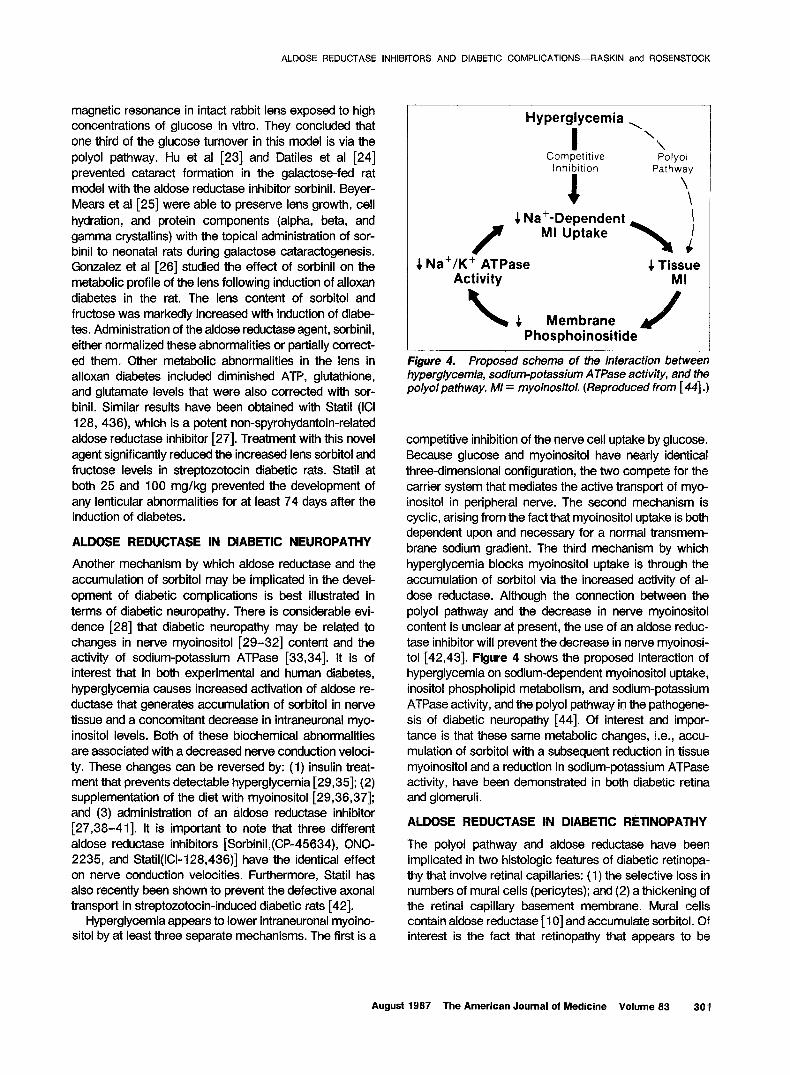
In other studies, the presence of aldose reductase in various tissues has been implied by the demonstration that sorbitol was present and/or sorbitol levels were found to increase in the presence of diabetes or upon incubation of that tissue in a high-glucose medium in vitro. Thus, it is thought that aldose reductase is present in spinal cord [ 131 and in erythrocytes [ 14- 171. The finding that sorbitol levels can be measured in human erythrocytes and that ,they will change proportionally to plasma glucose levels is an important issue. This makes it possible to relate tissue sorbitol levels to those of plasma glucose and gives us a simple way to assess the effectiveness of the various aldose reductase inhibitors. Figure 2 shows the effect of increasing the glucose concentration on the production of sorbitol in intact human erythrocytes in vitro. Hubinont et al [ 151 have studied the effect of the in vivo administration of intravenous glucose and the hyperglycemia that results on erythrocyte sorbitol concentration. They showed that by raising the plasma glucose concentration to approxi- mately 300 mg/dl by the infusion of glucose, erythrocyte sorbitol levels almost doubled within 45 minutes. When the glucose infusion was terminated and plasma glucose levels decreased, erythrocyte sorbitol levels returned to normal. Raskin et al [ 181 showed the relationship between fasting plasma glucose and erythrocyte sorbitol levels in patients with diabetes mellitus. A similar relationship has been observed by others as well [ 14,161. Thus, the use of erythrocyte sorbitol levels is, with some limitations, fairly
TABLE I Tissue Distribution of Aldose Reductase
Organ Tissue
Eye
Cornea Conjunctiva Retina
I Lens
Nerves Peripheral nerves Schwann cell Optic nerve Axons within myelin sheath Medulla Loop of Henle, conducting tu-
Kidney Glomeruli
Localization
Epithelium and endothelial Single layer of basal cells Ganglion, Mueller cells, peri-
cytes (mural cells) of retina capillaries
Epithelium
bule Podocytes
0 L ’ I I I E 100 300 500
Glucose (mg/dl)
Figure 2. Effect of in vitro glucose concentration on the production of sorbitol in intact human erythrocytes. (Repro duced from [ 141.)
well accepted by most investigators in the field as repre- sentative of sorbitol levels in other tissues. They also are used to measure the relative effectiveness of various aldose reductase inhibitor agents in vivo.
ALDOSE REDUCTASE IN DIABETIC CATARACT FORMATION
The formation of diabetic cataracts has been exclusively studied in terms of aldose reductase and the polyol path- way. If the polyol pathway is important in terms of the development of diabetic complications, then how does this occur? The pathogenesis of diabetic cataracts seem- ingly has been well worked out. Although the “osmotic
August 1987 The American Journal of Medicine Volume 83 299

ALDOSE REDUCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
Diabetic Cataract Development
Lenticular Changes
Normal Vacuolar Stage Cortical Cataract Nuclear Cataract
Biochemical Changes
Glucose K7
Glucose v
Glucose
Water-
Ygure 3. Schematic design of biochemical changes that occur during the development of a sugar cataract. Actual pictures of in vitro cataract formation. GSH = reduced glutathione; AA = amino acids. (Reproduced from [ 2 I] .)
theory” seems an appropriate explanation for the devel- opment of diabetic and galactosemic cataracts, we are not certain that it is operative in tissues other than the lens. The osmotic theory has been promulgated by Kino- shita and co-workers [19,20]. Stated simply, the theory suggests that the intracellular accumulation of polyols initiated by aldose reductase leads to an influx of water that results in permeability changes and eventually leads to a loss of cellular integrity. Figure 3 [21] shows a schematic of biochemical changes that occur during the development of a sugar cataract as well as pictures of actual in vitro cataract formation that correlate with the proposed biochemical changes. The increase in osmolali- ty caused by the accumulation of sorbitol and fructose draws water into the lens fibers, causing them to swell. The swelling has adverse effects since it increases the permeability to substances normally retained in the lens at concentrations higher than surrounding intraocular fluids. Thus, the concentrations of potassium, amino acids, glu- tathione, inositol, and ATP begin to decrease, and sodium and chlorine ions slowly begin to build up. As the process continues, a secondary osmotic change results from the electrolyte change of increased sodium and chlorine ions;
eventually the increases in these electrolytes become the predominant factor in lens swelling. The lens membranes become freely permeable to all substances other than the larger proteins. In this later stage, swelling is explained by the Donnan principle. It is accompanied by the appear- ance of the dense nuclear cataracts. In the formation of diabetic cataracts, the earliest visible change is the ap- pearance of swollen lens fibers caused by an increase in lens hydration. The swollen lens fibers eventually rupture with the liquification of the fibers, resulting in vacuole formation. In our judgment, the only tissue in which os- motic changes play any role is in the lens relative to cataract formation. In other tissues, the amount of water influx is insufficient to cause tissue damage. Other patho- genic mechanisms seem to be more important. These changes will be discussed subsequently.
The inhibition of in vitro cataract formation is a well- established method for evaluating the effectiveness and relative potency of aldose reductase inhibitors. There are considerable experimental data to support the effect of aldose reductase inhibitor on sugar cataracts. To begin with, Gonzalez et al [22] were able to measure the metabolic flux through the polyol pathway using nuclear
300 August 1987 The American Journal of Medicine Volume 83
magnetic resonance in intact rabbit lens exposed to high concentrations of glucose in vitro. They concluded that one third of the glucose turnover in this model is via the polyol pathway. Hu et al [23] and Datiles et al [24] prevented cataract formation in the galactose-fed rat model with the aldose reductase inhibitor sorbinil. Beyer- Mears et al [25] were able to preserve lens growth, cell hydration, and protein components (alpha, beta, and gamma crystallins) with the topical administration of sor- binil to neonatal rats during galactose cataractogenesis. Gonzalez et al [26] studied the effect of sorbinil on the metabolic profile of the lens following induction of alloxan diabetes in the rat. The lens content of sorbitol and fructose was markedly increased with induction of diabe- tes. Administration of the aldose reductase agent, sorbinil, either normalized these abnormalities or partially correct- ed them. Other metabolic abnormalities in the lens in alloxan diabetes included diminished ATP, glutathione, and glutamate levels that were also corrected with sor- binil. Similar results have been obtained with Statil (ICt 128, 436), which is a potent non-spyrohydantoin-related aldose reductase inhibitor [27]. Treatment with this novel agent significantly reduced the increased lens sorbitol and fructose levels in streptozotocin diabetic rats. Statil at both 25 and 100 mg/kg prevented the development of any lenticular abnormalities for at least 74 days after the induction of diabetes.
ALDOSE REDUCTASE IN DtABETtC NEUROPATHY
Another mechanism by which aldose reductase and the accumulation of sorbitol may be implicated in the devel- opment of diabetic complications is best illustrated in terms of diabetic neuropathy. There is considerable evi- dence [28] that diabetic neuropathy may be related to changes in nerve myoinositol [29-321 content and the activity of sodium-potassium ATPase [33,34]. It is of interest that in both experimental and human diabetes, hyperglycemia causes increased activation of aldose re- ductase that generates accumulation of sorbitol in nerve tissue and a concomitant decrease in intraneuronal myo- inositol levels. Both of these biochemical abnormalities are associated with a decreased nerve conduction veloci- ty. These changes can be reversed by: (1) insulin treat- ment that prevents detectable hyperglycemia [29,35]; (2) supplementation of the diet with myoinositol [29,36,37]; and (3) administration of an akfose reductase inhibitor [27,38-411. It is important to note that three different aldose reductase inhibitors [Sorbinil,(CP-45634), ONO- 2235, and Statil(lCl-128,436)] have the identical effect on nerve conduction velocities. Furthermore, Statil has also recently been shown to prevent the defective axonal transport in streptozotocin-induced diabetic rats [42].
Hyperglycemia appears to lower intraneuronal myoino- sitol by at least three separate mechanisms. The first is a
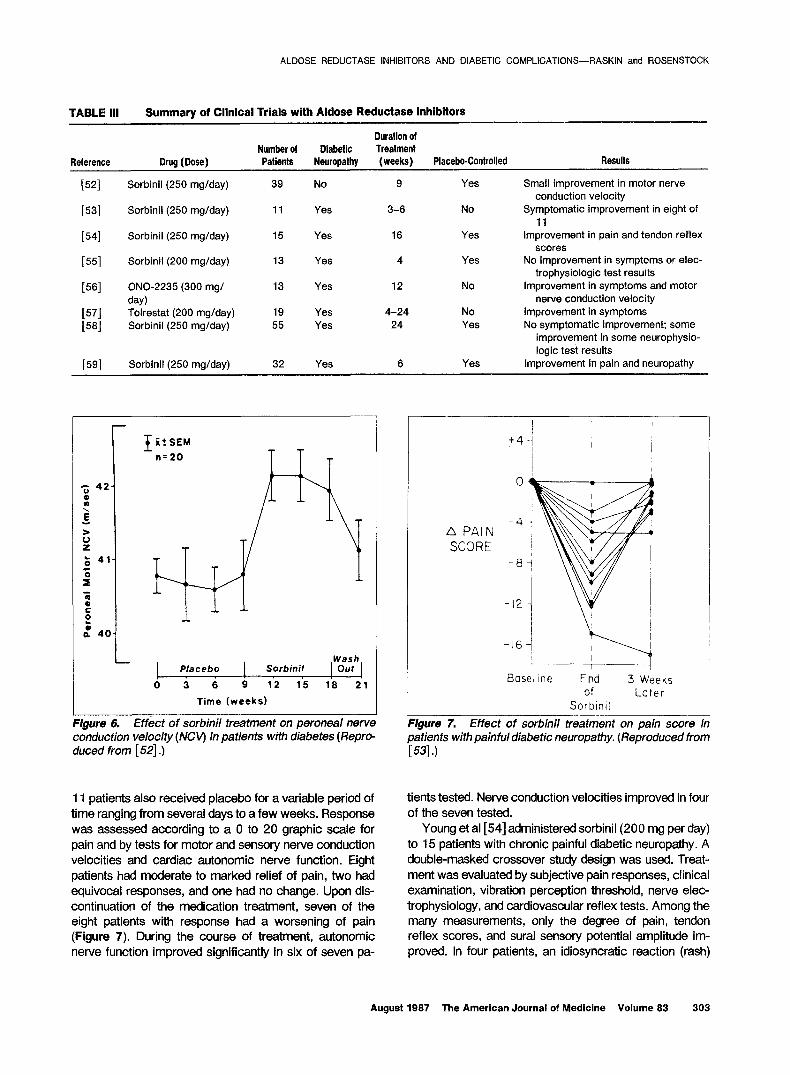
Hyperglycemia ,
I \
\ Competitive Polyol
Inhibition
1
Pathway
\
\
4 Na+-Dependent I MI Uptake
i 4 Na+/K+ ATPase 4 Tissue
Activity MI
\ 4 Membrane Phosphoinositide
ALDOSE REDuCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
Figure 4. Proposed scheme of the interaction between hyperglycemia, sodium-potassium ATPase activity, and the polyolpathway. MI = myoinositol. (Reproduced from [ 441.)
competitive inhibition of the nerve cell uptake by glucose. Because glucose and myoinositol have nearly identical three-dimensional configuration, the two compete for the carrier system that mediates the active transport of myo- inositol in peripheral nerve. The second mechanism is cyclic, arising from the fact that myoinositol uptake is both dependent upon and necessary for a normal transmem- brane sodium gradient. The third mechanism by which hyperglycemia blocks myoinositol uptake is through the accumulation of sorbitol via the increased activity of al- dose reductase. Although the connection between the polyol pathway and the decrease in nerve myoinositol content is unclear at present, the use of an aldose reduc- tase inhibitor will prevent the decrease in nerve myoinosi- tol [42,43]. Figure 4 shows the proposed interaction of hyperglycemia on sodium-dependent myoinositol uptake, inositol phospholipid metabolism, and sodium-potassium ATPase activity, and the polyol pathway in the pathogene- sis of diabetic neuropathy [44]. Of interest and impor- tance is that these same metabolic changes, i.e., accu- mulation of sorbitol with a subsequent reduction in tissue myoinositol and a reduction in sodium-potassium ATPase activity, have been demonstrated in both diabetic retina and glomeruli.
ALDOSE REDUCTASE IN DtABETtC RETtNOPATHY
The polyol pathway and aldose reductase have been implicated in two histologic features of diabetic retinopa- thy that involve retinal capillaries: (1) the selective loss in numbers of mural cells (pericytes); and (2) a thickening of the retinal capillary basement membrane. Mural cells contain aldose reductase [lo] and accumulate sorbitol. Of interest is the fact that retinopathy that appears to be
August 1987 The American Journal of Medicine Volume 83 301

-- 28 weekr 44 week8
0 Control
m Gelectore
[PPI Gslsctoes l rorbinit I
Figure 5. Effect of sorbinil treatment on retinal capillary basement membrane (BMA) width in galactose-fed fats. (Reproduced from [ 4 73 .)
similar to diabetic retinopathy in humans develops in dogs [45] and rats [46,47] made galactosemic by the feeding of a high-galactose diet. The retinopathy in galactosemic dogs [45] is marked by saccular capillary aneurysms, hemorrhages, nonperfused or acellular vessels, tortuous hypertrophic capillaries, loss of capillary pericytes, and other lesions typical of diabetic patients. Furthermore, in both galactose-fed dogs [45] and rats [46,47] and in experimental diabetes in rats [48], retinal capillaries de- veloped a thickening of the basement membrane. Admin- istration of sorbinil to galactose-fed rats [47] (Figure 5) or alconil [48] to diabetic rats prevents the thickening of retinal capillary basement membrane.
ALDOSE REDUCTASE IN DIABETIC NEPHROPATHY
The role of aldose reductase in the pathogenesis of exper- imental diabetic nephropathy has only recently been in- vestigated. Beyer-Mears [49] recently measured polyols in glomeruli isolated from control and streptozotocin- induced diabetic rats. Compared with control (nondiabet- ic) animals, the polyol content was increased lo-fold at six weeks following the induction of diabetes, and the myoinositol content was significantly reduced in diabetic glomeruli nine weeks following,the induction of diabetes. Administration of the aldose reductase inhibitor sorbinil prevented both the accumulation of polyol and the reduc- tion of myoinositol. Sorbinil has also been shown to prevent renal hypettrophy in galactose-fed rats [50] and to diminish proteinuria in streptozotocin-induced diabetic rats [5 I].
TABLE II Development of Aldose Reductase Inhibitor Drugs
Drua Name Pharmaceutical
ComPanv Status
ALDOSE REDUCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
ICI-128,436 Statil Stuart Pharma- ceuticals, Im- perial Chemi- cal Industries (United King- dom)
Tolrestat Ayers&American Home Prod- ucts
Phase 213 stud- ies (neuropa- thy) well un- derway
AY-27,773
CP-45,634 Sorbinil Pfizer Laborato- ries
ONO-2235 - ON0 Pharma- ceuticals (Ja- w)
Some phase 21 3 studies (neuropathy) have been completed; retinopathy trial ongoing
Some phase 21 3 studies (neuropathy) have been completed; retinopathy trial ongoing
Several open clinical trials (neuropathy) completed in Japan
ALDOSE REDUCTASE IN CLINICAL TRIALS
Clinical trials with the various aldose reductase inhibitor agents are now underway. Table II lists the various aldose reductase agents that are now in various stages of devel- opment.
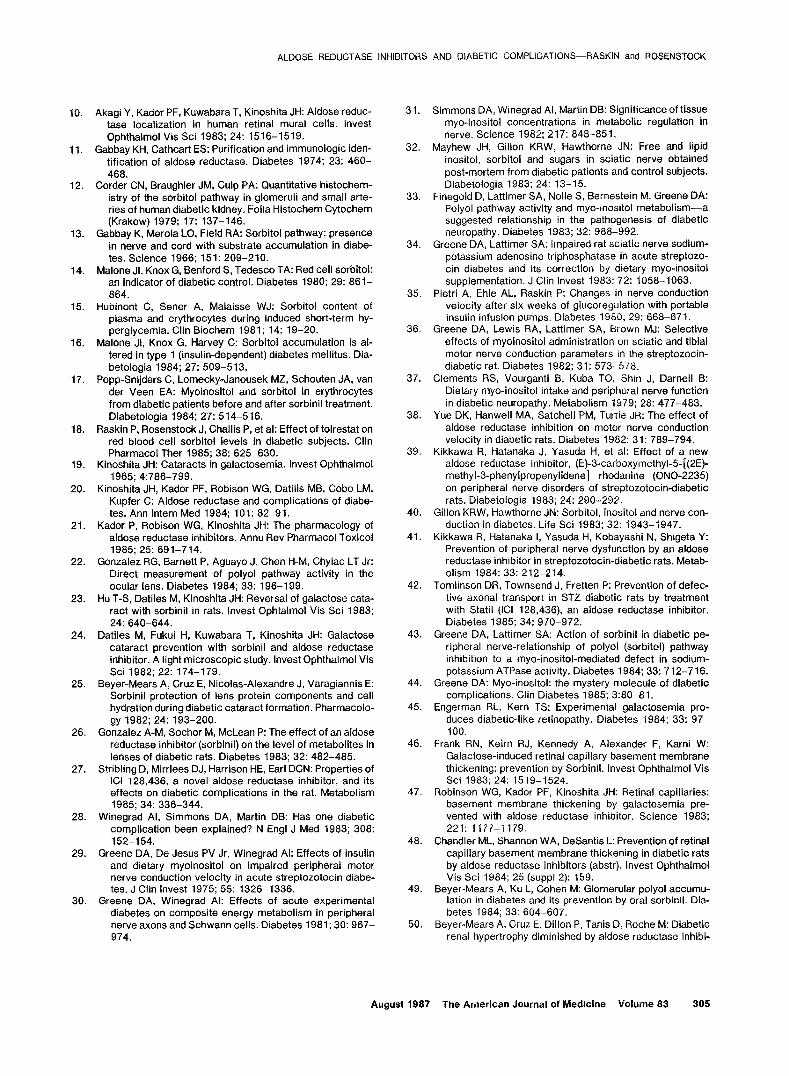
The clinical trials involving the use of aldose reductase inhibitors have been limited to studies involving the use of these various agents for the treatment of diabetic neurop- athy (Table Ill). Judzewitsch et al [52] conducted a dou- ble-masked, placebo crossover trial in 39 diabetic pa- tients without clinical evidence of diabetic neuropathy. During the nine-week study period, each patient received either placebo or a single daily dose of 250 mg of sorbinil. During the nine weeks of treatment with sorbinil, nerve conduction velocity was greater than during a nine-week period of placebo therapy for all three nerves tested (Figure 6). There were no changes in glycemic control during the study. Nerve conduction velocity for all three nerves declined significantly within three weeks after cessation of the drug. As can be seen from Figure 6, the improvement in nerve conduction velocity was small, approximately 1 meter/second. Such small changes hardly warrant an enthusiastic response.
Jaspan et al [53] treated 11 patients with severe pain- ful diabetic neuropathy with a single daily dose of 250 mg of sorbinil for a period of three to six weeks. Eight of the
302 August 1987 The American Journal of Medicine Volume 83
ALDOSE REDUCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
TABLE III
Reference
Summary of Clinical Trials with Aldose Reductase Inhibitors
Duration of Number 01 Diabetic Treatment
Drug (Dose) Patients Neuropalhy (weeks) Placebo-Controlled Results
[521
1531
[541
[551
WI
t;i;
[591
Sorbinil (250 mglday)
Sorbinil (250 mg/day)
Sorbinil (250 mg/day)
Sorbinil (200 mg/day)
ONO-2235 (300 mg/ day) Tolrestat (200 mg/day) Sorbinil (250 mg/day)
Sorbinil(250 mg/day)
39 No
11 Yes
15 Yes
13 Yes
13 Yes
19 Yes 55 Yes
32 Yes 6
9
3-6
16
4
12
4-24 24
Yes
No
Yes
Yes
No
No Yes
Yes
Small improvement in motor nerve conduction velocity
Symptomatic improvement in eight of 11
improvement in pain and tendon reflex scores
No improvement in symptoms or elec- trophysiologic test results
Improvement in symptoms and motor nerve conduction velocity
Improvement in symptoms No symptomatic improvement; some
improvement in some neurophysio- logic test results
Improvement in pain and neuropathy
+SEM
n- 20
Wash Placebo Sorbinil 1 Out
0 3 6 9 12 15 18 21
Time (weeks)
Figure 6. Effect of sorbinil treatment on peroneal nerve Figure 7. Effect of sorbinil treatment on pain score in conduction velocity (/VCVj in patients with diabetes (Repro patients with painful diabetic neuropathy. (Reproduced from duced from [ 5.21.) L531.1
11 patients also received placebo for a variable period of time ranging from several days to a few weeks. Response was assessed according to a 0 to 20 graphic scale for pain and by tests for motor and sensory nerve conduction velocities and cardiac autonomic nerve function. Eight patients had moderate to marked relief of pain, two had equivocal responses, and one had no change. Upon dis- continuation of the medication treatment, seven of the eight patients with response had a worsening of pain (Figure 7). During the course of treatment, autonomic nerve function improved significantly in six of seven pa-
A PAIN SCORE
-a
-16
Base1 Ine End 3 Weeks of Later
Sorbrnil
tients tested. Nerve conduction velocities improved in four of the seven tested.
Young et al [54] administered sorbinil(200 mg per day) to 15 patients with chronic painful diabetic neuropathy. A double-masked crossover study design was used. Treat- ment was evaluated by subjective pain responses, clinical examination, vibration perception threshold, nerve elec- trophysiology, and cardiovascular reflex tests. Among the many measurements, only the degree of pain, tendon reflex scores, and sural sensory potential amplitude im- proved. In four patients, an idiosyncratic reaction (rash)
August 1987 The American Journal of Medicine Volume 83 303

ALDOSE REDUCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
developed that rapidly disappeared upon termination of the drug treatment. It is important to note that use of the aldose reductase inhibitor drug sorbinil has been associ- ated with an alarmingly high incidence of side effects. These side effects are primarily skin lesions that are most likely related to the hydantoin structure of the drug. Stud- ies are now underway to evaluate if a lower initial dose of sorbinil will be effective in reducing the high incidence of side effects.
Lewin et al [55] administered sorbinil 200 mg daily for four weeks in 13 patients with symptomatic diabetic neuropathy. A double-masked placebo crossover study design was used. No beneficial effects of the sorbinil on nerve conduction velocities, abnormal autonomic nervous system function, or symptoms of painful neuropathy were observed. As pointed out by the authors, the population studied was older with longer duration of diabetes than in previous trials, and the study period was very short.
Two other studies, although quite preliminary, are worth mentioning. The first by Hotta et al [56] used a 300 mg daily dose of the aldose reductase inhibitor drug, ONO- 2235, in 13 patients with painful diabetic neuropathy. The drug was given for 12 weeks without any placebo control. Significant improvement in motor nerve conduction ve- locity in the ulnar nerve was observed over the 12-week treatment period. The improvement in electrophysiologic studies as well as those of subjective symptoms (pain and numbness) correlated with the reduction of erythrocyte sorbitol levels. Koglin et al [57] administered tolrestat in a dose of 200 mg per day to 19 patients with painful or paresthetic diabetic distal, symmetric peripheral neuropa- thy. They reported a marked improvement in symptoms in a large proportion of their patients. In fact, of the eight patients who had been treated for 24 weeks, seven reported improvement. Unfortunately, there was no pla- cebo control in this study. Fagius et al [58] studied the effect of a 250 mg daily dose of sorbinil in patients with symptomatic diabetic polyneuropathy during a six-month
double-masked placebo-controlled trial. There was no improvement in the symptoms of diabetic neuropathy in those patients treated with sorbinil. There were, however, some improvements noted in the results of three of nine neurophysiologic tests and one of five tests of autonomic nerve function.
Finally, Rosenstock et al [59] have recently studied the short-term effect of sorbinil in 32 patients with severe painful diabetic neuropathy unresponsive to conventional analgesic and tricyclic therapy. A double-masked ran- domized study design was used. Patients received either placebo or 250 mg per day of sorbinil. Assessment was made using a 20-point self-administered neuropathy and pain symptom score. Pain scores and overall neuropathy improved after the six-week study in the sorbinil-treated group as compared with those patients who received placebo. They concluded, however, that longer studies will be required to assess the full effect of aldose reduc- tase inhibitors, preferably in patients with less advanced diabetic neuropathy.
CONCLUSION
Aldose reductase inhibitors, from a theoretic perspective, seem to offer promise as possible agents for the treat- ment or even the prevention of the microvascular compli- cations of diabetes. Although considerable theoretic data are available to support their effectiveness in experimen- tal diabetes, there have been relatively few studies in humans. Those that have been performed often were poorly designed, i.e., lacked an appropriate control group, or were carried out in patients with markedly advanced disease. Longer prospective controlled trials are certainly required before these compounds can be advocated on a routine basis. Our bias is, however, that the real utility of these drugs will be as agents for the prevention of the complications of diabetes in some tissues (nerve and retina seem the most likely candidates) rather than as treatment for advanced disease.
REFERENCES
1. Mann T: Studies on the metabolism of semen. 3. Fructose as a normal constituent of seminal plasma: site of formation and function of fructose in semen. Biochem J 1946; 40: 481-491.
2. Mann T, Parsons U: Studies on the metabolism of semen. 6. Role of hormones, effect of castration, hypophysectomy and diabetes: relation between blood glucose and seminal fructose. Biochem J 1950; 46: 440-450.
3. Hers HG: Le mecanisme de la transformation de glucose en fructose par les vesicules seminales. Biochim Biophys Acta 1956; 22: 202-203.
4. Clarke BF, Young RJ, Martyn CN, Ewing DJ: Aldose reduc- tase inhibition in diabetes. Diabetic Medicine 1984; 1: 88- 90.
5. Gabbay KH: The sorbitol pathway and the complications of diabetes. N Engl J Med 1973; 288: 831-836.
6. Friberg TJ, Rosenstock J, Sanborn G, Vaghefi A, Raskin P: The effect of long-term near-normoglycemic control on mild diabetic retinopathy. Ophthalmology 1985; 92: 1051-1058.
7. Kador F, Kinoshita JH, Tung WH, Chylack LT: Differences in the susceptibility of various aldose reductases to inhibi- tion Invest Ophthalmol Vis Sci 1960; 19: 980-982.
8. Akagi Y, Yajima Y, Kador PF, Kuwabara T, Kinoshita JH: Localization of aldose reductase in the human eye. Diabe- tes 1984; 33: 562-566.
9. Ludvigson MA, Sorenson RL: lmmunohistochemical local- ization of aldose reductase. Diabetes 1980: 29: 450-459.
394 August 1987 The American Journal of Medicine Volume 83
10. Akagi Y, Kador PF, Kuwabara T, Kinoshita JH: Aldose reduc- tase localization in human retinal mural cells. Invest Ophthalmol Vis Sci 1983; 24: 1516-1519.
1 I. Gabbay KH, Cathcart ES: Purification and immunologic iden- tification of aldose reductase. Diabetes 1974; 23: 460- 468.
12. Corder CN, Braughler JM, Culp PA: Quantitative histochem- istry of the sorbitol pathway in glomeruli and small arte- ries of human diabetic kidney. Folia Histochem Cytochem (Krakow) 1979; 17: 137-146.
13. Gabbay K, Merola LO, Field RA: Sorbitol pathway: presence in nerve and cord with substrate accumulation in diabe- tes. Science 1966; 151: 209-210.
14. Malone JI, Knox G, Benford S, Tedesco TA: Red cell sorbitol: an indicator of diabetic control. Diabetes 1980; 29: 861- 864.
15. Hubinont C, Sener A, Malaisse WJ: Sorbitol content of plasma and erythrocytes during induced short-term hy- perglycemia. Clin Biochem 1981; 14: 19-20.
16. Malone JI, Knox G, Harvey C: Sorbitol accumulation is al- tered in type 1 (insulin-dependent) diabetes mellitus. Dia- betologia 1984; 27: 5099513.
17. Popp-Snijders C, Lomecky-Janousek MZ, Schouten JA, van der Veen EA: Myoinositol and sorbitol in erythrocytes from diabetic patients before and after sorbinil treatment. Diabetologia 1984; 27: 514-516.
18. Raskin P, Rosenstock J, Challis P, et al: Effect of tolrestat on red blood cell sorbitol levels in diabetic subjects. Clin Pharmacol Ther 1985; 38: 625630.
19. Kinoshita JH: Cataracts in galactosemia. Invest Ophthalmol 1965; 4:786-799.
20. Kinoshita JH, Kador PF, Robison WG, Datilis MB, Cobo LM, Kupfer C: Aldose reductase and complications of diabe- tes. Ann Intern Med 1984; 101: 82-91.
21. Kador P, Robison WG, Kinoshita JH: The pharmacology of aldose reductase inhibitors. Annu Rev Pharmacol Toxicol 1985; 25: 691-714.
22. Gonzalez RG, Barnett P, Aguayo J, Chen H-M, Chylac LT Jr: Direct measurement of polyol pathway activity in the ocular lens. Diabetes 1984; 33: 196-199.
23. Hu T-S, Datiles M, Kinoshita JH: Reversal of galactose cata- ract with sorbinil in rats. Invest Ophtalmol Vis Sci 1983; 24: 640-644.
24. Datiles M, Fukui H, Kuwabara T, Kinoshita JH: Galactose cataract prevention with sorbinil and aldose reductase inhibitor. A light microscopic study. Invest Ophthalmol Vis Sci 1982; 22: 174-179.
25. Beyer-Mears A, Cruz E, Nicolas-Alexandre J, Varagiannis E: Sorbinil protection of lens protein components and cell hydration during diabetic cataract formation. Pharmacolo- gy 1982; 24: 193-200.
26. Gonzalez A-M, Sochor M, McLean P: The effect of an aldose reductase inhibitor (sorbinil) on the level of metabolites in lenses of diabetic rats. Diabetes 1983; 32: 482-485.
27. Stribling D, Mirrlees DJ, Harrison HE, Earl DCN: Properties of ICI 128,436, a novel aldose reductase inhibitor, and its effects on diabetic complications in the rat. Metabolism 1985; 34: 336-344.
28. Winegrad Al, Simmons DA, Martin DB: Has one diabetic complication been explained? N Engl J Med 1983; 308: 152-154.
29. Greene DA, De Jesus PV Jr, Winegrad Al: Effects of insulin and dietary myoinositol on impaired peripheral motor nerve conduction velocity in acute streptozotocin diabe- tes. J Clin Invest 1975; 55: 1326-1336.
30. Greene DA, Winegrad Al: Effects of acute experimental diabetes on composite energy metabolism in peripheral nerve axons and Schwann cells. Diabetes 1981; 30: 967- 974.
31. Simmons DA, Winegrad Al, Martin DB: Significance of tissue myo-inositol concentrations in metabolic regulation in nerve. Science 1982; 217: 848-85 1.
32. Mayhew JH, Gillon KRW, Hawthorne JN: Free and lipid inositol, sorbitol and sugars in sciatic nerve obtained post-mortem from diabetic patients and control subjects. Diabetologia 1983; 24: 13-15.
33. Finegold D, Lattimer SA, Nolle S, Bernestein M, Greene DA: Polyol pathway activity and myo-inositol metabolism-a suggested relationship in the pathogenesis of diabetic neuropathy. Diabetes 1983; 32: 988-992.
34. Greene DA, Lattimer SA: Impaired rat sciatic nerve sodium- potassium adenosine triphosphatase in acute streptozo- tin diabetes and its correction by dietary myo-inositol supplementation. J Clin Invest 1983; 72: 1058-1063.
35. Pietri A, Ehle AL, Raskin P: Changes in nerve conduction velocity after six weeks of glucoreyulation with portable insulin infusion oumos. Diabetes 1980; 29: 668-671.
36. Greene DA, Lewis RA; Lattimer SA, brown MJ: Selective effects of myoinositol administration on sciatic and tibia1 motor nerve conduction parameters in the streptozocin- diabetic rat. Diabetes 1982; 31: 573-578.
37. Clements RS, Vourganti B, Kuba TO, Shin J, Darnell B: Dietary myo-inositol intake and peripheral nerve function in diabetic neuropathy. Metabolism 1979; 28: 477-483.
38. Yue DK, Hanwell MA, Satchel1 PM, Turtle JR: The effect of aldose reductase inhibition on motor nerve conduction velocity in diabetic rats. Diabetes 1982; 31: 789-794.
39. Kikkawa R, Hatanaka J, Yasuda H, et al: Effect of a new aldose reductase inhibitor, (E)-3-carboxymethyl-5-[(2E)- methyl-3-phenylpropenylidene] rhodanine (ONO-2235) on peripheral nerve disorders of streptozotocin-diabetic rats. Diabetologia 1983; 24: 290-292.
40. Gillon KRW, Hawthorne JN: Sorbitol, inositol and nerve con- duction in diabetes. Life Sci 1983; 32: 1943-1947.
41. Kikkawa R, Hatanaka I, Yasuda H, Kobayashi N, Shigeta Y: Prevention of peripheral nerve dysfunction by an aldose reductase inhibitor in streptozotocin-diabetic rats. Metab- olism 1984; 33: 212-214.
42. Tomlinson DR, Townsend J, Fretten P: Prevention of defec- tive axonal transport in STZ diabetic rats by treatment with Statil (ICI 128,436) an aldose reductase inhibitor. Diabetes 1985; 34: 970-972.
43. Greene DA, Lattimer SA: Action of sorbinil in diabetic pe- ripheral nerve-relationship of polyol (sorbitol) pathway inhibition to a myo-inositol-mediated defect in sodium- potassium ATPase activity. Diabetes 1984; 33: 712-716.
44. Greene DA: Myo-inositol: the mystery molecule of diabetic complications. Clin Diabetes 1985; 3:80-81.
45. Engerman RL, Kern TS: Experimental galactosemia pro- duces diabetic-like retinopathy. Diabetes 1984; 33: 97- 100.
46. Frank RN, Keirn RJ, Kennedy A, Alexander F, Karni W: Galactose-induced retinal capillary basement membrane thickening: prevention by Sorbinil. Invest Ophthalmol Vis Sci 1983; 24: 1519-1524.
47. Robinson WG, Kador PF, Kinoshita JH: Retinal capillaries: basement membrane thickening by galactosemia pre- vented with aldose reductase inhibitor. Science 1983; 221: 1177-l 179.
48. Chandler ML, Shannon WA, DeSantis L: Prevention of retinal capillary basement membrane thickening in diabetic rats by aldose reductase inhibitors (abstr). Invest Ophthalmol Vis Sci 1984; 25 (suppl 2): 159.
49. Beyer-Mears A, Ku L, Cohen M: Glomerular polyol accumu- lation in diabetes and its prevention by oral sorbinil. Dia- betes 1984; 33: 604-607.
50. Beyer-Mears A, Cruz E, Dillon P, Tanis D, Roche M: Diabetic renal hypertrophy diminished by aldose reductase inhibi-
ALDOSE REDUCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
August 1987 The American Journal of Medicine Volume 83 305

ALDOSE REDUCTASE INHIBITORS AND DIABETIC COMPLICATIONS-RASKIN and ROSENSTOCK
tion (abstr). Fed Proc 1983; 42: 505. 51. Varagiannis E, Beyer-Means A, Cruz E: Diminished protein-
uria by an aldose reductase inhibitor, sorbinil (abstr). Diabetes 1985; 34 (suppl 1): 43A.
52. Judzewitsch RG, Jaspan JB, Polonsky KS, et al: Aldose reductase inhibition improves nerve conduction velocity in diabetic patients. N Engl Med 1983; 308: 119-125.
53. Jaspan J, Maselli R, Herold K, Bartkus C: Treatment of severely painful diabetic neuropathy with an aldose re- ductase inhibitor: relief of pain and improved somatic and autonomic nerve function. Lancet 1983; II: 758-762.
54. Young RJ, Ewing DJ, Clarke BF: A controlled trial of sorbinil, an aldose reductase inhibitor, in chronic painful diabetic neuropathy. Diabetes 1983; 32: 938-942.
55. Lewin IG, O’Brian IAD, Morgan MH, Corral1 RJM: Clinical and neurophysiological studies with the aldose reductase in-
hibitor, sorbinil, in symptomatic diabetic neuropathy. Dia- betologia 1984; 26: 445-448.
56. Hotta N, Kakuta H, Kimura M, et al: Experimental and clinical trial of aldose reductase inhibitor in diabetic neuropathy (abstr). Diabetes 1985; 34 (suppl 1): 98A.
57. Koglin L, Clark C, Ryder S, Mullane JF: The results of the long-term open-label admlnistration of ALREDASE in the treatment of diabetic neuropathy (abstr). Diabetes 1985; 34 (suppl 1): 202A.
58. Fagius J, Brattberg A, Jameson S, Berne C: Limited benefit of treatment of diabetic polyneuropathy with an aldose reductase inhibitor: a 24-week controlled trial. Diabetolo- gia 1985; 28: 323-329.
59. Rosenstock J, Challis P, Raskin P: The effect of sorbinil on severe painful diabetic neuropathy (abstr). Diabetes 1986; 35 (suppl2): 101A.
306 August 1987 The American Journal of Medicine Volume 83