airway assessment & recognition of difficult airway
TRANSCRIPT
AIRWAY ASSESSMENT & RECOGNITION OF POSSIBLE
COMPROMISED AIRWAY
DR. KHAIRUNNISA BINTI AZMAN
Anaesthesia Dept TGH
INTRODUCTION
• The human airway is a dynamic structure that extends from the nares to the alveoli
• Obstruction can occur at any point because of anatomic collapse or a foreign body which includes:
– Mucuous
– Blood
– Gastric content
DIFFICULT AIRWAY
American society of Anesthesiologist (ASA) suggested that when sign of inadequate
ventilation could not be reversed by mask ventilation OR oxygen saturation could not
be maintained above 90% OR
if a trained Anaesthetist using conventional larangoscope take’s more than 3 attempts OR
more than 10 minute are required to complete tracheal intubation
TERMINOLOGY
• Difficult airway
– Difficult with mask ventilation, tracheal intubation or both
• Difficult mask ventilation
– an unassisted anaesthesiologist unable to maintain SpO2 >90% using 100% oxygen & positive pression mask ventilation
• Difficult laryngoscopy
– Unable to visualize any portion of vocal cords with conventional laryngoscopy CL 3 & 4
• Difficult endotracheal intubation
– proper insertion of ETT wth conventional laryngoscopy requires > 3 attempts or > 10 minutes

WHY IS IT IMPORTANT TO ASSESS AIRWAY
• Respiratory events are the most common anaesthetic related injuries, following dental damage
• Main causes:
– Inadequate ventilation
– Oesophageal intubation
– Difficult tracheal intubation
• To look at patient physical features to predict ability to see the vocal cords (with laryngoscopy) and therefore predict ease of intubation
• Predicting a difficult airway allows you to
– Have extra equipment available
– Change your approach (eg: awake intubation)
WHY IS IT IMPORTANT TO ASSESS AIRWAY
Airway Asssessment
• History
• Physical examination: – Mallampati Classification
– Mouth opening
– Dentitian
– TMJ Mobility
– Thyromental distance (TMD)
– Cervical spine range of motion
– Other factors: Obesity, pregnancy
HISTORY
• Adverse events related to prior airway management
• Radiation/surgical history – Distortion of Anatomy
– Scar Tissue
– Fixed Flexion Deformity of the Spine
• Burns/swelling/tumor/masses
• Obstructive sleep apnoea
• Problem with phonation
• C-spine disease
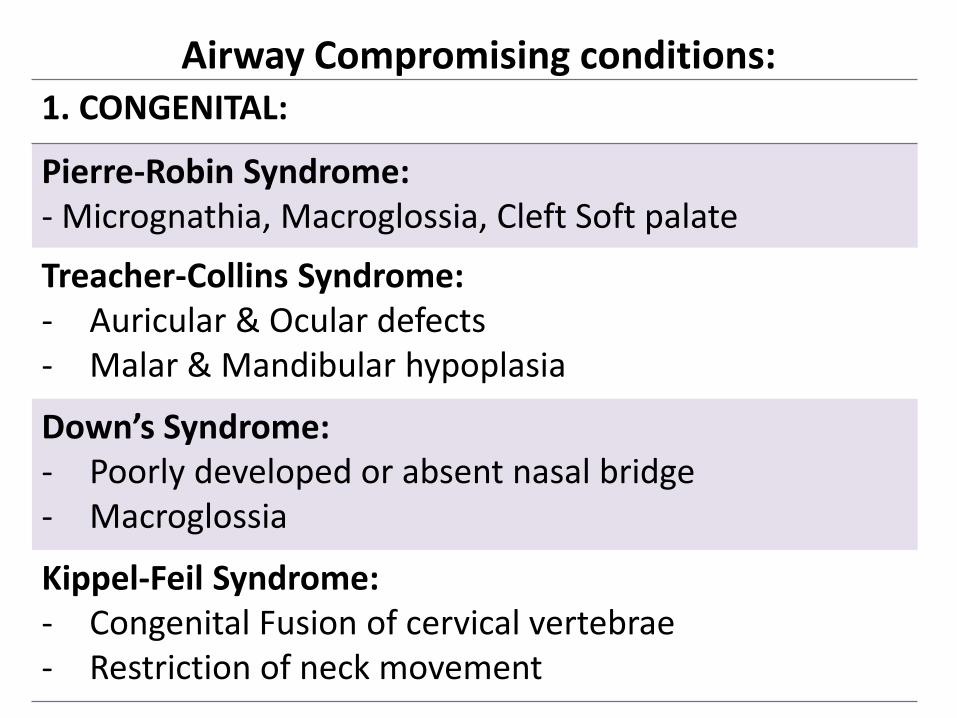
Airway Compromising conditions: 1. CONGENITAL:
Pierre-Robin Syndrome: - Micrognathia, Macroglossia, Cleft Soft palate
Treacher-Collins Syndrome: - Auricular & Ocular defects - Malar & Mandibular hypoplasia
Down’s Syndrome: - Poorly developed or absent nasal bridge - Macroglossia
Kippel-Feil Syndrome: - Congenital Fusion of cervical vertebrae - Restriction of neck movement

Pierrre- Robin
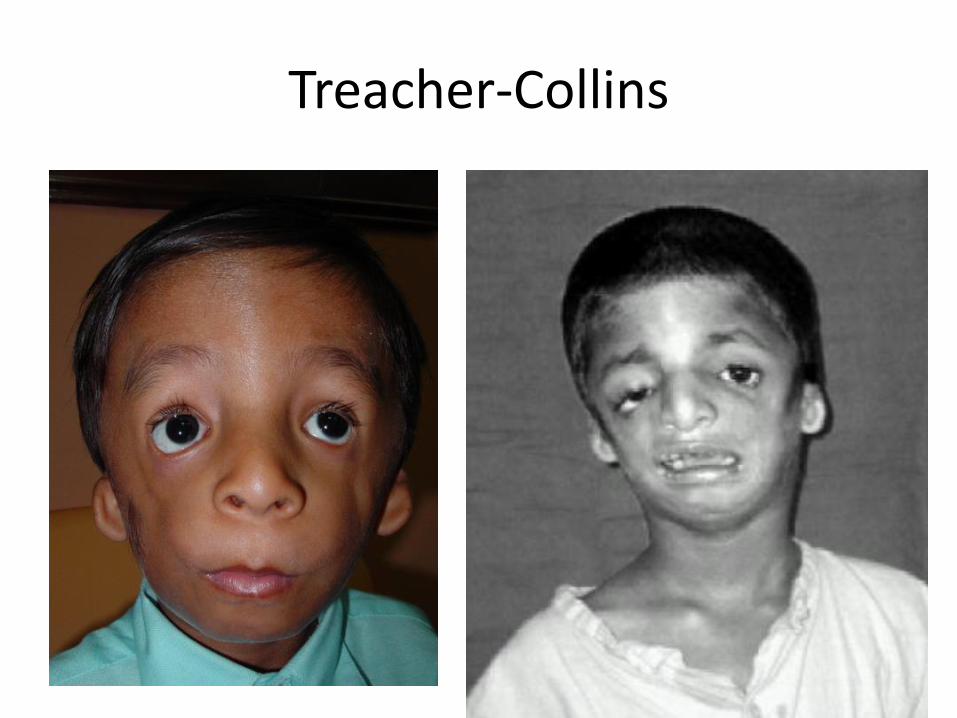
Treacher-Collins

Goldenhar

Down’s Syndrome

Klippel-Feil
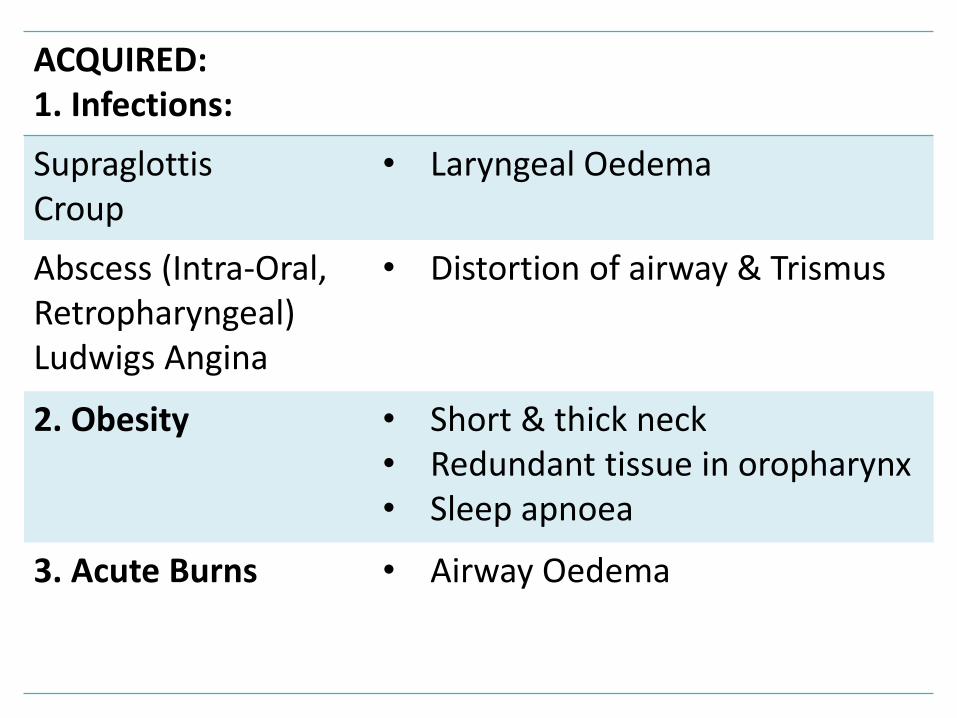
ACQUIRED: 1. Infections:
Supraglottis Croup
• Laryngeal Oedema
Abscess (Intra-Oral, Retropharyngeal) Ludwigs Angina
• Distortion of airway & Trismus
2. Obesity • Short & thick neck • Redundant tissue in oropharynx • Sleep apnoea
3. Acute Burns • Airway Oedema
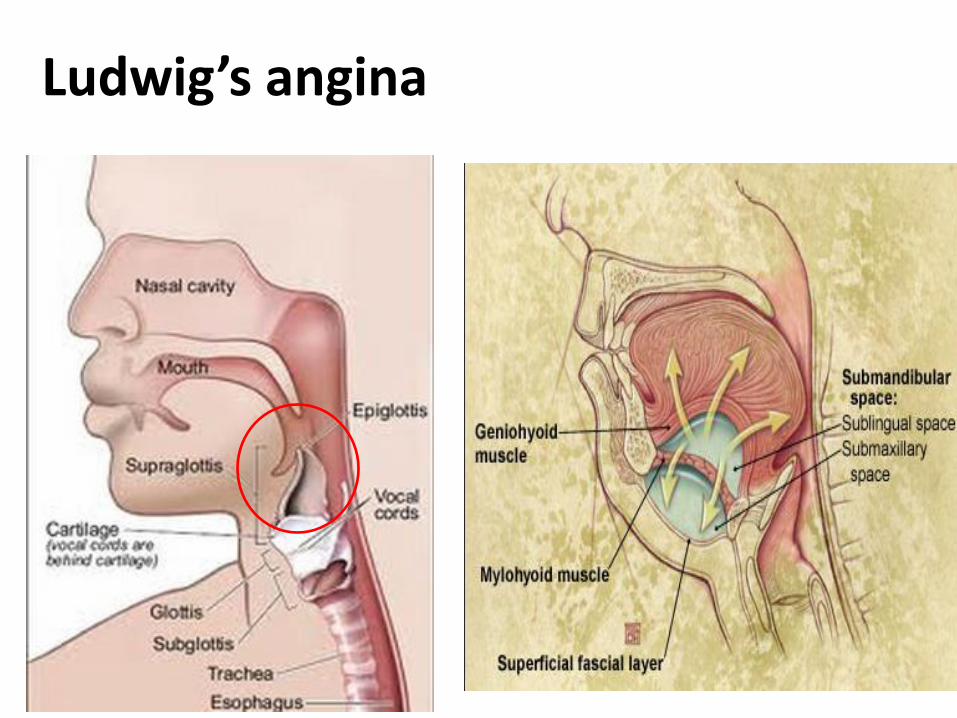
Ludwig’s angina
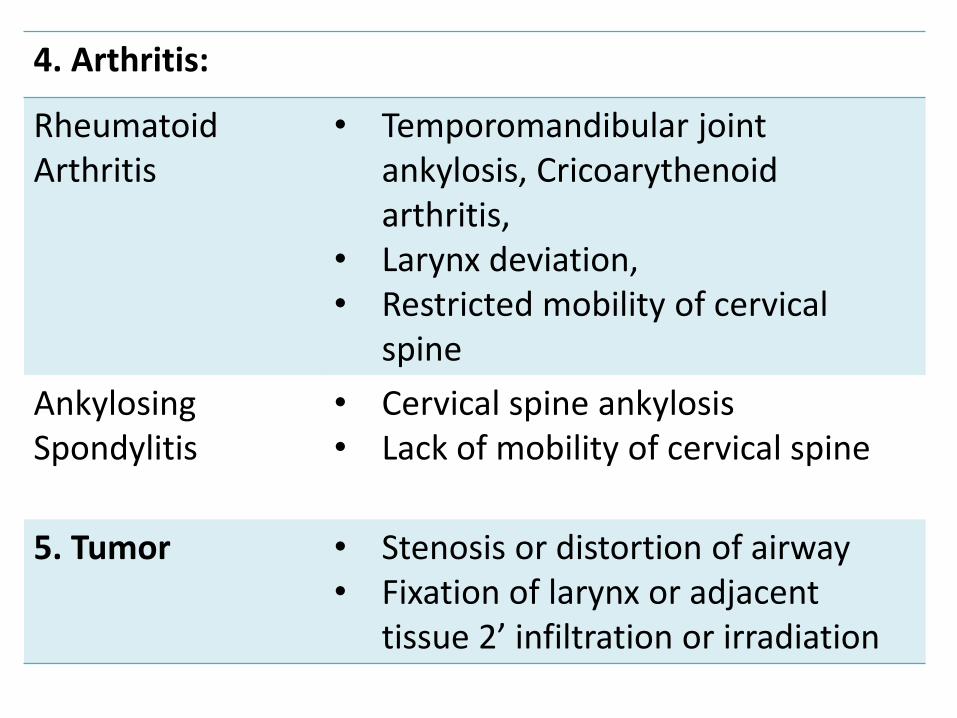
4. Arthritis:
Rheumatoid Arthritis
• Temporomandibular joint ankylosis, Cricoarythenoid arthritis,
• Larynx deviation, • Restricted mobility of cervical
spine
Ankylosing Spondylitis
• Cervical spine ankylosis • Lack of mobility of cervical spine
5. Tumor • Stenosis or distortion of airway • Fixation of larynx or adjacent
tissue 2’ infiltration or irradiation

Arthritis
Rheumatoid Arthritis Ankylosing Spondylitis
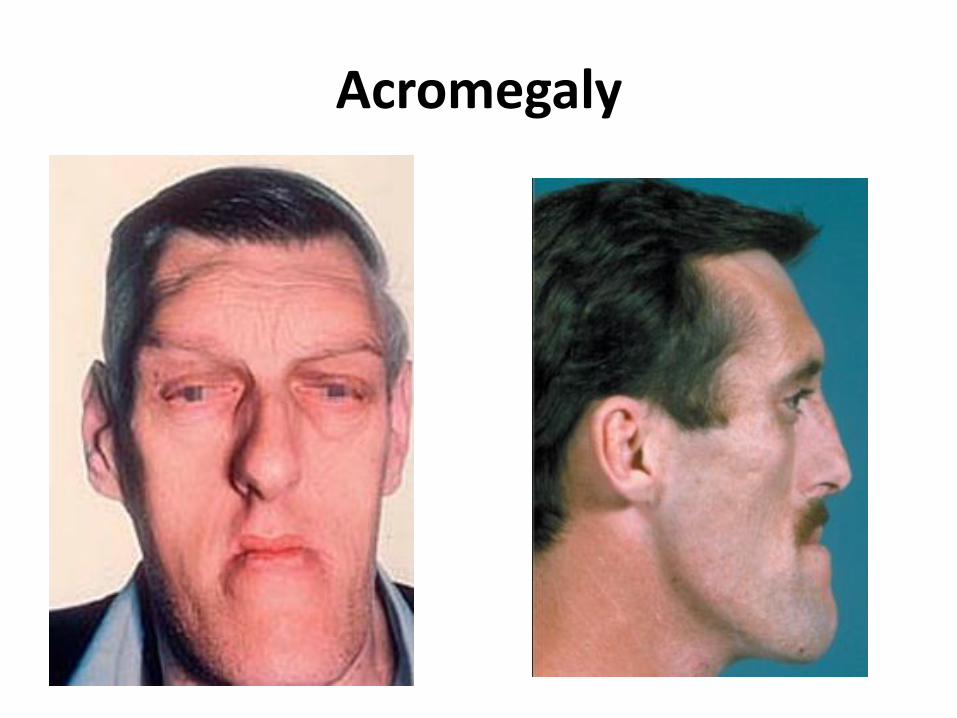
Acromegaly
Examination
1. Dentitian:
• Prominent upper incisors
• Receding chin
• Teeth: Loose, chipped, dentures

2. Mouth opening: • Male assessor: 2 finger
breadths • Female assessor: 3
finger breadths
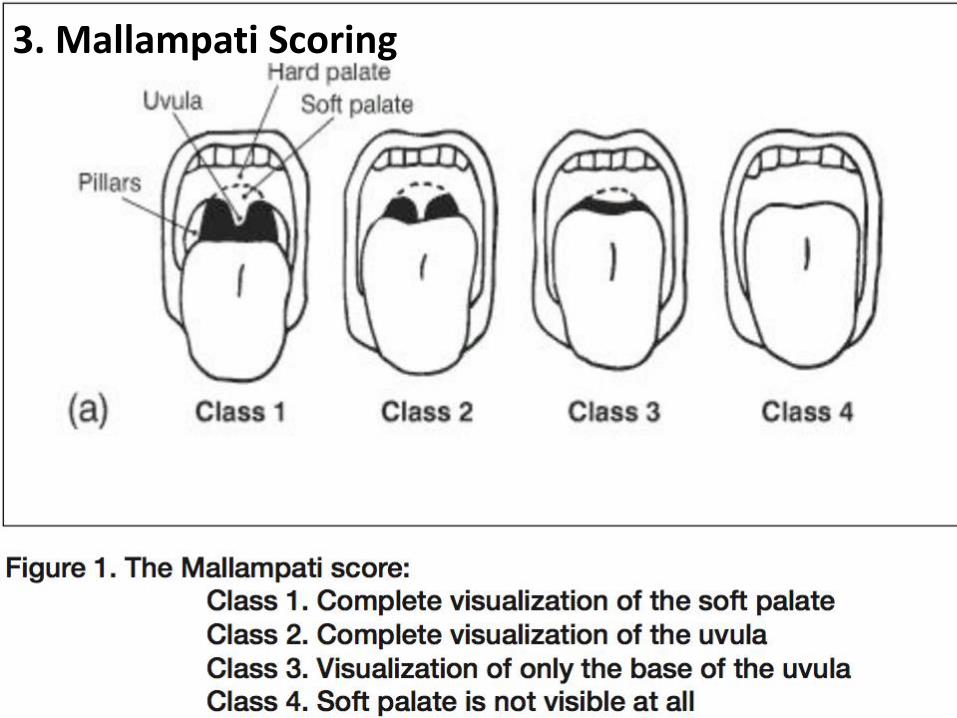
2. Ability to visualize uvula
• Malampati scoring
3. Mallampati Scoring
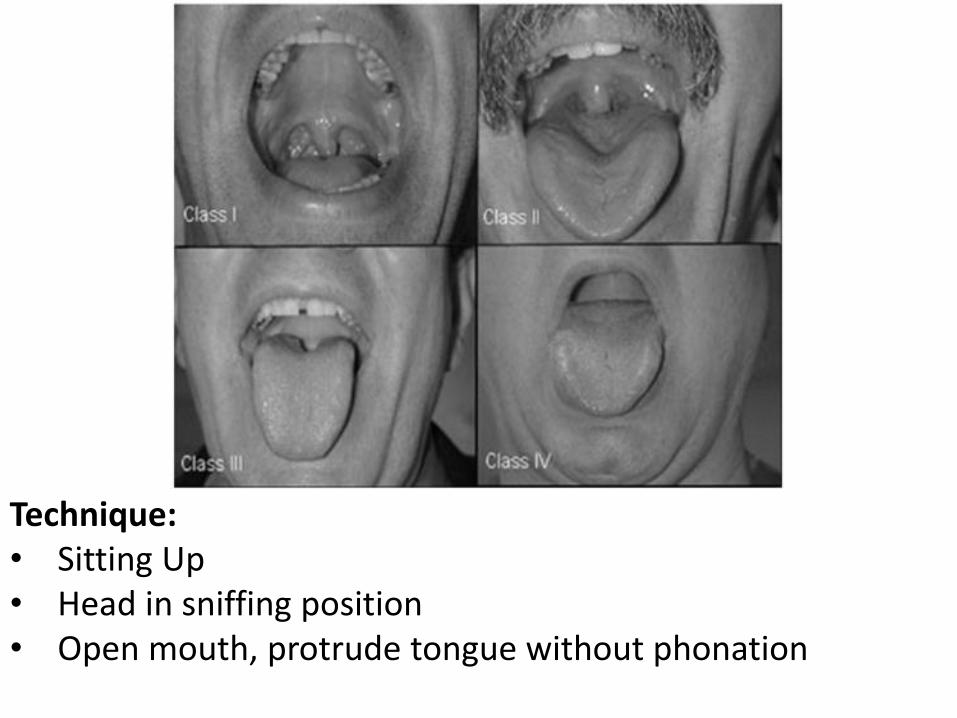
Technique: • Sitting Up • Head in sniffing position • Open mouth, protrude tongue without phonation
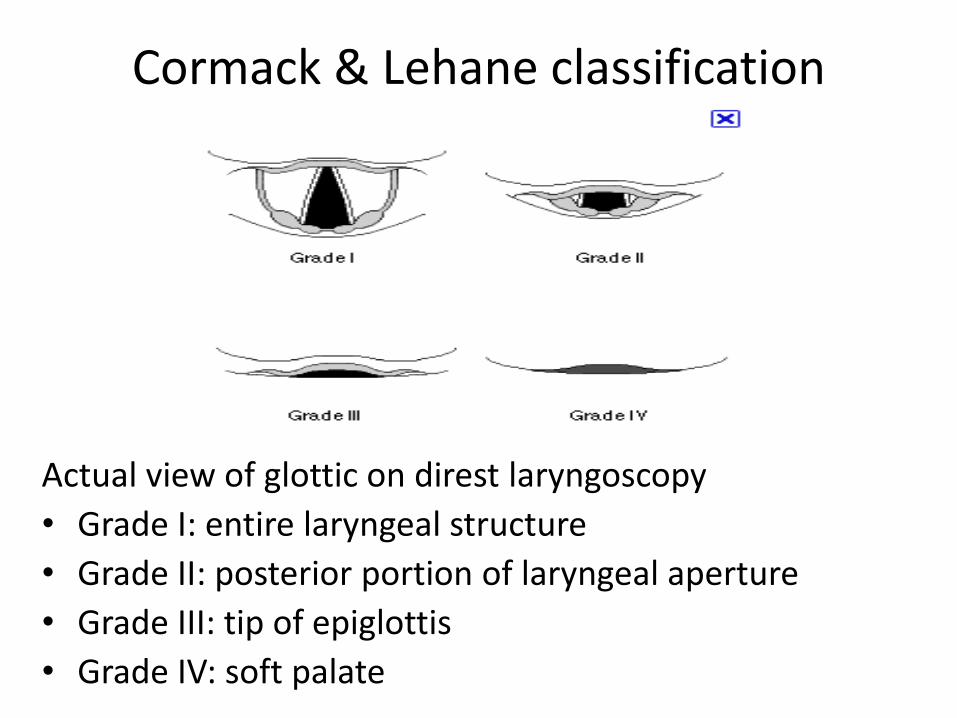
Cormack & Lehane classification
Actual view of glottic on direst laryngoscopy
• Grade I: entire laryngeal structure
• Grade II: posterior portion of laryngeal aperture
• Grade III: tip of epiglottis
• Grade IV: soft palate
4. Mobility
• Cervical spine mobility
• Temporomandibular mobility
• Thyromental distance (TMD)
Examination
Neck mobility:
• Ask patient to place their chin on their chest & tilt head backwards as far as possible
– Not possible in trauma patient

Thyromental distance:
• Measure from upper edge of thyroid cartilage to chin with head fully extended
• 6cm
• >3- 4 FB
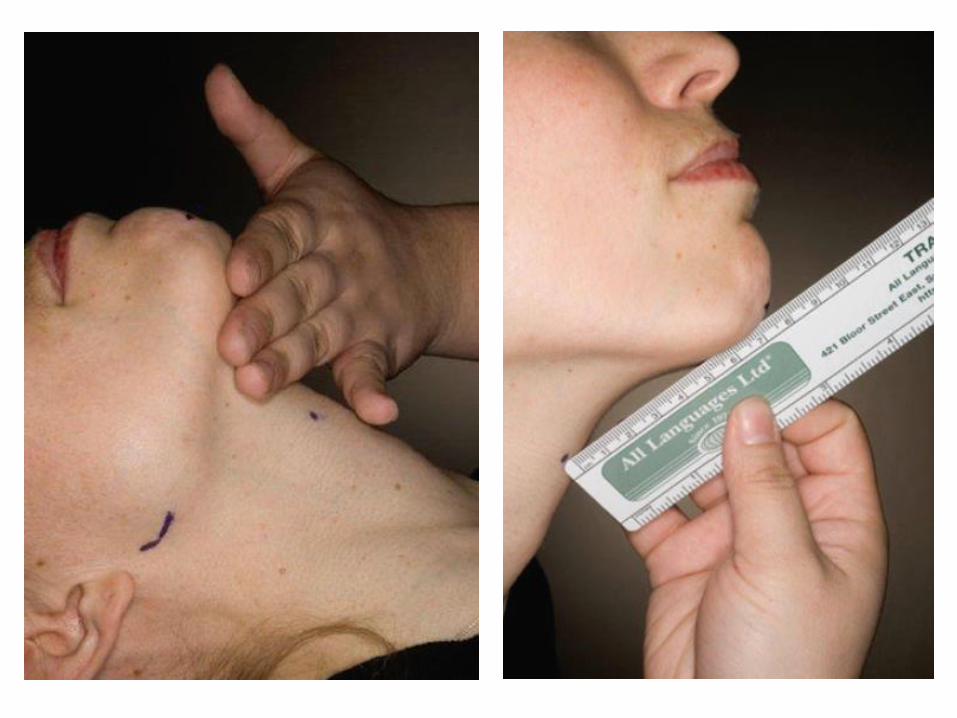
Atlanto-occipital movement:
• Flexion of the neck, by elevating the head approximately 10 cm, aligns the laryngeal and pharyngeal axes.
• Extension of the head on the atlanto-occipital joint is important for aligning the oral and pharyngeal axes to obtain a line of vision during direct laryngoscopy
• Sniffing position
STERNOMENTAL DISTANCE:
• From sternum to tip of the mandible with the head extended
• > 12.5cm: Difficult intubation
Mandibular Protrusion:
• If the patient able to protrude the lower teeth beyond upper incisor intubation usually straight foward
• if patient cannot get upper & lower incisor into alignment intubation likely difficult
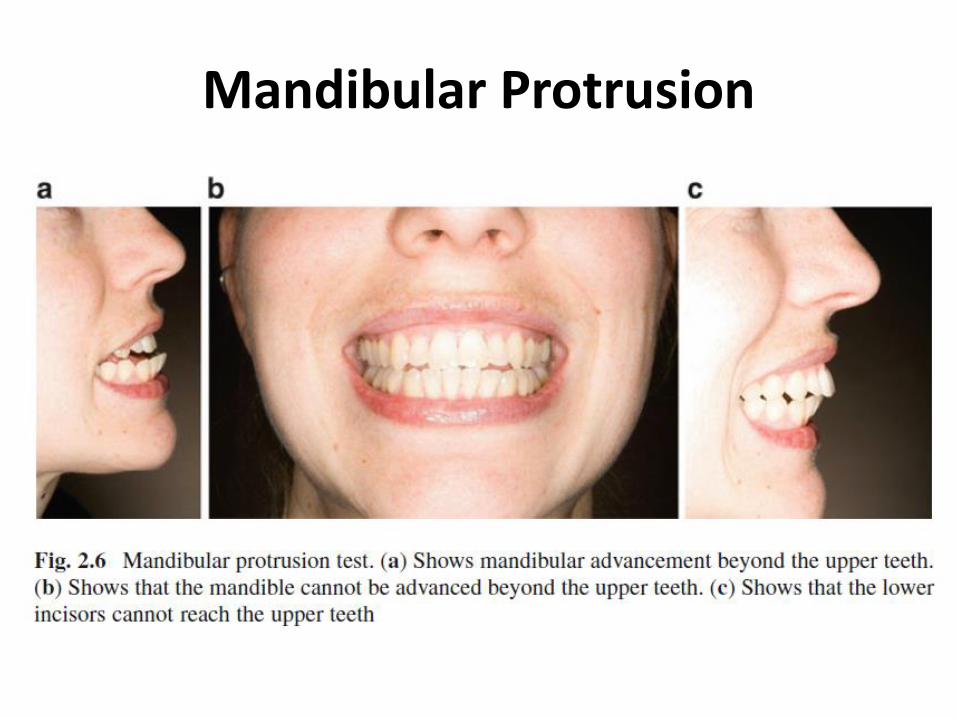
Mandibular Protrusion


The Three Pillars of airway management:
• Patency Airflow integrity
• Protection against aspiration
• Assurance of Oxygenation & Ventilation

Clinical Signs of Compromised Airway
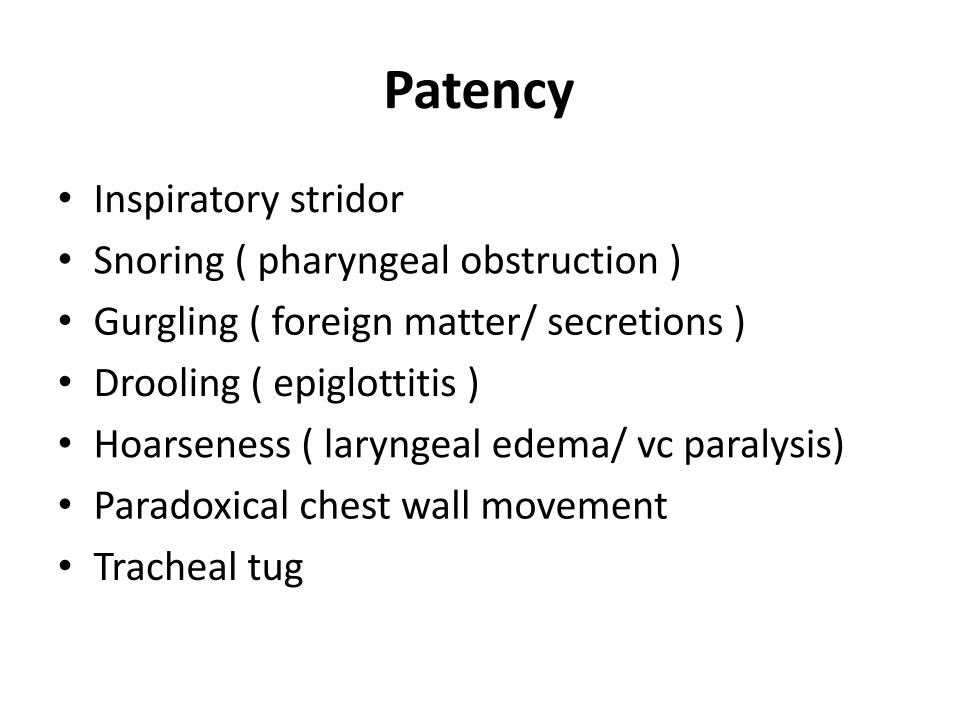
Patency
• Inspiratory stridor
• Snoring ( pharyngeal obstruction )
• Gurgling ( foreign matter/ secretions )
• Drooling ( epiglottitis )
• Hoarseness ( laryngeal edema/ vc paralysis)
• Paradoxical chest wall movement
• Tracheal tug

Protection
• Blood in upper airway
• Pus in upper airway
• Persistant vomiting
• Loss of protective airway reflexes

Oxygenation and Ventilation
• Central cyanosis
• Obtundation and diaphoresis
• Rapid shallow breathing
• Accessory muscle use
• Retractions
• Abdominal paradox
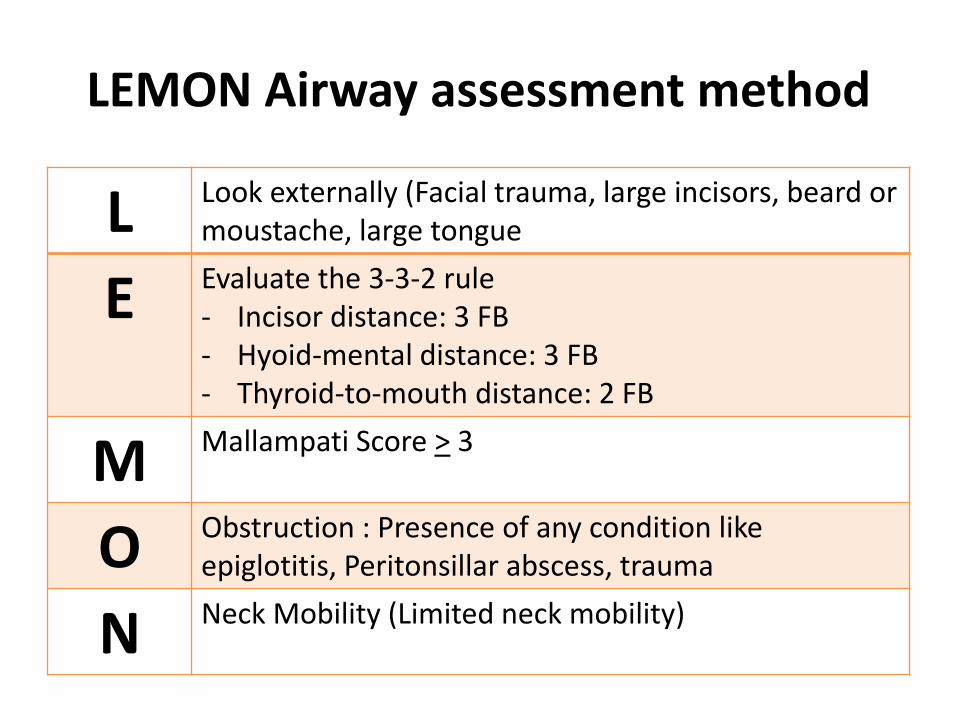
LEMON Airway assessment method
L Look externally (Facial trauma, large incisors, beard or moustache, large tongue
E Evaluate the 3-3-2 rule - Incisor distance: 3 FB - Hyoid-mental distance: 3 FB - Thyroid-to-mouth distance: 2 FB
M Mallampati Score > 3
O Obstruction : Presence of any condition like epiglotitis, Peritonsillar abscess, trauma
N Neck Mobility (Limited neck mobility)
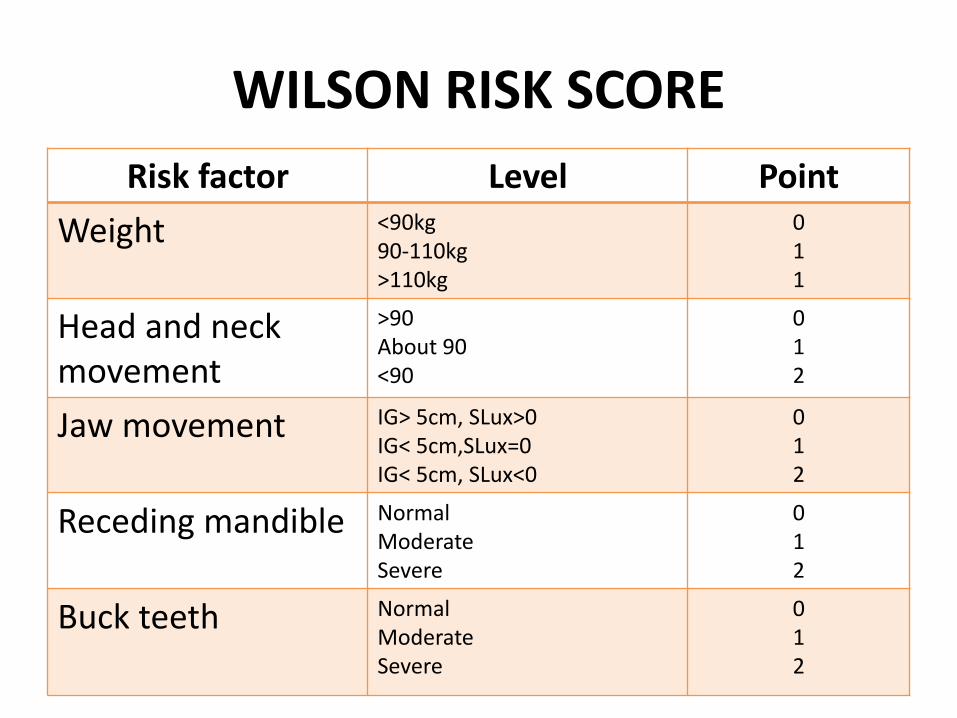
WILSON RISK SCORE
Risk factor Level Point
Weight <90kg 90-110kg >110kg
0 1 1
Head and neck movement
>90 About 90 <90
0 1 2
Jaw movement IG> 5cm, SLux>0 IG< 5cm,SLux=0 IG< 5cm, SLux<0
0 1 2
Receding mandible Normal Moderate Severe
0 1 2
Buck teeth Normal Moderate Severe
0 1 2
• Score > 3 75% of difficult intubations • score> 4 predicts 90%. • The test has a poor specificity and may fail to predict
more than 50% of difficult intubations. • IG: interincisor gap: distance between upper & lower
incisor measured with mouth fully open • Slux: subluxation: maximal forward protrusion of lower
incisor beyond upper incisiors • SLux>0: upper incisor can protrude beyond upper
incisor • SLux=0: both are edge to edge • SLux<0: lower incisors cannot be brought edge to edge
WILSON RISK SCORE
Indications for Active Airway Intervention
• Patency - relief of obstruction
• Protection from aspiration
• Hypoxic/ hypercapnic respiratory failure
– Failure to oxygenate
– Failure to remove CO2
• Neuromuscular weakness
• CNS failure
• Cardiovascular failure
Management of Compromised Airway
• Bag-Valve-Mask Ventilation
• Endotracheal Intubation
• Rapid Sequence Intubation
• Airway adjuncts





Take Home Messages
• Learn Basic Theory
• Practice basic principles on an airway trainer
• Perform technique or procedure in a patient under supervision
• Perfect the acquired skills
• Place an airway in patients with an anticipated difficult airway
• Participate in continuing education and training
And....
