ahs implementation in universitas gadjah...
TRANSCRIPT

AHS Implementation in Universitas Gadjah Mada
Rukmono Siswishanto Dr. Sardjito Hospital/ Fac. of Medicine
Outline
① Introduction
② Why do we need AHS
③ The risk of not being integrated
④ The underlying concept
⑤ Implementation of AHS
⑥ Challenges ahead
Yogyakarta Special Region
• Located in the central part of Java Island
• Population: more than 3.5 million
• Four districts and 1 city:
– Yogyakarta city
– Sleman
– Bantul
– Kulonprogo
– Gunungkidul
FACULTY OF MEDICINE
UNIVERSITAS GADJAH MADA
Universitas Gadjah Mada (UGM)
established on December 19, 1949
Faculty of Medicine UGM
established on March 5, 1946
General Profile Faculty of Medicine UGM
• 3 undergraduate programs
• 6 master programs
• 1 doctoral program
• 20 clinical specialization programs
• 32 Departments
• 14 Research centers-WGs
• >1,000 staff (teaching and administrative)
• >500 new undergraduate students
• >600 new graduate students and residents
Human Resources
Lecturers: 673*
• 303 (45%), full time
– 209 (government civil servant) and 94 (university-based)
• 156 (23%) clinical teachers from Sardjito
• 214 (32%) clinical teachers from other teaching hospitals
*Excluding part-time lecturers from non-teaching hospitals and 77 retired lecturers
Quality Assurance Systems
Internal
• Quality assurance office (University level)
• Quality assurance unit (Faculty level)
• Academic standard committee (Study program level)
External
• National accreditation – Public health graduate program
accreditation: A
• International accreditation – IMIA (HMIS, provisionally
accredited)
– PAASCU (Medicine, in process)
– FERCAP (IRB)
– JCI for AMC (Sardjito hospital)
– ISO certification 9001:2008 (Faculty administration)

5 Hospital 1927 beds++
Sardjito General Hospital
• Ministry of Health owned hospital in Yogyakarta
• 750 beds capacity
• Top referral hospital for Yogyakarta Special Province and southern part of mid Java Province (23 million population)
• Cardiac and Cancer excellence services
• JCI accreditation for AMC
Soeradji Tirtonegoro Hospital
• Ministry of Health owned hospital in Klaten (30 kms east of Yogyakarta)
• 400 beds capacity
• Located in rural/ suburban area
• Geriatric excellence services

Universitas Gadjah Mada Hospital
• University owned hospital
• 200 beds capacity, secondary services
• Official opened in 2012
• Disabled child growth excellence services

Hardjolukito Hospital
• Air-force military owned hospital
• 400 beds capacity, tertiary services
• Located at eastern part of Yogyakarta city
• Special in Flight Medicine
Banyumas Hospital
• District government owned hospital
• Located in rural area, 200 kms west of Yogyakarta
• 300 beds capacity, secondary services
• Comprehensive Mental Health excellence services
② WHY DO WE NEED AHS
1/13/2017
Legislation related to AHS
• UU no 12 tahun 2012 tentang pendidikan tinggi • UU no 12 tahun 2013 tentang pendidikan kedokteran • UU no 44 tahun 2009 tentang rumah sakit • UU no 29 tahun 2004 tentang praktek kedokteran • UU no 36 tahun 2014 tentang tenaga kesehatan • UU no 5 tahun 2014 tentang ASN • PP no 93 tahun 2015 tentang RS Pendidikan • Permenristekdikti no 26 tahun 2015 tentang
pendidikan • Permenristekdikti no 2 tahun 2016 tentang
perubahan permenristekdikti no 26 tahun 2015
Mission
Disruption?
• Changing in societal needs and values
• Disease patterns
• Economics
• Globalization
• Politics
• Population demographics
• Market consolidation
• Consumer empowerment
• Policy changes
• Enterpreneurism
16
Wartman: The Transformation of Academic Health Centers (2015)

① Free trade of AEC (31 December 2016)
② Legislation
③ Medical & information technology
④ Customer orientation
⑤ JKN (BPJS & referral system)
⑥ Remuneration system
⑦ AHS/ AMC/ AHC 17

Current Situation
Faculty of Medicine
• Clinical educator
• Cost of medical education
• Unmet need of clinical educator (focus on health care, quota)
• Clinical & translational research , not optimal
• Low contribution on medical/ health science
• Community services less comprehensive
Hospital
• Less priority on educational activity (not included in remuneration system)
• Quota of HR based on case load
• Research is not priority
• Un-strategic choice of featured services (inefficient)
• Less responsibility to foster the others
Other problems
- Limited facilities: patients booming long waiting list
- Limited budget: Hospital priority
- Different Regulations between Institutions/ hospitals
- Administration system
- Remuneration

Education
Research
Healthcare
Community

③ THE RISK OF NOT BEING INTEGRATED

① Less adaptive in dynamic world
② Failure to thrive
④ THE UNDERLYING CONCEPT

Large-scale social change requires broad cross-sector coordination, yet the social sector remains focused on the isolated intervention of individual organizations
(Kania & Kramer, Collective impact, 2011)
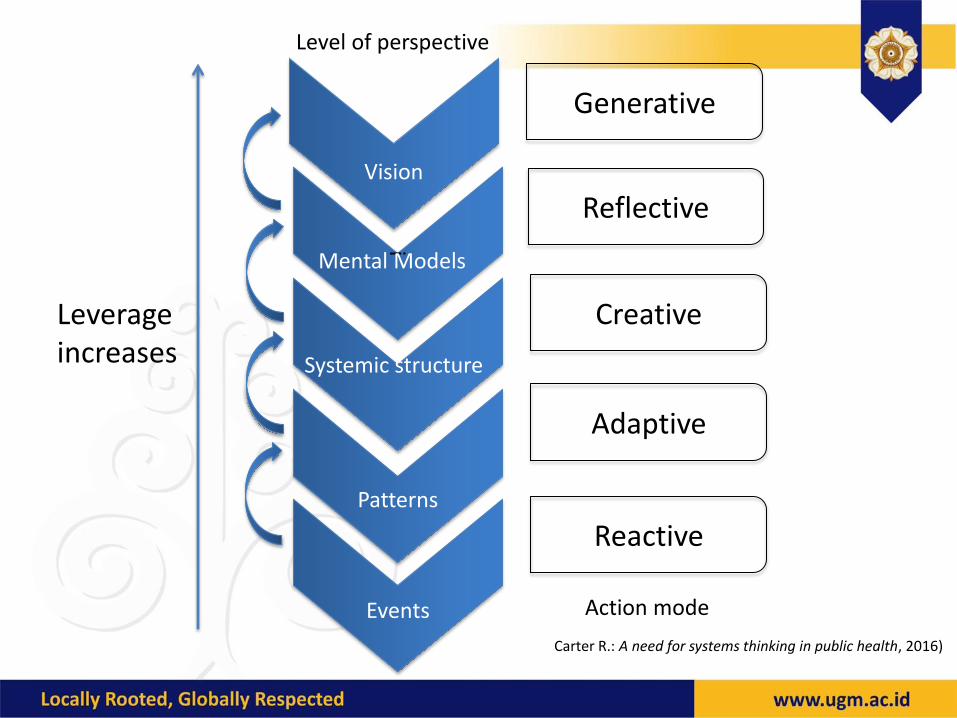
Vision
i
Mental Models
Systemic structure
Patterns
Events
Generative
Reflective
Creative
Adaptive
Reactive
Leverage increases
Level of perspective
Action mode
Carter R.: A need for systems thinking in public health, 2016)

Collective Success
① Common agenda
② Shared measurement systems
③ Mutually reinforcing activities
④ Continuous communication
⑤ Backbone support organization
(Kania & Kramer, Collective impact, 2011)
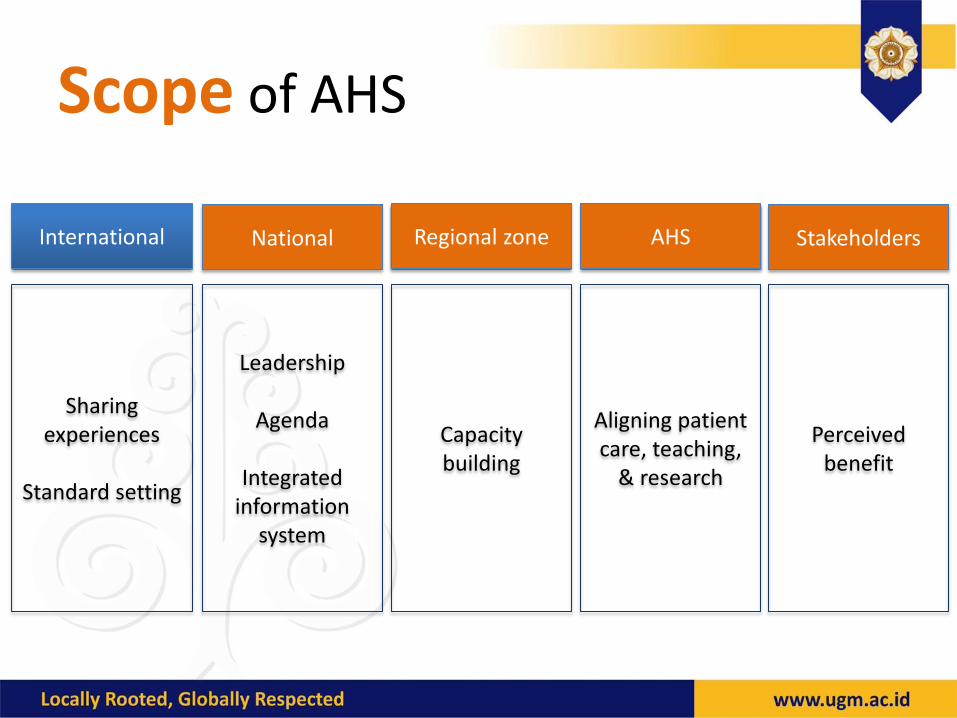
Scope of AHS
International National Regional zone AHS Stakeholders
Sharing experiences
Standard setting
Leadership
Agenda
Integrated information
system
Capacity building
Aligning patient care, teaching,
& research
Perceived benefit
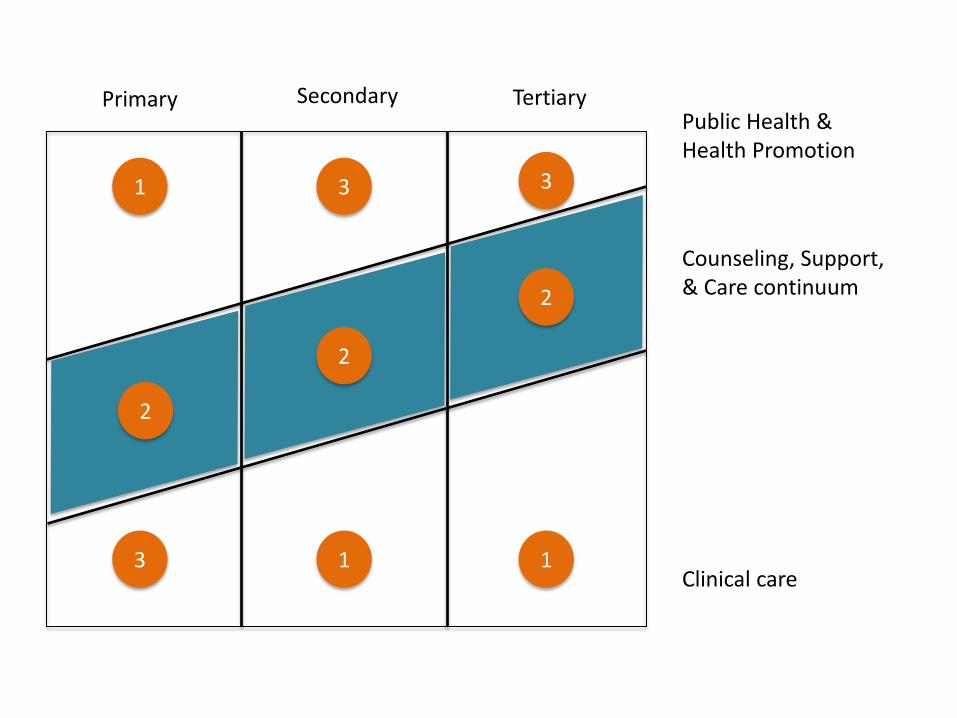
Primary Secondary Tertiary Public Health & Health Promotion
Counseling, Support, & Care continuum
Clinical care
1
2
1
2
2
3 1
3 3
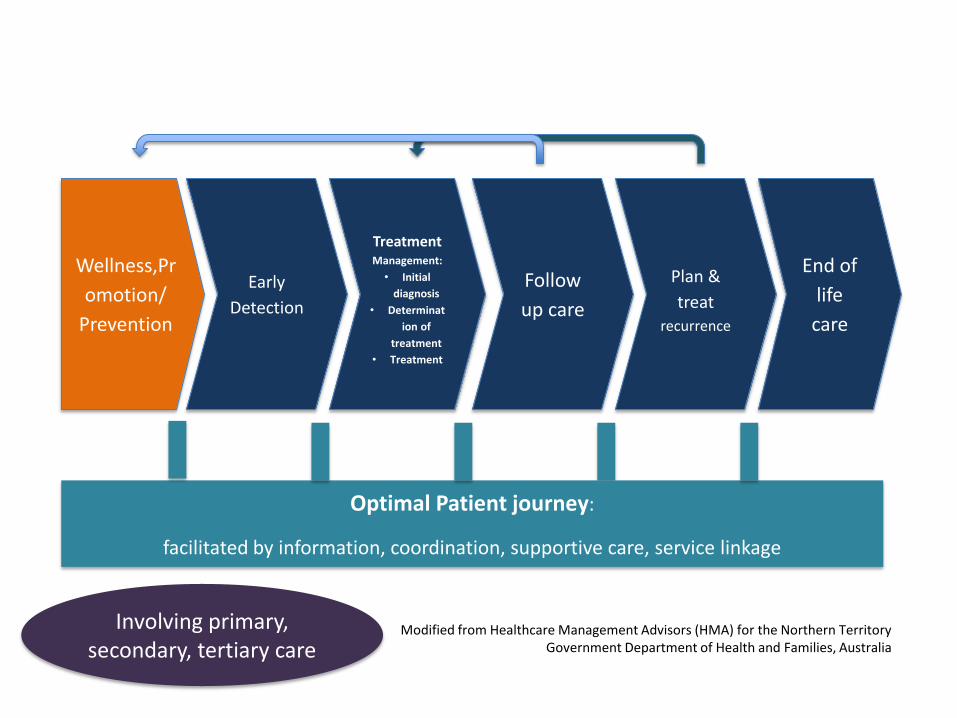
Plan &
treat recurrence
Wellness,Pr
omotion/
Prevention
Early
Detection
Treatment Management:
• Initial
diagnosis
• Determinat
ion of
treatment
• Treatment
Follow
up care
End of
life
care
Optimal Patient journey:
facilitated by information, coordination, supportive care, service linkage
Modified from Healthcare Management Advisors (HMA) for the Northern Territory Government Department of Health and Families, Australia
Involving primary, secondary, tertiary care

Integration: Functional PP 93/2015 (ps 21)
FK
RS
Perjanjian kerjasama tertulis
Integrasi Fungsional Koordinasi & kolaborasi dalam perencanaan, pelaksanaan, &
evaluasi: pendidikan, pelayanan, penelitian, & abdimas
Integrasi Struktural
Penyatuan institusi menjadi satu kesatuan kerja
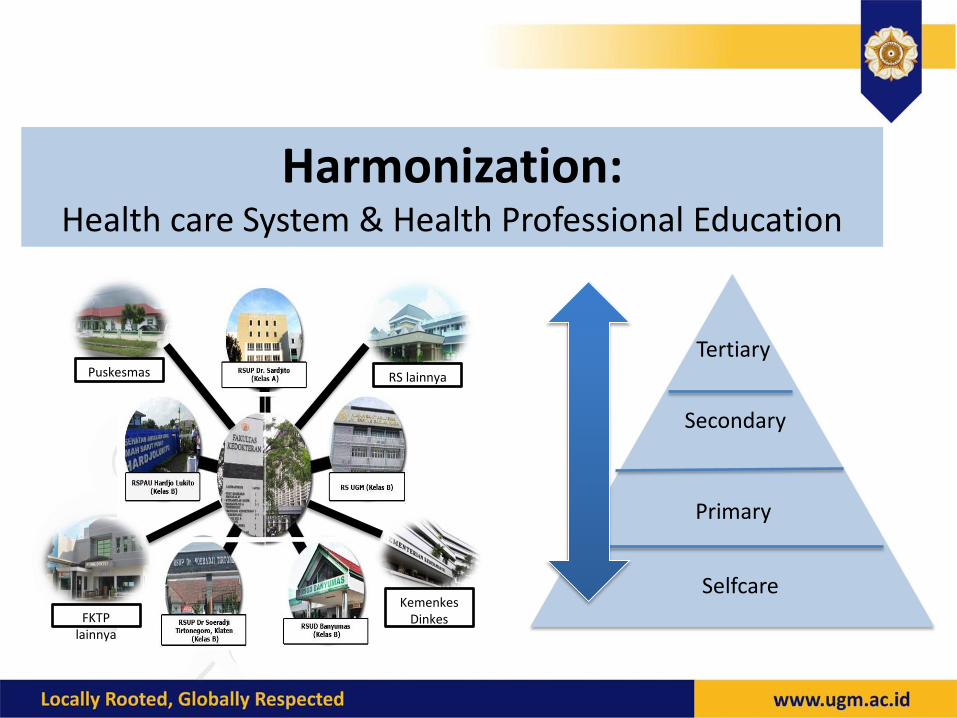
Harmonization: Health care System & Health Professional Education
Puskesmas RS lainnya
FKTP lainnya
Kemenkes Dinkes
Tertiary
Secondary
Primary
Selfcare
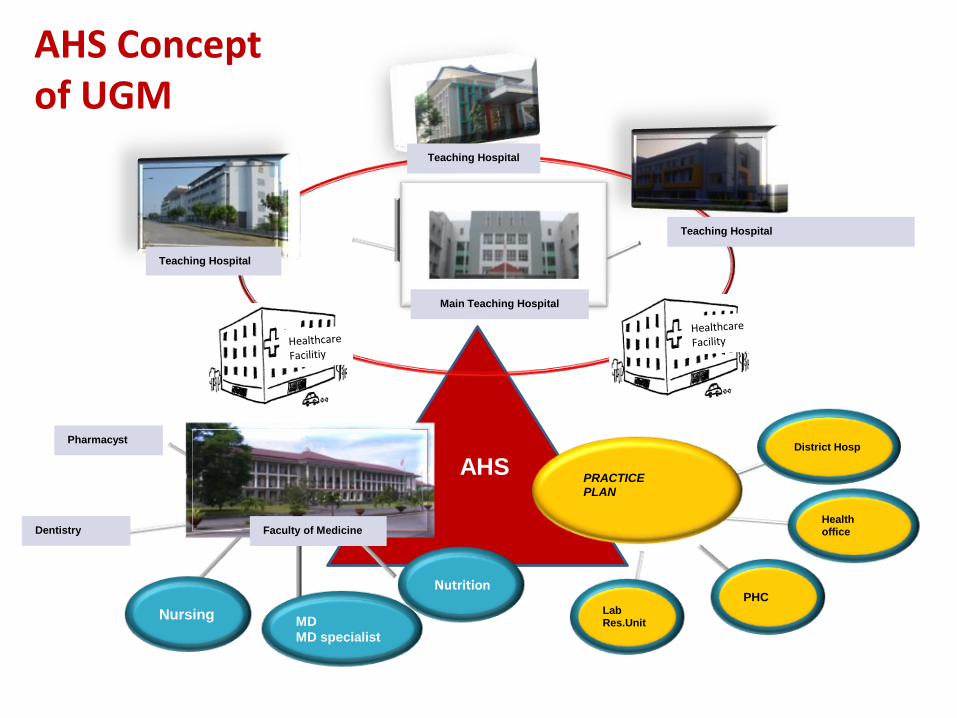
AHS Concept of UGM
Health office
Lab Res.Unit
PHC
District Hosp
MD
MD specialist
Nursing
AHS UNIVERSITAS
PRACTICE
PLAN
Main Teaching Hospital
Teaching Hospital
Teaching Hospital
Teaching Hospital
Faculty of Medicine Dentistry
Nutrition
Pharmacyst
⑤ IMPLEMENTATION OF AHS
Partnership & vehicles
Synergy of program
Organization

Partnership & Vehicles
• 10 Hospitals – Combine for MD& Specialist training
• 32 Hospitals – For Specialist training
• Sister hospitals – Bajawa, Balikpapan, Jayapura, etc.
• Health Office
• Public Health Center
Synergy of Program Education
-Share education facilities, IT
-Standardized curricula for undergraduate,
profession and residents for teaching and
partner hospitals
-Capacity building for staffs in teaching hospitals : TOT
-Quality control in education

Sample AHS Agenda for Spesialist Training
• Involving related stakeholders:
– GCU, Vaccination
– Insurance
– Insentive
• Working hours (referring to ACGME)
• Professional behaviour

Teleconference: AHS Management

Case Teleconference (Dept. of Skin & Venerology)

Library Sharing
• Library facility sharing: Connection between UGM & Dr. Sardjito Hospital

Synergy of Program
Research
- Coordinated Ethical Committee in Faculty of Med and University Hospital
-Sharing research budget, scholarships
-Sharing Laboratory Facilities
-Capacity building for researchers: GCP, GCLP
-Organize clinical trial

2014-Project Highlights
Oral Rv3 rotavirus vaccine research in
Indonesia (Bill&Melinda Gates
Foundation)
Malaria Transmission Consortium
(Bill&Melinda Gates Foundation)
Monitoring progress Family Planning 2020 (Future Institute and Bill&Melinda Gates
Foundation)
USAID-TBCTA Regional Training
Centre for TB control & Neglected Infectious Disease Diagnostic
Consortium (EU)
Primary Care Accelerator Program and InterUniversity
Consortium on Global Health (New Proposal)
Knowledge Sector Initiative, HIV-AIDS,
Sister hospital (Ausaid), Health policy
network (Ausaid, IDRC)
Eliminate Dengue Project-Tahija
Foundation and Dengue Waening
Signs (WHO-TDR)
Fever Study-INA Respond (NIH USA R&D in collaboration with MOH & Teaching
Hospitals)
Translational research on Nasopharyngeal Cancer and other types of Cancer (IRAC, AvL and
partners)

Our Partners
• 62 international partners
• 51 new national partners
• Leading national consortiums
Synergy of Program
Health/ Patient Care • Center of Excellence
• Improvement quality (JCI Accreditation)
• Sharing Facilities: CT Scan, MRI, Gamma Camera, ICU – not only 3 hospitals
• Sharing health professionals: send specialist to referral hospitals
• Send senior residents for health services and training
• Referral system
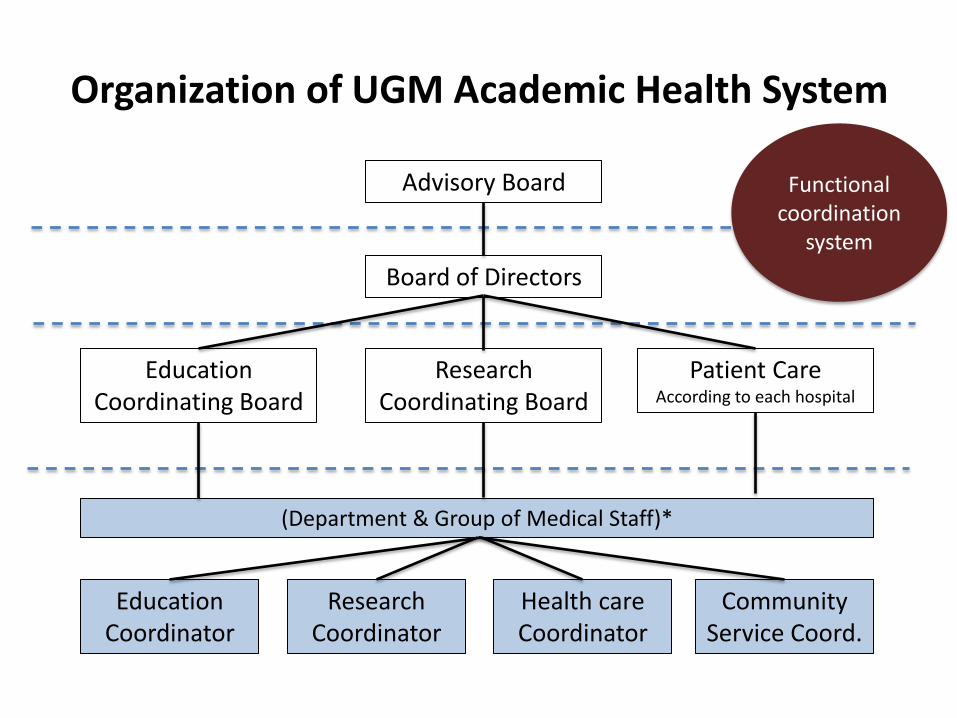
Organization of UGM Academic Health System
Advisory Board
Board of Directors
Education Coordinating Board
Research Coordinating Board
Patient Care According to each hospital
(Department & Group of Medical Staff)*
Education Coordinator
Research Coordinator
Health care Coordinator
Community Service Coord.
Functional coordination
system
⑤ CHALLENGES AHEAD
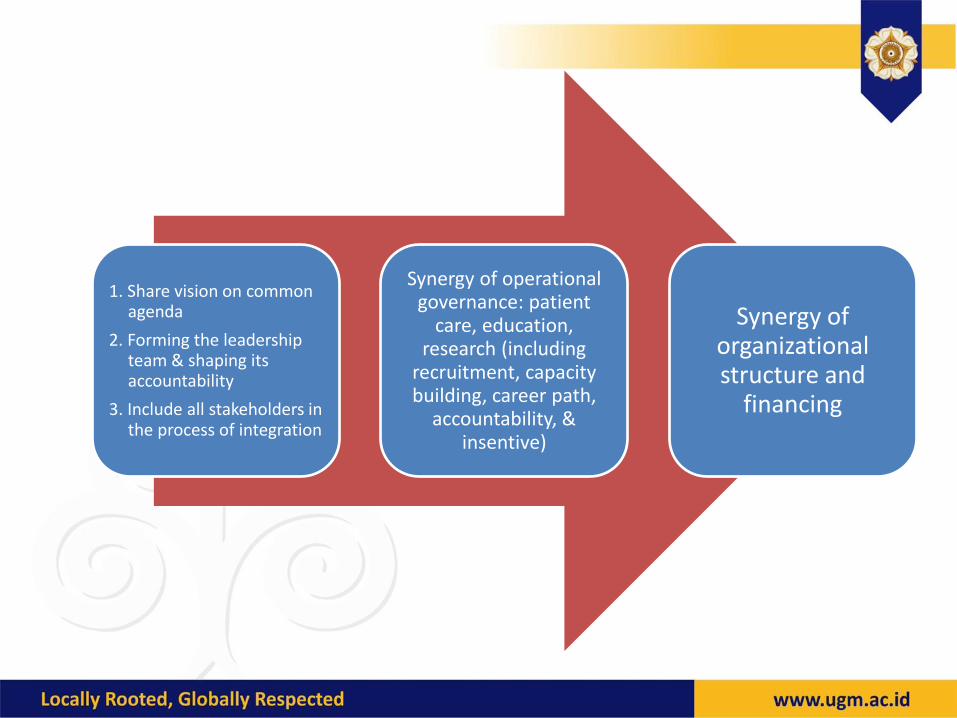
1. Share vision on common agenda
2. Forming the leadership team & shaping its accountability
3. Include all stakeholders in the process of integration
Synergy of operational governance: patient
care, education, research (including
recruitment, capacity building, career path,
accountability, & insentive)
Synergy of organizational structure and
financing
Summary
• Academic Health System, with one established faculty of medicine, university hospitals, referral hospitals, and primary care in surrounding areas seems promising because lack of facilities, workforces, and funding could be shared together to improve community health care
• All effort should be made to share the idea to all
stakeholders: government, universities, all ministry involved to fasten the program
• Key success factors of AHS: Optimal Leadership, Strategic Organization, & Good Governance
Acknowledment
• Prof. dr. Ali Ghufron Mukti, MSc., PhD. • Prof. DR. dr. Teguh Aryandono, SpBK (Onk) • Prof. dr. Ova Emilia, PhD. • dr. M. Syafak Hanung, MSc., SpA • Prof. dr. Arif Faisal, SpRad • Prof. dr. Budi Mulyono, SpPK, PhD. • Prof. dr. Laksono Trisnantoro, PhD. • dr. Alida Lienawati, Mkes. • et all.
