advanced biometry for advanced lenses - eyeworld...advanced biometry for advanced lenses advanced...
TRANSCRIPT
Advanced biometry for advanced lenses
www.eyeworld.org Advanced IOL platform provides benefits for surgeons and patients
2013 ASCRS•ASOA San Francisco Show Daily Supplement This Show Daily supplement is sponsored by Alcon.
The Lenstar helps increase refractive accuracy for patients,especially those with advancedIOL options
Today’s cataract patients,and especially those withpremium lenses, havelearned to anticipate nothing short of excellent
postoperative vision, and using themost advanced biometry preopera-tively helps us achieve that goal forour patients. Accuracy in IOL powercalculations requires precise meas-urements, including axial length,lens thickness and keratometry, toprovide the best estimate of the effective lens position by advancedformulas.
In my opinion, the LenstarLS900 (Haag-Streit AG, Koeniz,Switzerland) goes beyond what wegenerally expect from a biometer.The autokeratometry feature is bothprecise and uniquely suited to thetoric IOL; a total of five axial meas-urements (central corneal thickness,aqueous depth, anterior chamberdepth, lens thickness, and axiallength) are by optical biometry.Every aspect of every measurementprocess is open to physician inspec-tion, validation, and correction.
K readingsThe Lenstar LS900 uses dual-zonekeratometry, with two concentricrings of 1.65 and 2.30 mm. The 16measurement points in each ringcomprise a total of 32 measurementpoints. Each displayed K reading is acomposite of four measurements,representing 128 measurementpoints. Performing five scans is rec-ommended, which generates a totalof 640 individual measurements pereye. Because the greatest distancethat any measurement can be from aprincipal meridian is only 11 degrees, the K readings are uniquelysuited for identifying the steep andflat meridians and the power differ-ence between them, a requirementof the AcrySof toric IOL calculator(Alcon, Fort Worth, Texas). The Kmeasurements can also be used withthe ASCRS online post-keratorefrac-tive surgery IOL power calculator.Comparatively, the IOLMaster (CarlZeiss Meditec, Dublin, Calif.) meas-ures only three points above andbelow the horizontal at 60 degrees,120 degrees, and 180 degrees.
With the Lenstar, each buttonpush generates four displayed images, and if any displayed meas-urement point is not well formed,it’s an indication the information inthat quadrant may not be accurate.
(This is fairly common with moder-ate dry eye patients.) Users can eas-ily repeat measurements until thequality is sufficient. In this way,there are far fewer keratometric surprises than might be seen by simply looking at numbers with noother information.
We recently reported that theuse of the dual-zone keratometryfeature of the Lenstar in toric IOLswas equivalent to manual Ks.1 Wealso proposed validation criteria,with the proposed values for thestandard deviation to achieve supe-rior refractive results at 0.25 D orless for the K readings and 3.5 degrees or less for the axis.
The repeatability of this biome-ter is unsurpassed. What has im-pressed me is that working with the combination of the Lenstar and advanced formulas like Haigis,Holladay 2, and Olsen, our out-comes are now tighter. It’s the firstautomated biometer with keratome-try accurate enough for me to trustit completely for my toric lens calcu-lations.
Precise axial length and lens thicknessThe company notes its optical co-herence technology uses a superlu-minescent diode as a light source toallow axial length measurementseven through dense cataracts. Axialmeasurements include the anteriorand posterior cornea, aqueousdepth, anterior chamber depth, lensthickness, and the full length of theeye. The device segments the eyeinto three areas—cornea and aque-ous, lens, and posterior segment—and combines the data from thosethree segments to produce an overallaxial length. In addition, the measurements are displayed in thefamiliar immersion A-scan format,making it easy to identify the loca-tions of basic structures. Addition-ally, incorporating a measured lensthickness into the Holladay 2 for-mula increases refractive accuracy. A measured lens thickness is an important component of the Olsenformula as well. Having both the
Warren E. Hill, MD
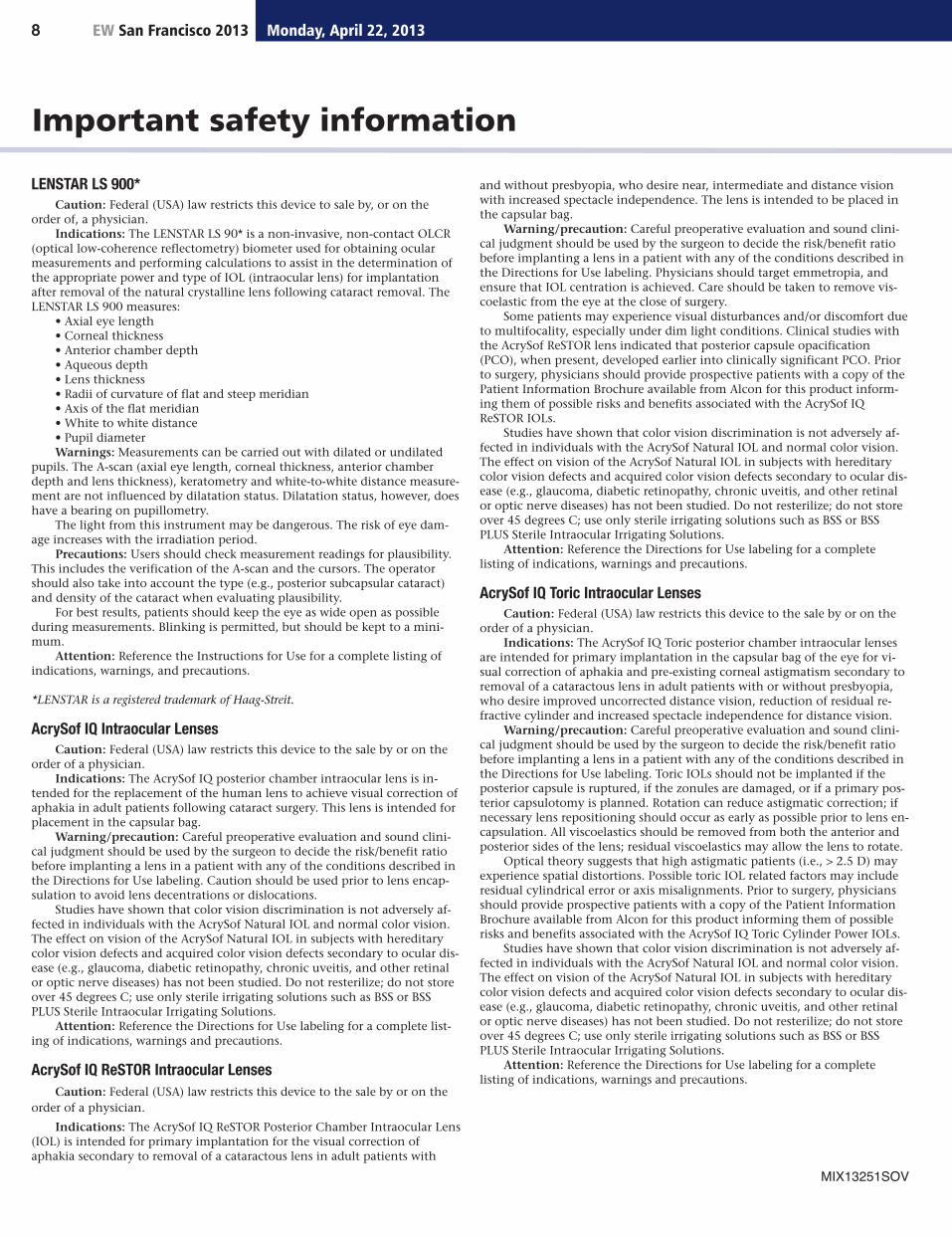
The Lenstar provides the key biometry readings. Source: Haag-Streit
This supplement was produced by EyeWorld and sponsored by Alcon. Thedoctors featured in this supplement received compensation from Alcon for their contributions to this supplement.
Copyright 2013 ASCRS Ophthalmic Corporation. All rights reserved. The viewsexpressed here do not necessarily reflectthose of the editor, editorial board, or the publisher, and in no way imply endorsement by EyeWorld or ASCRS.
by Warren E. Hill, MD
continued on page 2
Please refer to page 8 for important safety information about the Alcon products described in this supplement.
“This precisionmakes the Lenstar anexcellent device forsurgeons who are
looking to optimizetheir outcomes for all patients, as well
as expand their premium lens patient
population.”

2
anterior chamber depth and the lensthickness measurements by opticalbiometry allows the user access to allthe features of the most advancedformulas.2
Expanding your premium lenspopulationBecause of increased precision withbiometry, it is likely that a higherpercentage of our premium lens pa-tients will have accurate outcomes.Combined with newer generationformulas (Holladay 2, Haigis, andOlsen), the Lenstar represents the current state-of-the-art optical biometer.
The Lenstar is, in short, chang-ing how we approach the process ofIOL power calculations. By allowingthe user access to every part of themeasurement process, along withthe ability to edit the results againstvalidation criteria, there is a signifi-cant increase in the control over thefinal accuracy. This precision makesthe Lenstar an excellent device forsurgeons who are looking to opti-mize their outcomes for all patients,as well as expand their premiumlens patient population.
References1. Hill WE, Osher R, Cooke D, et al. Simulationof toric IOL results comparing manual ker-atometry to dual-zone automated keratometryfrom an integrated biometer. J Cataract Refract Surg. 2011; 37 (12): 2181-2187.2. Lam S. Comparison of age-derived lensthickness to optically measured lens thicknessin IOL power calculation: a clinical study. J Refract Surg. 2012;28(2):154-155.
Dr. Hill is in private practice, East Valley Ophthalmology, Mesa, Ariz. He can be contacted at 480-981-6130.
EW San Francisco 2013 Monday, April 22, 20132
Achieving optimal outcomeswith multifocal IOLs
Advanced continued from page 1
Preop evaluation and intraopastigmatism management arecritical to success
Particularly as new IOLs become available, and asmore Baby Boomers requirecataract surgery, interest inrefractive options will
continue to climb. Most ophthal-mologists believe that appropriatecataract patients should be informedabout these options as part of thesurgical informed consent. Deter-mining which patients are good candidates for a multifocal IOL is acomplex process, but if properly selected and informed, a certain per-centage of our cataract populationwill be thrilled with the results.
Careful patient selection and effective preoperative education andcounseling are time consuming, butextremely important. Patient satis-faction is very much a function ofpreoperative expectations, and ourmessaging competes with the inter-net, boastful friends, comparison toLASIK, and the power of suggestionthat they will be rid of eyeglasses.Understandable and effective com-munication about expectations isjust as important as the ability tomake a proper capsulorhexis. I beginpreoperative education by mailinghandouts and my modification ofthe Dell refractive questionnaire toall cataract patients prior to their ap-pointment. These carefully wordedhandouts explain presbyopia andastigmatism and the non-coveredelective refractive options, so that
patients will be better prepared tomake a decision regarding their IOL.
Creating a multifocal optic withtwo disparate focal points entailssome optical compromise. Preopera-
tive preparation and the patient’spersonality and motivation can facilitate adaptation to unwantedimages such as halos. Summationfrom bilateral multifocality helps to
by David F. Chang, MD
“Determining whichpatients are goodcandidates for a
multifocal IOL is acomplex process, butif properly selected
and informed, a certain percentage of
our cataract population will be thrilled with the results.”
David F. Chang, MD
Please refer to page 8 for important safety information about the Alcon products described in this supplement.
Preoperative right and left eye topography and wavefront analysis of apatient who desires a multifocal IOL. The corneal higher order aberrations(within the green outline) are computed from the same corneal diameter as the patient’s scotopic pupil. The high amounts of coma and sphericalaberration increase the risk of poor visual quality with a multifocal IOL.
Source: David F. Chang, MD
continued on page 3

Brad Black, MD
offset the slight reduction in con-trast sensitivity. However, thesesame tradeoffs mean that the multi-focal IOL performance is very unfor-giving of any additional optical orfunctional compromise. Poor imagequality may result from residual re-fractive error, poor centration, andotherwise minor concomitant ocularabnormalities, such as a subtleepiretinal membrane or an irregularocular surface.
Preoperative testingAppropriate attention has beengiven to assessing the macular pre-operatively, and spectral domainOCT allows us to evaluate its ultra-structural anatomy. However, al-though the slit lamp exam confirmscorneal clarity, cataract surgeonshave historically tended to overlookthe optical quality of the cornea,which may be impaired by an un-even or abnormal ocular surface. Topography provides a qualitativeassessment of the corneal surfaceand may reveal irregular steepeningor an abnormal contour.
Many topographers now offeradditional software analysis that cal-culates the wavefront of the anteriorcorneal surface. Wavefront analysisadds quantitative data about moresubtle higher order aberrations(HOAs) that increase the risk of poorimage quality with a multifocal IOL.I use the iTrace (Tracey Technologies,Houston), which can computecorneal HOAs from only the area ofthe cornea overlapping the patient’sscotopic pupil diameter. I particu-larly worry about RMS values of 0.2microns or more of corneal coma orspherical aberration and will usuallyrecommend against placing multifo-cal IOLs in these eyes.
The astigmatism factorThere is no question that the opticalperformance of multifocal IOLs ismuch less tolerant of residual refrac-tive error compared to monofocalIOLs. Adaptive optics wavefrontstudies from Scott MacRae, MD,and colleagues at the University ofRochester show that this is particu-larly true for astigmatism.1
Astigmatic keratotomy is an important adjunct technique foreyes undergoing multifocal IOL im-plantation. Preoperatively, it is im-portant to discuss the possible needfor postoperative excimer laser en-hancement of residual astigmatismand spherical error.
Intraoperative aberrometryIntraoperative wavefront aberrome-try offers the potential to improvethe refractive outcome for any eye.For multifocal IOL patients, intraop-erative pseudophakic measurementsmay help surgeons to minimizeresidual refractive cylinder.
These intraoperative wavefrontaberrometry devices attach directlyto the operating microscope andhave the advantage of assessing notjust the cornea, but the entire ocularrefractive state. Pseudophakic meas-urements allow surgeons to make intraoperative adjustments, such astoric IOL alignment. Three potentialshortcomings of relying on preoper-ative keratometry or topography areaddressed by an intraoperative meas-urement. First, the wavefront refrac-tion will include the contribution ofany posterior corneal astigmatism.Second, any astigmatic change induced by the surgical incisionshould be accounted for. Finally, thesurgeon will not be misled if the
patient’s head was tilted during pre-operative keratometry or topographymeasurements by the technician.The refractive cylinder axis will beapparent without the need for exter-nal reference landmarks.
The value propositionWith multifocal IOLs we walk a fineline in an effort to maximize func-tional convenience while minimiz-ing optical compromise. The IOLtechnology alone doesn’t assuregood results because this delicatebalance can be upset by residual refractive error, subtle macular,corneal, or ocular surface abnormali-ties, and insufficient neuroadapta-tion to unwanted images. Overlyoptimistic patient expectations arepotentially problematic because ofour inability to fully control all ofthese factors. Nevertheless, premiumrefractive IOLs are the patient valueadded proposition that restoresproper value to our skills as cataractsurgeons and clinicians. Many patients want to have refractive options and expect us to help themdecide what might best meet theirneeds.
References1. Zheleznyak L, Kim MJ, MacRae S, Yoon G.Impact of corneal aberrations on through-focus image quality of presbyopia-correctingintraocular lenses using an adaptive opticsbench system. J Cataract Refract Surg. 2012;38: 1724-1733.
Dr. Chang is clinical professor of ophthalmol-ogy, University of California, San Francisco,and in private practice, Los Altos, Calif. He canbe contacted at 650-948-9123.
EW San Francisco 2013 3
Achieving continued from page 2
Attention to detail
by Brad Black, MD
Advanced IOL platform provides benefits for surgeons and patients
“As opposed tolooking for things
that might ‘qualify’ apatient for a
multifocal IOL, wesuggest the surgeonlook at every patient
as a potential candidate for a
multifocal lens, andthen determine
if there any contraindications
to the lens.”
Minimizing compromise withthe ReSTOR IOL +3 add
Both perioperative and intraoperative approachesto optimizing outcomeswith multifocal IOLs haveevolved significantly over
the past few years, largely due to ourincreased knowledge of how to en-sure maximum patient satisfaction.While we know patient selection is amajor influence, other factors such
as capsulotomy size and shape, IOLpositioning and orientation, and aggressive treatment of ocular sur-face disorders as well as even smallamounts of residual refractive errorare equally important. Advances intechnology, such as the +3 multifo-cal IOLs (including the AcrySof*ReSTOR* IOL +3, Alcon, Fort Worth,Texas), offer the advantage of excel-lent near vision with minimal com-promise of intermediate acuity.
Realistic expectationsWhen a patient expresses an interestin spectacle freedom for near anddistance tasks, we consider him orher a potential candidate for multi-focal lenses. In addition to a thor-ough eye exam and patient history,we look at the patient’s lifestyle, expectations, and personality. Is this person adaptable? Is he or shemotivated to be without glasses?
We attempt to establish realisticexpectations for the patient. In my
continued on page 4

4 EW San Francisco 2013 Monday, April 22, 20134
way of thinking, that means we tellpatients we’re confident the lens willallow for their best chance of specta-cle freedom. We explain that if thelighting is not adequate, the print isvery small, or the contrast is inade-quate for what they’re reading, theymight require some help with mag-nifiers. While those scenarios are arare occurrence, patients need toknow that this is a possibility. Wealso want them to anticipate a dis-tinct ring around lights at night. Wetell patients that this isn’t a matterof “if it happens,” but “when it happens,” and that it means “theimplant is working.” Explain thatthese “rings,” which may seem particularly bothersome prior to theadaptation process, become almostunnoticeable over time; that is veryreassuring to patients.
Identifying contraindicationsAs opposed to looking for thingsthat might “qualify” a patient for amultifocal IOL, we suggest the sur-geon look at every patient as a po-tential candidate for a multifocallens, and then determine if thereany contraindications to the lens. I recommend surgeons start at theback of the eye and work forwardwhen evaluating the clinical qualifi-cations of a potential multifocal patient. We look for retinal issues—such as diabetic retinopathy, macu-lar degeneration, or epiretinalmembranes—that might reduce con-trast sensitivity. We look at the opticnerve, assessing it for glaucomadamage, neuropathy, or optic atro-phy. We evaluate the lens for loosezonules or traumatic subluxation. Finally, we look for anything prob-lematic on the cornea, such as ectasia, ocular surface disease, highdegrees of astigmatism (which arebetter treated with toric IOLs), oreven previous refractive surgery. Pa-tients with expected postoperativeastigmatism >1.0 D may not achieveoptimal visual outcomes. It’s beenmy experience that, even if treated,there is enough reduction in con-trast sensitivity to interfere with thepatient’s quality of vision.
Pearls for multifocal lensesIt is generally felt that reducing incision size will lessen surgically induced astigmatism (SIA). In con-verting to a 2.2- or 2.4-mm incision,the surgeon may simply use thesame technique, instrumentation(except for a smaller phaco tip andsleeve), and even fluidic parametersas used with a larger incision. In myexperience, the smaller incision hasresulted in more predictable out-comes by reducing SIA.
Orienting a multifocal lens ver-tically (with the footplate at the 12and 6 o’clock positions) allows forbetter consistency in maneuveringthe lens to the visual axis. With avertically oriented lens, it’s mucheasier to “nudge” the IOL nasallywhen needed. I ask the patient tolook directly at the microscope light.Because of the central diffractivezone the lens has a “bull’s eye” thatallows for easy alignment. My adviceto those without a great deal of mul-tifocal IOL experience: Don’t beafraid to rotate the lens away fromthe vertical axis. Orient the lenshowever necessary to ensure thelight reflex is directly centered onthe lens.
Another pearl: Avoid touchingthe optic of the implant at all times.I recommend maneuvering the im-plant with a soft tip I/A instrumentrather than forceps or hooks.
It is very important that the an-terior capsule overlap the optic for360 degrees. Some excessive overlapor even a slightly smaller capsulo-tomy is preferable to a larger capsu-lotomy that might not ensureoverlap. Without this anterior cap-sule overlap, centration and effectivelens position may be significantly affected.
ReSTOR +3: A “quantum leap”forwardIn my experience, the asphericReSTOR +3 multifocal IOL is a signif-icant improvement over earlier ver-sions. The range of vision the +3provides is much more in line withthe needs of today’s patient—visionthat is not only excellent at near butalso at intermediate distances.1 The+4 simply didn’t provide adequateintermediate vision for our premiumlens patients. In Figure 1, the defo-cus curve of the +3 clearly providespatients a much better range of vi-sion than the +4, with intermediatevision “only” dropping to the 20/25-30 level. The +3 is a quantum leapforward, a significant improvementover previous lenses, and certainlyworth trying for any surgeon previ-ously disenchanted with the earliermultifocal IOLs.
Surgical timingWith multifocal IOLs, I prefer per-forming bilateral surgery a bit closertogether. It’s been my experiencethat patients adapt better to thetechnology if the implants are donea week or two apart, even soonerwhen schedules permit. The closertogether the surgeries, the faster thepatient seemingly adapts to thetechnology. There are some surgeonswho argue that bilateral surgeries
spaced weeks apart allow the patientto determine whether or not themultifocal lens was a good choiceand if not, convert the contralateraleye to a monofocal lens. In my opin-ion, maybe these patients (similar tothose who require an hour-long dis-cussion about the multifocal IOL)are not good candidates for the implant in the first place. I wouldagree, however, that unilateral mul-tifocal IOLs can, at times, be verywell tolerated with an opposite eyethat is either phakic or pseudopha-kic with a monofocal IOL.
Minimizing compromiseNo matter which method of correct-ing “surgically induced, pseudopha-kic presbyopia” we are choosingright now, there are some compro-
Please refer to page 8 for important safety information about the Alcon products described in this supplement.
Figure 2: The ranges of visual acuity achievable with the AcrySof IQ ReSTOR IOL +3.0 D and +4.0 Dmodels
Source: AcrySof IQ ReSTOR Directions For Use
Figure 1: The best case mean defocus curves in cataract patients at six months postop who hadreceived either the AcrySof IQ ReSTOR IOL +3.0 D or +4.0 D
Source: AcrySof IQ ReSTOR Directions For Use
Attention continued from page 3
mises you—and your patients—willneed to accept. What we’re trying todo is minimize compromises andfind those that patients can adapt to most readily. That’s why I’m astrong believer in multifocal lenses.Cataract surgeons who are not yetembracing these lenses are missing abig opportunity.
*AcrySof, ReSTOR, and IQ ReSTOR aretrademarks of Novartis.
Reference1. AcrySof ReSTOR IOL +3 Directions For Use
Dr. Black is founder of Eye Associates, Jeffersonville, Ind. He can be contacted at [email protected].

James McCulley, MD
Offering an excellent standardlens to cataract patients
The AcrySof* (Alcon, FortWorth, Texas) line of IOLsis, in my opinion, a fantas-tic design platform formonofocals, multifocals,
and toric lenses. The AcrySof IQmonofocal IOL has lived up to itspromise not only as a monofocal,but also a foundation upon whichpresbyopic and astigmatic correctioncan be applied in the multifocal andtoric platforms.
The basic platform features asingle-piece design with excellentbiomechanics and unsurpassed bio-compatibility in the lens materi-als.1,2,3 For patients seeking excellentdistance vision who don’t want topay out of pocket and/or do notmind wearing glasses after surgery,using a monofocal lens for theircataract surgery is economically fea-sible and easy. Knowing I’m using alens that has advanced optics formaximum refractive clarity for mypatients gives me even more peaceof mind. For these and many morereasons, the AcrySof IQ IOL is mylens of choice.
Biomechanics and designThe AcrySof IQ monofocal IOL hastraditionally been the true platformof the AcrySof line. Biomechanically,it centers in the bag and adheresrapidly, something particularly im-portant for premium lenses. The lenshas a square edge, which, combined
with the excellent centration, reduces the incidence of posterior required YAGs.4 In fact, the Nd:YAGrates published in the AcrySof IQIOL Directions For Use are lowerthan the rates included in othermanufacturers’ product labeling (although not all manufacturers include this information in theirproduct labeling).5
Also minimizing YAG rates isthe bioinert hydrophobic acrylatematerial used in the AcrySof line.This proprietary material is neitherbiostimulatory nor biotoxic to theepithelial cells left behind. The lens material also offers superior fibronectin affinity to the anteriorcapsule,1 which increases the chanceof adhesion to the capsular bag.When the capsulorhexis overlapsthe optic of the lens by as little as 1mm, the result is a “sandwich” struc-ture, with the lens sandwiched inplace between the anterior and pos-terior capsules. According to thistheory, the overlap prevents furtherproliferation of lens epithelial cells.6
The AcrySof lens platform fea-tures an aspheric design, which wasdeveloped with a negative sphericalaberration to counteract the positivespherical aberration in the averagecornea. This improves quality of vision and contrast sensitivity.
The incidence of glistenings inIOLs has been a hot topic recently.To some degree, all lens materialshave microvacuoles that can be ob-served under the slit lamp and arecalled “glistenings.”7 I’ve observedthem in the AcrySof lens material,but in my hands, they have neverhad any clinical significance. I’venever had a patient complain aboutthem. AcrySof lenses manufacturedtoday have reduced the incidence ofthese microvacuoles by 87%.8
Ideal lens designIn an ideal world, any lens weplace in the eye would recreatethe characteristics of a naturallens present in a young per-son. The blue light filteringchromophore mimics lighttransmissibility of the naturalhuman lens and has beenadded onto the AcrySof IQ IOLplatform. Without the chro-
mophore, blue light is transmittedthrough to the retina that the retinawas not designed to see, nor hasadapted to see. I opt against creatingan unnatural situation in the eye.Implanting the AcrySof IQ IOL toavoid blue light makes sense.
A “go-to” lensThe AcrySof IQ IOL is my go-tomonofocal lens and has been mypreferred lens for years. It offers advanced design, excellent visualquality, and the lowest labeledNd:YAG rates of all lenses currentlyon the market. For cataract patients,it is a sensible and financially viablechoice.
Moreover, the AcrySof IQ IOLplatform offers exciting possibilitiesfor premium lens technology. Ifirmly believe the high quality de-sign, biomechanics, and biocompati-bility make AcrySof an excellentplatform for all existing lenses andoffer unparalleled promise for pre-mium lenses of the future.
*AcrySof is a trademark of Novartis.
References1. Linnola RJ, Sund M, Ylonen R, Cand M, Pihlajaniemi T. Adhesion of soluble fibronectin,laminin, and collagen type IV to intraocularlens materials. J Cataract Refract Surg.1999;25:1486-1491.2. Oshika T, et al. Adhesion of lens capsule tointraocular lenses of PMMA, silicone, andacrylic foldable materials: an experimentalstudy. Br J Ophthalmol. May 1998; 82:468.3. Lane SS, Burgi P, Milios GS, Orchowski MW,Vaughan M, Schwarte E. Comparison of thebiomechanical behavior of foldable intraocularlenses. J Cataract Refract Surg.2004;30:2397- 2402.4. Schmidbauer J, Vargas L, Apple D, Escobar-Gomez M, Izak A, Arthur S, Golescu A, Peng Q.Evaluation of neodymium:yttrium–aluminum–garnet capsulotomies in eyes implanted withAcrySof intraocular lenses. Ophthalmology.2002;109(8):1421-6. 5. AcrySof IQ Directions For Use6. Reijo J, Linnola. Sandwich theory: Bioactiv-ity-based explanation for posterior capsuleopacification. J Cataract Refract Surg.1997;23:1539-1542.7. Werner L. Glistenings and surface lightscattering in intraocular lenses. J Cataract Refract Surg. 2010;36:1398-1420.8. Data on file
Dr. McCulley is chair of ophthalmology, University of Texas Southwestern MedicalCenter, Dallas. He can be contacted at 214-648-3407.
EW San Francisco 2013 5
The AcrySof IQ monofocal: a platform IOL
by James McCulley, MD
Advanced IOL platform provides benefits for surgeons and patients
“The AcrySof IQ has the lowest
labeled Nd:YAG rate of all currently
available IOLs.”
AcrySof IQ IOLSource: Alcon

John Berdahl, MD
6
Toric lens success depends on stability
Toric IOLs are an ideal option forastigmatic cataract patients with .75D of corneal astigmatism or greater.They address a known problem, onethat is intuitive and logical to pa-tients. Just as I would not prescribespectacles to patients without cor-recting astigmatism, it would makeno sense to me not to offer a toriclens to my cataract patients.
Toric lenses are more predictablethan limbal relaxing incisions (LRIs)or astigmatic keratotomy (AK) in patients with more than 0.75 D ofastigmatism. Incisional techniqueshave a less predictable healing re-sponse, and (if using a manual LRItechnique) surgeons need to con-sider the variability in incisiondepth, arc, and angulation.
The AcrySof* IQ toric IOL(Alcon, Fort Worth, Texas) featuresthe aspheric technology and refrac-tive clarity of the AcrySof platform.Its excellent rotational stabilitymakes treating corneal astigmatismin cataract patients very simple.
Rotational stability, lens placementThere cannot be enough emphasison how crucial rotational stability isin a toric lens.
The AcrySof lens material has aunique “tackiness” and has beenshown to have greater fibronectinbinding than other IOL materials,which promotes adhesion to thecapsule (Figure 1).1 This bond be-tween the anterior and posteriorcapsule helps to stabilize the lens inplace and contributes to the rota-tional stability of the lens.2
Delivering the lens in the capsu-lar bag is equally important. Wewant a lens that’s flexible enough tobe easily positioned to align on theaxis. At the same time, we want alens that is stable enough that thecontraction forces of the capsularbag won’t vault or distort the lens.
The AcrySof platform is a nicebalance between these two features.The single-piece platform’s combina-tion of material and Stableforce hap-tics keep the AcrySof IQ toric lensstable and centered in the capsularbag, while the flexible haptic designallows for optimal placement in thebag, regardless of size.
EW San Francisco 2013 Monday, April 22, 20136
Toric IOLs: Are they all the same?by John Berdahl, MD
“The AcrySof lensmaterial has a unique‘tackiness’ and hasbeen shown to havegreater fibronectinbinding than other
IOL materials … Thisbond between the
anterior and posteriorcapsule helps to
stabilize the lens inplace and contributes
to the rotational stability of the lens.”
Please refer to page 8 for important safety information about the Alcon products described in this supplement.
Unfolding of the hapticsAn aspect of the AcrySof platform Iparticularly appreciate is the speedat which the haptics open in thebag. Surgeons have the appropriatetime (about 10-20 seconds) to ma-nipulate the lens into its rough posi-tion before it is fully unfolded; thoseof us using intraoperative aberrome-try to refine outcomes enjoy that thelens unfolds relatively quickly.
One pearl: Ensure the hapticsare entirely unfolded when the caseis finished, and completely removethe viscoelastic from behind theIOL. Then just “tap” the center ofthe lens posteriorly, so there is con-tact between the posterior capsuleand the lens. If a surgeon realizes inthe OR the lens has not been prop-erly aligned, my advice is to put alittle viscoelastic under the lens, androtate (always clockwise as the hap-tics move more freely in that direc-tion) the lens to the proper position.
Clinical pearl: Finding the ideal axisFinding the ideal axis is the mostimportant and sometimes the mostchallenging aspect of toric IOL im-plantation. Although this does notoccur often, sometimes the lens isexactly where we intended to placeit—but that location is not the idealaxis. Differentiating between the intended and ideal axis is necessaryfor these lenses.
If there is residual astigmatismpostoperatively, there are two op-tions: perform laser vision correctionor return the patient to the OR androtate the lens. David Hardten, MD,and I developed an online tool thatis hosted by ASCRS that can help
surgeons, www.ascrs.org/toric-results-analyzer. Surgeons input themanifest refraction, what toric lensis being used and its axis, and thesite will calculate where the lensshould be rotated to and estimatethe new refraction. The key issuesfor surgeons to consider are whetherthe spherical equivalent is accept-able and whether the residual astig-matism is acceptable. I personallyfind that anything under 0.50 D ofresidual astigmatism is usually notnoticeable to patients.
A quality lens platformIn my hands, the AcrySof IQ toriclens tackles some of the most chal-lenging issues of toric lenses throughits material and design, and pro-duces great alignment, adhesion tothe bag, and most importantly, ex-cellent rotational stability. As wecontinue to advance into more so-phisticated toric lenses and multifo-cal torics, I believe this lens platformwill evolve seamlessly with us.
*AcrySof is a trademark of Novartis.
References1. Linnola RJ, Sund M, Ylonen R, et al. Adhesion of soluble fibronectin, laminin, collagen type IV to intraocular lens materials.J Cataract Refract Surg. 1999;25:1486-1491.2. Linnola RJ. Sandwich theory: Bioactivity-based explanation for posterior capsule opaci-fication. J Cataract Refract Surg.1997;23:1539-1542.
Dr. Berdahl is in private practice, VanceThompson Vision, Sioux Falls, S.D. He can becontacted at 605-328-3937.
Figure 1Source: Alcon

James A. Davison, MD, FACS
7
When should you use a toric IOL forvisually significant corneal astigmatism?by James A. Davison, MD, FACS
Advanced IOL platform provides benefits for surgeons and patients EW San Francisco 2013
“Even when usingan average SIA of
0.25 D and anteriorkeratometric astigmatism
measurement, themean postoperativerefractive astigma-
tism was statisticallysignificantly lowerwith toric IOLs thanwith spherical IOLs
(0.31 D versus 1.06 D;P<0.001).”
Clinic’s best machines and practices,show 7% of my patients have resid-ual spherical equivalent of 0.75 D ormore.
Toric lenses are quite appropri-ate for patients with keratometricastigmatism between 0.75 and 1.38D. Even when using an average SIAof 0.25 D and anterior keratometricastigmatism measurement, the meanpostoperative refractive astigmatismwas statistically significantly lower with toric IOLs than withspherical IOLs (0.31 D versus 1.06 D;P<0.001).3 Hill reported SIA becomesa more significant issue for patientswith lower levels of cylinder.4
Intraoperative aberrometry oneach case may be an ideal option,but those of us without the technol-ogy use an average SIA derived fromour own experience. I’ve found 2.2to 2.4 mm incisions will induceabout 0.25 D of astigmatism on average; that’s what I use in toriccalculations. As Ernest and Potvinfound: “the lower the degree ofastigmatism induced at the time ofsurgery, the more precise the postop-erative correction is likely to be because the variability in that SIAwill be lower and lower.”3
Flipping axesIf we ignore the SIA, we can say that postoperative refractive cylindermagnitude is independent of preop corneal astigmatism axis orientation.3 In essence, that meansthat a patient with 0.75 D of preopastigmatism may be corrected with atoric IOL value of 1.0 D—leavinghim with 0.25 D in the other direc-tion. Some may argue that “flip-ping” the axis creates more of an
issue or thatastigmatism pro-vides increaseddepth of focus. Ibelieve that it’smore the magni-tude of astigma-tism that affectsuncorrected vision ratherthan the axis ofcylinder.
Corneal vs.lens-based correctionCompared withlimbal relaxingincisions (LRIs),toric IOLs are
Patients with low cylinder—as well as higher levels of astigmatism—can benefit from toric lenses
Warren Hill, MD, eval-uated 6,000 cataractpatients and found18% had at least 1.5 Dof keratometric astig-
matism.1 He also found that 52.6%had at least 0.75 D. So if we confineourselves to thinking about toricIOL correction only for patients withat least 1.5 D astigmatism, we maybe missing more than half the pa-tients who could benefit from thetechnology. It has been shown thatrefractive cylinder becomes substan-tially visually significant somewherearound 1.0 D.2 But when prescribingspectacles or performing LASIK, 0.75D is normally considered significant.In those cases, correction is fairlyeasily achieved because those technologies are direct, extremely accurate, and additional individualvariables are few.
Implanting a lens to do thesame job is similar but has a coupleof additional variables that need tobe considered to produce good results. In order to predict the bestresult, the equation variables thatneed to be included are: preopera-tive measurements of corneal astigmatism and surgically inducedastigmatism. Further, to achievegood uncorrected vision, we mustminimize the residual sphericalequivalent in addition to minimiz-ing refractive cylinder. Without theuse of intraoperative aberrometry,my own data, using Wolfe Eye
more reliable, which translates tobetter postop vision for ourpatients.5 Toric lenses are manufac-tured to tight laboratory specifica-tions that are extremely consistentand thus predictable. LRIs, however,are notoriously unpredictable because they are so variably per-formed, because of the variousamounts the diamond knife willpenetrate, and because the locationsof the arcs are not consistent. In ad-dition, LRIs have a less direct effectthan toric IOLs, i.e., operating onthe cornea’s periphery while tryingto effect a change of shape at the visual axis.
ConclusionsThe key to toric lenses and astig-matic correction is to discuss withpatients that we’re trying to predicttheir results. Surgeons are happierwith higher toric powers because weknow we’ll be able to help someoneimprove his/her vision (presumingwe properly insert and align, ofcourse). But with proper measure-ments including accurate preopera-tive measurements and equipmentand accurately determined variables,we should be able to reduce evensmaller amounts of astigmatism aswell.
References1. Hill WE. Surgeon recommends toric IOL for patients with low corneal astigmatism. EyeWorld Show Daily Supplement. 2010:Boston.2. Wolffsohn JS, Bhogal G, Shah S. Effect ofuncorrected astigmatism on vision. J CataractRefract Surg. 2011;37:454-460.3. Ernest P and Potvin R. Effects of preopera-tive corneal astigmatism orientation on resultswith a low-cylinder-power toric intraocularlens. J Cataract Refract Surg. 2011;37:72-732.4. Hill W. Expected effects of surgically induced astigmatism on AcrySof toric intraocular lens results. J Cataract RefractSurg. 2008; 34:364–367.5. Mingo-Botin D, Munoz-Negrete FJ, KimHRW, Morcillo-Laiz R, Rebolleda G, Oblanca N.Comparison of toric intraocular lenses and peripheral corneal relaxing incisions to treatastigmatism during cataract surgery. JCataract Refract Surg. 2010;36:1700-1708.
Dr. Davison is in private practice, Wolfe EyeClinic, Marshalltown and West Des Moines,Iowa. He can be contacted at 641-754-6200or [email protected]. Pentacam reading at 3.0 mm ring shows total corneal refractive power of
1.0 D at 7.0 degrees vs. anterior sagittal of 0.8 D at 9.7 degreesSource: James Davison, MD, FACS
8
LENSTAR LS 900* Caution: Federal (USA) law restricts this device to sale by, or on the
order of, a physician.Indications: The LENSTAR LS 90* is a non-invasive, non-contact OLCR
(optical low-coherence reflectometry) biometer used for obtaining ocularmeasurements and performing calculations to assist in the determination ofthe appropriate power and type of IOL (intraocular lens) for implantationafter removal of the natural crystalline lens following cataract removal. TheLENSTAR LS 900 measures:
• Axial eye length• Corneal thickness• Anterior chamber depth• Aqueous depth• Lens thickness• Radii of curvature of flat and steep meridian• Axis of the flat meridian• White to white distance• Pupil diameterWarnings: Measurements can be carried out with dilated or undilated
pupils. The A-scan (axial eye length, corneal thickness, anterior chamberdepth and lens thickness), keratometry and white-to-white distance measure-ment are not influenced by dilatation status. Dilatation status, however, doeshave a bearing on pupillometry.
The light from this instrument may be dangerous. The risk of eye dam-age increases with the irradiation period.
Precautions: Users should check measurement readings for plausibility.This includes the verification of the A-scan and the cursors. The operatorshould also take into account the type (e.g., posterior subcapsular cataract)and density of the cataract when evaluating plausibility.
For best results, patients should keep the eye as wide open as possibleduring measurements. Blinking is permitted, but should be kept to a mini-mum.
Attention: Reference the Instructions for Use for a complete listing of indications, warnings, and precautions.
*LENSTAR is a registered trademark of Haag-Streit.
AcrySof IQ Intraocular LensesCaution: Federal (USA) law restricts this device to the sale by or on the
order of a physician.Indications: The AcrySof IQ posterior chamber intraocular lens is in-
tended for the replacement of the human lens to achieve visual correction ofaphakia in adult patients following cataract surgery. This lens is intended forplacement in the capsular bag.
Warning/precaution: Careful preoperative evaluation and sound clini-cal judgment should be used by the surgeon to decide the risk/benefit ratiobefore implanting a lens in a patient with any of the conditions described inthe Directions for Use labeling. Caution should be used prior to lens encap-sulation to avoid lens decentrations or dislocations.
Studies have shown that color vision discrimination is not adversely af-fected in individuals with the AcrySof Natural IOL and normal color vision.The effect on vision of the AcrySof Natural IOL in subjects with hereditarycolor vision defects and acquired color vision defects secondary to ocular dis-ease (e.g., glaucoma, diabetic retinopathy, chronic uveitis, and other retinalor optic nerve diseases) has not been studied. Do not resterilize; do not storeover 45 degrees C; use only sterile irrigating solutions such as BSS or BSSPLUS Sterile Intraocular Irrigating Solutions.
Attention: Reference the Directions for Use labeling for a complete list-ing of indications, warnings and precautions.
AcrySof IQ ReSTOR Intraocular Lenses Caution: Federal (USA) law restricts this device to the sale by or on the
order of a physician.
Indications: The AcrySof IQ ReSTOR Posterior Chamber Intraocular Lens(IOL) is intended for primary implantation for the visual correction ofaphakia secondary to removal of a cataractous lens in adult patients with
and without presbyopia, who desire near, intermediate and distance visionwith increased spectacle independence. The lens is intended to be placed inthe capsular bag.
Warning/precaution: Careful preoperative evaluation and sound clini-cal judgment should be used by the surgeon to decide the risk/benefit ratiobefore implanting a lens in a patient with any of the conditions described inthe Directions for Use labeling. Physicians should target emmetropia, andensure that IOL centration is achieved. Care should be taken to remove vis-coelastic from the eye at the close of surgery.
Some patients may experience visual disturbances and/or discomfort dueto multifocality, especially under dim light conditions. Clinical studies withthe AcrySof ReSTOR lens indicated that posterior capsule opacification(PCO), when present, developed earlier into clinically significant PCO. Priorto surgery, physicians should provide prospective patients with a copy of thePatient Information Brochure available from Alcon for this product inform-ing them of possible risks and benefits associated with the AcrySof IQReSTOR IOLs.
Studies have shown that color vision discrimination is not adversely af-fected in individuals with the AcrySof Natural IOL and normal color vision.The effect on vision of the AcrySof Natural IOL in subjects with hereditarycolor vision defects and acquired color vision defects secondary to ocular dis-ease (e.g., glaucoma, diabetic retinopathy, chronic uveitis, and other retinalor optic nerve diseases) has not been studied. Do not resterilize; do not storeover 45 degrees C; use only sterile irrigating solutions such as BSS or BSSPLUS Sterile Intraocular Irrigating Solutions.
Attention: Reference the Directions for Use labeling for a complete listing of indications, warnings and precautions.
AcrySof IQ Toric Intraocular Lenses Caution: Federal (USA) law restricts this device to the sale by or on the
order of a physician.Indications: The AcrySof IQ Toric posterior chamber intraocular lenses
are intended for primary implantation in the capsular bag of the eye for vi-sual correction of aphakia and pre-existing corneal astigmatism secondary toremoval of a cataractous lens in adult patients with or without presbyopia,who desire improved uncorrected distance vision, reduction of residual re-fractive cylinder and increased spectacle independence for distance vision.
Warning/precaution: Careful preoperative evaluation and sound clini-cal judgment should be used by the surgeon to decide the risk/benefit ratiobefore implanting a lens in a patient with any of the conditions described inthe Directions for Use labeling. Toric IOLs should not be implanted if theposterior capsule is ruptured, if the zonules are damaged, or if a primary pos-terior capsulotomy is planned. Rotation can reduce astigmatic correction; ifnecessary lens repositioning should occur as early as possible prior to lens en-capsulation. All viscoelastics should be removed from both the anterior andposterior sides of the lens; residual viscoelastics may allow the lens to rotate.
Optical theory suggests that high astigmatic patients (i.e., > 2.5 D) mayexperience spatial distortions. Possible toric IOL related factors may includeresidual cylindrical error or axis misalignments. Prior to surgery, physiciansshould provide prospective patients with a copy of the Patient InformationBrochure available from Alcon for this product informing them of possiblerisks and benefits associated with the AcrySof IQ Toric Cylinder Power IOLs.
Studies have shown that color vision discrimination is not adversely af-fected in individuals with the AcrySof Natural IOL and normal color vision.The effect on vision of the AcrySof Natural IOL in subjects with hereditarycolor vision defects and acquired color vision defects secondary to ocular dis-ease (e.g., glaucoma, diabetic retinopathy, chronic uveitis, and other retinalor optic nerve diseases) has not been studied. Do not resterilize; do not storeover 45 degrees C; use only sterile irrigating solutions such as BSS or BSSPLUS Sterile Intraocular Irrigating Solutions.
Attention: Reference the Directions for Use labeling for a complete listing of indications, warnings and precautions.
EW San Francisco 2013 Monday, April 22, 20138
Important safety information
MIX13251SOV