adhd treatment: subtypes and comorbidity
TRANSCRIPT
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 1/22
© 2006 Russell Barkley, PhD
Optimizing ADHD Treatment:Subtypes & ComorbidityOPTI M I ZI NG ADHD Tre a tm e n t :
Sub t ypes and Com orb id i t y
Russel l A. Bark ley, Ph.D.
Research Professor, Department of Psychiatry
SUNY Upstate Medical University
Syracuse, NY
Website: russellbarkley.orgEmail: [email protected]
©Copyright by Russell A. Barkley, Ph.D., 2005
Source: R. A. Barkley (2006)
Attention Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York: Guilford. ( [email protected] or 800-365-7006)
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 2/22
Page 2© 2006 Russell Barkley
Disclosure
• Retirement: State of Massachusetts
• Salary: Medical U of South Carolina (to 6/1/05)
• Speaker/Consultant:
– Eli Lilly Co. (Strattera)
– Shire Richwood (Adderall)
– McNeil and Janssen-Ortho (Concerta)
– Pfizer, Inc.
• Speaking Fees (misc. organizations)
• Grants:
– National Institute of Mental Health (to U of Maryland – J. Schweitzer)
– Department of Education (to Medical U of SC)
– Eli Lilly Co. (to Medical U of SC)• Royalties:
– Guilford Publications
– Compact Clinicals
– J & K Seminars
– New England Educational Institute

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 3/22
Page 3© 2006 Russell Barkley
Consensus Definition
• A Developmental Disorder of:
– Inattention and/or
– Hyperactivity-Impulsivity
• These are largely delays in rate but can be acquired in some cases (20-25%?)
• Developmentally Inappropriate Levels of Symptoms
• Childhood Onset (Symptoms - Impairment)
• Cross-setting Occurrence of Symptoms
• Significant Impairment in Major Life Activities
• Exclusion of Other Disorders (MR, PDD ??, Psychosis)
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 4/22
Page 4© 2006 Russell Barkley
Unresolved Problems with DSM-IV Criteria
• Inattention list may be misnamed
– Its likely executive functioning, e.g. Working memory
• Symptoms are not developmentally referenced
– Need more appropriate items for adults
• Cutoffs are not developmentally referenced
– May have to adjust thresholds if > 16 or < 4 yrs.
• Cutoffs not sex-referenced (lower for girls)
• Duration may be too short for preschoolers: try 1 yr.
• Age of onset of 7 has no validity (childhood)
• Developmental deviance undefined (93%??)• Implies need for parent-teacher agreement
– Blend reports and use history of cross setting impairment
• No requirement for corroboration by others (adults)
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 5/22
Page 5© 2006 Russell Barkley
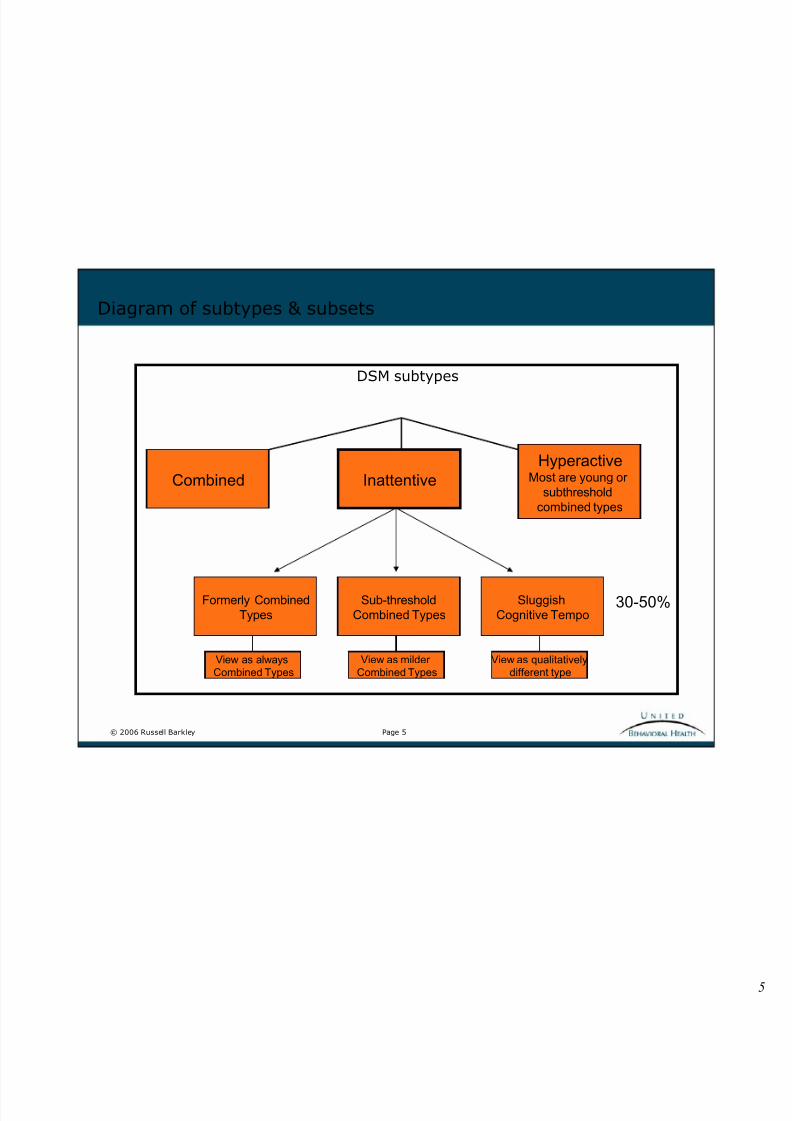
Diagram of subtypes & subsets
DSM subtypes
Combined
HyperactiveMost are young or
subthresholdcombined types
Inattentive
Formerly CombinedTypes
Sub-thresholdCombined Types
SluggishCognitive Tempo
View as alwaysCombined Types
View as milderCombined Types
View as qualitativelydifferent type
30-50%

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 6/22
Page 6© 2006 Russell Barkley
ADHD - Inattentive TypeA Subset May Be A New Disorder
• Known as Sluggish Cognitive Tempo (SCT)
• Comprise 30-50% of Inattentive Type cases
• Common Presenting Symptoms:
– Daydreaming, Spacey, Stares
– Hypoactive, Slow moving, Lethargic, Sluggish
– Easily Confused, Mentally “Foggy”
• Slow, Error Prone Information Processing
• Poor Focused or Selective Attention
• Erratic Retrieval - Long-Term Memory (?)
• Socially Reticent or Withdrawn
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 7/22
Page 7© 2006 Russell Barkley
ADHD Inattentive Type with SCT
• Comorbidity
– Rarely show Aggression or ODD/CD
• Not Impulsive (By Definition)
• Greater risk of anxiety and possibly depression
– If so, consider atomoxetine
• Less Likely to Have a Clinically Impressive Response to Stimulants (only afew studies)
– (65% improve but only 20% show clinical response)
• Possibly Greater Family History of Anxiety Disorders and LD (?)
• Better response to social skills training than ADHD cases are likely to show
• More responsive to behavioral treatments (??)
• More responsive to cognitive therapy (??)
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 8/22
Page 8© 2006 Russell Barkley
Comorbid DSM-IV Disorders
• Oppositional Defiant Disorder (40-80%; odds ratio of 11)
– ADHD contributes to and likely causes ODD
– Some ODD is related to disrupted parenting• Which can arise from parental ADHD
– Predicts persistence of ADHD
• Conduct Disorder (20-56%)/ Psychopathy (20%)
– If starts early, represents a unique family subtype
• More severe, more persistent antisocial behavior
• Worse family psychopathology
• Less responsive to treatment than late onset
– If starts late (>12), more related to social disadvantage, family disruption, & deviant peers
– Father desertion, parent divorce more common – Major depression more likely to co-exist
– School drop out and teen pregnancy more likely

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 9/22
Page 9© 2006 Russell Barkley
• Anxiety Disorders (10-40%) (odds ratio = 3)
– Related in part to poor emotion regulation
– But some legitimate anxiety disorders are likely – Most common are simple phobias or separation anxiety; GAD becomes more common
with age
– Often show lower levels of impulsiveness (better course & outcomes?)
– Anxiety disorders more likely in parents and family
• Major Depression (0-45%; 27% by age 20)
– Likely genetic linkage to ADHD
– Also related to presence of CD in child & family
– Often manifest low self-esteem in childhood
– MDD onset may not be until adolescence or later
• Bipolar Disorder (0-27%; likely 6-10% max.)
– Not documented in any follow-up studies to date
– Some cases are misdiagnosed (ADHD/ODD)
– Requires substitution of severe irritability for mania and chronic for episodic course
– Significant family history of bipolar disorder
– Probably a one-way comorbidity (like Tourette Syndrome)
More Comorbidities
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 10/22
Page 10© 2006 Russell Barkley
More Comorbidities
• Tic disorders
– 10-15% for simple tics; TS is rare
– TS shows one-way comorbidity
• <2% of ADHD, but ADHD occurs in 50-80% of TS
• ADHD is often most impairing disorder in TS
• OCD (rare, 3-4% of adult cases)
– More common in TS cases or TS families
– Risk increases slightly with age
• Sleep disorders (30-56%)
– Mainly delayed onset and greater night waking leading to shorter sleep time
– More activity during sleep
– May exacerbate attention problems in school
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 11/22
Page 11© 2006 Russell Barkley
Comorbidity Affects Treatment Options in Mixed ADHD Cases
Oppositional Defiant Disorder:
• Both stimulants and ATX reduce it markedly
• Often requires adjunctive parent training in behavior managementmethods
– 60-75% successful for children
– 25-35% treatment response after 13+ yrs. of age
• May need to add problem-solving communication training after age 14years
• Severely explosive anger may require use of atypical antipsychotics or
antihypertensives
– (check for childhood bipolar disorder)

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 12/22
Page 12© 2006 Russell Barkley
Conduct Disorder
• Stimulants and ATX reduce aggressive behavior and antisocial acts butstimulants may work more rapidly to gain case control
• Mood stabilizers, atypicals, or antihypertensives may be needed for highlyaggressive/explosive cases
• Parent and family interventions often required
– Problem-solving, communication training
– Multi-systemic therapy where available
– Family relocation to better neighborhoods
• Avoid group treatment formats due to deviancy training by aggressive peers
• Involvement of juvenile justice agencies likely

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 13/22
Page 13© 2006 Russell Barkley
Anxiety Disorders
• More responsive to behavioral therapies
• May respond better to social skills training (and possibly cognitivetherapies)
• Stimulants can exacerbate anxiety
– Studies are conflicting – 7 say it can but MTA study did not find this effect
• Atomoxetine (ATX) reduces anxiety
– Effect Size = .3-.5
• Family counseling may be required to limit family setting induction of anxiety
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 14/22
Page 14© 2006 Russell Barkley
Major Depressive Disorder
Use ADHD drug first if:
– ADHD is chief complaint
– ADHD symptoms are more disabling – MDD is mild: No current functional impairment from depression
– Neuro-vegetative signs are mild
– ADHD symptoms clearly preceded MDD symptoms
Start with Antidepressant first if:
– Clear History of non-response to ADHD drugs
– Prominent neuro-vegetative signs or health is compromised
– MDD symptoms are chief present complaint
– ADHD symptoms are mild, late onset, or coincident with MDD onset.
– Suicidal/Psychotic

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 15/22
Page 15© 2006 Russell Barkley
More on MDD
• May require mixed ADHD/SSRI therapy
• May need cognitive-behavioral therapy
• In parent training programs, use a “go slow” approach to punishmentcontingencies (e.g., time outs, etc.) so as not to contribute to depressivecognitive schemas (self-statements)
– start with all reward programs initially until MDD symptoms lift thenintroduce mild, selective punishments
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 16/22
Page 16© 2006 Russell Barkley
Childhood Bipolar Disorder
• Requires poly-pharmaceutical management for long-term (mood stabilizers,atypicals, anticonvulsants likely)
• Often require periodic hospitalization for safety (suicidality or violence) andstabilization
• Medical management of bipolarity should be done first before managing ADHDsymptoms with ADHD drugs
• Consider all-reward or non-confrontational parent training programs
• Interventions are more likely to be focused on parental coping with explosiveepisodes rather than remediation of disruptive behavior
• Counsel parents on stress management; ADHD/BPD cases have highest ratesof physical abuse and PTSD of all ADHD cases
• Special education (ED) programs are likely
• Adolescent or adult SUDs are likely and require management

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 17/22
Page 17© 2006 Russell Barkley
Tic disorders
• If mild or episodic, require no treatment
• Stimulants may exacerbate tics• ATX does not adversely affect tics
• If tics or TS are socially disabling, consider behavior therapies
– Massed practice, stress management
• If TS is as or more disabling than ADHD, medically manage it first
– (haloperidol, atypicals, antihypertensives)

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 18/22
Page 18© 2006 Russell Barkley
Sleep Disorders
• If severe, consider polysomnograms at a sleep lab
• Treating sleep disorder may improve attention at school
• Stimulants may cause insomnia (30-54% of cases); take care not to worsenproblems
• Consider ATX - no adverse affect on sleep onset
• Advise parents to transition from highly stimulating activities to lesser onesbefore bedtime
• Keep low lighting on in room with background sounds (music)
• Antihypertensive, tricyclic, or chlorhydrate may be needed for short periodsto induce sleep and re-establish new sleep-wake cycle

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 19/22
Page 19© 2006 Russell Barkley
Choosing Medications: Patient Characteristics
• No need for urgent drug response in severe disruptive cases
• Comorbid anxiety/depression
• Comorbid tic disorders
• Pre-existing bedtime or morning behavior problems
• Prior history of drug dependence or abuse
• Adolescents or college students where concern is recreational misuse ordiversion
5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 20/22
Page 20© 2006 Russell Barkley
Issues Related to Stimulants
• Old cases unresponsive to stimulants
• Adverse responses to stimulants
• Significant sleep problems from stimulants
• Significant morning behavior problems from stimulants
• Significant appetite suppression from stimulants
• Significant blunting or constriction of normal affect from stimulants(withdrawn, automaton-like affect)

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 21/22
Page 21© 2006 Russell Barkley
2006 Upcoming Courses
Visit w w w . u b h o n l i n e . c o m for a complete details of upcoming teleconferences and available web courses.
Treatm ent o f Depression and Med ical Com orb id i t y , Charles DeBattista, D.M.H, M.D.
Out come- I n f o rm ed Cl i n i ca l W ork , Scott Miller, Ph.D.
Addressi ng Anx i e t y Comorb i d i t y i n B i po l a r D i so rde r , Michael Otto, Ph.D.
St ra teg ic Trea tm ent o f Depression , Michael Yapko, Ph.D.
Cogn i t i ve Therapy fo r Pa t ien ts w i th Persona l i t y D isorders , Judith Beck, Ph.D.

5/13/2018 ADHD Treatment: Subtypes and Comorbidity - slidepdf.com
http://slidepdf.com/reader/full/adhd-treatment-subtypes-and-comorbidity 22/22
Page 22© 2006 Russell Barkley
Continuing Education Certification
You m u s t complete the attendanceverification form, post-test and course
evaluation to obtain yourCE/CME certificate.
Click here to access the CE/CME formsand print your certificate.