acute inflammatory upper airway obstruction
TRANSCRIPT

Acute Inflammator
y Upper Airway
Obstruction
Dr. S. Ismat Bukhari
• Acute respiratory tract infections are the most common of the acquired infections with an increasing tendency in childhood.
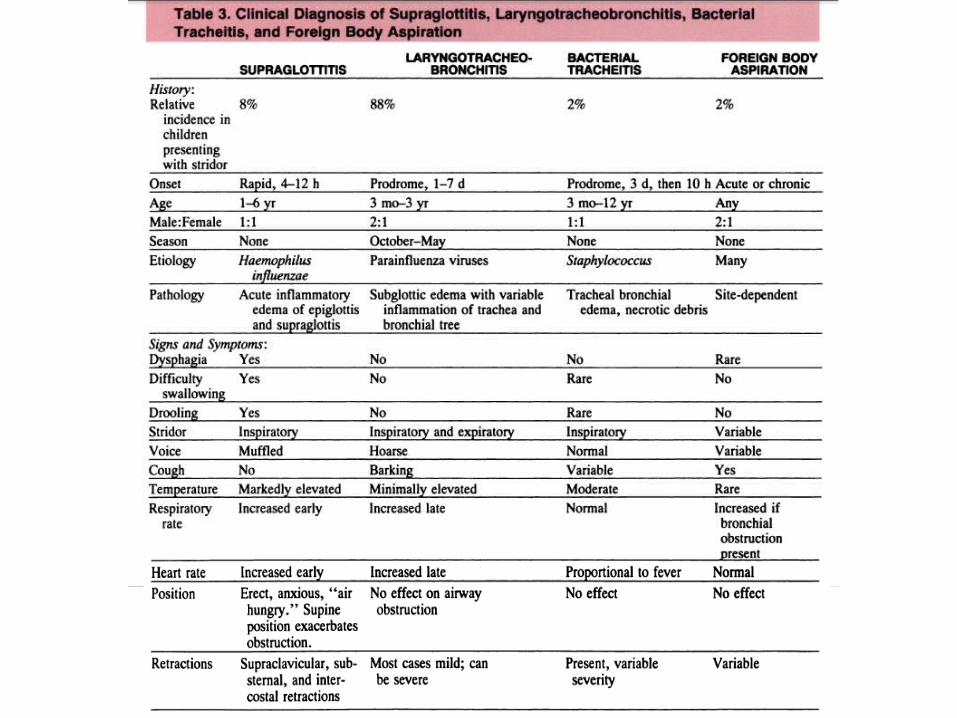
• Out of all the causes that can causes inflammatory obstruction; 89% of the cases are found to be croup, 8% have epiglottitis and nearly 2% have non-bacterial tracheitis.

• Croup (laryngotracheitis) is almost always benign, but very rarely can produce severe obstruction.
• The age of those presenting with epiglottitis is younger than historically described.
• Bacterial tracheitis is a rare but potentially lethal disease that presents with a prodrome similar to that of mild croup and then an abrupt, toxic decompensation.
• Laboratory tests are generally not helpful in the management of these severe cases.

• CROUP
• EPIGLOTTITIS
• LARYNGTIS
• TRACHEITIS
CROUP
• Croup is a disease of viral origin, causing subglottic and tracheal swelling.
• The narrow diameter of the subglottic structures, notably the cricoid ring in the upper trachea, renders the child physiologically vulnerable to inflammation in this area.
• The narrowed airway is responsible for the hallmark of the clinical presentation, which is stridor, and for its physiologic consequence, which is increased respiratory effort.
• Rarely, the child may tire and progress to respiratory failure.
• More than 95% of the patients will not require hospitalization.
• In a toddler, 1 mm of edema will result in a 65% reduction in the cross-sectional area of the subglottis.
• Thick secretions may exacerbate the symptoms.
Epidemiology
• The majority of cases of croup occur in children 6 months to 3 years of age.
• It occurs twice as frequently in males as in females.
• Most cases occur during fall and winter.
• The infecting agents are predominantly viral; parainfluenzae type 1, 2, and 3 cause the majority of cases.
• Influenza and mycoplasma infection may be implicated rarely as causes of croup in children older than 5 years.
• Endemics are associated closely with the incidence of parainfluenzae viral infections during the fall and winter months.
• Adenovirus, respiratory syncytial virus, influenza, and measles virus are less common.
Pathogenesis
• Inflammation is not confined to the upper airway.
• Inflammation of small airways produces increased secretions.
• Subsequent atelectasis and the plugging of airways by mucus causes ventilation perfusion inequality and results in hypoxia.
• Carbon dioxide accumulates primarily from obstruction and the increased work of breathing, fever, and distress.
• “Air hunger” reflects the increased respiratory drive associated with hypoxia and hypercarbia.
• The prominent cough associated with croup probably is caused by a pharyngeal irritation and accumulated secretions in the upper and lower airways.
• Gas exchange abnormalities lead to anxiety, lethargy, and obtundation.
• The presence of these latter symptoms signals the need for intervention.
• This negative pleural pressure alters the balance of hydrostatic and oncotic forces within the pulmonary vasculature, predisposing the infant to pulmonary edema.
• Edema and secretions cause further atelectasis and airway closure.
• These contribute to further hypoxia, higher respiratory drive, and increased air hunger.
Clinical features• The stereotypical presentation of croup is a child 6
months to 3 years of age who has a several-day history of a progressive upper respiratory infection.
• Usually, a cough begins, classically described as “barking” or “seal-like,” on the second or third day of illness.
• This is associated with fluctuating inspiratory stridor unaffected by posture.
• Breathing is frequently noisy, and secretions may be copious or meager.
• Fever is common, but usually less low grade.
Signs • Is the color normal, dusky or cyanosis?
• Is the air entry normal or decreased?
• Is the stridor mild or severe?
• If restractions are present, are they minimal or maximal?
• Is the child agitated, restless or obtunded?
A child who demonstrates severity in two or more of these signs merits consideration for further intervention or observation in the hospital.
Laboratory investigations
• Laboratory investigations are not helpful in the early assessment of the child suspected of having croup and have no place in the management of the acutely ill child.
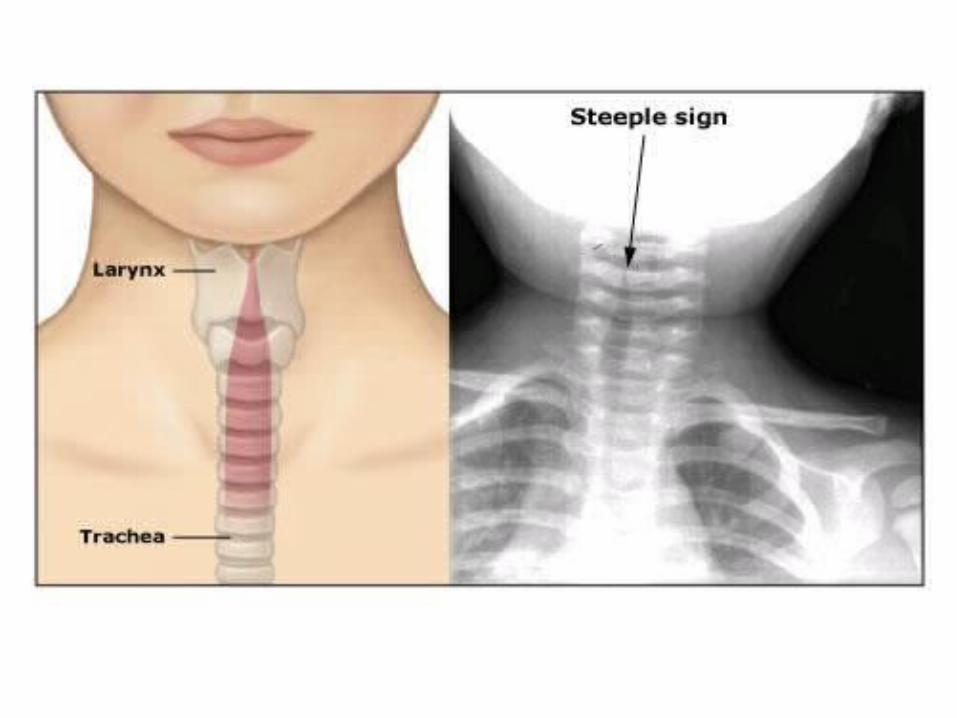
• Antero-posterior radiograph views of the neck confirm the diagnosis of croup by the presence of the “steeple sign” in the upper airway.
• Viral cultures are not valuable in the routine management of croup; nor are serologic tests.
Management • The vast majority of patients who have croup do not
require hospitalization.
• Of those admitted, fewer than 10% will require monitoring in the intensive care unit; only a fraction of these will require intubation.
• If symptoms progress, the child must be intubated or transferred prior to the onset of hypoxia and hypercarbia.
• There is no substitute for ongoing serial bedside assessment.
• Pulse oximetry, though helpful, cannot substitute for nursing observations of respiratory distress.
• In the case of upper airway obstruction, oxygen saturation measured by pulse oximetry can exceed 90% despite the presence of hypercapnea severe enough to produce agitation or obtundation.
• A decision to admit the patient to a continuous observation or intensive care unit should be based on the severity of symptoms.
• Contact isolation is recommended.
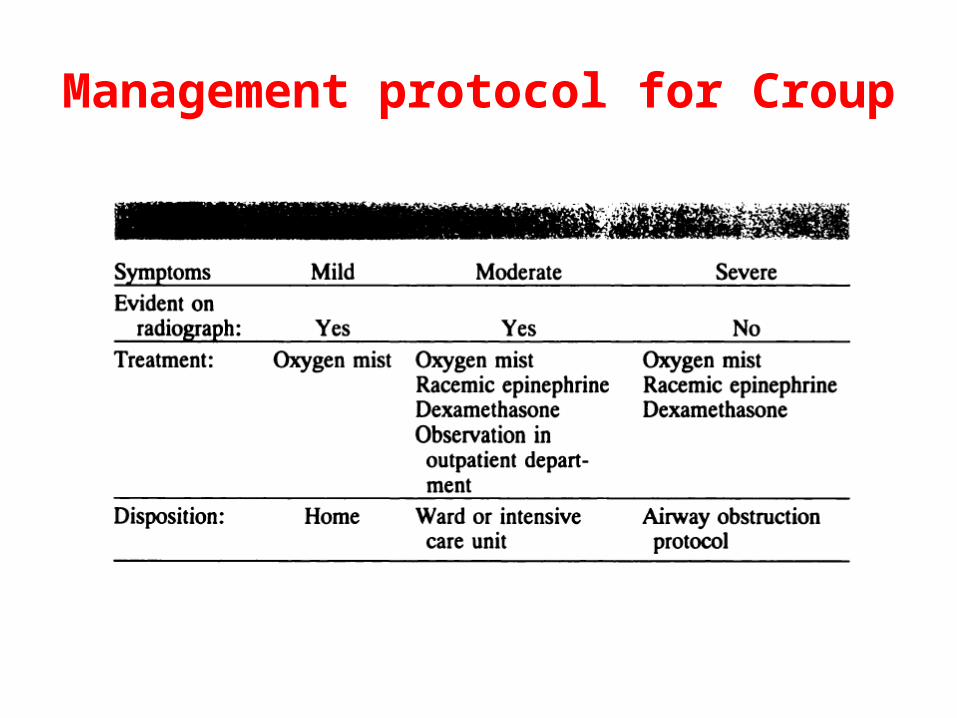
Management protocol for Croup
• The administration of cool mist has been a mainstay of treatment for decades. Several hazards to this generally beneficial therapy should be considered, however. Small children can be excessively cooled. The traditional “mist tent” may obscure the child from view, preventing the discovery of cyanosis and obtundation.
• Rarely, bronchospasm can be triggered by cold air, in which case its use must be discontinued.
• Racemic epinephrine has a long history of successful use, although dose-effect studies are not available.
• Commonly, 0.5 mL of a 2.25% solution is diluted in 6 to 9 times that amount of normal saline and delivered by hand-held nebulizer.
• Pressure delivery systems are cumbersome, frightening to the child, and of unproven benefit.
• Steroid treatment produced salutary benefits at 12 and 24 hours after a single systemic dose at admission.
• The incidence of intubation fell from 1.27% to 0.17% in the patients treated with steroids.
• Patients who received therapy with racemic epinephrine and steroid had a tendency to develop modest respiratory alkalosis.
• Doses of dexamethasone (0.3 to 0.6 mg/kg) now are given systemically at admission.

• Intubation will be required in fewer than 1% of all patients needing hospitalization.
• Guides to intubation are necessarily subjective. The primary principle is to avoid respiratory arrest and hypoxia.
• Admission to an intensive care unit should be anticipatory.
• The child who requires racemic epinephrine more frequently than every hour is in danger of respiratory failure and merits continuous nursing observation and monitoring of heart and respiratory rate and oxygen saturation by pulse oximetry.

Prognosis
• The overall prognosis of crop is good.
• Development of bronchial reactivity is common following the infection.
EPIGLOTTITIS
• Epiglottitis or supraglottitis is a lifethreatening condition that is caused by bacterial infection of the epiglottis, aryepiglottis, and arytenoids.
• It is differentiated from viral croup and foreign body aspiration by the acutely ill appearance of its victims and its fulminant onset.
• All facilities caring for children should have a detailed protocol for the management of epiglottitis.
Epidemiology
• Acute disease generally occurs in children between the ages of 2 and 6 years.
• More than 75% of cases are caused by H. influenzae type b. Rarely, other bacterial causes include beta-hemolytic streptococci, staphylococci, and pneumococci.
• There is no seasonal incidence, and no gender preference has been described.
Pathogenesis
• The supraglottic structures, swollen with inflammation, can obstruct the passage of air. The subglottic airway is not affected.
• Pneumonitis occurs in less than 20% of cases.
• Although the majority of patients are bacteremic (as many as 90% having positive blood cultures), distant infections are rare.
• Circulatory collapse is rare but, when present, usually is caused by a combination of hypoxia and dehydration.
• Pulmonary edema has been described in 25% of cases. Notably, this occurs both with the acute obstruction and after its relief by intubation.
• Large intrathoracic pressure fluctuations, damage to the alveolarcapillary membrane, enhanced yenous return to the right heart, and cievated systemic resistance secondary to catecholamine release are proposed mechanisms
Clinical presentation
• Epiglottitis in the child older than 2 years is distinguished easily by its severe, abrupt presentation.
• Children are usually ill less than 12 hours and have fever.
• In older child will complain of sore throat; difficulty in swallowing or refusal of liquids is common.
• Three findings are associated with epiglottitis: – stridor– the absence of spontaneous cough – the presence of drooling and agitation.
Signs • Acutely ill appearance• Febrile • Muffled speech• Cough may or may not be present• Refusal to lie down, preferral to sit, with arms extended
behind in a “tripod” position• Open mouth• Frequesnt drooling,• Jaw is thrust forward• Inspiratory stridor is prominent
• The use of accessory muscles of breathing, when present, is associated with a high degree of airway obstruction
• The presence of cyanosis, obtundation, or extreme agitation signal the presence of severe compromise.
Laboratory investigation • Laboratory evaluation has no place in the management
of supraglottitis.
• Blood gas measurements, cultures, radiographs, and blood cell counts are not required to establish the diagnosis in the critically ill, and agitating the child may precipitate complete airway obstruction.
• Lateral neck radiographs should not be required to establish the need to notify appropriate team members.
• In less severe cases of obstruction, when time is not an issue, the lateral neck radiograph is confirmatory.

• The classic radiographic sign is the “thumbprint-like” swollen epiglottis,
• seen just at the level of the hyoid bone. • Often, “ballooning” of the hypopharynx is seen on
inspiration.
• Cultures of blood and epiglottis are obtained after the airway is stabilized in the operating room.
• These may prove helpful later by identifying resistant strains or unusual pathogens.
• Blood cultures are reported positive in 50% to 90% of cases, but epiglottic swabs are positive in fewer than 33% of cases.

• The definitive diagnosis is made by direct laryngoscopy in the operating room.
• Extreme agitation, obtundation, pronounced stridor with use of accessory muscles of breathing, and a compatible history are indications for intubation.
Management
• Establishing an airway supersedes the need to establish a diagnosis in the most severe cases.
• The most widely accepted approach is naso-tracheal intubation in the operating room.
• Once intubated, the child should be placed in an intensive care unit and mildly sedated with midazolam alone or in conjunction with morphine.
• Mechanical ventilation is not routinely indicated.
• Intubation should be maintained for a minimum of 24 hours.
• Most patients will be extubated within 36 hours and the vast majority within 72 hours.
• The patient is extubated after the presence of a leak around the endotracheal tube is apparent.
• Direct laryngoscopy or indirect fiberoptic laryngoscopy is employed to confirm resolution of swelling in the supraglottic region.
• The fiberoptic examination has the advantage of requiring less sedation and being less uncomfortable for the patient.
• Antibiotics are administered for 5 to 7 days.
• Once an airway is established, we administer parenteral ceftriaxone.
• It should be appreciated that 30% of Haemophiius species are resistant to ampicillin.
• The use of chloramphenicol mandates the monitoring of serum levels.
• Parenteral therapy is discontinued after extubation and therapy is switched to oral medication.
• If there are household contacts younger than 4 years and H. influenzae is the causative agent, a 4- day course of rifampin should be administered to family members or daycare providers and to the patient upon completion of the initial antibiotic course.
• Complete recovery is the rule; recurrences are rare.

LARYNGITIS
• It causes hoarse voice or temporary complete loss of the voice because of irritation to the vocal cords.
• It is one of the causes of dysphonia.
• Laryngitis is categorised as:– Acute: lasts less than three weeks. – Chronic: may last over three weeks.
Laryngitis can be infectious or non-infectious
Infectious • Viral
rhinovirus, influenza, parainfluenza, adenovirus, coronavirus, RSV
• Bacterialgroup A streptococcus, S. pneumoniae, C. diphtheriae, M. catarrhalis, H. influenzae, B. pertussis, B. anthracis, M. TB
• Fungal histoplasma, blastomyces, candida, cryptococcus, coccidioides
Non-infectious• GERD• Allergies• Over use of vocal cords• Prolonged use of
inhaled corticosteroids• Thermal or chemical
burns• Laryngeal trauma
(iatrogenic / intubation)
Symptoms • Dysphonia (hoarseness) or aphonia (inability to speak)
• Dry, sore, burning throat
• Coughing
• Dysphagia (difficulty in swallowing)
• Cold or flu-like symptoms (which, like a cough, may also be the causal factor for laryngitis)
• Lymphadenopathy
• Fever
• Hemoptysis (coughing out blood)
• Dyspnea (difficulty in breathing), predominantly in children
• Increased production of secretion

Signs
• Erythema and edema of the epiglottis, aryepiglottic folds, arytenoids and centricular folds occurs in the early stages.
• In late stages, vocal cords and sub-glottic structures are also involved.
• Increased secretions
• Submucous haemorrhage (vocal abuse)
• Acute membranous laryngitis (no-specific pyogenic organisms, to be differentiated from diphtheria)
Management
• General measures:
• H-2 inhibitor (ranitidine) or Proton pump inhibitor (omeprazole)
• Steroids (thermal or chemical burns)
• Fluid resuscitation (viral laryngitis)
• Antibiotic /antifungal
• Speech therapy (persistent nodules)
Prognosis
• Most cases of laryngitis are viral and resolve without treatment with sufficient voice rest.
• Laryngitis, hoarseness, or breathiness that lasts for more than two weeks may signal a voice disorder and should be followed up with a voice pathologist.

TRACHEITIS
• Bacterial tracheitis is rare, but has the potential for serious sequelae and a difficult course.
• Case reports are notable for the frequent occurrence of cardiac arrest.
• The illness produces symptoms similar to those of croup, but is characterized by prominent, copious tracheal secretions.
• These children appear gravely ill and have symptoms compatible with septicemia.
Epidemiology
• Affected children range in age from several months to adolescence.
• A viral-like prodrome is common; bacterial infection may be secondary.
• The most common pathogens reported are staphylococci, H influenzae, streptococci, and Neisseria species.
• There is no seasonal variance.
Pathogenesis
• The trachea, larynx, and bronchi can become obstructed from inflammation or with purulent debris.
• The formation of adherent pseudomembranes over inflamed friable mucosa commonly 0is noted on bronchoscopy.
Clinical aspects
• The majority of patients have a mild prodrome of upper respiratory symptoms for 2 to 3 days and then worsen precipitously during the next 8 to 10 hours.
• The course is often described as being between that of croup and epiglottitis.
• The children appear systemically ill.
• Paroxysms of coughing may produce tenacious sputum.
• Older children may complain of burning substernal pain.
• The voice may be hoarse, but swallowing is unaffected.
• Fever is high, and stridor is prominent.
• Those affected may be tachypneic.
• Breathing is noisy and rhonchi are coarse. Retractions are common.
• Toxic shock syndrome has been reported in association with staphylococcal tracheitis.
• Laboratory tests are not indicated as part of the acute management of bacterial tracheitis.
• The white blood count will be high, and blood cultures are rarely positive.
• Gram stains of tracheal secretions are invaluable in determining antimicrobial choice.
• Cultures should be obtained when bronchoscopy is performed.
• Chest radiographs may demonstrate small dense material resembling foreign bodies in the trachea.
• Pseudomembranes may produce an irregular “scalloping” of the tracheal borders; the trachea may appear narrow.

Diagnosis
• Diagnosis is confirmed at bronchoscopy by the observation of pseudomembranes and purulent secretions.
• In less severe cases, the history, radiography, purulent secretions, and culture results may support a clinical diagnosis.

Management • Although racemic epinephrine and steroids have no
proven effect in cases of bacterial tracheitis, they should be employed while the diagnosis is in doubt.
• A decision to intubate must be made clinically.
• These patients must be managed in consultation with otolaryngologists.
• Long hospitalization is required, often in intensive care units. Significant acute complications, such as sepsis and cardiac arrest from endotracheal tube obstruction, are common.
• Late sequelae, such as granulation tissue and tracheal stricture, can emerge.
• Vancomycin and ceftriaxone, chosen empirically, will cover staphylococcal, streptococcal, and Haemophilus species.
• Antibiotics are continued for 10 to 14 days.
• A tracheostomy may be required if stricture or granulation tissue are discovered on serial fibreoptic examination of the trachea.
• In general, recovery is uncomplicated.