acute hemichorea in a 14-year-old boy
TRANSCRIPT

Acute H e m i c h o r e a in a 14 -Year -Old Boy
Walter C. Allan
The differential diagnosis of chorea or hemichorea in an adolescent boy is discussed. Sydenham's chorea, still the most common cause of chorea in childhood, is only one of many important diseases in the differential diagnosis in this clinical situation. Copyright �9 1996 by W.B. Saunders Company
P, A 14-YEAR-OLD white male, pre- sented with a 2-week history of difficulty
using his right hand, slurred speech, and prob- lems with his right leg. He had begun to notice difficulties drawing in art class. Subsequently his parents noted he had difficulty speaking and his gait looked odd to them. He had a history of a sore throat 3 weeks prior and had seen his pediatrician, but no studies were done. Past medical history was unremarkable. Review of systems was negative for change in mood or behavior and he felt well. The parents thought he was sleeping more than previously. The family history showed his mother had discoid lupus erythematosus.
EXAMINATION
His general exam was normal. His neurologi- cal examination was remarkable for right hemi- chorea, more prominent in the arm and face, a "sing-song" voice and bilateral hyper-reflexia. His plantar responses were flexor.
Impression
The impression was probable Sydenham's Chorea.
Laboratory and Course
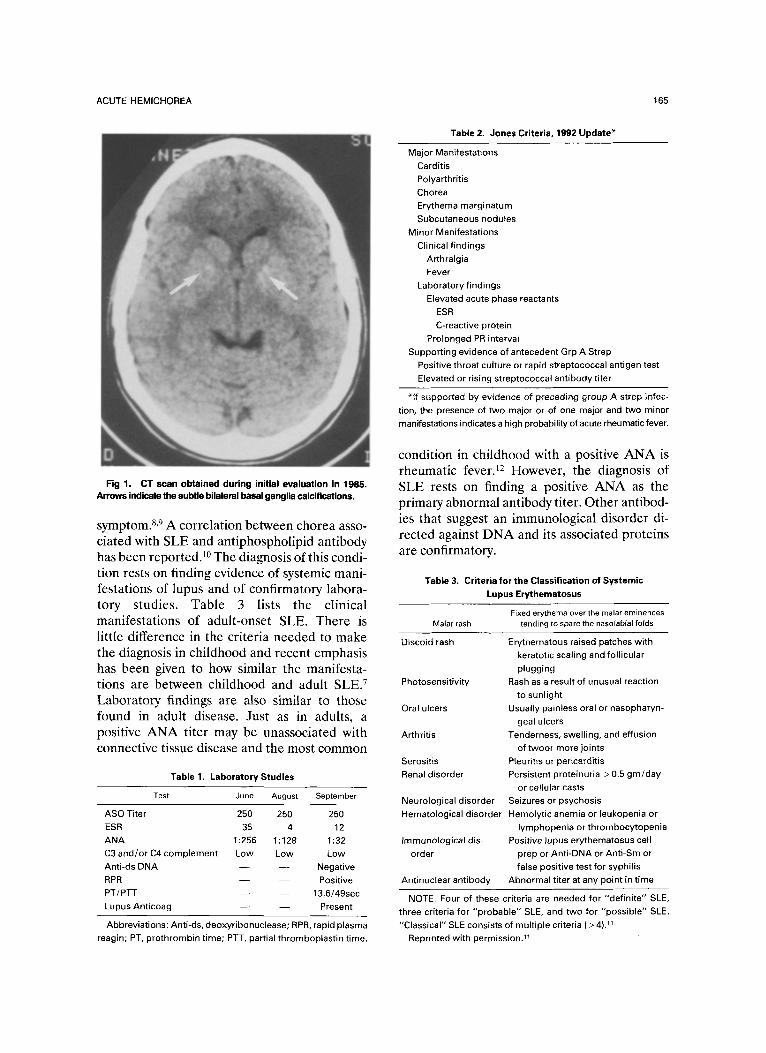
June 1985. Antistreptolysin-O titer: 250; erythrocyte sedimentation rate (ESR): 37; im- munoprofile: low C3; antinuclear antibody (ANA): 1:256 diffuse; electrocardiogram: nor- mal; computed tomography (CT) scan: bilateral basal ganglia calcifications (Fig 1). There was no initial treatment except a course of penicillin because his chorea was mild.
From the University of Vermont College of Medicine, Burling- ton, VT, and Maine Medical Center, Portland, ME.
Address reprint requests to Walter C. Allan, MD, 180 Park Ave, Portland, ME 04102.
Copyright �9 1996 by W.B. Saunders Company 1071-9091/96/0303-000255.00/0
August-September 1985. Fatiguability, tow mood, and increased hemichorea developed. A course of Haldol (McNeil Pharmaceutical, Rari- tan, N J) was given without improvement. Labo- ratory studies were repeated and he was hospi- talized for further evaluation when he developed chorea in the left arm. Laboratory findings are summarized in Table 1. A lumbar puncture was also performed and showed no cells, cerebrospi- nal fluid (CSF) protein 24, CSF glucose 58, and a normal CSF immunoprofile without oligoclo- nal bands or evidence of CSF production of immunoglobulin.
Differential Diagnosis
Sydenham's chorea. This seemed the most likely diagnosis at presentation. This condition was first described by Thomas Sydenham in 1686. Chorea is one of the major criteria in the Jones Classification (see Table 2) of rheumatic fever and presumes a prior (although often remote) infection with group A streptococcus. Chorea has been associated with up to 31% of recent outbreaks of this diseaseY Evidence of carditis is the usual associated rheumatic fever criterion, but subcutaneous nodules, erythema marginatum or the minor criteria of elevated ESR may also be seen. The usual time course for chorea is brief (weeks) but can at times be insidious in onset and not resolve. Besides looking for change in streptococcal antigens (anti-streptolysin-O, antihyaluronidase, anti- deoxyribonuclease B), recent information sug- gests testing for the cell surface antigen-B-cell alloantigen D8/17-may help differentiate Syden- ham's chorea from systemic lupus erythemato- SUS ( S E E ) . 6
Systemic lupus erythematosus. In childhood- onset SLE, the presentation is similar to adult disease with the exception that some features are seen more frequently. Chorea is one of these unusual manifestations along with nephri- tis, hepatosplenomegaly, and avascular necrosis of bone. 7 Chorea can be the sole presenting
164 Seminars in Pediatric Neurology, Vol 3, No 3 (September), 1996: pp 164-169
ACUTE HEMICHOREA 165
Fig 1. CT scan obtained during initial evaluation in 1985. Arrows indicate the subtle bilateral basal ganglia calcifications.
symptom. 8,9 A correlation between chorea asso- ciated with SLE and antiphospholipid antibody has been reported. 1~ The diagnosis of this condi- tion rests on finding evidence of systemic mani- festations of lupus and of confirmatory labora- tory studies. Table 3 lists the clinical manifestations of adult-onset SLE. There is little difference in the criteria needed to make the diagnosis in childhood and recent emphasis has been given to how similar the manifesta- tions are between childhood and adult SLE. 7 Laboratory findings are also similar to those found in adult disease. Just as in adults, a positive ANA titer may be unassociated with connective tissue disease and the most common
Table 1. Laboratory Studies
Test June August September
ASO Titer 250 250 250
ESR 35 4 12 ANA 1:256 1:128 1:32 C3 and/or C4 complement Low Low Low
Anti-ds DNA - - - - Negative
RPR - - - - Positive PT/PTT - - - - 13.6/49sec Lupus Anticoag - - - - Present
Abbreviations: Anti-ds, deoxyribonuclease; RPR, rapid plasma reagin; PT, prothrombin time; P'IT, partial thromboplastin time.
Table 2. Jones Criteria, 1992 Update*
Major Manifestations
Carditis Polyarthritis
Chorea
Erythema marginatum
Subcutaneous nodules Minor Manifestations
Clinical findings Arthralgia
Fever
Laboratory findings Elevated acute phase reactants
ESR
C-reactive protein
Prolonged PR interval Supporting evidence of antecedent Grp A Strep
Positive throat culture or rapid streptococcal antigen test
Elevated or rising streptococcal antibody titer
*I f supported by evidence of preceding group A strep infec- tion, the presence of two major or of one major and two minor
manifestations indicates a high probability of acute rheumatic fever.
condition in childhood with a positive ANA is rheumatic fever. 12 However, the diagnosis of SLE rests on finding a positive ANA as the primary abnormal antibody titer. Other antibod- ies that suggest an immunological disorder di- rected against DNA and its associated proteins are confirmatory.
Table 3. Criteria for the Classification of Systemic Lupus Erythematosus
Fixed erythema over the malar eminences Malar rash tending to spare the nasofabial folds
Discoid rash Erythematous raised patches with keratotic scaling and follicular
plugging Rash as a result of unusual reaction
to sunlight Usually painless oral or nasopharyn-
geal ulcers Tenderness, swelling, and effusion
of twoor more joints
Pleufitis or pericarditis Persistent proteinuria > 0.5 gin/day
or cellular casts
Neurological disorder Seizures or psychosis Hematological disorder Hemolytic anemia or leukopenia or
lymphopenia or thrombocytopenia Immunological dis- Positive lupus erythematosus cell
order prep or Anti-DNA or Anti-Sin or false positive test for syphilis
Antinuclear antibody Abnormal titer at any point in time
Photosensitivity
Oral ulcers
Arthritis
Serositis Renal disorder
NOTE. Four of these criteria are needed for "definite" SLE,
three criteria for "probable" SLE, and two for "possible" SLE. "Classical" SLE consists of multiple criteria ( > 4). 11
Reprinted with permission? 1
166
Antiphospholipid antibody syndrome. This syn- drome, first described in 1987,13 is defined by the presence of antiphospholipid antibody (APA) or lupus anticoagulant, usually in high titer, and some or all of the following: recurrent thromboses, recurrent fetal loss, thrombocytope- nia. Although this syndrome was defined in adults, there has been a recent report describ- ing APA and lupus anticoagulant in a group of children with idiopathic cerebral ischemia. 14 A confusing overlap exists between this condition and "primary antiphospholipid antibody syn- drome plus," which includes patients with other evidence of autoimmune dysregulation. This means the individual also has low complement levels and/or close family members with a definable connective tissue disease eg, lupus or rheumatoid arthritis. 15 A few of these patients may go on to have evidence of SLE. In retro- spect, this seems the most likely diagnosis in KP.
Other causes of chorea. The clinical course and associated findings did not suggest other conditions but for completeness, Table 4 lists the manifold causes of acquired chorea.
What does basal ganglia calcification mean? No cases of basal ganglia calcification (BGC) associated with APA or lupus were uncovered in a literature search, at the time. Subsequently, this has been described. 17 The literature is rife with the debate as to whether or not this finding on CT scan is simply "physiological" or of pathological significance especially in persons over 40 years of age. In a recent prospective study in adults in whom the CT scan was ordered for reasons other than signs or symp- toms referable to the basal ganglia, basal gan- glia calcifications were found in 30 of 1,478 or 2%. 18 Table 5 lists recognized pathological causes of BGC. Certainly in persons under 40 years of age a search for a definable cause is necessary. In KP the associated chorea would suggest a causal link between this sign and the BGC.
Working Diagnosis Without systemic signs of SLE but with a
positive APA, a tentative diagnosis of lupus- associated chorea was then made. The APA syndrome had yet to be described in 1985.
Subsequent Course KP was evaluated by rheumatologists locally
and at Boston Children's Hospital, Boston, MA.
WALTER C. ALLAN
Table 4. Etiologies of Chorea in Childhood
Infectious Disease Sydenham's chorea Viral encephalitis infectious mononucleosis Lyme disease Postvacciniel or postinfectious encephalomyelitis AIDS
Drug Associated Neuroleptics (chlorpromazine, thioridazine, pimozide, halo-
peridol, metochlopramide, prochlorperazine) Anticonvulsants (phenytoin, carbamazepine, phenobar-
bital, ethosuximide) Antiparkinson agents Noradrenergic stimulants (theophylline, aminophylline,
caffeine) Steroids (estrogen, anabolic steroids) Isoniazid Reserpine
Immunological Systemic Lupus Erythematosus Bechet's disease
Heredodegenerative Disorders Wilson's disease Huntington's disease Ataxia-telangiectasia Hallervorden-Spatz disease Pelizeus-Merzbacher disease Hereditary dentatorubral-pallidoluysian atrophy Benign hereditary chorea Paroxysmal kinesigenic chorea
Global Insults Cerebral palsy Post-op cardiac bypass chorea Cerebral anoxia
Metabolic Disorders Hyperthyroidism Hypo-Hypernatremia Hyperparathyroidism Hypoglycemia Hepatic encephalopathy Renal encephalopathy Malnutrition
Toxins Thallium Maganese
Structural Lesions Tumor Trauma Central nervous system hemorrhage
Modified and reprinted with permission. TM
It was thought that steroid treatment should be undertaken given the likelihood of SLE. His chorea resolved spontaneously without steroid treatment in late 1985. He was started on low-dose aspirin at that time and follow-up is summarized below. �9 January 1986: On routine follow-up he was
without chorea but has slight posturing of his
ACUTE HEMICHOREA
Table 5. Causes of Bilateral Basal Ganglia Calcifications
Primary and post-op hypoparathyroidism Pseudo hypoparathyroidism Hyperparathyroidism Carbon monoxide poisoning AIDS & other Central nervous system infections Down's syndrome Systemic lupus erythematosus Mitochondrial encephalomyopathies Chronic lead exposure Radiation therapy Familial idiopathic cerebral calcification
Reprinted with permission. TM
right hand. Lab: ESR, 5; normal complete blood count; ANA, 1:64, speckled; low C4 complement. RX: aspirin (ASA).
�9 October 1986: Right hemichorea returned. Lab: ESR, 6; partial thromboplastin time, 40; low C3 and C4 complement; anticardio- lipin antibody (aCL) -immunoglobulin G (IgG)-associated-strongly positive, immuno- globulin M-associated-borderline positive, immunoglobulin A-associated-absent. RX: Haldol; ASA.
�9 December 1986: The patient complained of pain in knees and improved but persistent hemichorea. Magnetic resonance imaging (MRI) of the brain was negative. RX: Hal- dol; ASA.
�9 January 1987: The patient experienced steadily worse chorea and complained of knee pain. Lab: urinary sediment 10 to 20 red blood cells with 25mg% protein but negative 24-hour urinalysis for elevated pro- tein; other labs unchanged. RX: Prednisone (Roxane Laboratories, Columbus, OH); ASA.
�9 February 1987," Patient's condition improved. RX: begin slow taper of Prednisone.
�9 December 1987: The patient had a normal exam after being off Prednisone for 1 month. RX: ASA.
�9 December 1988: Routine follow-up exam was normal. KP is now playing hockey for high school team. Lab: platelet count 128,000; strongly positive IgG-associated aCL. RX: ASA.
�9 December 1989: Right-sided hemichorea re- turned. Lab: thrombocytopenia and strongly positive IgG-associated aCL. RX: Predni- sone with rapid taper.
�9 February 1990: Chorea resolved after being off Prednisone for 2 weeks.
167
�9 July 1990: The patient complains of joint symptoms in hands and fingers. Exam is without redness or warmth but there is a raised erythematous patch in right flank. No chorea seen. The rheumatologist felt a defi- nite synovitis was present and lupus rash was present confirming SLE. RX: Naprosyn (Roche Laboratories, Nutley, NJ); Plaquenil (Sanofi Winthrop Pharmaceuticals, New York, NY); ASA.
�9 August 1990: The joints and skin returned to normal. RX: Plaquenil; ASA.
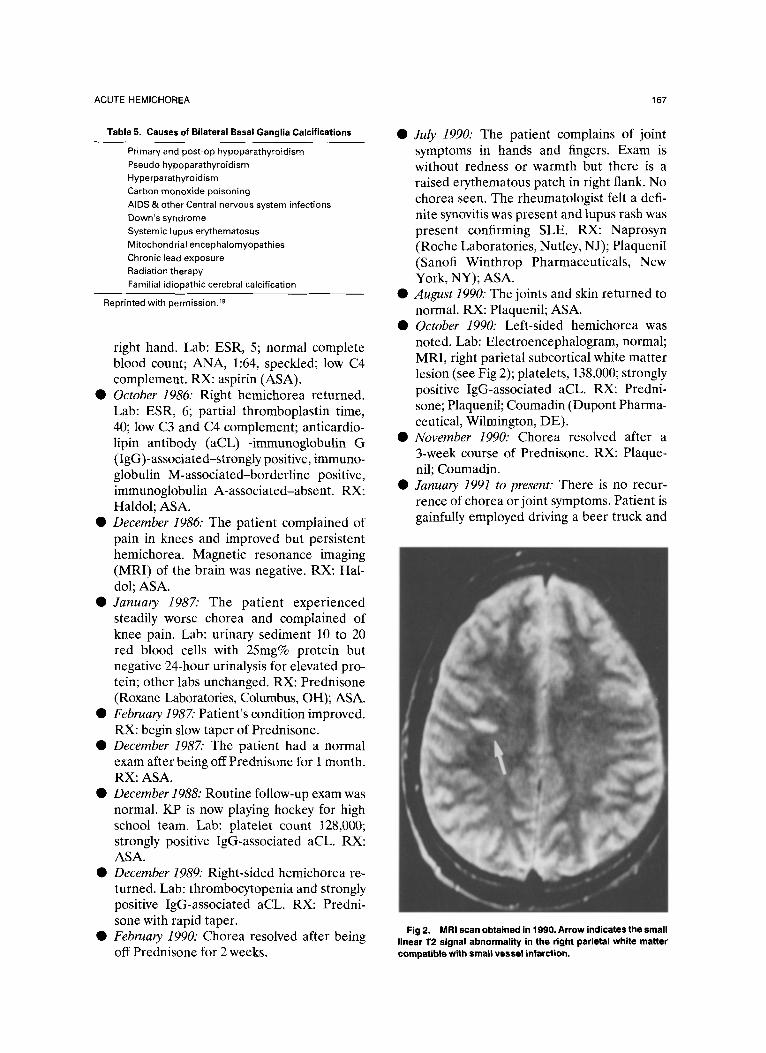
�9 October 1990: Left-sided hemichorea was noted. Lab: Electroencephalogram, normal; MRI, right parietal subcortical white matter lesion (see Fig 2); platelets, 138,000; strongly positive IgG-associated aCE RX: Predni- sone; Plaquenil; Coumadin (Dupont Pharma- ceutical, Wilmington, DE).
�9 November 1990: Chorea resolved after a 3-week course of Prednisone. RX: Plaque- nil; Coumadin.
�9 January 1991 to present." There is no recur- rence of chorea or joint symptoms. Patient is gainfully employed driving a beer truck and
Fig 2. MRI scan obtained in 1990. Arrow indicates the small linear I"2 signal abnormality in the right parietal white matter compatible with smali vessel infarction.

168 WALTER C. ALLAN
is recently married. Lab: persistent thrombo- cytopenia and strongly positive IgG-associ- ated aCL. RX: Plaquenil; Coumadin.
FINAL CONSIDERATIONS
The course of illness has contained elements of SLE in this young man with chorea whom we originally thought had pure chorea as a manifes- tation of rheumatic fever. He had an abnormal urinary sediment in 1987, a persistent thrombo- cytopenia since 1989, and a characteristic rash of SLE and arthritis by 1990. In 1990, when he had another attack of hemichorea, this time on the left side, his MRI scan showed a subcortical abnormality that suggested an infarct and neces- sitated long-term anticoagulation. Thus, in ret- rospect, rheumatic fever seems an untenable diagnosis and we did not consider that diagnosis for long. The APA syndrome plus may provide the link between these diseases. 15 That is, as in KP, the early manifestations of what will eventu- ally become SLE may closely resemble rheu- matic fever as well as other connective tissue diseases. In this regard, it is interesting to note the recent reports of valvular heart disease in patients with APAs mentioned by Asherson et al. 19 Thus, even another major Jones criteria may not mean the diagnosis is rheumatic fever. Screening for APAs in all patients presenting with chorea seems warranted. As in KP, the usual finding is a persistent elevation of one of the anticardiolipin antibodies. The IgG-associ- ated aCL is said to be most characteristic of patients with chorea.l~
COMMENT
Chorea is movement abnormality observed on physical examination while Sydenham's chorea is generally used to signify a diagnosis of a form of rheumatic fever. When cardiac or other major manifestations of rheumatic fever have occurred in the past, one is usually correct when recently acquired chorea is labeled Sydenham's or rheu- matic chorea. However, in current times, the sudden devel- opment of chorea presumed to be rheumatic is usually so-caUed "pure" chorea, that is, chorea believed to be poststreptococcal in origin but without past cardiac or
articular features of rheumatic fever. While it is definitely true that "pure" chorea can represent an isolated manifesta- tion of rheumatic fever provoked by a preceding streptococ- cal infection, the certainty that it is becomes more problem- atic in the absence of other rheumatic manifestations. Thus, what "looks like" Sydenham's chorea usually is just that, but occasionally it turns out to be chorea induced by one of many drugs, a neurological manifestation of thyrotoxicosis, basal ganglia dysfunction secondary to SLE, or rarely, a manifestation of a degenerative disorder or even brain tumor.
In the child described above, the male sex, the absence of recent personality changes, and the unilateral character of chorea would not have been considered inconsistent with Sydenhams's chorea but would be thought of as less than characteristic. Over the age of 10 years, Sydenham's chorea is considerably more common in girls than boys. It is usually associated with rather striking emotional lability and is usually bilateral although often asymmetrical. Muscle tone is diminished in most and deep tendon reflexes are usually decreased; hyperreflexia would be a signal suggesting that other causes could be looked for.
The identification of APAs in this child lead to a search for SLE, the illness with the strongest association with APA production. Production of these antibodies is also now known to be related to a variety of non-SLE associated neurological conditions including retinal ischemic attacks, cerebral thrombosis, migraine, and probably some cases with Sneddon's syndrome. Chorea in adolescents virtually identical to "pure" chorea of the Sydenham type has now been described on a number of occasions as the initial manifestation of SLE, sometimes long before other systemic features of the autoimmune disease. Conversely, chorea is not closely associated with the presence of APAs unrelated to SLE. With time, this child eventually developed synovial inflammation and rash, confirming the diagnosis of SLE.
This case exemplifies the point that acute onset of chorea can simulate Sydenham's, or rheumatic, chorea yet ulti- mately be found to be caused by another disease process. This, in fact, is an unusual event, thus raising the question of the cost-effectiveness of an extensive evaluation for a search for unlikely disease. The conservative physician will prob- ably settle for a work-up, which includes cardiac assessment, anti-streptococcal antibody studies, and ESR. The more aggressive approach would include the above in addition to the evaluation of thyroid function, ANA titer, APAs, studies of copper metabolism, and a neuroimaging study. Still others will be more selective and decide on studies on the basis of degree of probabilities developed from the history and findings on physical examination.
William E. Bell, MD
REFERENCES 1. American Heart Association Recommendat ions:
Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 Update. JAMA 268:2069-2073, 1992
2. Kaplan EL, Hill HR: Return of rheumatic fever: Consequences, implications and needs. J Pediatr 111:244- 246, 1987
3. Hosier DM, Craenen JM, Teske DW, et al: Resur- gence of acute rheumatic fever. Am J Dis Child 141:730- 733, 1987
4. Griffiths SP, Gersony WM: Acute rheumatic fever in New York City (1969 to 1988): A comparative study of two decades. J Pediatr 116:882-887, 1990

ACUTE HEMICHOREA 169
5. Westlake RM, Graham TP, Edwards KM: An out- break of rheumatic fever in Tennessee. Pediatr Infect Dis J 9:97-100, 1990
6. Feldman BM, Zabriskie JB, Silverman ED, et al: Diagnostic use of B-cell alloantigen D8/17 in rheumatic chorea. J Pediatr 123:84-86, 1993
7. White PH: Pediatric systemic lupus erythematosus and neonatal lupus. Rheum Dis Clin NA 20:119-127, 1994
8. Auisaka O, Obinata K, Sassi H, et al: Chorea as initial manifestation of SLE: a case report of a 10 year old girl. Clin Pediatr 23:298-300, 1984
9. Herd JK, Medhi M, Uzendoski DM, et al: Chorea associated with SLE: Report of two cases and review of the literature. Pediatrics 61:308-315, 1978
10. Asherson RA, Hughes GRV: Antiphospholipid anti- bodies and chorea. J Rheumatol 15:377-379, 1988
11. Tan EM, Cohen AS, Fries JF, et al: The 1982 revised criteria for the classification of systemic lupus erythemato- sus. Arthritis Rheum 25:1271-1277, 1982
12. Cabral DA, Petty RE, Fung M, et al: Persistent antinuclear antibody in children without identifiable inflam- matory rheumatic or autoimmune disease. Pediatrics 89:441- 444, 1992
13. Harris EN, Baguley E, Asherson RA, et al: Clinical and serological features of the antiphospholipid syndrome (APS). Br J Rheumatol 26:19, 1987 (abstr)
14. Angelini L, Ravelli A, Caporali R, et al: High prevalence of antiphospholipid antibodies in children with idiopathic cerebral ischemia. Pediatrics 94:500-503, 1994
15. Asherson RA: Antiphospholipid antibodies and syn- dromes, in Lahita RG (ed): Systemic Lupus Erythematosus, ed 2. New York, NY, Churchill Livingstone, 1992, pp 587-635
16. Klawans HL, Brandabur MM: Chorea in childhood. Pediatr Ann 22:41-50, 1993
17. Nordstrom DM, West SG, Andersen PA: Basal ganglia calcification in central nervous system lupus erythem- atosus. Arthritis Rheum 28:1412-1416, 1985
18. Fenelon G, Gray F, Paillard F, et al: Pallidal calcifica- tions. J Neurol Neurosurg Psychiatry 56:622-625, 1993
19. Asherson RA, Khamashta MA, Gil A, et al: Cerebro- vascular disease and antiphospholipid antibodies in sys- temic lupus erythematosus, lupus-like disease, and the primary antiphospholipid syndrome. Am J Med 86:391-399, 1989