acute aortic dissection am report 6/29/09 brandon m. williams, md
Post on 21-Dec-2015
213 views
TRANSCRIPT
Acute Aortic Dissection
AM Report 6/29/09
Brandon M. Williams, MD
Classification
• Two systems:
• DeBakey
• Daily (Stanford) = most used

DeBakey
• Type 1: origin in ascending aorta and propagates to at least arch
• Type 2: origin in ascending and confined within ascending
• Type 3: origin in descending and extends (distally or proximally)
Daily (Stanford)
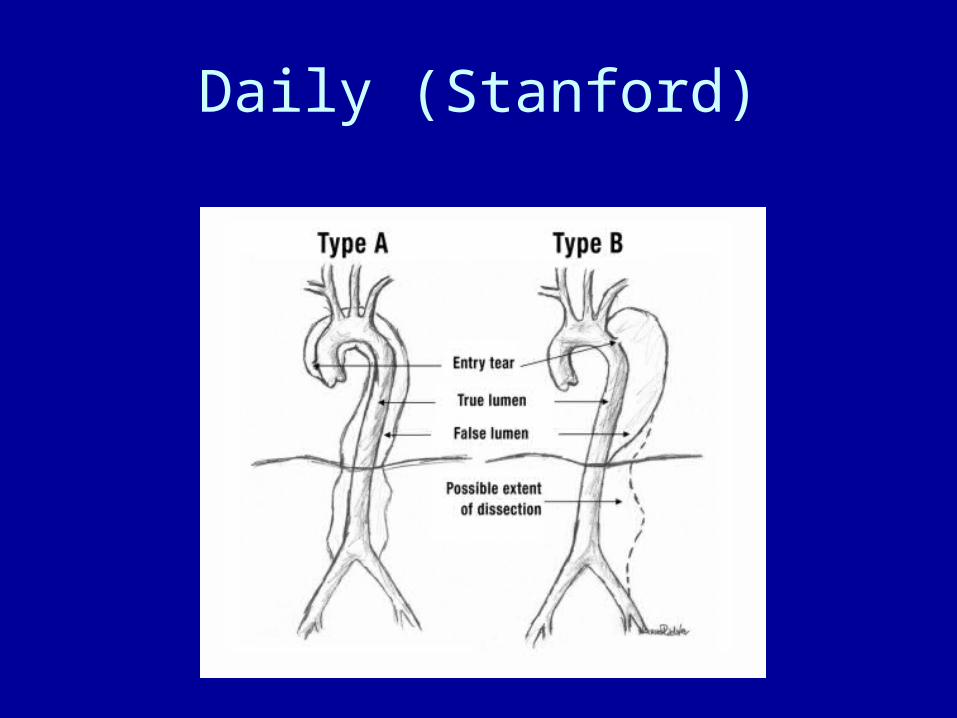
• Type A: involves ascending aorta
• Type B: all others
- Nomenclature doesn’t change secondary to site of origin
Daily (Stanford)
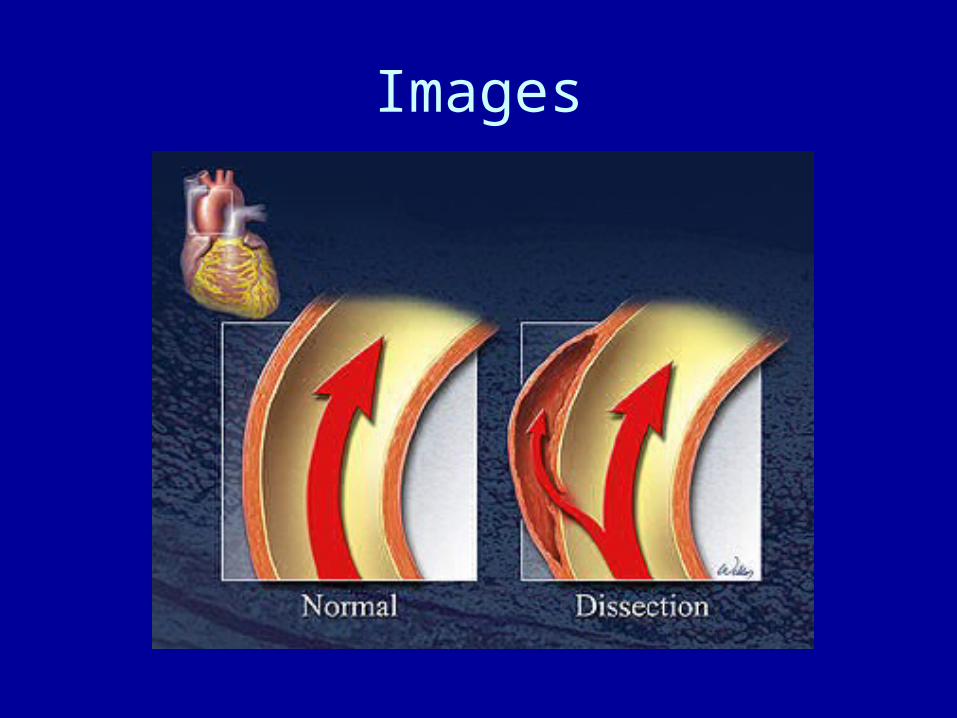
Pathophysiology
• Tear in aortic intima• Need degeneration of media or cystic
medial necrosis for nontraumatic dissections
• Blood crosses into media via tear and separates intima from media/adventitia creating a false lumen
• ? If rupture of intima or hemorrhage within media causing rupture of intima is initiating event
Incidence
• Acute aortic dissection
- 2.6-3.5/100,000 person years
Incidence
• Classic is 60 – 80 yo males (mean 63yo)
• Women 67
• Ascending 2x more likely than descending, with right lateral wall most common site
Risk Factors
• 13% with known aortic aneurysm (19% if < 40yo)
• Inflammatory disease vasculitis
-giant cell arteritis
-takayasu arteritis
-rheumatoid arthritis
-syphilitic aortitis
Risk Factors• HTN (71%)• Atherosclerosis (31%)• DM (5.1%)• Collagen disorders (Marfan, Ehlers-Danlos)• 19% of thoracic with family history • Bicuspid aortic valve (9% < 40yo)• Aortic coarctation (post intervention)• CABG• AVR• Cardiac catheterization• Trauma• High-intensity weight lifting and cocaine via transient HTN - cocaine 37% of AA inner city population
Signs and Symptoms
• Abrupt, tearing pain, back (if distal to L subclavian) or anterior (ascending)
• Associated: syncope, CVA, MI, HF• Syncope assoc with worse outcome (almost all type A)• Pulse deficit• Aortic insufficiency: murmur more at RSB than valve
assoc AI (LSB)• >20mmHg difference in SBP between UE• Vocal cord paralysis (compression of L laryngeal nerve)• Hypotension (hemorrhage, tamponade, HF)• Spinal cord ischemia• “STEMI:” 3/820 EKGs showing STEMI found to have
ascending aortic dissection
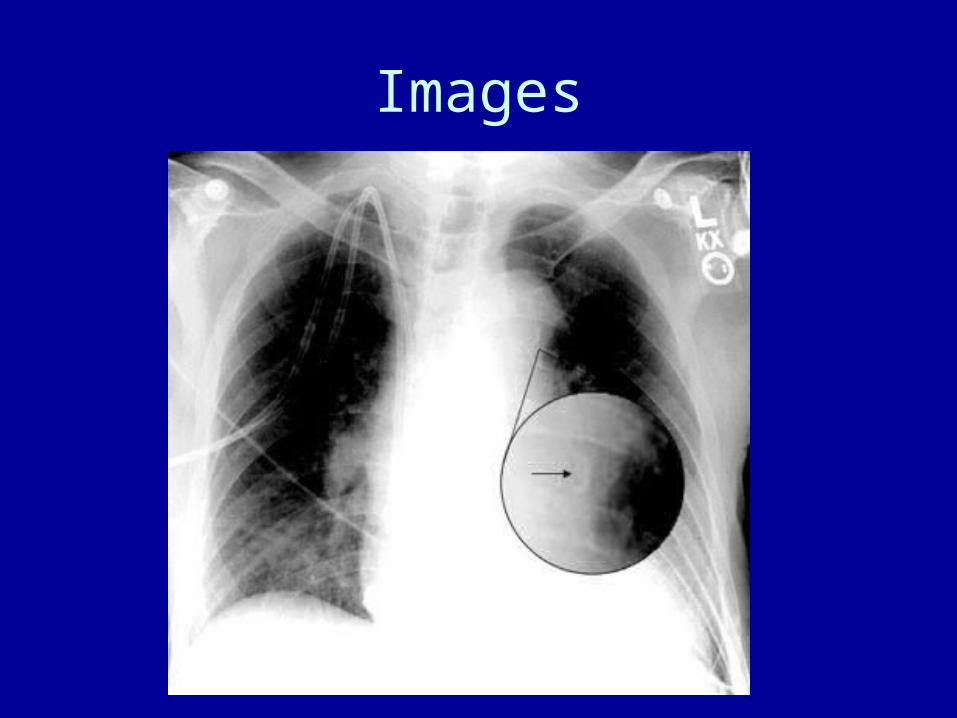
Images
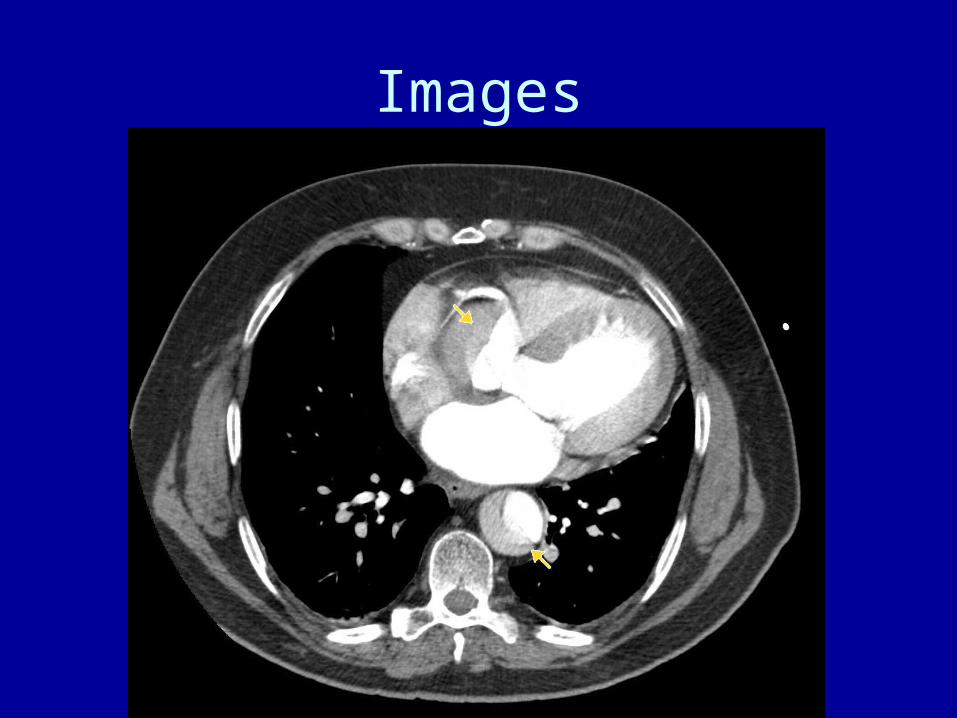
Images
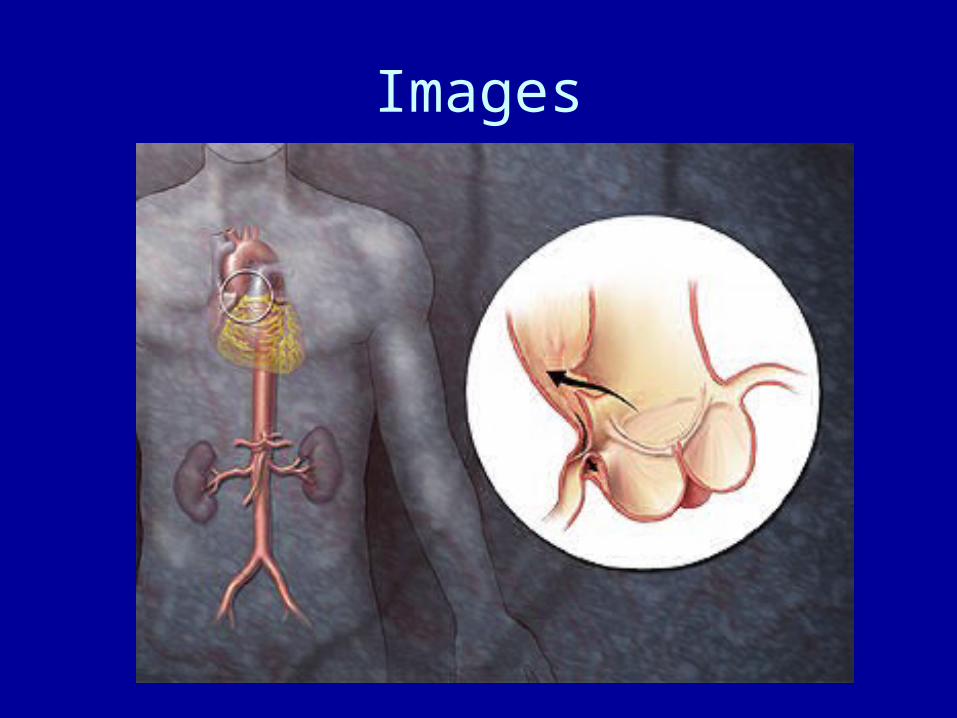
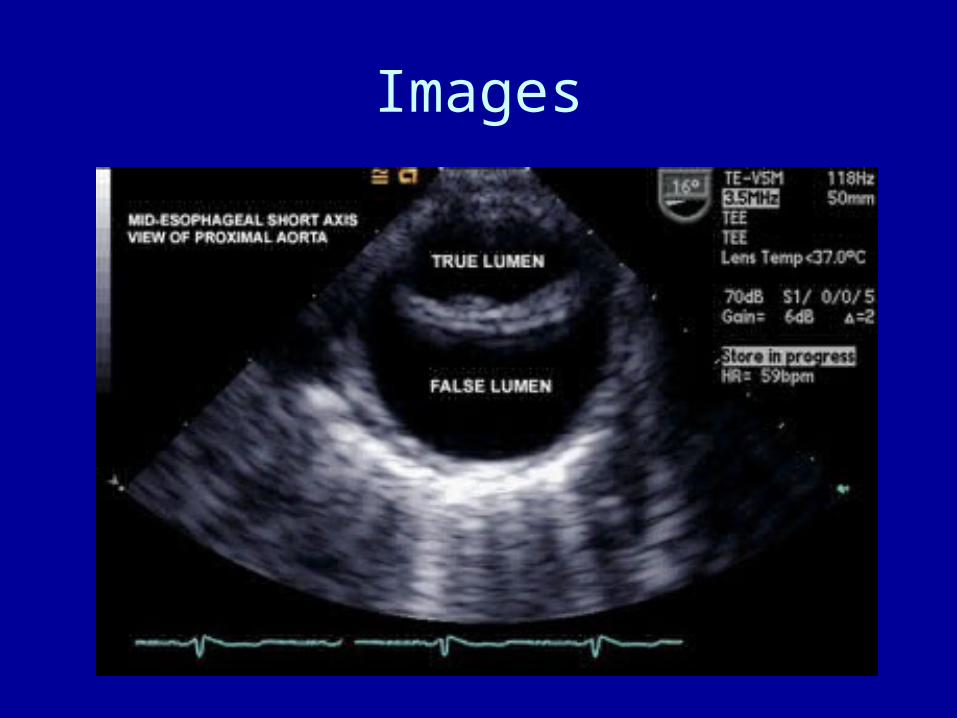
Images
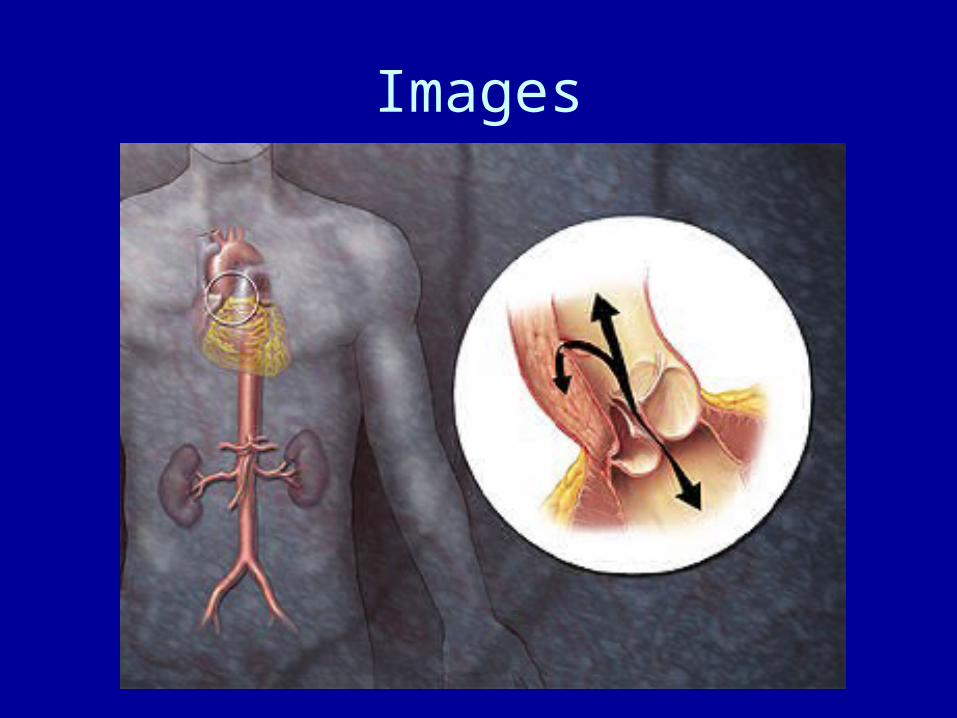
Images
Diagnosis
• Abrupt onset of pain, tearing/ripping
• Mediastinal/aortic widening on Chest X ray
• Variation in pulse
Imaging
• Chest Xray
• TTE
• TEE
• CTA chest
• MRI
• Coronary angiography
Images
Images
Images
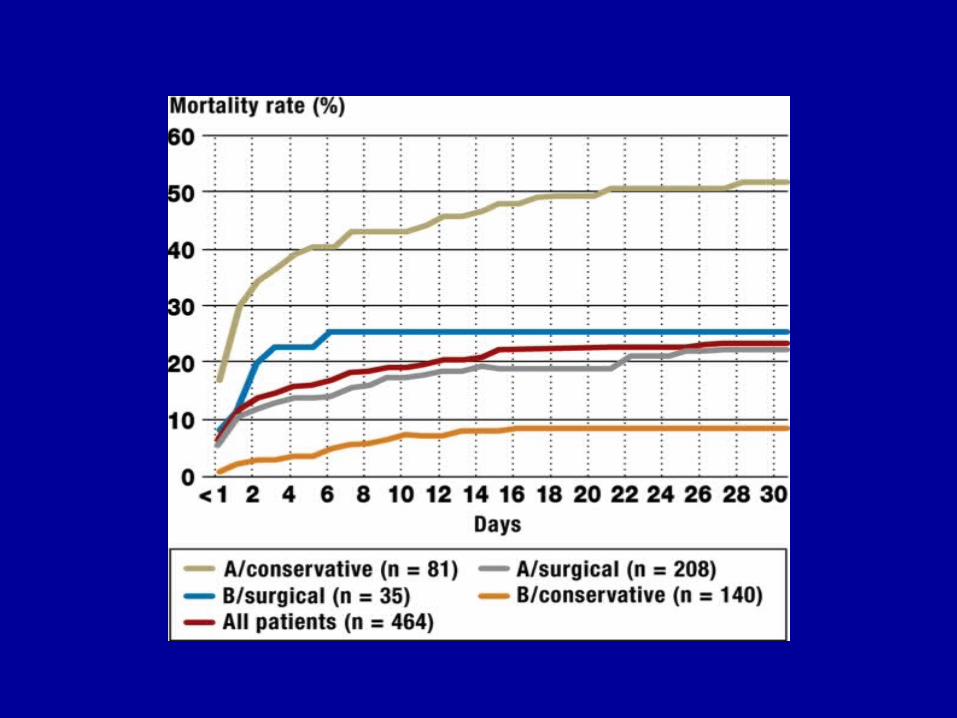
Treatment
• Involvement of ascending aorta = surgical emergency
• Descending aorta: medical management unless progression or hemorrhage into pleural or retroperitoneal space
-morphine -SBP 100-120 or lowest tolerated *beta blocker titrate to HR < 60 (labetalol, propranolol,
esmolol) *if beta blocker intolerant: verapamil, diltiazem *no nitroprusside until HR < 60 *no hydralazine *no inotropic agents, if hypotensive look for bleeding• A-line in radial artery with highest auscultatory pressure
References
• UpToDate• Management of Patients with Aortic Dissection. Weigang
et al. Dtsch Arztebl Int. 2008 Sep. 105 (38) 639-645• Conditions mimicking acute ST-segment elevation
myocardial infarction in patients referred for primary percutaneous coronary intervention. Gu et at. Neth Heart Journal. 2008 Oct: 16 (10) 325-31
• Google images