achieving excellence in kidney care - home » national ... · achieving excellence in kidney care:...
TRANSCRIPT

Achieving Excellence in Kidney CareDelivering the National Service Framework for Renal Services

DH INFORMATION READER BOX
Policy EstatesHR/Workforce CommissioningManagement IM&TPlanning FinanceClinical SocialCare/PartnershipWorking
Document purpose Forinformation
Gateway reference 12797
Title �Achieving�Excellence�in�Kidney�Care:�Delivering�the�National�Service�Framework�for�Renal�Services
Author NationalClinicalDirectorforKidneyCare
Publication date 14Dec2009
Target audience PCTCEs,NHSTrustCEs,SHACEs,CareTrustCEs,FoundationTrustCEs,MedicalDirectors,DirectorsofPH,DirectorsofNursing,LocalAuthorityCEs,PCTChairs,NHSTrustBoardChairs,DirectorsofHR,DirectorsofFinance,AlliedHealthProfessionals,GPs,CommunicationsLeads,EmergencyCareLeads
Circulation list
Description TheNationalServiceFrameworkforRenalServicessetoutthefirsteversetofnationalstandardsforthetreatmentofrenaldisease.ThisreporthighlightsprogressoverthefiveyearssincethepublicationoftheNationalServiceFramework
Cross reference TheNationalServiceFrameworkforRenalServices,PartOneandTwo.
Superseded documents N/A
Action required N/A
Timing N/A
Contact details StephanieParkerRenalPolicyTeam408WellingtonHouse133-155WaterlooRoadLondonSE18UG
For recipient use
©Crowncopyright2009
FirstpublishedDecember2009

Achieving Excellence in Kidney CareDelivering the National Service Framework for Renal Services


Contents
Foreword by the Secretary of State for Health 4
Introduction by the National Clinical Director for Kidney Care 6
Summary of National Service Framework standards, quality requirements and markers of good practice 8
1 A patient-centred service 10
2 Prevention, early detection and management of chronic kidney disease 15
3 Preparation, choice and dialysis access surgery 22
4 Dialysis 27
5 NHS Kidney Care – ‘Better Kidney Care for All’ 34
6 Transplantation 38
7 Acute kidney injury (acute renal failure) 43
8 End-of-life care 46
Annex: Organ donor form 51

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
4
TheNationalServiceFramework(NSF)forRenalServicesprovidedforthefirsttimeacompellingvisionforkidneyservicescentredontheneedsofeachpatient.
RealprogresstoimplementthevisionsetoutintheNSFhasbeenmadethroughtheeffortsofpatients,carersandpractitioners.TheNHSnowleadsontheinternationalstageinearlydetectionandpreventionofkidneydisease,withincreasingnumbersofpatientsbeingeffectivelymanagedinprimarycare.Dialysiscapacityhasexpanded
asmorefacilitiesandsatelliteunitshavecomeonstream,andthenumberofregisteredorgandonorsinEnglandnowexceeds13million.Ratesofhospital-acquiredinfectionamongkidneypatientshavebeendrivendownthroughincreasingadoptionofbestpracticeinvascularaccess.
Againstthisbackdrop,thenumberofpeoplewithkidneydiseasecontinuestoriseyearonyear.Thisisbecausekidneydiseasesharesmanyofthesameriskfactorsasothervasculardiseasessuchasdiabetes.ThismakesthecontinuedimplementationoftheNSFinconjunctionwithotherpreventativeinitiatives,suchastheNHSHealthCheckprogramme,oftheutmostimportance.
ThisreportrecordsandcelebratesprogressoverthefiveyearssincepublicationoftheNSF.TheNHShaschangedenormouslyoverthistime.Itisnowledbyfrontlinestaff,whichenableslocalservicestolistentotheirlocalpopulationandprovideservicesthataretailoredtotheircommunities.
Inthenextfiveyearsandbeyond,ourmissionmustbetotakeNHSservicesfromgoodtogreat,makingthemmorepreventativeandpeople-centred,keepingpeoplewellandoutofhospital,andempoweringthemtochoosewhattheyknowisbestforthemandwheretheywanttobetreated.
Variationindetectionratesforchronickidneydiseaseneedstobeaddressed,andmoreattentiongiventotherecognitionandmanagementofacutekidneyinjury.Theserviceneedstomovetowardsbeingmorepatient-centred,givingpeoplechoiceandcontroloverhowtheymanagetheircondition;inparticular,choiceforpatientswishingtoselfcareathomemustbeimproved,includingprovisionofhomehaemodialysisasrecommendedbytheNationalInstituteforHealthandClinicalExcellence(NICE).Thebigchallengenowistomakeinnovativechangesthroughservicereform–withtimelyinterventionandbydoingthingsrightfirsttime–toensurethatresourcesareusedtobesteffect,andthatpatientsgetthebestoutcomes.
Foreword by the Secretary of State for Health

ForewordbytheSecretaryofStateforHealth
5
Renalservices,togetherwiththeimprovementorganisationNHSKidneyCare,arewellplacedtoreapthebenefitsofthisapproach.Ilookforwardtoacelebrationofthenextfiveyears’achievementsinimprovingkidneycare.
Andy Burnham MP Secretary of State for Health

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
6
PublicationoftheNSFwasaseminalmoment,andhasledtoasocialmovementwithinthekidneycommunity,withthevisionoftransformingtheexperienceand,whenpossible,theoutcomesforeverypersonwithkidneydisease.
Therehasbeenrealprogressoverthelastfiveyears,andmanyexcitingdevelopmentsateverylevel,fromnationalcommissioningrightthroughtoputtingindividualpatientsatthecentreofshareddecision-making.Better
preparationandchoiceforthosewithadvancedkidneydisease,developmentsintransplantationandimprovementsinvascularaccessfordialysishavecontributedtokidneyunitsbeingsaferplacesthatdeliverimprovedoutcomesandqualityoflife.NHSKidneyCarehasplayedavitalroleinfacilitatingthedevelopmentoflocalkidneycarenetworksandhassupportedtheimplementationofeffectivecareplanningbydevelopingapersonalisedcareplanforallkidneypatients.
Yet,weknowthatthereisstillconsiderablevariationinaccesstocare,therearemissedopportunitiesforprevention,unnecessarydelaysintreatmentandoftenafailuretoprovidetheconditionsforshareddecision-making.
Weneedtoaccelerateimplementationofwhatweknowworks,suchasearlierandbetterbloodpressurecontrol,implementationoftheNICEguidanceonchronickidneydiseaseandanaemiamanagement,andtimelypreparationforreplacementtherapyorconservativecare.Weneedtobebold,toinnovateandchallengethenormsothatwecanachieveimprovements.Thisrequiresco-ordination,partnershipandleadershipbycommissionersandproviders,andbyclinical,socialcareprofessionalsandmanagers,inandbetweenprimaryandspecialistcare.
Changehappenslocally.Fundamentalserviceimprovementsareledbylocalteamsworkinginanempoweringenvironment.Theyneedtobegiventheresponsibilitytoachieve,andpermissiontotakerisks,aspartofalearningorganisation.Nationalpoliciesandguidelinessettheframework,butitisthroughthegrass-rootsunderstandingofqualityandproductivitythatdevelopmentofinnovativeapproaches,whichleadtolastingimprovements,happens.Atthecentreofthisarepatientsandthehigh-qualityrelationshipsbuiltbetweenthemandempathetic,motivatedandskilledpractitioners.
Introduction by the National Clinical Director for Kidney Care

IntroductionbytheNationalClinicalDirectorforKidneyCare
7
Kidneydiseaseiscommon,harmfulandtreatable.Animprovedunderstandingoftheimplicationsofkidneydiseasewillsupportthebehaviouralandlifestylechangesthatcandeliverthepreventativedividend.Achangeinemphasisfromdiseasemanagementtopromotinghealthisneeded,supportingourstaff,motivatingpeoplewithkidneydiseaseandencouraginga‘cando’mentalityinoursystem,informedbymoreresearchandbetterevidence.Weshouldstrivetointerveneearly;endeavourtomotivatepatientstokeepthemselveswell;andprovideevidence-based,accessibleinformationtosupportourpatients.Whenweengageserviceusersfullyinsettinggoalsandplanningtheirowncare,greatstepsforwardcanbemade.
Improvingcoding,measurement,analysisandreportingofpatientexperiences,clinicaleffectiveness,costs,safetyandoutcomeswillhelptoinformservicetransformation.
Thiswillnotbeeasy.Itwillrequirelocalandnationalleadership,newpartnerships,difficultchoicesandasystematicapproachinsupportingindividualstoachieveoptimalhealthateverystageofthekidneycarepathway.Theprize–movingourservicesfrombeinggoodinpartstobeinggreateverywhere–isworththateffort.Iwouldliketothankthekidneycommunityfortheirenthusiasm,passionanddedicationtoimprovingcareacrosstheentirekidneycarepathway.IlookforwardtoworkingalongsidethemtodelivertheNSFvision.
Dr Donal O’Donoghue National Clinical Director for Kidney Care

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
8
These standards and quality requirements apply to all people with, or at risk of, kidney failure. In some cases, for example children and youngpeople and some older people, they will also apply in varying degrees to families, guardians or carers.
Part one of the NSF:
STANDARD ONE: All children, young people and adults with chronic kidney disease are to have access to information that enables them withtheir carers to make informed decisions and encourages partnership in decision-making, with an agreed care plan that supports them in managingtheir condition to achieve the best possible quality of life.
Markers of good practice• Provision of high quality, culturally appropriate and comprehensive information and education programmes.
• Education programmes tailored to the needs of the individual.
• Individual care plans, regularly audited, evaluated and reviewed.
• Access to a multi-skilled renal team whose members have the appropriate training, experience and skills.
• For children and young people, meeting the standards of Getting the right start: National Service Framework for Children, Young People andMaternity Services.
STANDARD TWO: All children, young people and adults approaching established renal failure are to receive timely preparation for renal replacementtherapy so the complications and progression of their disease are minimised, and their choice of clinically appropriate treatment options is maximised.
Markers of good practice• Referral to a multi-skilled renal team, where possible at least one year before the anticipated start of dialysis treatment, for appropriate clinical
and psychological preparation. This principle should also be followed for people with a failing transplant.
• Accelerated process with intensive input from the renal team for those who present late to renal units or as acute uraemic emergencies.
• People with ERF given information about all forms of treatment so that an informed choice can be made.
• Patients put on the national transplant list within six months of their anticipated dialysis start date if clinically appropriate.
• Anaemia treated to maintain an adequate haemoglobin level.
• Management of cardiovascular risk factors and diabetes according to the National Service Frameworks for Coronary Heart Disease and for Diabetes.
STANDARD THREE: All children, young people and adults with established renal failure are to have timely and appropriate surgery forpermanent vascular or peritoneal dialysis access, which is monitored and maintained to achieve its maximum longevity.
Markers of good practice• Early referral for assessment and investigation for the best means of access, and timely surgery (current best practice being six months before
haemodialysis, four weeks before peritoneal dialysis) which enables patients to begin dialysis with their vascular or peritoneal dialysis accessestablished and functioning.
• Monitoring and early intervention to minimise complications of the access.
• Recording and regular auditing of the type of access in use at the start of dialysis, time from referral to surgery, and complication rates foreach procedure. Temporary access replaced by permanent access as early as possible.
• Proper training for patients, carers and members of the renal team in the care of the access.
• For children and young people: Dialysis access surgery to follow the principles set out in Getting the right start: the National ServiceFramework for Children, Young People and Maternity Services – Standard for Hospital Services.
STANDARD FOUR: Renal services are to ensure the delivery of high quality clinically appropriate forms of dialysis which are designed aroundindividual needs and preferences and are available to patients of all ages throughout their lives.
Markers of good practice• All dialysis methods available interchangeably for patients, including home haemodialysis and automated peritoneal dialysis.
• Patients receive an adequate and effective dialysis dose.
• Peritonitis rates to be less than one per 18 patient months for adults undergoing peritoneal dialysis, one per 14 patient months for children.
• Patients have their nutritional status monitored and appropriate nutritional support in place.
• Efficient patient transport services available.
• Specialist renal staff, equipment and care available throughout admission, whatever the setting, for patients with established renal failureadmitted to hospital.
STANDARD FIVE: All children, young people and adults likely to benefit from a kidney transplant are to receive a high quality service whichsupports them in managing their transplant and enables them to achieve the best possible quality of life.
Markers of good practice• Early provision of culturally appropriate information; discussion with and counselling of patients, relatives and carers about the risks and
benefits of transplantation.
• Application of a national matching scheme using criteria agreed through UK Transplant to optimise blood group and tissue matching forkidneys from deceased donors.
• Effective preventive therapy to control infections.
• Timely operating theatre availability to ensure optimal cold ischemia times.
• Appropriate immunosuppression and anti-rejection treatment in accordance with forthcoming NICE guidance and effective monitoring andtreatment to minimise the risks of adverse effects of immunosuppressive treatment.
• Clear explanation for patients of tests, procedures and results, and especially information and education about anti-rejection therapy.
• Specialist advice from the transplant team available for patients with a renal transplant admitted to hospital, whatever the setting.
• Organ procurement and transplantation to follow the principles set out in Saving Lives, Valuing Donors: A Transplant Framework for England.
Summary of National Service Framework standards, quality requirements and markers of good practice

SummaryofNationalServiceFrameworkstandards,qualityrequirementsandmarkersofgoodpractice
9
Part two of the NSF:
QUALITY REQUIREMENT ONE: People at increased risk of developing or having undiagnosed chronic kidney disease, especially people withdiabetes or hypertension, are identified, assessed and their condition managed to preserve their kidney function.
Markers of good practice• All people at increased risk of CKD are identified, and given appropriate advice, treatment and support (which is sensitive to the differing
needs of culturally diverse groups) to preserve their kidney function.
• People identified as having an increased risk of CKD have their kidney function assessed and appropriately monitored, using estimated GFR.
• Implementation of the NICE clinical guideline on the management of Type 1 diabetes.
• Implementation of the NICE clinical guidelines on the management of Type 2 diabetes: renal disease; blood glucose; blood pressure and bloodlipids.
• Implementation of the NICE clinical guideline on the management of hypertension in adults in primary care.
• For children and young people with potential urinary tract infection, accurate diagnosis and prompt antibiotic treatment, and investigationsufficient to identify structural renal defects and to prevent renal scarring.
• For children and young people with bladder dysfunction, planned investigation and follow-up, with access to urology services with paediatricexpertise.
QUALITY REQUIREMENT TWO: People with a diagnosis of chronic kidney disease receive timely, appropriate and effective investigation,treatment and follow-up to reduce the risk of progression and complications.
Markers of good practice• All people diagnosed with CKD have access to care which is sensitive to the differing needs of culturally diverse groups, to maximise the
benefits of treatment and minimise the effects of the disease; and have a care plan.
• Use of the best available evidence to inform the management of blood pressure, cardiovascular disease and cardiovascular risk, and urinarytract obstructions and infections in people with CKD.
• In people with diabetes and CKD, interventions to reduce microvascular complications, in accordance with the National Service Framework forDiabetes.
• Implementation of the forthcoming NICE guideline on the treatment of anaemia in CKD.
• Referral from primary care to the specialist renal service at an appropriate stage to optimise outcomes.
QUALITY REQUIREMENT THREE: People at risk of, or suffering from, acute renal failure are identified promptly, with hospital servicesdelivering high quality, clinically appropriate care in partnership with specialised renal teams.
Markers of good practice• Timely identification and referral to renal and critical care services for specialist, culturally appropriate advice and assessment.
• Appropriate pre-operative testing and interventions, in accordance with the NICE guideline on pre-operative testing.
• Involvement of local critical care networks in planning, commissioning and monitoring the delivery of critical care services to acutely ill renalpatients.
• Liaison with specialist renal services to facilitate optimal management of people with ARF in the most clinically appropriate setting.
• For children and young people: Treatment and care in accordance with Getting the right start: National Service Framework for Children,Young People and Maternity Services.
QUALITY REQUIREMENT FOUR: People with established renal failure receive timely evaluation of their prognosis, information about thechoices available to them, and for those near the end of life a jointly agreed palliative care plan, built around their individual needs and preferences.
Markers of good practice• The renal multi-skilled team has access to expertise in the discussion of end of life issues including those of culturally diverse groups and varied
age groups, the principles of shared decision making, and training in symptom relief relevant to advanced non-dialysed ERF.
• Prognostic assessment based on available data offered to all patients with stage 4 CKD as part of the preparation for RRT described instandard two of part one of this NSF.
• People receive timely information about the choices available to them, such as ending RRT and commencing non-dialytic therapy, and havea jointly agreed care plan built around individual needs and preferences in line with palliative care principles.
• People who are treated without dialysis receive continuing medical care including all appropriate non-dialytic aspects of CKD, and whereverpossible are involved in decisions about medication options.
• Individuals are supported to die with dignity, and their wishes met wherever practicable regarding where they die, their religious and culturalbeliefs, and the presence of the people closest to them.
• The care plan includes culturally appropriate bereavement support for family, partners, carers and staff.

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
10
NationalServiceFrameworkstandard/qualityrequirement:
All children, young people and adults with chronic kidney disease (CKD) are to have access to information that enables them with their carers to make informed decisions and encourages partnership in decision-making, with an agreed care plan that supports them in managing their condition to achieve the best possible quality of life.
Keyprogresstodateincludes:
●● thelaunchofMyKidneyCarePlan1resourcestosupportcareplanning,andtheRenalHaemodialysisPatientChecklist2
●● anewNHSChoiceswebsiteincludinganonlinekidneydiseaseself-assessmenttool
●● provisionofadvocacyofficersbytheNationalKidneyFederation3tosupportpatientswithkidneyfailure.
SincetheintroductionoftheNSFforRenalServices,thepublicationoftheNHSNextStageReview4rightlyplacedfurtheremphasisontheempowermentofpatientsandmadequalitytheorganisingprincipleoftheNHS.Patientsmustbegivenmoreinformationandchoice,increasedcontrolovertreatmentoftheirconditionandinclusionintheplanningofservicesiftheyaretoofferquality,valueformoneyandimprovedoutcomes.ThisconceptalsounderpinsimplementationoftheNSF.
Weareworkingtoensurethatkidneyservicescontinuetoberesponsivetoeveryindividual,focusedonpreventionofill-health,andcapableofengagingpatientsandcliniciansinshareddecision-makingateverystageofthecarepathway.
1 www.kidneycare.nhs.uk2 HMGovernment(2008)RenalHaemodialysisPatientChecklist.www.dh.gov.uk/en/
Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_0824593 www.kidney.org.uk4 Darzi,Lord(2008)High�Quality�Care�For�All:�NHS�Next�Stage�Review�Final�Report.
London:DepartmentofHealth.www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/DH_085825
1 A patient-centred service

1Apatient-centredservice
11
Information for patientsInformationisvitalininvolvingpatientsatallstagesofkidneydiseaseandmuchworkhasbeendonetoimproveeducationalinformation.NHSChoices,5 whichprovidesasingle‘frontdoor’forthepublictoallNHSonlineservicesandinformationthroughthecountry’sbiggesthealthwebsite,hascreatedameansofunlockingtheinformationresourcesoftheNHS.Atanationallevel,NHSKidneyCareiscontinuingtodevelopandrefinethecontentontheprevention,diagnosisandtreatmentofkidneydisease.
Charities,industry,patientgroupsandhealthprofessionalscontinuetoworktogethertoproducemanyvaluableinformationmaterials.OneexampleistheLivingwithKidneyDisease DVD6 project.ThisisauniquehealthawarenessresourceproducedwiththeinvolvementoftheBritishRenalSocietyKidneyResearchUK,theRenalAssociation,theBritishTransplantationSocietyandtheNationalKidneyFederation.TheDVDcoversunderstandingofkidneydiseasefornewlydiagnosedpatientsandpracticaladviceforthosebeginningdialysis.
5 www.nhs.uk/Pages/HomePage.aspx6 www.kidneyresearchuk.org/shopping/living-with-kidney-disease-dvd.php

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
12
The ABLE Programme
TheABLE7(ABetterLifethroughEducationandEmpowerment)programmeiscommittedtoensuringthathealthinequalityissuesareprioritisedalongthewholespectrumof,andevenbefore,CKDisdiagnosedinblackandminorityethnic,andotherat-riskgroups.Thishastakenplacethroughaportfolioofresearchandawarenessprojects,thedevelopmentofliteratureandDVDsandthedevelopmentofapeereducatormodelwithfundingsupportfromtheDepartmentofHealth.
Theuseofpeereducationisanestablishedmethodologyforpromotinghealthawarenessingroupsthataredifficulttoaccess.Peereducatorsarelaymembersofacommunitywhoaretrainedandsupportedtoimpartkeymessages.Theyhavelinguisticandculturalempathyaswellasanunderstandingofsharedhealthexperiences.KidneyResearchUKhasbeenutilisingthismodelinseveralofitsABLEprojects.
Onepatientsaid:“Had�a�project�like�ABLE�been�in�place�long�before,�I�feel�that�my�renal�failure�may�have�been�prevented�or�at�least�delayed�and�my�family�and�I�would�have�been�prepared.�I�am�sure�many�patients’�thoughts�mirror�mine.”
ThroughABLE,KidneyResearchUKaimstodetermineeffectivemethodsofattractingindividualsfromdifferentethniccommunitiestoparticipateinhealthawarenessprogrammes.Thiswillhelptodeterminethemosteffectivemethodologyandinformbestpractice.
ArecentlycompletedABLEstudyintoattitudestowardsorgandonationhighlightedtheneedformoreresourcesaboutorgandonationtobeavailableforblackandminorityethnicgroups.Theseresourcesareneededinordertofacilitatediscussionanddecision-making.KidneyResearchUKbelievespeereducatorsplayakeyroleinfacilitatingthesediscussions.
Care planningInEngland,15.4millionpeoplehavealong-termcondition.Asaresultofanageingpopulation,itisestimatedthatby2025,therewillbe42%morepeopleinEnglandaged65orover.Thiswillmeanthatthenumberofpeoplewithatleastonelong-termconditionwillrisebynearly3millionto18million.
Thevastmajorityofpatientswithlong-termconditions,includingkidneydisease,wanttobeinvolvedindecisionsabouttheircare.Theywanttochoosewhichtreatmentprocessbestsuitstheirneeds,andtoshareresponsibilityformanagingtheircondition.Weknowthathealthimproveswhenpatientsaregivenmoreinformationandcontrolovertheirtreatmentoptions.
7 www.kidneyresearchuk.org/special-projects/able.php
1Apatient-centredservice
13
BoththeNSFandtheNextStageReviewhavesetoutavisionforpatientsofallagestooptimisetheroletheytakeinmanagementoftheirowncare.Individualcareplans,educationandaccesstoamulti-skilledteamallplayaroleinthis.GuidanceissuedbytheDepartmentofHealth,Supporting�people�with�long-term�conditions�to�self�care,8 highlightedtheneedtocreateafullyintegratedsystem,withappropriatelytrainedfrontlinestaff,toenablepeoplewithlong-termconditionstotakegreaterresponsibilityfortheirowncare.Tohelpwithimplementation,Your�Health,�your�way�–�a�guide�to�long-term�conditions�and�self�care9waslaunchedonNHSChoicesinNovember2008.Thisprovidesinformationaboutthechoicesthatshouldbeavailablelocallytosupportself-careinpartnershipwithhealthandsocialcareprofessionals.
My Kidney Care Plan
Individualcareplansareacriticalpartofcareandarenowusedeffectivelyinmanykidneyunits.Agreedcareplansprovideindividualswithpersonalinformationandpeaceofmind,buttheyalsohelptobuildimprovedpartnershipsbetweenpatients,thecliniciansandthewholemultidisciplinaryteam.Careplansforchildrenandyoungpeoplecontinuetoinvolveparentsaswellasthekidneycareteam.
NHSKidneyCarelaunchedMy�Kidney�Care�PlanonWorldKidneyDayinMarch2009.EveryadultpatientwithCKDwillnowbegivenapersonalfolder.Theywillbeabletousethemtodiscussindetailtheirneedsandconcernswithaspecialistnurse,orothertrainedmemberoftheirkidneyteam,andkeepnotesintheirfolder.Careplanningisnot,however,simplyaboutfillinginforms.Itisadiscussionthatputstheperson,theirneedsandchoicesatthecentrewithafocusonachievingoutcomes.MyKidneyCarePlan allowstimeforpatientstoaskquestionsthatreallyconcernthemaboutaspectsoftheirdiseaseandhowitaffectstheirdailylife.
Forhaemodialysispatients,theDepartmentofHealth,inpartnershipwiththeNationalKidneyFederationandtheBritishRenalSociety,haveproducedtheRenal�Haemodialysis�Patient�Checklist.Thisisachecklistofquestionsthatpatientshighlightedasparticularlyimportanttoaskfromtimetotimeandtodiscusswithanurseordoctor.ThechecklistwasdistributedbytheNationalKidneyFederation.
8 DepartmentofHealth(2008)Supporting�people�with�long-term�conditions�to�self�care:�A�guide�to�developing�local�strategies�and�good�practice.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4130725
9 DepartmentofHealth(2008)Your�health,�your�way�–�a�guide�to�long-term�conditions�and�self�care.www.dh.gov.uk/en/Healthcare/Longtermconditions/yourhealth/index.htm

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
14
Inaddition,theNHSInstituteforInnovationandImprovementpublishedFocus�on:�Preparing�for�End�Stage�Renal�Disease10 inearly2008,providinganswerstoquestionsonallaspectsofaneffectiveclinicalpathwayfromdiagnosisofendstagerenalfailure,throughtoassessmentandadditiontothetransplantlist.Theaimofthe‘Focuson’seriesistohelplocalhealthcommunitiesandorganisationsimprovethequalityandvalueofthecaretheydeliver.
Patientinvolvementintheplanningofservicesisalsoimprovingatapersonal,localandnationallevel.Inthelasttwoyears,majorstakeholderconferencesinvolvingpatientshavebeenheldatnationalandlocallevel.Patientengagementhasbeenachievedwithinkidneyunits,andisbeingfacilitatedbythecreationoflocalkidneynetworks.
TheDepartmentofHealthproducedtheVascularProgrammeBriefingPacks11toprovidethe10strategichealthauthorities(SHAs)withanassessmentofprogress,opportunitiesandfuturechallengesinkeyareasofvasculardisease,includingrenaldisease.Theyprovidedataaboutrenaldiseasefromthevarioussourcesavailable,includingtheQualityandOutcomesFramework(QOF)12andHospitalEpisodeStatistics(HES).13ThisdatacanbeusedtofacilitateimplementationoftheNSF.
SummaryProgresscontinuestobemadeinprovidingpatientswithbetterinformationandresourcestosupportchoiceandarealpartnershipwithprofessionalsintheplanninganddeliveryoftheircare.Thismustremainakeyfocusandbecomefullyembeddedacrossthecarepathwayifthebestqualityoutcomesforpeoplewithkidneydiseasearetobeachieved.
10 NHSInstituteforInnovationandImprovement(2008)Focus�on:�Preparing�for�End�Stage�Renal�Disease.�London:NHSInstituteforInnovationandImprovement.www.institute.nhs.uk/option,com_joomcart/Itemid,26/main_page,document_product_info/products_id,367.html
11 DepartmentofHealth(2007)VasularProgrammeBriefingPacks.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_073830
12 www.dh.gov.uk/en/Healthcare/Primarycare/Primarycarecontracting/QOF/index.htm13 www.hesonline.nhs.uk

15
2Prevention,earlydetectionandmanagementofchronickidneydisease
NationalServiceFrameworkstandard/qualityrequirements:
People at increased risk of developing or having undiagnosed chronic kidney disease, especially people with diabetes or hypertension, are identified, assessed and their condition managed to preserve their kidney function.
People with a diagnosis of chronic kidney disease receive timely, appropriate and effective investigation, treatment and follow-up to reduce the risk of progression and complications.
Keyprogresstodateincludes:
●● increaseddiagnosisandmanagementofchronickidneydiseaseinprimarycare
●● introductionofNICEguidanceontheearlyidentificationofchronickidneydisease
●● inclusionofkidneyandothervascularindicatorsintheQOFinprimarycare
●● productionofapatientleafletonidentifyingunhealthykidneys.
CKDisthoughttoaffectupto1in8peopleinEngland.Itisacommon,harmfulandtreatablecondition,andwithoutearlydiagnosispatientsaresubjecttoprogressiveillnessandpossibleirreversibleestablishedrenalfailure,resultingintheneedfortransplantation,dialysisorconservativemanagement.
Prevention of chronic kidney diseaseKidneydiseaseisontheincrease–itiscloselylinkedwithotherconditions,includingdiabetesandhypertension,whichhaveincreasingprevalence.Theseconditionsallsharesimilarriskfactors,includingobesity.IncidenceofCKDincreaseswithage,whichishighlysignificantinviewoftheincreasingproportionofolderpeopleinourpopulation.Also,CKDtendstobemoreprevalentamongblackandminorityethniccommunities.CKDisalsoariskfactorforacutekidneyinjury.
2 Prevention, early detection and management of chronic kidney disease

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
16
Oneofthegreatestchallengesfacingkidneyservicesnow,andoverthecomingyears,israisingawarenessaboutkidneydiseaseanditsprevention.Itisonlybyunderstandingtheeffectthatwiderinfluencesandriskfactors,suchasotherdiseasesormodifiablelifestylefactorsincludingobesity,haveonkidneydisease,thatpreventionandtreatmentwillbeimproved.
Change4Life
Change4Life14waslaunchedinJanuary2009.Itisasociety-widemovementthatencourageseveryonetomakechangestotheirdietandactivitylevelsinordertoreversethegrowingtrendofobesityandobesity-relatedillnesses.This,alongwithHealthy�Weight,�Healthy�Lives15andtheNICEguidanceObesity:�the�prevention,�identification,�assessment�and�management�of�overweight�and�obesity�in�adults�and�children,16demonstratethecommitmenttotacklingriskfactorsassociatedwithkidneydiseaseatacommunitylevel.
Early detection and managementEarlydiagnosisandgoodmanagementofCKDwithinprimarycarearevital.Giventhestronglinksbetweenkidneydiseaseandotherdiseases,NICEguidelinesonCKD,diabetes,hypertensionandanaemiaareprovingcriticalinpreventionandmanagementofkidneydisease.Inaddition,theNHSHealthCheckprogramme(seeboxopposite)isamajorinitiativeaimedatpreventingandreducingtheriskofheartdisease,stroke,diabetesandkidneydisease.
14 www.nhs.uk/Change4life15 HMGovernment(2008)Healthy�Weight,�Healthy�Lives:�A�cross-government�strategy�for�
England.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_082378
16 NICE(2006)Obesity:�the�prevention,�identification,�assessment�and�management�of�overweight�and�obesity�in�adults�and�children.NICEClinicalGuideline43.www.nice.org.uk/CG43

2Prevention,earlydetectionandmanagementofchronickidneydisease
17
NHS Health Check
PhasedimplementationoftheNHSHealthCheck17programmebeganinearly2009.Everyonebetweentheagesof40and74,whohasnotalreadybeendiagnosedwithoneoftheseconditions,willbeinvited,onceeveryfiveyears,tohaveachecktoassesstheirriskofheartdisease,stroke,kidneydiseaseanddiabetes.Theywillbegivensupportandadvicetohelpthemreduceormanagethatrisk.
Atfullroll-outthisprogrammecoulddetectatleast20,000casesofdiabetesorkidneydiseaseearlier,allowingindividualstobebettermanagedandimprovetheirqualityoflife.
NHSChoicesalsohostsanonline kidneydiseaseself-assessmenttool.18ThistoolcomplieswithNICEguidanceandhelpstoassessanindividual’sriskofkidneydiseasebasedonsimplequestions,includingmedicalanddrughistory.
NICEguidelines, Early�identification�and�management�of�chronic�kidney�disease�in�adults�in�primary�and�secondary�care,19publishedin2008areprovingavitaltoolforhealthcareprofessionalsthroughprovisionofdefinitive,evidence-basedadviceonoptimumtreatmentandcareofpatients.Theguidelinessetouthowbesttoidentifythoseatriskofprogressionandseriouscomplications,andoutlinehowtomanagetheircare.
Wehaveseenrealprogressinthediagnosisandearlymanagementofkidneydiseaseoverthelastfiveyears,anditisanareatobeproudofandtocontinuetobuildon.TheNHSisaworldleaderintheareaofkidneydiseasepreventionandearlydetection.ThishascomeaboutfollowingthestandardisationoftestsforkidneydiseaseusingestimatedGlomerularFiltrationRate(eGFR)andtheintroductionoftheNICEguidelinesin2008,whichinclude;guidanceonproteinuriatesting.
Before2006,CKDwasrarelyidentifiedinprimarycare.Theintroductionofthe QOF,withGPsrewardedpartlybasedonhowwelltheymanagepatientswithkidneydisease,hashelpedtoensurebetterdiagnosisinprimarycare.TheintroductionoftheQOFhasseenadramaticincreaseinthenumberofpatientsbeingdiagnosedwithCKD,whopreviouslymaynothavebeenidentified.
17 www.nhs.uk/planners/nhshealthcheck/Pages/NHSHealthCheck.aspx18 www.nhs.uk/Tools/Pages/Kidneydisease.aspx?Tag=Lifestyle+checks19 NICE(2008)Early�identification�and�management�of�chronic�kidney�disease�in�adults�
in�primary�and�secondary�care.NICEClinicalGuideline73.http://guidance.nice.org.uk/CG73/NiceGuidance/pdf/English
AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
18
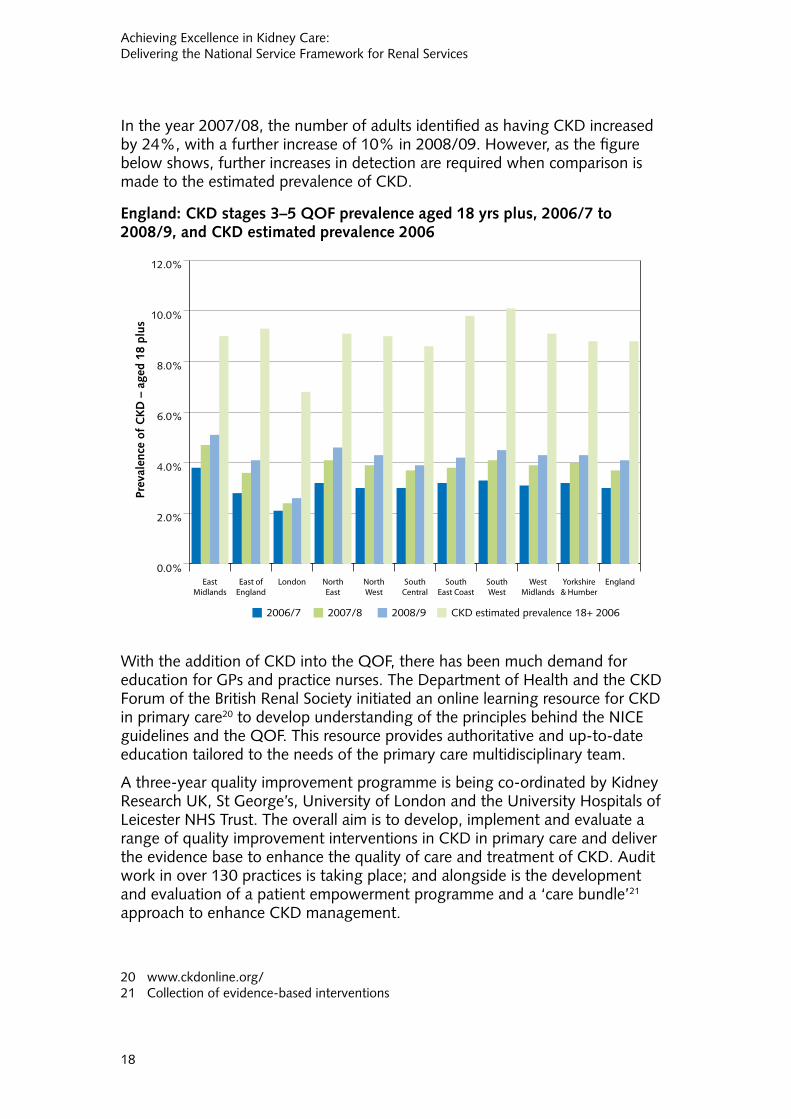
Intheyear2007/08,thenumberofadultsidentifiedashavingCKDincreasedby24%,withafurtherincreaseof10%in2008/09.However,asthefigurebelowshows,furtherincreasesindetectionarerequiredwhencomparisonismadetotheestimatedprevalenceofCKD.
England: CKD stages 3–5 QOF prevalence aged 18 yrs plus, 2006/7 to 2008/9, and CKD estimated prevalence 2006
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
EnglandYorkshire& Humber
WestMidlands
SouthWest
SouthEast Coast
SouthCentral
NorthWest
NorthEast
LondonEast ofEngland
EastMidlands
Prev
alen
ce o
f C
KD
– a
ged
18 p
lus
2006/7 2007/8 2008/9 CKD estimated prevalence 18+ 2006
WiththeadditionofCKDintotheQOF,therehasbeenmuchdemandforeducationforGPsandpracticenurses.TheDepartmentofHealthandtheCKDForumoftheBritishRenalSocietyinitiatedanonlinelearningresourceforCKDinprimarycare20 todevelopunderstandingoftheprinciplesbehindtheNICEguidelinesandtheQOF.Thisresourceprovidesauthoritativeandup-to-dateeducationtailoredtotheneedsoftheprimarycaremultidisciplinaryteam.
Athree-yearqualityimprovementprogrammeisbeingco-ordinatedbyKidneyResearchUK,StGeorge’s,UniversityofLondonandtheUniversityHospitalsofLeicesterNHSTrust.Theoverallaimistodevelop,implementandevaluatearangeofqualityimprovementinterventionsinCKDinprimarycareanddelivertheevidencebasetoenhancethequalityofcareandtreatmentofCKD.Auditworkinover130practicesistakingplace;andalongsideisthedevelopmentandevaluationofapatientempowermentprogrammeanda‘carebundle’21approachtoenhanceCKDmanagement.
20 www.ckdonline.org/21 Collectionofevidence-basedinterventions

2Prevention,earlydetectionandmanagementofchronickidneydisease
19
TheDepartmentofHealth,inassociationwiththeNationalKidneyFederation,andtheBritishRenalSociety,hasproducedaninformationleafletforpatientswhohavebeenofferedatestforproteinuria,Identifying�unhealthy�kidneys:�what�do�l�need�to�know�about�proteinuria?.22Thisleafletincludesinformationaboutthecausesofproteinuria,thetestsandtheimplicationsofmanagingunhealthykidneystogetherwithdiabetesandhighbloodpressure.
BuildingagreaterunderstandingofCKDatprimarycarelevelandensuringthatcareisintegratedbetweenprimaryandsecondaryorganisationsisoneofthekeyimprovementsbroughtaboutbytheNSFwithmoreeffectivesharingofinformationbetweenorganisationsacrossthecarepathway.InMiddlesbrough,forexample,nephrologistsareofferinganemailhelplineforGPswithallqueriesansweredwithin24hours.Anotherexampleofinnovationinthisareaisthedevelopmentofe-consultationsinBradfordandAiredale(seebox).
22 DepartmentofHealth(2009)Identifying�unhealthy�kidneys:�what�do�l�need�to�know�about�proteinuria?�Information�for�patients.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_104643

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
20
Electronic consultation (e-consultation) in Bradford and Airedale
PrimarycareteamsinEnglandhaverecentlyassumedgreaterresponsibilityforthemanagementofCKD.ImprovementsinthedetectionofCKDhaveledtoagreaterdemandforspecialistrenalservices.Theavailabilitytonephrologistsoftheclinicalinformationcontainedinprimarycareelectronichealthrecordsislikelytoenhancecommunication,hencesupportingthemanagementofpatientswithrelativelymildandnon-progressiveCKDinthecommunity,allowingspecialistresourcestobedirectedtowardssupportingpatientswithmorecomplexneeds.
DrJohnConnolly(GeneralPractitioner,BradfordandAiredalePrimaryCareTrustandPrimaryCareLeadforTechnology,NHSYorkshireandtheHumber)andDrJohnStoves(ConsultantinNephrology,BradfordTeachingHospitalsNHSFoundationTrust)haveexploredtheuseofe-consultationtosupporttheongoingmanagementofpatientswithmildtomoderateCKDinprimarycare,thusavoidingtheneedforinitialassessmentinahospitalclinic.
TheChronicKidneyDiseaseElectronicAdvisoryService(CKDEAS)wasdevelopedusingacentralisedprimarycareITsystem.TheserviceallowsGPstosendelectronicreferralsandsharepatients’electronichealthrecordswitharenalspecialist.GPsuselocale-guidancetorequestane-consultation.Therenalspecialistisabletoviewimportantclinicaldetailsintheelectronichealthrecord,suchaspatientco-morbidities,medicationhistory,lifestylefactorsandpreviouscommunicationsfromotherspecialists.Adecisionisthenmadeastowhetherapatientshouldbereferredtoclinic,undergotestsorinterventionsintheprimarycaresetting,orcontinuetobemonitoredandtreatedbytheprimarycareteam.
Anevaluationoftheservicehasconfirmedthat,inselectedpatients,e-consultationisafeasiblealternativetohospitalreferral.DrStovescommented:“Manypatientsdon’tneedtoattendahospitalclinic.e-consultationisanexcellentwayofsupportingtheircareinthecommunity.Icanaccessawealthofclinicalinformationandthisallowsmetomakeadetailedclinicalassessmentandgivetimelyspecialistadvice.GPsvaluetheeducationalelementoftheservice,andtheyfeelbetterabletomanageuncomplicatedCKD.”DrConnollyadded:“GPsappreciategettingspecialistadviceaboutthemanagementofborderlinecases.ThispathwaymakesefficientuseofNHSresourcesandimprovespatientexperiencesimultaneously.”
Thepotentialenvironmentalbenefitsofe-consultationhavebeenrecognisedbytheGreenerHealthcareCampaign.RegionalinitiativessupportedbyYorkshireandtheHumberSHAmayleadtoformalcommissioningofsuchservicesinthefuture.

2Prevention,earlydetectionandmanagementofchronickidneydisease
21
SummaryTherehasbeenastep-changeimprovementintherecognitionofCKDinprimarycarebutthereisstillworktobedone.AlthoughmanymorepatientsarenowidentifiedashavingCKD,notallarereceivingbest-practicecare–forexamplehavingtheirbloodpressurecontrolled.Weknowfromtheimprovedcollectionofprevalencedatathatthereisstillconsiderablevarianceindetectionratesbetweenpracticeswithineachprimarycaretrustarea.
AppropriatesupportmustcontinuetobegiventoensurethatthosemostatriskarediagnosedandofferedthenecessarycareandmanagementacrossthewholeoftheNHS,toreapthefullbenefitsofthedramaticimprovementsindetection.

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
22
NationalServiceFrameworkstandard/qualityrequirements:
All children, young people and adults approaching established renal failure are to receive timely preparation for renal replacement therapy so the complications and progression of their disease are minimised, and their choice of clinically appropriate treatment options is maximised.
All children, young people and adults with established renal failure are to have timely and appropriate surgery for permanent vascular or peritoneal dialysis access, which is monitored and maintained to achieve its maximum longevity.
Keyprogresstodateincludes:
●● adecreaseinthenumberofpeoplepresentinglatewithestablishedrenalfailure
●● adecreaseinratesofmethicillin-resistantStaphylococcus�aureus(MRSA)infectionsinkidneypatients
●● developmentofan18-weekcommissioningpathwayforCKD
●● auditofvascularaccess.
Patientchoicesshouldbeavailablefromdiagnosistoend-of-lifecare,andthisisparticularlyimportantduringthetimebeforedialysis.Patientswithestablishedrenalfailureshouldfeelempoweredtochoosethetypeofrenalreplacementtherapythatisbestfortheirownpersonalcircumstances,andtheircareplanshouldreflectthis.Whetherdialysis,transplantationorconservativemanagementischosen,qualityofcareisachievedwhenpatientsandtheirfamiliesunderstandtheoptions,andhoweachchoicewillaffecttheirqualityoflife,andultimatelylengthoflife.
DatacollectedbytheUKRenalRegistry23showsthattherehasbeenasustainedreductioninlatereferralsovertheperiod2002–07,moremarkedoverthelasttwoyears,andalsoanincreaseinthepercentageofpatientsreferredover12monthsbeforedialysisinitiation.
23 www.renalreg.com/Reports/2008.html
3 Preparation, choice and dialysis access surgery

3Preparation,choiceanddialysisaccesssurgery
23
Timely preparation and informed choicesInorderforpatientstomakeinformedchoices,itremainscriticalthattheyhaveaccesstoeasy-to-understand,treatment-specific,comparableinformationonsafety,experiencesandpatientsatisfaction.Thechallengeistoensurethatsuitableinformationisavailableforallaudiences.InformationisavailableonlineviaNHSChoicesonthedifferenttreatmentmodalitiesavailableandthe18-week�commissioning�pathway24clearlysetsouttheneedfortimelyinformation,educationandreview.
Renal PatientView25
Liaisonwithdifferentmembersofthekidneymultidisciplinaryteamisbecomingstandard,andITisnowbeingusedmorewidelytosupportpatients.Morethan11,000patientsarenowregisteredwithRenalPatientViewandthisnumbercontinuestogroweachmonth.RenalPatientViewisanaward-winninginitiativethatusestechnologytogivepatientsrapidaccesstotheirbloodresults,cliniclettersandinformationabouttheirdiagnosisandtreatment,allviaasecureinternetlogin.Thistechnologyoffersanopportunityforgreaterpatientinvolvementthroughoutthecarepathway.RenalPatientViewwasdevelopedbytherenalcommunityinconjunctionwiththeRenalAssociationandtheRenalInformationExchangeGroup.
The year before renal replacement therapyIn2006/07,PhaseIIoftheRenalActionLearningSetprogramme,sponsoredbytheDepartmentofHealth,includedtwoactionlearningsetsfromCambridge(Addenbrooke’sHospital)andNorthYorkshire(YorkHospital).Theirlearningsetsfocusedonwhypatientsmaybereferredwithinsufficienttimeforadequatepreparationandhowthiscouldbeimproved.ThelearningandgoodpracticeexamplesarecapturedinDriving�Service�Improvement�through�Patient�Focus:�Report�of�the�Phase�II�Renal�Action�Learning�Sets�2006–2007.26
KidneyResearchUKisundertakingresearchspecificallyfocusedonthedialysispopulationtoexploretheimpactofpatientchoiceinrelationtothetypesofdialysistreatmentanditsimpactonthepatient’sabilitytocopewiththeirtreatment.Initsthirdyear,theBroadeningOptionsforLong-termDialysisintheElderly(BOLDE)27researchstudyisalreadyshowingpromisingprimaryoutcomes;forexample,thereisadifferenceinperceivedmentalwell-being
24 www.18weeks.nhs.uk/Content.aspx?path=/achieve-and-sustain/Specialty-focussed-areas/Renal/chronic-kidney-disease/
25 www.renalpatientview.org26 DepartmentofHealth(2008)Driving�Service�Improvement�through�Patient�Focus:�Report�
of�the�Phase�II�Renal�Action�Learning�Sets�2006–2007.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_083968
27 www.kidneyresearchuk.org

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
24
betweenperitonealdialysispatientsandhaemodialysispatients.Apublicationisdueoutshortlyontheinitialresults.
Transfer from paediatric to adult servicesTransferfrompaediatrictoadultservicesisanareathatneedsimproving.GettingtransitionalcarerightforyoungpeoplewithCKDiscrucial.Itrequiresrecognitionofthecomplexityoftransition,andthechangeinculturebetweenpaediatriccentresandadultrenalservices.Ifnotproperlyaddressed,itcanleadtonon-concordancewithmedicationortreatmentregimes,withsignificantclinicalandpsychologicalconsequences.
TheRenalActionLearningSetprogrammeincludedtwoactionlearningsetsontransitionsfromLondonandBirmingham.Theyidentifiedthattransitionwasaprocessthatrequiresthought,timeandresources.Planningshouldbeoveraperiodoftime,involvingbothpaediatricandadultteams,ratherthansimplyarrangingatransferdate.TheirlearningandgoodpracticeexamplesarecapturedinDriving�Service�Improvement�through�Patient�Focus:�Report�of�the�Phase�II�Renal�Action�Learning�Sets�2006–2007.
InJulytheBritishAssociationforPaediatricNephrology28andtheRenalAssociation29publishedatransitionstrategy,whichconsiderstheorganisationofservices,componentsoftransitionandworkforcerequirements.NHSKidneyCareislookingatwaystosupportyoungadultswithkidneydiseaseandhowtosustainandspreadgoodpractice.Itisintheprocessofaskingforexpressionsofinterestfromrenalnetworkstofundakeyworkerfor18months.Thekeyworker’srolewillbenotonlytocreatelinkswiththedifferentservices,butalsotolookatthegeographicplacingofservicesandinequalities,especiallyforminoritiesanddisabledpatients.
Dialysis access surgeryOneoftheprincipalaspectsofpre-dialysiscareforpatientsisthetimelyformationofvascularaccessforpatientsplanningtoreceivehaemodialysis,ortheappropriateplacementofacatheterforperitonealdialysis.
Forhaemodialysispatients,surgerytocreateanarteriovenousfistulaprovidesthebestlong-termvascularaccesswiththefewestcomplications.Arteriovenousfistulastakebetweenoneandtwomonthstodevelopandtimemustbebuiltintocareplansforpossiblerevisionwork.Achievingbestpracticeineverycaseischallenginggivensurgicalprioritiesandtheneedtoestablishpermanentaccesssixmonthspriortostartingdialysis.
Forperitonealdialysis,patientsmustalwaysbeinvolvedindecisionsaboutthepositioningofthecatheteranditshouldbeinsertedingoodtimebeforethestartofdialysis.
28 www.bapn.org/29 www.renal.org/

3Preparation,choiceanddialysisaccesssurgery
25
Audit of vascular access
TheNHSInformationCentreforhealthandsocialcarehasbeencommissionedtoconductanauditofvascularaccess30overthreeyears(2009–11).ThekeyaimistofindoutwhethertheproportionofpatientsstartinghaemodialysiswithfunctioningpermanentaccessmeetstheRenalAssociationandVascularSocietyguidelines31forpermanentvascularaccess,whichrecommendthat80%ofpatientscommencedialysiswithappropriateaccessandwhatthehealthcare-associatedinfectionratesassociatedwithvascularaccessareinthemaintenancehaemodialysispopulationandhowthiscompareswiththenationalaverageandbestperformance.
Itisthroughlearningfromthefindingsofsuchauditsthatwewillbeabletoimproveservicesforpatientsandensurethataccesssurgeryisappropriateandprovidingeffectiveandsafecare.
Minimising infectionsAswellasprovidingtimelyandappropriateaccessfordialysis,theadditionalkeyissuessurroundingdialysisaccesssurgeryincludeinfection,thrombosisandstenosis(narrowingofthearteries).Patientsreceivinghaemodialysisforkidneyfailureareatincreasedriskofinfection,particularlyiftheydonothaveappropriatevascularaccess.TheevidencesuggeststhattheriskofMRSAbacteraemiaiseighttimeshigherforpatientswithacathetercomparedwithapatientreceivingdialysisviaanintravenousfistula.MRSAbacteraemiamaybeamajorcontributortothehighermortalityofthosepatientswhopresentlatewithend-stagerenalfailure.
BetweenApril2007andMarch2008,188MRSAbacteraemiacaseswerereportedinpatientsreceivingdialysis,representing4.2%ofallMRSAbacteraemiacasesreportedduringthisperiod.Wheredataonaccesswasavailable,themajorityofpatientssufferingfromMRSAbacteraemiahadavenouscatheter,orhadusedoneintheprevious28days.
TheHealthProtectionAgency’snationalsurveillancesystemforthecollectionofdataonMRSAbacteraemia–theMandatoryEnhancedSurveillanceSystem(MESS)32–hasbeenadaptedfollowingapilotprojectineightrenalunitsandassociatedsatellitesin2006.ThissupportscollectionofdataonthosepatientswhodevelopMRSAbacteraemiaandwhoareonrenalreplacementtherapyandwillhelpauditandimproveservices.Datafromthe2008UKRenalRegistryannualreport33onreportedMRSAepisodesshowsa62%reductioninMRSAbacteraemiaratesamongdialysispatientsinEnglandsince2004.
30 www.ic.nhs.uk/services/national-clinical-audit-support-programme-ncasp/kidney-care/vascular-access
31 www.vascularsociety.org.uk/home.html32 www.hpa.org.uk/web/HPAweb&Page&HPAwebAutoListName/Page/119194216977333 www.renalreg.com/Reports/2008.html

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
26
SummaryProgresscontinuestobeshowninpreparingpatients,boththroughtheprovisionofinformationresourcesandvascularaccessfordialysispatients,gearedtooptimiseoutcomesforpeopleinneedofrenalreplacementtherapy.Goodresultshavebeenshownindrivingdownthenumberofhospital-acquiredinfectionsaffectingkidneypatients.Acontinuedeffortisrequiredtoimplementtimelybestpracticeinpreparingallpatientsforrenalreplacementtherapy(RRT),bothtominimisecomplicationsoftheirconditionandtomaximisechoice.

27
4Dialysis
NationalServiceFrameworkstandard/qualityrequirement:
Renal services are to ensure the delivery of high-quality clinically appropriate forms of dialysis which are designed around individual needs and preferences and are available to patients of all ages throughout their lives.
Keyprogresstodateincludes:
●● expansionofhaemodialysiscapacity
●● developmentoftheMORRIScapacityplanningtoolforrenalreplacementtherapy
●● developmentofaperitonealdialysiscommissioningspecification
●● developmentandmandatingoftheNationalRenalDataset
●● completionofthefirstnationaltransportaudit.
DemandforRRT,andespeciallydialysis,isonanupwardtrend.Thisisdueinparttotheageingpopulation,togetherwiththeincreasingincidenceofdiabetesandbettersurvivalratesforpatientsonRRT.Overalldemandforrenalreplacementtherapyroseby4%perannumbetween2002and2007.
Capacity and choiceManyfactorsinfluencedialysistreatmentchoiceandoptions,includinggeography,localpopulationdensity,agedistribution,ethniccompositionandthesocialdeprivationindexofthelocalpopulation.Inaddition,localresourcesandprofessionalunderstandingandexperienceofdialysisoptionsaffectavailabilitiesofmodalities.
GivenitssignificancewithintheNHS,dialysiscapacitywasbroughttotheattentionoftheNHSleadershipandhighlightedinthe2008/09operatingframework34asanareathatprimarycaretrustsandspecialisedcommissioninggroupswillwishtoconsider.NHSKidneyCareisworkingcloselywithspecialised
34 DepartmentofHealth(2007)The�operating�framework:�For�the�NHS�in�England�2008/09.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/publicationspolicyandguidance/dh_081094
4 Dialysis

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
28
commissioninggroupstoreviewdialysiscapacity.Thiswillincludeensuringthatexpansionplansarebasedonsoundassessmentoflocalneedandarecomprisedofabalancedportfoliooftreatmentoptions.
APaymentbyResults35(PbR)projectgrouphasbeensetuptoreviewthekeyissuesinrelationtothequalityofcosting,andtherecommendationsfornationaltariffs,inkidneyservicestoencouragebestpractice.Sixteenrenalunitshavetakenpartinsupplyingdetailedreferencecostdata,whichhasbeenusedtoinformtheproductionofachecklisttoensurecomprehensiveandconsistentreturnsfromall52trustsacrossEnglandthathaveakidneyservice.TheaimistoproduceabestpracticetariffandtobringdialysiswithinthescopeofPbR.
Model for optimising renal replacement investment and services (MORRIS)
Inordertoplaneffectivelyforthegrowingdemandforrenalreplacementtherapy,wemustgainanunderstandingofthecomplexrelationshipsthatexistinendstagerenaldisease,includingtheavailabilityoforgansfortransplantation.
MORRISisamodelcommissionedandbuiltbytheDepartmentofHealthtopredictthecostandvolumeofrenalreplacementtherapy,atbothanationalandlocallevel,overa10-yeartimehorizon.
MORRISrepresentsthealternativetreatmentmodalitiesofRRTandtracksovertimethenumberofadultscommencingRRT,movingbetweenmodalities(includingreceivingkidneytransplants)anddying.
Testingofthebasicmodelusingnationalassumptions,includingtransplantratesandmortalityrates,tookplaceintheautumnof2009.Itwillbeusedtogenerateanannuallyupdatednationalforecastofdemand.Thecurrentprevalencerateshowsa4%growthonlastyear,inlinewithpreviousyearonyear4%annualgrowthoverthepastdecade.Runningtheprojectionbasedoncurrentassumptionsproducestheresultsshowninthegraphopposite,whichsuggestthehighlevelsofgrowthseenoverthepastdecadewillbegintoslowoverthenexttenyears.
TheintentionisthatMORRISwillbeavailabletocommissionerstosupportlocalplanning,usingtheirlocalassumptions.
35 www.dh.gov.uk/en/Managingyourorganisation/Financeandplanning/NHSFinancialReforms/index.htm

4Dialysis
29
Actual and estimated number of total renal replacement patients 2001–2017 – England
20,000
30,000
40,000
50,000
60,000
Estimate high2
Estimate low2
UK RR1
20172016201520142013201220112010200920082007200620052004200320022001
1 Figures from UK Renal Registry.
2 Department of Health estimates: annual growth rates 2.8% (low), 3.2% (high) using the MORRIS renal replacement model.
HaemodialysisThelatestunpublishedfiguresfromtheUKRenalRegistryshowthatin2008therewere17,349patientsonhaemodialysisand3,564patientsonperitonealdialysisinEngland.Fifty-twoacutetrustsnowofferhaemodialysis,and,togetherwithsatelliteunits,theserviceisnowprovidedon213sitesacrossEngland.
TheDepartmentofHealthhasfacilitatedtheIndependentSectorTreatmentCentreelectivesprogrammetoprovideexpandedhaemodialysiscapacityinnewfacilities,suchasthosefacilitiesinSouthport,BassetlawandBridlington.Itisexpectedthatthisschemewilldelivercapacityforapproximately178additionalhaemodialysisstationsoveraseven-yearperiod.
Theincreasingnumberofsatelliteunitsmeansthatmanypatientsarenowbeginningtobenefitfromdialysisclosertohome.However,withthedialysispopulationincreasing,fullconsiderationofalloptions,includinginparticulardialysisathome,isneededtomatchavailabilitywithpatientchoice.
TheAshfurlongDialysisCentrewasthefirstunitinEnglandtobebasedinaprimarycaresetting,andwas‘HighlyRecommended’intheHealthServiceJournalawardsin2006.

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
30
Haemodialysis in primary care premises – a potential solution: the Ashfurlong Dialysis Centre
Thisisajointventurebetweenprimaryandsecondarycareproviders.
TheAshfurlongDialysisCentrehousesfivestationsandisopensixdaysaweek.Upto25patientscanbetreatedthreetimesaweek.Theunitisnurseled,andsupportedbyspeciallytrainedGPsfromwithinthepracticewhoholdreviewclinicsfortnightly,andmultidisciplinarymeetingsmonthly.FurthersupportisavailablefromtheconsultantsbasedatHeartofEnglandFoundationTrust,ifrequired.
Approvalfortheincreasedrevenuecostswereobtainedfromthepan-Birmingham,StaffordshireandShropshirespecialisedcommissioninggroups.Approvalwasgrantedbecausethisprojectwaslikelytodeliveradditionalcapacityatlowcapitalcost,withasignificantimprovementinpatientexperience.
OutcomesaremonitoredmonthlybyauditagainsttheRenalAssociationstandardsfordialysisprovision.Overall,theperformanceagainstthesestandardshasimprovedsignificantlyforthepatientswhohavetransferredtoAshfurlongfromlargerunits.
ExperienceatAshfurlongDialysisCentrehasshownthathaemodialysiscanbeprovidedinprimarycare,underthesupervisionofGPs,safelyandeffectively.Patientslikethelocationandenvironment,andoutcomesaregood.AttheAshfurlongDialysisCentretheyhavefoundthistobeacapital-efficientmethodofprovidinghaemodialysiscapacityveryquickly,withonlyamodestincreaseinrevenuecosts.
Themajorityofhaemodialysispatientsdialyseinhospital,withhomehaemodialysisaccountingforjust2%ofdialysispatients.Thepercentageofdialysispatientsreceivinghomehaemodialysisvariedgreatly,fromzeroin20centrestogreaterthan5%ofalldialysisactivityinsixcentresduring2008,andsomehavesinceimprovedonthisposition.
Actionisstillneededtoclosethegapbetweenthenumbersofpatientswhocurrentlychooseself-care,andthesuggestionbyNICEthatupto15%ofchronichaemodialysispatients,whereclinicallyappropriate,maybeexpectedtochoosehomehaemodialysis.Whileself-caremaynotbesuitableforeveryone,itcanofferrealbenefits,includinglesshospitalisation,reducedmedicationandgreaterindependence.
Dialysis away from baseTheNSFemphasisedthat,forreasonssuchaswork,education,holidaysandfamilyvisits,itisimportantthatpatientsareabletodialyseawayfromhome.

4Dialysis
31
Theissueofdialysisawayfromhome(nowreferredtoasdialysisawayfrombase(DAFB))isacontinuingproblem.
TheDepartmentofHealthissuedguidanceinJune2007,Temporary�haemodialysis�away�from�home:�funding�arrangements�for�NHS�patients�resident�in�England,36highlightingtheneedfortruststomakeprovisionforDAFBandtodeveloplocalpoliciestomanagethis.However,progressinimplementingthishasbeenslow.
TheDepartmentofHealthsetupaworkinggroupin2008,ledbyBobDunn,RegionalAdvocatefortheNationalKidneyFederation,tolookspecificallyatwaystoimproveapatient’sexperienceofDAFB.Followingthereportfromtheworkinggroup,theDepartmentofHealthandNHSKidneyCarearecurrentlyworkingwithspecialisedrenalcommissionerstoidentifywaysinwhichwecanimprovetheavailabilityofdialysisforpatientsawayfrombase.
Theintroductionofastandardtarifffordialysis,initiallyonanon-mandatorybasis,willhelptoreducethevariationsinthechargesinEngland.
Peritoneal dialysisAssistedperitonealdialysis(PD)canofferanalternativeforkidneypatients,particularlythosewhoareelderlyorfrail,whoseonlyotheroptionsmaybehospitalhaemodialysisorconservativemanagement.
Thereiswidevariationaroundthecountry,bothinthenumberofpatientsonPDandinthetypesofPDavailable.Ithasbeenshownthat50%ofpatientsgivenfreechoicewillchoosePD.AcommissioningspecificationforPD37hasbeendevelopedbyNHSKidneyCarethathasbeenwrittenforpatients,commissionersandprovidersofrenalservices.Allrecommendationsarederivedfrompublishedevidence,currentbestpracticeandconsultationwithstakeholders.
ThisspecificationprovidesacomprehensiveguidetobestpracticePD,withoutcomemeasuresapplicableateachstage.Thiswillbeavitaltoolinbroadeningthedeliveryofhigh-qualitycare,drivingforwardserviceimprovementbyofferinggreaterchoiceandflexibilityforpatientsacrossEngland.
National Renal DatasetTheNationalRenalDataset38(ROCR/OR/0192/001)hasbeenapprovedbytheInformationStandardsBoardforHealthandSocialCareasaFullOperationalInformationStandardtomonitorimplementationoftheNSF.Thedataset
36 DepartmentofHealth(2007)Temporary�haemodialysis�away�from�home:�funding�arrangements�for�NHS�patients�resident�in�England.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4084218
37 NHSKidneyCare(2009)Specification�for�the�Commissioning�of�Peritoneal�Dialysis�Pathway.www.kidneycare.nhs.uk/i/assets/Commissioning_of_PD_Pathway_Oct_09.pdf
38 www.dh.gov.uk/en/Healthcare/Renal/DH_103601

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
32
ismandatedforcollectionbytheUKRenalRegistry39andNHSBloodandTransplant40.Implementationofthedatasetismandatedintwophases:
●● collectionof693dataitemsfromMay2009and
●● collectionofanadditional188dataitemsfromApril2011.
TransportTransportremainsamajorissueforthemajorityofpatientsreceivinghaemodialysis,withthoseonhospital-baseddialysismakingonaverage312journeystoandfromtheirdialysisunitseveryyear.
In2006,theDepartmentofHealthissuedrevisedandupdatedguidance,Income�generation�car�parking�charges�best�practice�for�implementation,41withastrongrecommendationthattrustsconsidertheprovisionofsubsidisedorfreecarparkingforthosepatientsattendingregularlyforongoingtreatment.
AnexampleofaninnovativetransportsolutioncanbefoundatBirminghamChildren’sHospital.
Transport innovation in Birmingham
AgoodexampleofinnovativesolutionsforrenaltransportisBirminghamChildren’sHospital’soptionforparentstodrivethemselves,withaguaranteedfreeparkingspaceandreimbursementforfuel.Inthethreeyearsthattheschemehasbeenrunning,thetrustcalculatesthatithassavedmorethan£110,000onhospitaltransportcosts.
Inordertogatherevidenceofareasofparticulartransportchallengesandtoensureappropriategoodpracticeiscommissioned,theHealthcareQualityImprovementPartnershiphasproduced,viatheNHSInformationCentre,high-levelresultsfromatransportsurveyundertakeninOctoberthisyear.Itsfirstannualreport,National�Kidney�Care�Audit,�Patient�Transport�Survey�Report,42 madeeightclearrecommendationsincludingarecommendationthatnopatientshouldhavetopayfortransporttoandfromdialysisunits.
Asecondannualreportwilltaketheformofextendedadviceandgoodpracticegiventokidneyunitsandcommissioners,andathirdreportwillassessreturnsprovidedbyallofthekidneyunitsduringOctoberandNovember2010.
39 www.renalreg.com/40 www.nhsbt.nhs.uk/41 DepartmentofHealth(2006)Income�generation�car�parking�charges�best�
practice�for�implementation.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_062857
42 www.ic.nhs.uk/services/national-clinical-audit-support-programme-ncasp/kidney-care/patient-transport/results-of-the-patient-transport-survey-2008

4Dialysis
33
SummaryIfpatientsaretohaverealchoiceintheirpreferredmodeofdialysis,andifsupplyistokeeppacewithdemand,theremustbeacontinuedfocusonmorestrategicplanningofhaemodialysis,andincreasedoptionsforDAFB.Theprovisionofappropriatedialysis,anddialysisthatmeetsthepersonalchoiceofeverypatient,includingtodialyseathomeandawayfrombase,remainsoneofthemajorchallengesfacingtherenalcommunitytoday,overthenextfiveyearsandbeyond.

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
34
5 NHS Kidney Care – ‘Better Kidney Care for All’
NHSKidneyCarewassetupin2008andworkscloselywiththeDepartmentofHealthtoimproverenalservices.
Thischapterdetailstheorganisation’sroleandachievementstodate.
National Programme Lead
Research Officer
Information Officer
Communications Officer
Evaluation Officer
The role of NHS Kidney Care
NHSKidneyCareworkstoenablethekidneycommunitytobuildakidneyservicethatisfitforthe21stcentury,whichoffersaconsistent,highstandardofcareacrossthecountry.
ProgrammeDirector,BeverleyMatthews,headsupateamof12basedacrossEngland,andworksalongsidetheNationalClinicalDirectorforKidneyCareandtherenalpolicyteamattheDepartmentofHealth.
NHSKidneyCarehasnowbeenfullyoperationalforayear,andismakingrealprogressinfacilitatingthesuccessfulimplementationoftheNSFforrenalservices.
Administrator
Admin Support
NHS kidney organisation chart

5NHSKidneyCare–‘BetterKidneyCareforAll’
35
Kidney Care
National Programme Lead
National Programme Lead
National Programme Lead
National Programme Lead
National Programme Director
PA to Programme Director
NHS kidney organisation chart

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
36
What we do
NHSKidneyCarehasclearobjectivesthatenableustodeliverthestandardsandqualityrequirementsoutlinedwithintheNSFforRenalServices.Theseobjectivesfallwithinthestepsofthekidneycarepathway:
●● Primaryprevention
●● Kidneydiseaseinprimarycare
●● Advancedkidneydisease
●● Kidneytransplantation
●● In-centredialysis
●● Self-caredialysis
●● Renalreplacementtherapies
●● Conservativekidneycare
●● AcutekidneyInjury
Key achievements
●● DevelopmentofSHA-widekidneycarenetworksacrossEngland
●● Supportoftheimplementationofeffectivecareplanningthroughthedevelopmentofapersonalisedcareplanforallkidneypatients
●● DevelopmentandpublicationofEnd�of�Life�Care�in�Advanced�Kidney�Disease:�A�framework�for�implementation43
●● DevelopmentofrobustReferenceCostsforkidneydialysistoinformthecreationofanationaltariff
●● DevelopmentofaspecificationforthecommissioningofPeritonealDialysis
●● CreationofanAutonomousKidneyServicestoolkit
●● FundingofaSpecialistRegistrartoworkongreennephrology
43 www.kidneycare.nhs.uk/?sID=2&aID=92

5NHSKidneyCare–‘BetterKidneyCareforAll’
37
Projects in progress
NHSKidneyCareworkswithclinicalteamsandcommissionersofkidneycaretolookattheservicestheyoffertopatientswithkidneydisease.
Currentprojectsinclude:
●● End-of-lifecareinadvancedkidneydisease
● Kidneycommunitiesareactingasdevelopmentsitestocreatecarepathwaysandtosupportstafftodeliverhigh-qualityend-of-lifecarebyactioningEnd�of�Life�Care�in�Advanced�Kidney�Disease:�A�Framework�for�Implementation.
●● SupportingyoungadultswithCKD
● Kidneycarenetworksaredevelopingandwilldelivernewservicestosupportyoungadultswithkidneydisease,withtheaimofestablishingexamplesofbestpracticethatcanbeusedtohelpyoungadultswithotherlong-termconditions.
Formoreinformation,visitwww.kidneycare.nhs.uk,[email protected].

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
38
NationalServiceFrameworkstandard/qualityrequirement:
All children, young people and adults likely to benefit from a kidney transplant are to receive a high-quality service which supports them in managing their transplant and enables them to achieve the best possible quality of life.
Keyprogresstodateincludes:
●● increaseinorgandonationrates,particularlyfromlivingdonors
●● increaseinratesofpre-emptivetransplant
●● developmentofan18-weeklivedonorcommissioningpathway.
Organtransplantationisoneofmedicine’sgreatsuccessstories.Weknowthatasuccessfulkidneytransplantisthemostclinicallyeffectiveandcost-effectivetreatmentformanypatientswithestablishedrenalfailure.Kidneytransplantationisassociatedwithlowermortalityrates,higherqualityoflifeandlowercoststhaneitherhaemodialysisorPD.However,everyyearmanypatientsstilldiewhilewaitingforakidneyorotherorgantransplant.
Thereisalsoanurgentneedtoaddresshealthinequalities.PeopleofAsianorAfrican–Caribbeandescentarethreetofourtimesmorelikelythanwhitepeopletodevelopend-stagerenalfailureandneedakidneytransplant.However,theyarefacedwithamuchsmallernumberofpotentiallymatchingdonors.
Encouraging organ donationTheGovernmentisstronglysupportingtheneedtoexpandorgandonationthroughimplementationoftheworkoftheOrganDonationTaskforce,establishedin2006,withrepresentativesfromthetransplantcommunity,NHSBloodandTransplant,andthevoluntarysector.TheTaskforcehasworkedtoidentifybarrierstoorgandonationandaddressissuesaffectingdonationrates,andhassubsequentlytakenactiontoincreaseorgandonation.
6 Transplantation

6Transplantation
39
Organ Donation Taskforce
AreportbytheTaskforceinJanuary2008,Organs�for�Transplants:�A�report�from�the�Organ�Donation�Taskforce,44offered14recommendationsforthewayforward.Theserecommendationswereacceptedasafocusforactionoverthenextfiveyears,aimingtoachievea50%increaseindonation,whichequatesto700morekidneytransplants.
Significantprogresshasalreadybeenmade,althoughdialysisremainsthemostcommontreatmentoption.
ThefirstannualreportoftheOrganDonationTaskforceImplementationProgrammehighlightstheprogressthathasbeenmadeinthefirstyearoftheImplementationProgramme,particularlythechangesinstructuresandarrangementsintheNHS,withthemovetoacentrallymanaged,andenlarged,networkofdonortransplantco-ordinatorsandtheappointmentofclinicalleadsfororgandonationwithinhospitaltrusts.
Thesechanges,coupledwithgreaterpublicawarenessoforgandonation,haveledto:
●● anincreaseof11%indeceaseddonorrates
●● anincreaseof12%inlivingdonation
●● anincreaseof6.5%inthenumberofpeopleontheNHSOrganDonorRegister,takingthetotalto16.3million.
In2008/09,£16.5millionwasallocatedtotheNHSfororgandonationandtransplantation,withafurther£26.5millionallocatedfor2009/10.Anadditional£500,000wasprovidedfromtheDepartmentofHealthtosupportimplementationprogrammesandfundnationalevents,includingtheUKTransplantGamesandNationalTransplantWeek.
Increasing transplantationThetotalnumberofdeceasedkidneydonorsroseto859in2008/09from789in2007/08,andthenumberoftransplantsincreasedfrom1,453to1,570.Thenumberofnon-heart-beatingkidneydonorsincreasedto275from195in2007/08,andthenumberoftransplantsfromsuchdonorsincreasedby41%to474.
Livingdonorkidneytransplantsareincreasingandnowrepresentmorethanoneinthreeofallkidneytransplants.Therewere589in2005/06,690in2006/07,831in2007/08and927in2008/09.Thereis,however,stillmuchworktobedoneonraisingawarenessoflivingdonation,particularlyamongtheblack
44 DepartmentofHealth(2008)Organs�for�Transplants:�A�report�from�the�Organ�Donation�Taskforce.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_082122

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
40
andminorityethnicpopulationwhichmakesup23%ofthekidneytransplantwaitinglist,whilerepresentingonly8%ofthepopulation.
Extendedoptionsforlivingdonation isanimportantareaofprogress,andoverthelastfiveyearstherehasbeenmuchprogress,movingawayfromthesituationwheremosttransplantsbeingperformedarebetweenclosefamilymembers(bloodrelatives).Now,increasingly,extendedfamilyindividuals(non-bloodrelatives),spouses,partnersandfriendsarecomingforwardtodonate,andthesetransplantsareequallysuccessful.
In2008an18-weekcommissioningpathwayforlivingdonortransplantationwasdeveloped.Thispathwayplotsthepatientjourney,fromavolunteerbeingidentified,throughphasesofclinicalassessment,torehabilitationafterasuccessfultransplantoperation.
Bristol Children’s Hospital and Southmead renal unit have been using webcams so that patients can keep in touch with each other.
Livingdonortransplantsinchildrenareusuallyfromaparentorotherclosefamilymember,sothepatientexperiencecanbeparticularlystressful,withtwomembersofthesamefamilyundergoingsurgeryinaverysmalltimeframe.Thedonorcouldbethemaincarerforthechild,andasthesurgeryoftentakesplaceindifferentlocations,communicationbetweenpatientsisdifficult,visitingmaybeimpossibleinthefirstfewdays,andbothparentandchildareoftenveryworriedabouteachother.
UsingwebcamstokeepintouchisasimpleinnovationthatBristolChildren’sHospitalhaveintroduced.Theyhavefoundthatitcanmakeahugedifferencetothepatientexperience.Allroomsatthehospitalhaveinternetaccess,soallthatwasrequiredwasthepurchaseofalaptopfortherenalunitatSouthmeadtomakethiswork.
Followingarecentlivedonortransplantfrommothertoson,themotherwasabletoseeandtalktohersonontheeveningofthedayoftheoperation,andtheybothfoundthisextremelyreassuring.Thismeansofcommunicationwasagreatsupporttoallconcerneduntilthemotherwasabletocomeandvisitafewdayslater.
NHSKidneyCarerecentlysentoutquestionnairestogainanoverviewofcurrentcapacityanddemandforrenaltransplantationservices.ThiswastoensurethatcapacitywithintherenaltransplantcentresissufficienttomeettheriseindemandexpectedfromtheOrganDonationTaskforceReport(ODTR).Thequestionnairewassenttothespecialisedcommissioninggroups(SCGs),kidneycarenetworksandprovidertruststhathaveatransplantingcentre.

6Transplantation
41
TheresponsespointedtotheneedforfurtherpartnershipworktobringtogethercommissionersandprovidersforeachSCGarea,andledtothefollowingfourrecommendations:
●● Kidneycarenetworksshouldbringspecialisedcommissionersandprovidertruststogetherineachregion,establishingworkinggroupstomapoutcapacityissuesanddevelopfive-yearactionplans.
●● Specialisedcommissioners(withresponsibilityforkidneycare)shouldprovideleadershiplocallytothedevelopmentofthefive-yearplansthatareagreed,andensureinvestmentsfor2010/11andbeyondareidentifiedandprioritisedwiththeirSCGs/primarycaretrustsforconsiderationandinclusionasappropriateintoinvestmentplans.
●● NHSKidneyCareshouldco-ordinateanationalgroup,withonerepresentativefromeachoftheworkinggroups,toensurenationalconsistencyandenablecross-boundaryissuestobeaddressed.
●● TheOrganDonationTaskforceProgrammeDeliveryBoardshouldprovideresourcesfordedicatedprojectmanagementthroughtheNationalSpecialisedCommissioningTeam.
TherecommendationsarebeingtakenforwardonavoluntaryandcollaborativebasisthroughtheSpecialisedCommissionersforKidneyCareForum.
Pre-emptive transplantationAmarkerofgoodpracticeintransplantationis pre-emptivetransplantation,particularlyspecifyingthatpatientsareplacedonthenationaltransplantlistwithinsixmonthsoftheiranticipateddialysisstartdate,ifclinicallyappropriate.Currently,between10%and40%ofeachtransplantcentre’slistismadeupofpre-emptivepatients,andfiguresareincreasinglocallyyearonyear.
In2008/09,17%ofadulttransplantswerecarriedoutinpre-dialysispatients.Pre-emptivetransplantsaccountedfor25%ofallpaediatrickidneytransplants.
Itremainsessentialtoprovideclearandculturallyappropriateinformationtorecipientsanddonorsatallstagesoftheirtransplantifpatientchoiceistobebasedonsoundinformation.Inrecentyearswehaveseenmuchprogressinthisarea.Forexample,NHSBloodandTransplantoffersnationallyavailablepatient-focusedadviceandeducationalmaterial,asdomanylocalkidneyunitsandpatientorganisations.
Localinitiativesincludetheprovisionofpatientleaflets,togetherwithtransplantpatientinformationmeetingsforthoseconsideringlivingdonation.Theselocalmeetingsoftentakeplaceatthehospitalduringweekends,toallowdonors,recipientsandtheirfamiliestotalktosurgeons,clinicians,counsellorsandtransplantnurses,aswellaspost-transplantrecipientsanddonors,abouttheexperience.

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
42
SummaryImplementationoftherecommendationsoftheOrganDonorTaskforceisalreadyleadingtorisingnumbersofdonorsandtransplants,andseveralpromisinginitiativesareshowinggoodresults.However,sustainedprogresswillbeneededtoclosethegapbetweensupplyandrisingdemandsothatasmanypatientsaspossibleareabletobenefitfromakidneytransplant.ThecollectionofappropriatedatafromtransplantcentresfortheUKRenalRegistryandNHSBloodandTransplantremainscriticalforcomparativeandauditpurposes.

43
7Acutekidneyinjury(acuterenalfailure)
NationalServiceFrameworkstandard/qualityrequirement:
People at risk of, or suffering from, acute renal failure are identified promptly, with hospital services delivering high-quality, clinically appropriate care in partnership with specialised renal teams.
Keyprogresstodateincludes:
●● actionlearningsetstotackleacutekidneyinjury
●● AcuteKidneyInjuryCareInitiative(AKICI)conference
●● NICEguidance:Acutely�ill�patients�in�hospital:�Recognition�of�and�response�to�acute�illness�in�adults�in�hospital.
Acutekidneyinjury(AKI)(acuterenalfailure)occurswhenthereisafunctionaldeteriorationorstructuralchangeinthekidney.AKIcanoccurinavarietyofsettingsbutismostcommoninacutelyunwellpatientsinhospital.Thesepatientsareoftenolderadultswithco-existingillness,particularlyunderlyingCKDorcardio-vasculardisease,orthosereceivingtreatmentswithpotentiallynephrotoxicdrugs.WhilemanypatientswillmakeacompleterecoveryfromAKI,othersmaybeleftwithCKDwhichmayprogresstoestablishedrenalfailure.
Early recognition and prevention of acute kidney injuryAKImayaffectupto1in5peopleadmittedtohospital.ThedegreeofAKIvariesconsiderablybutismostlikelyinacutelyunwellpeople.MostepisodesofAKIoccurringinpatientswhereitisacomplicationofanotherconditionshouldbeappropriatelymanagedbyacutephysicians.Patientswithprimaryrenaldiseases,suchasacutenephritis,orthosewhomayrequirerenalreplacementtherapy,needpromptspecialistrenalinput.Closecollaborationbetweenkidneyandnon-kidneydepartmentsisvital.
In2007NICEproducedclinicalguidelinesfortherecognitionandtreatmentofacutelyunwellpatientsinhospital.45Theseguidelinesshouldassistcliniciansinrecognisingdeteriorationinpatients,andprovidethemwithguidanceonhowtotreatthesepatientsappropriately.NICEclinicalguidelinesonpreoperativetests,
45 NICE(2007)Acutely�ill�patients�in�hospital:�Recognition�of�and�response�to�acute�illness�in�adults�in�hospital.NICEClinicalGuideline50.www.nice.org.uk/CG50
7 Acute kidney injury (acute renal failure)

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
44
The�use�of�routine�preoperative�tests�for�elective�surgery,46publishedin2003,statethatthosewhoundergoelectivesurgeryshouldalwaysbeassessedpre-operativelytopreventavoidablecasesofAKI.
However,evidencesuggeststhatupto30%ofcasesofAKIarepreventable.ThegoodpracticehighlightedbytheNICEguidance,ifimplementedfully,shouldreducethesenumberssignificantly.Basicclinicalcareshouldidentifythoseatrisk,andsimpleinvestigationscanidentifyAKIatanearlystagewhentreatmentislikelytobemosteffective.Theseinvestigationsshouldestablishtheseverityandcauseofthekidneydisfunctionandhelpdirecttherapytotheunderlyingcondition,suchasinfection,heartfailureordrug-inducedinjury.
Earlyrecognition,togetherwithappropriateandtimelymanagementofAKI,iscriticalifpatientsaretoavoidprogressiontodialysisand,worsestill,multi-organfailure.Ithasbeenestimatedthat5–20%ofcriticallyillpatientsdevelopAKIandthemortalityratesarehigh,especiallyifrenalreplacementtherapyisrequired.
National Confidential Enquiry into Patient Outcome and Death – Adding Insult to Injury: A review of the care of patients who died in hospital with a primary diagnosis of acute kidney injury (acute renal failure)
TheneedtotackleAKIwasreinforcedbythepublicationofaNationalConfidentialEnquiryintoPatientOutcomeandDeath(NCEPOD)reportinJune2009.47 ThekeyfindingsandrecommendationshighlightedbythereportshowthatthereismuchworktobedonetoensurethatAKIisrecognisedandprevented.
Thekeyfindingsoftheadviserswhoreviewedthecaseswerethat:
●● only50%ofAKIcarewasconsideredgood
●● therewasanunacceptabledelayinrecognisingpost-admissionAKIin43%ofpatients
●● 33%ofpatientshadinadequateinvestigations.Theomissionswerebasicclinicalexaminationandsimplelaboratorytests
●● therewaspoorassessmentofriskfactorsforAKI
●● 20%ofpost-admissionAKIwasbothpredictableandavoidable.
Thesefindingscutacrossdifferentservicesandallspecialties,includingacutemedicineandnephrology.
46 NICE(2003)The�use�of�routine�preoperative�tests�for�elective�surgery.NICEClinicalGuideline3.http://guidance.nice.org.uk/CG3
47 NCEPOD(2009)Adding�Insult�to�Injury:�A�review�of�the�care�of�patients�who�died�in�hospital�with�a�primary�diagnosis�of�acute�kidney�injury�(acute�renal�failure).London:NCEPOD.www.ncepod.org.uk/2009report1/Downloads/AKI_report.pdf

7Acutekidneyinjury(acuterenalfailure)
45
A multidisciplinary approachAnAKICIconference,convenedbyNHSKidneyCare,washeldattheRoyalCollegeofPhysicianson18March2009.RepresentativesfrommanyspecialistcommunitiesfromaroundtheUKwereinvitedtosharetheirownperspectivesofAKIandhowitimpactsontheirspecialty.
Theaimsoftheconferencewerefordelegatestoworkcollaborativelyandconsiderarangeofkeyissues,includinghowtoworktowardsaconsensusdefinitionforAKI.ImprovementinthetreatmentofAKIhasbeenhinderedbythelackofauniformlyaccepteddefinitionandalackofsuitablysensitivebiomarkersforAKI.
TheDepartmentofHealthheldaworkshopinOctober2009withallkeystakeholders.Theaimwastoidentifytheactionthatneedstobetaken,bywhenandbywhom,tobestimplementtherecommendationsfromtheNCEPODreport.
TheDepartmentofHealthisdrawingupanactionplaninresponsetotherecommendationsmadebyNCEPOD.TheMedicalDirector,SirBruceKeogh,hastakenaspecialinterestinensuringthatservicesimprove,andtheNationalClinicalDirectorforKidneyCarehasbeenworkingwithSHAmedicaldirectorstoensurethatappropriateactionistaken.
Inadditiontothis,NICEisconsideringaproposaltodevelopaclinicalguidelinespecificallyaddressingtheprevention,detectionandmanagementofAKI.Thiswouldbuildontheguidelinefortherecognitionandtreatmentofacutelyunwellpatientsinhospital,andwouldbespecifictopatientssufferingfromAKI.Itwouldrequireimprovementsintrainingundergraduatesandpostgraduatestoprevent,detectandmanageAKI.ThiswouldaddressmanyoftheissuesraisedintheNCEPODreport.
SummaryPreventionandtreatmentofAKIneedstobeacorecompetencyforallclinicalstaff,wherevertheyareworkingandwhatevertheirprofessionorspecialty.ToimproveAKIidentification,managementandoutcomes,asystematicapproachisneeded.ThiswouldensurethatthepossibilityofAKIisconsideredinallacutelyunwellpatients,thatsimplebasicclinicalcareisalwaysdelivered,andthataco-ordinatedapproachtoAKImanagementisintegratedintothesafetyandqualitycultureoflocalNHSorganisations.

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
46
NationalServiceFrameworkstandard/qualityrequirement:
People with established renal failure receive timely evaluation of their prognosis, information about the choices available to them, and for those near the end of life a jointly agreed palliative care plan, built around their individual needs and preferences.
Keyprogresstodateincludes:
●● publicationofEnd�of�Life�Care�in�Advanced�Kidney�Disease:�A�Framework�for�Implementation
●● prescribingguidelinestoensurebestpracticeinthecareofkidneypatients
●● implementationoftheLiverpoolCarePathwayfortheDyingPatient.
TheNSFforRenalServiceswasthefirstnationalframeworktotalkaboutdeathanddying.End-of-lifecarecontinuestobeacriticalareaoffocusinkidneyservices.Itconcernsthosewhodecidenottoundergodialysis;thosewhochoosetowithdrawfromdialysisafteraperiodoftreatment;andthosewhoarecomingtotheendoftheirliveswhilecontinuingdialysis.
Personalattitudestodeathanddyingareinfluencedbymanyfactors,includingage,religionandculture,andkidneyteamsmustacknowledgetheseinfluencesandprovidethenecessarypatient-centredassessmentsandhigh-qualitycaresensitivetoeveryindividual’sneeds.Increasingly,thisinvolvesworkingacrossspecialtiesandempoweringboththepatientandthemultidisciplinaryteamwithend-of-lifecaretools.
A strategic approachInJuly2008,theDepartmentofHealthpublishedthe End�of�Life�Care�Strategy:�Promoting�high�quality�care�for�all�adults�at�the�end�of�life.48Tosupportthestrategy,theGovernmenthasmadeavailable£286millionofnewfundsforthe
48 DepartmentofHealth(2008)End�of�Life�Care�Strategy:�Promoting�high�quality�care�for�all�adults�at�the�end�of�life.London:DepartmentofHealth.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_086277
8 End-of-life care

8End-of-lifecare
47
periodto2011.Thestrategyincludedexamplesofgoodpracticeintheareaofkidneydisease.
NationalguidelinesandinitiativessuchastheLiverpoolCarePathwayfortheDyingPatient49arebeinglinkedmorecloselywithkidneyservices,andweareseeingmoresharingofgoodpracticebetweenunitsandimprovementinqualityend-of-lifecareinmanycentres.Inaddition,kidneyunitsareadoptingandcustomisinggenerictoolscreatedforotherdiseaseareas,suchasthepatient-heldPreferredPrioritiesofCare50documentthatrecordspersonalthoughtsandchoicesaboutend-of-lifecareandbestpracticeguidanceforcancerpatients,andtheGoldStandardsFramework,51whichsupportsmorepatientcontrolandchoiceinthecommunity.
Liverpool Care Pathway for the Dying Patient
TheLiverpoolCarePathwayfortheDyingPatientoffersthegoldstandardinend-of-lifecareandprovidesanevidence-basedframeworkforthedeliveryofappropriatecareforpatientsinthelastdaysandhoursoflife.Specialistpalliativecareteamsarenowtrainingrenalteamsonthe10-stepimplementationprogrammeinvolvingdeliveryofpersonalcarethatfocusesonthephysical,psychologicalandspiritualcomfortofpatients.
Prescribingguidelines,Liverpool�Care�Pathway�(LCP)�Guidelines�for�LCP�Drug�Prescribing�in�Advanced�Chronic�Kidney�Disease,52thatinformbestpracticeinthecareofkidneypatientsduringthelastweeksordaysoftheirliveswerepublishedin2008.Theguidelinesweredevelopedbyanexpertprojectgroup,overseenbytheLiverpoolCarePathwayRenalSteeringGroup,andhavebeenendorsedbytheRenalAssociationandtheBritishRenalSociety.Thisdocumentprovidesclearguidenceandadviceonmedicinesmanagementandthecontrolofdistressingsymptoms.Thiswillhelpprovidersofpalliativecaretorespectthewishesofpatientandcarersinthelastweeksanddaysoflife.
Support for patients, carers and cliniciansIn2008,aDepartmentofHealthrenalworkshopinvolvingpatients,carersandcliniciansgeneratedthemestofocusattentiononend-of-lifecare.Positiveoutcomesincludedagreementontheneedforclarityinterminology,developmentofmoreeffectivewaysofpatientsandcarersworkinginpartnership,collaborationwithnationalinitiatives,andexpansionofeducationandtrainingofstaff.
49 www.mcpcil.org.uk/liverpool-care-pathway50 www.endoflifecareforadults.nhs.uk/eolc/CS310.htm51 www.goldstandardsframework.nhs.uk52 DHRenalNSFTeamandMarieCuriePalliativeCareInstitute(2008) Liverpool�
Care�Pathway�(LCP)�Guidelines�for�LCP�Drug�Prescribing�in�Advanced�Chronic�Kidney�Disease. Liverpool:MarieCuriePalliativeCareInstitute.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_085320

AchievingExcellenceinKidneyCare:DeliveringtheNationalServiceFrameworkforRenalServices
48
In2009,thebestpracticeguide,End�of�Life�Care�in�Advanced�Kidney�Disease:�A�Framework�for�Implementation53waspublished.Thiswasanimportantstepinprovidingguidancetosupporttheservicetobeabletoofferpeoplewithadvancedkidneydiseasetheverybestcareinthelastyears,monthsanddaysoftheirlives.TheFrameworkisaboutenablingpeopletoachievehigh-qualityend-of-lifecare.Toachievethis,itexploresthekidney-specificissuesofend-of-lifecare,focusingonpatientsoptingforconservativekidneymanagementandthosedeterioratingdespitereceivingdialysis.
NHSKidneyCarehasbeenworkingcloselywiththeDepartmentofHealth,andanEndofLifeCareforAdvancedKidneyDiseaseProjectBoardhasbeenestablishedtosupporttheNHStofollowrecommendationsfromtheFramework,andtosupporttheimplementationoftheDepartmentofHealth’sEnd�of�Life�Care�Strategyforrenalpatients.
Keyareasinclude:
●● raisingthenationalandlocalprofileofkidneyend-of-lifecare,developinglocalagreementswithcommissionersforconservativekidneymanagementprogrammesandkidneyend-of-lifecareservices
●● trainingfrontlinestafftorecognisethesignsoftheapproachingend-of-lifephaseandhandlingcommunicationwithpatientsandtheirfamilies
●● developmentofcareplansforend-of-lifecare
●● co-ordinationofintegratedcareacrossspecialtiesandacrossprimaryandsecondarycare,andprovisionofcareinallappropriatelocations
●● rapidaccesstocare
●● theuseoftheLiverpoolCarePathwayinthelastdaysoflife
●● involvementandsupportoffamilyandcarers
●● buildingmodelsofcareforlocaluse
●● improvingeducationandtrainingofstaffandcontinuingprofessionaldevelopment.
Measurementofallthesedevelopmentswillbethekeytoensuringthatqualitypersonalcareisgiventoeverypatient.Kidneyunitswillbeencouragedtoparticipateinnationalaudits,andnetworksforresearchinkidneyend-of-lifecarewillbeestablished.
53 www.endoflifecareforadults.nhs.uk/eolc/kidney.htm

8End-of-lifecare
49
The Cause for Concern supportive care register
TherenalteamatListerHospitalinStevenagehasdevelopedaCauseforConcern(CfC)supportivecareregister.Theaimistoidentifyandsupportpatientswhoaredeterioratingdespitedialysis,toofferthemtheopportunitytodiscussfuturecareoptionsandtofacilitatecollaborativecareplanning.Communicationbetweenthepatientandrenal,primarycareandpalliativecareteamsisthekeytoenablingasupportivecareplanthatsupportstheneedsofthepatientandtheirfamily.
Itisamultidisciplinaryteamapproach,andincludeslinkCfCnursesineachhaemodialysisunit,hometherapiesandthein-patientward.Oncetheoptionshavebeendiscussedandthegoalsofcareestablished,acareplanisdevelopedanddocumented.Regularreviewsarebuiltinthroughoutthepathway.Medicalfactors,includingprognosis,andpracticalandpsychosocialissues,areconsideredanddiscussed.
MrsAwasontheCfCsupportivecareregisterfor13monthspriortotheendofherlife.Shehadbeenonthehaemodialysisprogrammeforsixyearsatthetimeoftheinitialdiscussionandhadexperiencedmultiplein-patientadmissionsforvariousproblems,includingissuesrelatingtohaemodialysisaccess.CfCwasinitiatedasaftereachadmissionoracuteevent,itwasnotedthatshedidnotregainherpreviousbase-linefunctioning.Shehadagoodnetworkoffamilyandprofessionalsocialcareinthecommunity.
Themedicalprognosis,herexpectationsandgoalsofcarewerediscussedwithherandherhusbandinasensitiveandrealisticmanner.Shewelcomedthediscussionsandparticipatedfully.Hercareplanwasimplementedanddocumentedandcontactsweremadewiththecommunityteams.Atalaterreview,shefeltthatherqualityoflifehadimproved.Asthisimpactedonhergoalsofcare,changesweremadetohercareplan.Allchangeswerecommunicatedinternallyaswellastothecommunityteamsinvolved.
Sometimelater,hermedicalconditiondeteriorated.Shereceivedend-of-lifecaresupportasagreed,andherhusbandwassupportedbytheteam,includingbereavementsupport.
SummaryItishardtopredicthowquicklyCKDwillprogress,especiallywhencomplicatedbyco-existingillnessandoldage.Thechallengeremainsinensuringthatpatientsandtheirfamiliesareinvolvedinalldecisionsaboutoptionsformedicationandtreatment,andthatthesearerecordedinpersonalcareplans.Keyelementsincludetimelyrecognitionthattheend-of-lifephaseisapproaching;sensitivecommunicationwithpatientsandcarers;andjoined-upplanningandeffectivemulti-professionalworkingacrossboundarieslinkingkidneycare,primarycare,communitycareandpalliativecareservices.

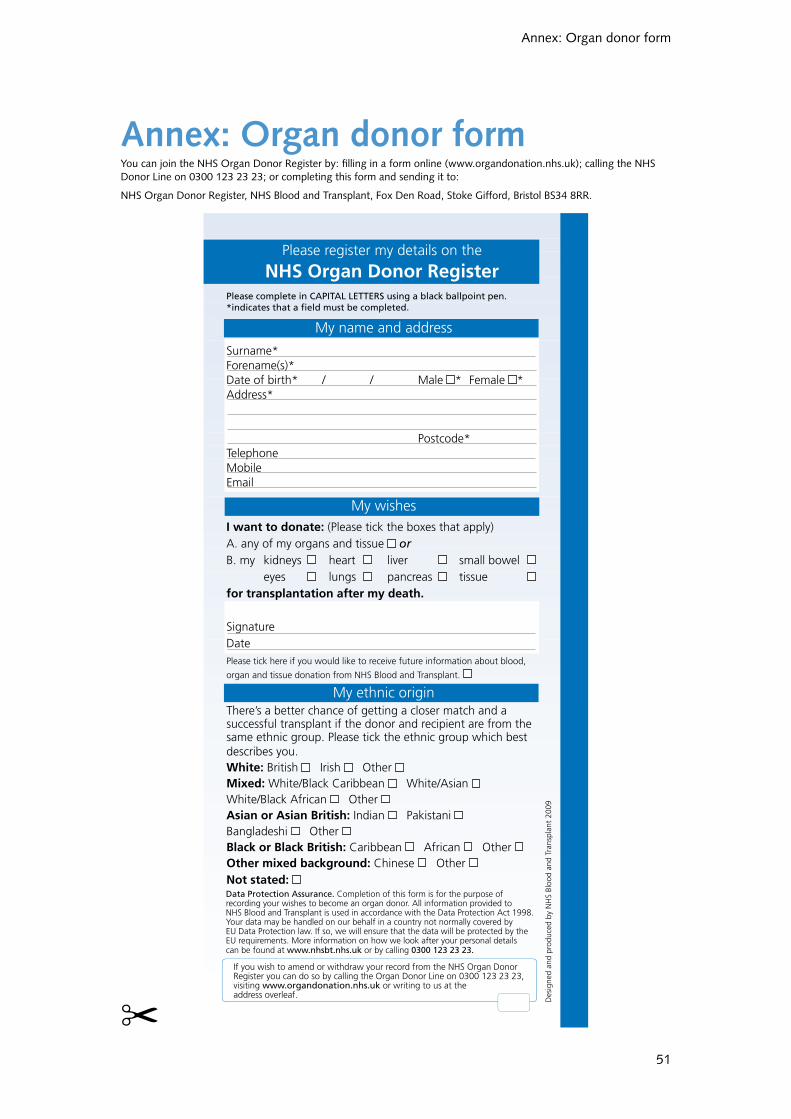
51
Annex:Organdonorform
Please complete in CAPITAL LETTERS using a black ballpoint pen.*indicates that a field must be completed.
My name and address
Surname* Forename(s)* Date of birth* / / Male * Female *Address*
Postcode*Telephone Mobile Email
My wishesI want to donate: (Please tick the boxes that apply)A. any of my organs and tissue orB. my kidneys heart liver small bowel eyes lungs pancreas tissue for transplantation after my death.
SignatureDatePlease tick here if you would like to receive future information about blood,
organ and tissue donation from NHS Blood and Transplant.
My ethnic origin There’s a better chance of getting a closer match and a successful transplant if the donor and recipient are from the same ethnic group. Please tick the ethnic group which best describes you.White: British Irish Other Mixed: White/Black Caribbean White/Asian White/Black African Other Asian or Asian British: Indian Pakistani Bangladeshi Other Black or Black British: Caribbean African Other Other mixed background: Chinese Other Not stated:
Please register my details on the
NHS Organ Donor Register
Des
igne
d an
d pr
oduc
ed b
y N
HS
Bloo
d an
d Tr
ansp
lant
200
9
Data Protection Assurance. Completion of this form is for the purpose of recording your wishes to become an organ donor. All information provided to NHS Blood and Transplant is used in accordance with the Data Protection Act 1998. Your data may be handled on our behalf in a country not normally covered by EU Data Protection law. If so, we will ensure that the data will be protected by the EU requirements. More information on how we look after your personal details can be found at www.nhsbt.nhs.uk or by calling 0300 123 23 23.
If you wish to amend or withdraw your record from the NHS Organ Donor Register you can do so by calling the Organ Donor Line on 0300 123 23 23, visiting www.organdonation.nhs.uk or writing to us at theaddress overleaf.
Annex: Organ donor formYoucanjointheNHSOrganDonorRegisterby:fillinginaformonline(www.organdonation.nhs.uk);callingtheNHSDonorLineon03001232323;orcompletingthisformandsendingitto:
NHSOrganDonorRegister,NHSBloodandTransplant,FoxDenRoad,StokeGifford,BristolBS348RR.
✂


©Crowncopyright2009
2988741p500Dec09(PCL)
ProducedbyCOIfortheDepartmentofHealth
FirstpublishedDecember2009
www.dh.gov.uk/publications