abnormal cerebral asymmetry and schizophrenia in a subject with klinefelter’s syndrome (xxy)
TRANSCRIPT
CASE REPORT
Abnormal Cerebral Asymmetry and Schizophrenia in aSubject with Klinefelter’s Syndrome (XXY)
Michael M. Warwick, Stephen M. Lawrie, Allan Beveridge, and Eve C. Johnstone
Background: A high incidence of schizophrenia has beenreported in individuals with sex chromosome aneuploides(SCAs), and extra-X aneuploidy appears to adverselyaffect neurodevelopment. We previously examined neuro-development in SCA subjects with structural magneticresonance imaging (MRI) of the brain. We present an XXYsubject who subsequently developed schizophrenia. Fur-ther examination of the MRI data was undertaken.
Methods: Graphs of MRI-determined regional brain towhole brain volume proportions and cerebral asymmetryindexes were generated for Klinefelter (n � 10) and malecontrol subjects (n � 25) to allow inter-individual compar-isons.
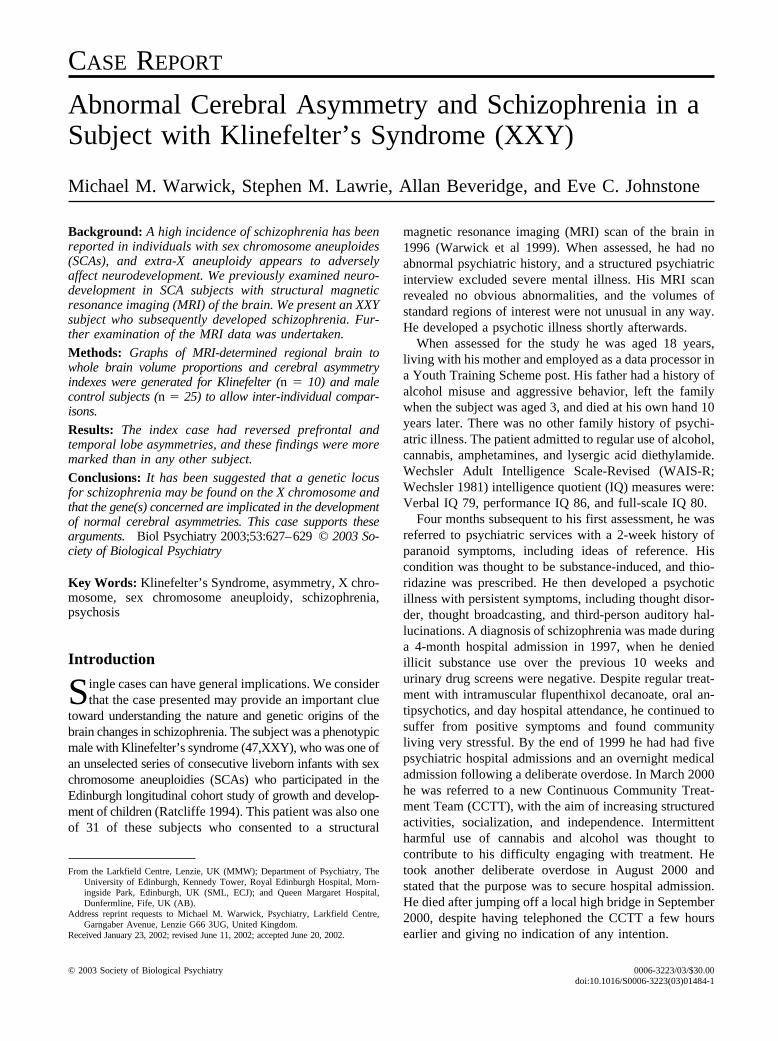
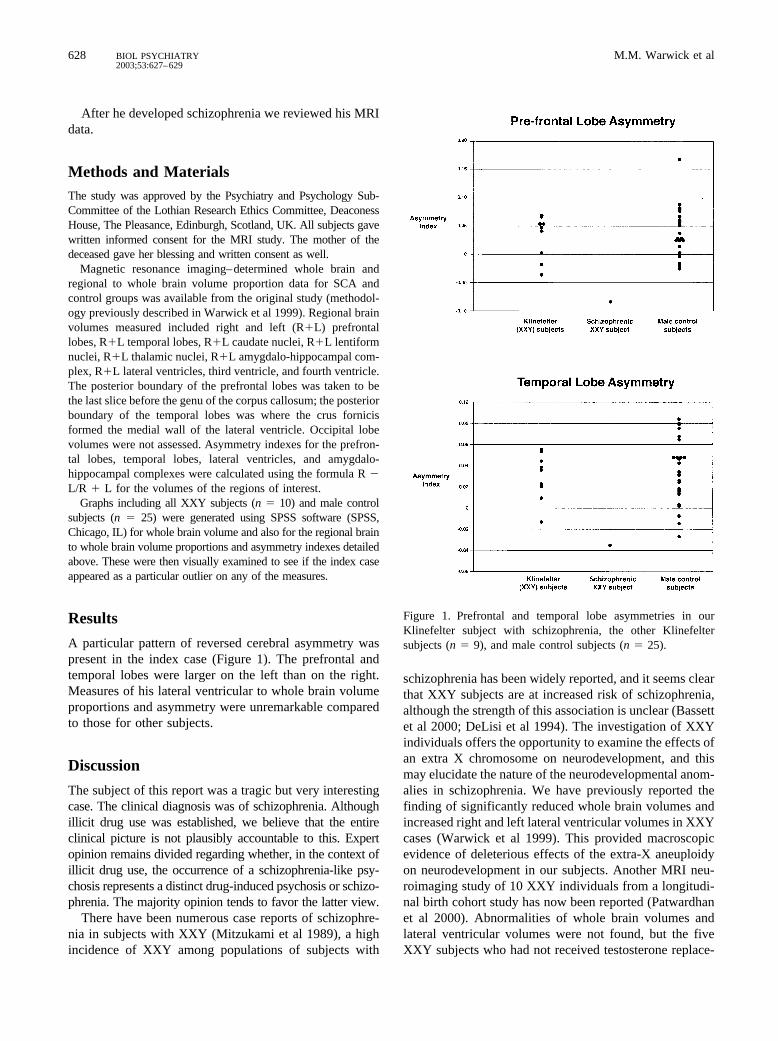
Results: The index case had reversed prefrontal andtemporal lobe asymmetries, and these findings were moremarked than in any other subject.
Conclusions: It has been suggested that a genetic locusfor schizophrenia may be found on the X chromosome andthat the gene(s) concerned are implicated in the developmentof normal cerebral asymmetries. This case supports thesearguments. Biol Psychiatry 2003;53:627–629 © 2003 So-ciety of Biological Psychiatry
Key Words: Klinefelter’s Syndrome, asymmetry, X chro-mosome, sex chromosome aneuploidy, schizophrenia,psychosis
Introduction
Single cases can have general implications. We considerthat the case presented may provide an important clue
toward understanding the nature and genetic origins of thebrain changes in schizophrenia. The subject was a phenotypicmale with Klinefelter’s syndrome (47,XXY), who was one ofan unselected series of consecutive liveborn infants with sexchromosome aneuploidies (SCAs) who participated in theEdinburgh longitudinal cohort study of growth and develop-ment of children (Ratcliffe 1994). This patient was also oneof 31 of these subjects who consented to a structural
magnetic resonance imaging (MRI) scan of the brain in1996 (Warwick et al 1999). When assessed, he had noabnormal psychiatric history, and a structured psychiatricinterview excluded severe mental illness. His MRI scanrevealed no obvious abnormalities, and the volumes ofstandard regions of interest were not unusual in any way.He developed a psychotic illness shortly afterwards.
When assessed for the study he was aged 18 years,living with his mother and employed as a data processor ina Youth Training Scheme post. His father had a history ofalcohol misuse and aggressive behavior, left the familywhen the subject was aged 3, and died at his own hand 10years later. There was no other family history of psychi-atric illness. The patient admitted to regular use of alcohol,cannabis, amphetamines, and lysergic acid diethylamide.Wechsler Adult Intelligence Scale-Revised (WAIS-R;Wechsler 1981) intelligence quotient (IQ) measures were:Verbal IQ 79, performance IQ 86, and full-scale IQ 80.
Four months subsequent to his first assessment, he wasreferred to psychiatric services with a 2-week history ofparanoid symptoms, including ideas of reference. Hiscondition was thought to be substance-induced, and thio-ridazine was prescribed. He then developed a psychoticillness with persistent symptoms, including thought disor-der, thought broadcasting, and third-person auditory hal-lucinations. A diagnosis of schizophrenia was made duringa 4-month hospital admission in 1997, when he deniedillicit substance use over the previous 10 weeks andurinary drug screens were negative. Despite regular treat-ment with intramuscular flupenthixol decanoate, oral an-tipsychotics, and day hospital attendance, he continued tosuffer from positive symptoms and found communityliving very stressful. By the end of 1999 he had had fivepsychiatric hospital admissions and an overnight medicaladmission following a deliberate overdose. In March 2000he was referred to a new Continuous Community Treat-ment Team (CCTT), with the aim of increasing structuredactivities, socialization, and independence. Intermittentharmful use of cannabis and alcohol was thought tocontribute to his difficulty engaging with treatment. Hetook another deliberate overdose in August 2000 andstated that the purpose was to secure hospital admission.He died after jumping off a local high bridge in September2000, despite having telephoned the CCTT a few hoursearlier and giving no indication of any intention.
From the Larkfield Centre, Lenzie, UK (MMW); Department of Psychiatry, TheUniversity of Edinburgh, Kennedy Tower, Royal Edinburgh Hospital, Morn-ingside Park, Edinburgh, UK (SML, ECJ); and Queen Margaret Hospital,Dunfermline, Fife, UK (AB).
Address reprint requests to Michael M. Warwick, Psychiatry, Larkfield Centre,Garngaber Avenue, Lenzie G66 3UG, United Kingdom.
Received January 23, 2002; revised June 11, 2002; accepted June 20, 2002.
© 2003 Society of Biological Psychiatry 0006-3223/03/$30.00doi:10.1016/S0006-3223(03)01484-1
After he developed schizophrenia we reviewed his MRIdata.
Methods and MaterialsThe study was approved by the Psychiatry and Psychology Sub-Committee of the Lothian Research Ethics Committee, DeaconessHouse, The Pleasance, Edinburgh, Scotland, UK. All subjects gavewritten informed consent for the MRI study. The mother of thedeceased gave her blessing and written consent as well.
Magnetic resonance imaging–determined whole brain andregional to whole brain volume proportion data for SCA andcontrol groups was available from the original study (methodol-ogy previously described in Warwick et al 1999). Regional brainvolumes measured included right and left (R�L) prefrontallobes, R�L temporal lobes, R�L caudate nuclei, R�L lentiformnuclei, R�L thalamic nuclei, R�L amygdalo-hippocampal com-plex, R�L lateral ventricles, third ventricle, and fourth ventricle.The posterior boundary of the prefrontal lobes was taken to bethe last slice before the genu of the corpus callosum; the posteriorboundary of the temporal lobes was where the crus fornicisformed the medial wall of the lateral ventricle. Occipital lobevolumes were not assessed. Asymmetry indexes for the prefron-tal lobes, temporal lobes, lateral ventricles, and amygdalo-hippocampal complexes were calculated using the formula R �L/R � L for the volumes of the regions of interest.
Graphs including all XXY subjects (n � 10) and male controlsubjects (n � 25) were generated using SPSS software (SPSS,Chicago, IL) for whole brain volume and also for the regional brainto whole brain volume proportions and asymmetry indexes detailedabove. These were then visually examined to see if the index caseappeared as a particular outlier on any of the measures.
Results
A particular pattern of reversed cerebral asymmetry waspresent in the index case (Figure 1). The prefrontal andtemporal lobes were larger on the left than on the right.Measures of his lateral ventricular to whole brain volumeproportions and asymmetry were unremarkable comparedto those for other subjects.
Discussion
The subject of this report was a tragic but very interestingcase. The clinical diagnosis was of schizophrenia. Althoughillicit drug use was established, we believe that the entireclinical picture is not plausibly accountable to this. Expertopinion remains divided regarding whether, in the context ofillicit drug use, the occurrence of a schizophrenia-like psy-chosis represents a distinct drug-induced psychosis or schizo-phrenia. The majority opinion tends to favor the latter view.
There have been numerous case reports of schizophre-nia in subjects with XXY (Mitzukami et al 1989), a highincidence of XXY among populations of subjects with
schizophrenia has been widely reported, and it seems clearthat XXY subjects are at increased risk of schizophrenia,although the strength of this association is unclear (Bassettet al 2000; DeLisi et al 1994). The investigation of XXYindividuals offers the opportunity to examine the effects ofan extra X chromosome on neurodevelopment, and thismay elucidate the nature of the neurodevelopmental anom-alies in schizophrenia. We have previously reported thefinding of significantly reduced whole brain volumes andincreased right and left lateral ventricular volumes in XXYcases (Warwick et al 1999). This provided macroscopicevidence of deleterious effects of the extra-X aneuploidyon neurodevelopment in our subjects. Another MRI neu-roimaging study of 10 XXY individuals from a longitudi-nal birth cohort study has now been reported (Patwardhanet al 2000). Abnormalities of whole brain volumes andlateral ventricular volumes were not found, but the fiveXXY subjects who had not received testosterone replace-
Figure 1. Prefrontal and temporal lobe asymmetries in ourKlinefelter subject with schizophrenia, the other Klinefeltersubjects (n � 9), and male control subjects (n � 25).
628 M.M. Warwick et alBIOL PSYCHIATRY2003;53:627–629

ment showed significant reduction in left temporal lobegray matter tissue compared to matched control subjects.
The normal pattern of cerebral asymmetry in right-handed males (such as our case) is that prefrontal andtemporal lobe volumes are greater on the right than theleft, and left occipital lobe volumes are greater than right.This is known as “cerebral torque.” The extent of thereversal of this expected pattern in the prefrontal andtemporal lobes of our case was very striking. Only oneother XXY subject showed reversal of both prefrontal andtemporal lobe asymmetries. He is left handed, and it hasbeen reported that normal brain asymmetries occur lessfrequently in left-handed individuals (Luchins et al 1982).
Crow (1990) has suggested that schizophrenia may beattributable to an abnormality in cerebral lateralization,possibly involving abnormal expression of a cerebraldominance gene on the X chromosome. He has reporteddata consistent with this hypothesis, including an XXphenotypic male with psychosis with the chromosomalbreakpoint on the Y in the Homo sapiens–specific Yp11.2region of homology with Xq21.3, a region linked todetermination of cerebral asymmetry (Laval et al 1998).The chromosomal breakpoint on the X in that individualhas now been established to be within the X-Y homolo-gous pseudoautosomal region 1 (Ross et al 2001).
Our case provides clinical and macroscopic evidencethat abnormal expression of X-linked genes may beassociated with abnormal development of cerebral asym-metries and psychosis.
MMW was employed as a Wellcome Research Registrar (monies forsalary provided by the Wellcome Trust).
We express our gratitude posthumously to the gentleman who is thesubject of this report and also to his mother for their co-operation with thestudy. We also thank Dr. Paul Cavanagh and Dr. Shirley Ratcliffe.
ReferencesBassett AS, Chow EW, Weksberg R (2000): Chromosomal
abnormalities and schizophrenia. Am J Med Genet 97:45–51.
Crow TJ (1990): Temporal lobe asymmetries as the key to theetiology of schizophrenia [review]. Schizophr Bull 16:433–443.
DeLisi LE, Friedrich U, Wahlstrom J, Boccio-Smith A, ForsmanA, Eklund K, et al (1994): Schizophrenia and sex chromo-some anomalies [review]. Schizophr Bull 20:495–505.
Laval SH, Dann JC, Butler RJ, Loftus J, Rue J, Leask SJ, et al(1998): Evidence for linkage to psychosis and cerebralasymmetry (relative hand skill) on the X chromosome. Am JMed Genet 81:420–427.
Luchins DJ, Weinberger DR, Wyatt RJ (1982): Schizophreniaand cerebral asymmetry detected by computed tomography.Am J Psychiatry 139:753–757.
Mizukami K, Koizumi J, Shiraishi H, Nagase S (1989): Aclinical case of Klinefelter’s syndrome with various psychi-atric symptoms. Jpn J Psychiatry Neurol 43:639–644.
Patwardhan AJ, Eliez S, Bender B, Linden MG, Reiss AL(2000): Brain morphology in Klinefelter syndrome Extra Xchromosome and testosterone supplementation. Neurology54:2218–2223.
Ratcliffe SG (1994): The psychological and psychiatric conse-quences of sex chromosome abnormalities in children, basedon population studies. In: Poustka F, editor. Basic Ap-proaches to Genetic and Molecularbiological DevelopmentalPsychiatry. Berlin: Quintessenz, pp 99–122.
Ross NLJ, Yang J, Sargent CA, Boucher CA, Nanko S, WadekarR, et al (2001): Triplication of several PAR1 genes and partof the Homo sapiens specific Yp11.2/Xq21.3 region ofhomology in a 46,X,t(X;Y)(p22.33;p11.2) male with schizo-phrenia. J Med Genet 38:710–719.
Warwick MM, Doody GA, Lawrie SM, Kestelman JN, Best JJ,Johnstone EC (1999): Volumetric magnetic resonance imag-ing study of the brain in subjects with sex chromosomeaneuploidies. J Neurol Neurosurg Psychiatry 66:628–632.
Wechsler D (1981): The WAIS-R Manual. New York, NY:Psychological Corporation.
XXY, Schizophrenia, and Reversed Cerebral Asymmetry 629BIOL PSYCHIATRY2003;53:627–629