abdominal “masses” in the infant phillip gordon images by : univ. of iowa virtual children’s...
TRANSCRIPT

Abdominal “Masses” in Abdominal “Masses” in the infantthe infant
Phillip GordonPhillip Gordon
Images by :
Univ. of Iowa Virtual Children’s Hospital Simon C. S. Kao, M.D.Michael P. D'Alessandro, M.D.,Steven J. Fishman, M.D.,Deborah E. Schofield, M.D.
Rainbow Babies & Children's Hospital
Victor Bykov, M.D.Sheila Berlin, M.D.Mufaddal Hashim, M.D.Sheila Berlin, M.D.Melissa Myers, M.D.Carlos Sivit, M.D.Stuart Morrison, M.D.Dayna Weinert, M.D.Alan D. Bortz, M.D.Carlos J. Sivit, M.D.Sheila C. Berlin, M.D. Vincent Keiser, M.D.
New England Journal of Medicine
Case Archives

Common Abdominal “Masses” in the NewbornCommon Abdominal “Masses” in the Newborn
Retroperitoneal Masses 65%
Polycystic kidneys, hydronephrosis, dysplastic kidneys, neoplasms, other
GI “Masses” 25%
Things that cause Obstruction, hepatic masses, other
Genito-sacral 10%
Teratomas, congenital genital anomalies, ovarian cysts, other
“This what I was taught, therefore it is what I will teach to you. However, I know of no convincing evidence that it is actually true or relevant to our current medical era.”
PVG

Retroperitoneal “Masses” in Retroperitoneal “Masses” in the infantthe infant

Presentation:
A term male infant is noted to have a firm and full right flank region during the newborn exam. The examiner is unable to palpate the pole of the kidney on the right, but does so easily on the left. The child’s eyes seem a little dilated and there is a mild hypospadias, but the remainder of the exam is otherwise normal.
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 15.
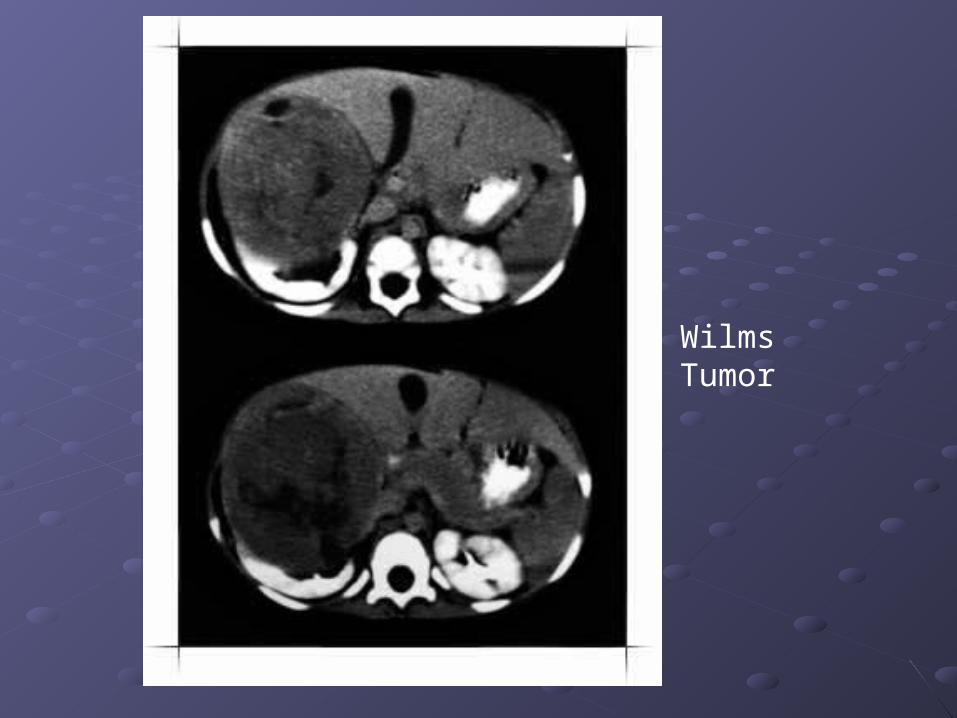
Wilms Tumor
Presentation:
A term male infant is noted to have a large and nodular mass in the right flank region during the newborn exam that ballots as if it were a kidney. The left kidney is normal upon palpation.There is a small hemangioma on the infant’s nape. The remainder of the exam is otherwise normal.
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 15.

Hydronephrosis secondary to ureteropelvic junction obstruction (also called a multicystic dysplastic kidney)
Presentation:
A 7 month old male infant is noted to have unusual weight gain, pustular acne, pubic hair and a palpable mass on the right flank.
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 15. LFTs are high normal.
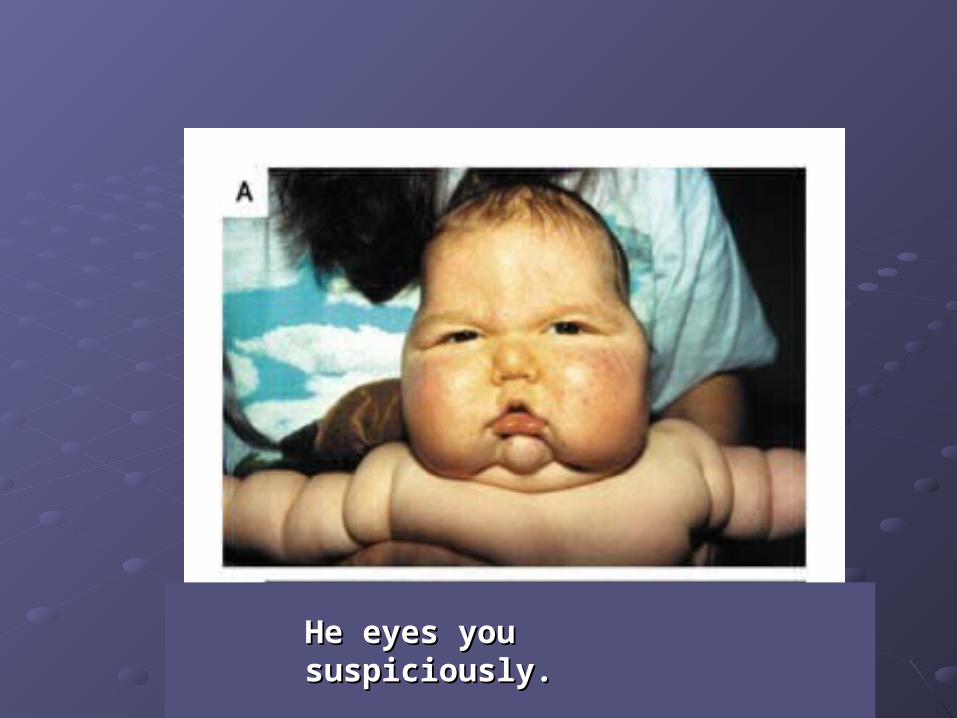
He eyes you suspiciously.He eyes you suspiciously.
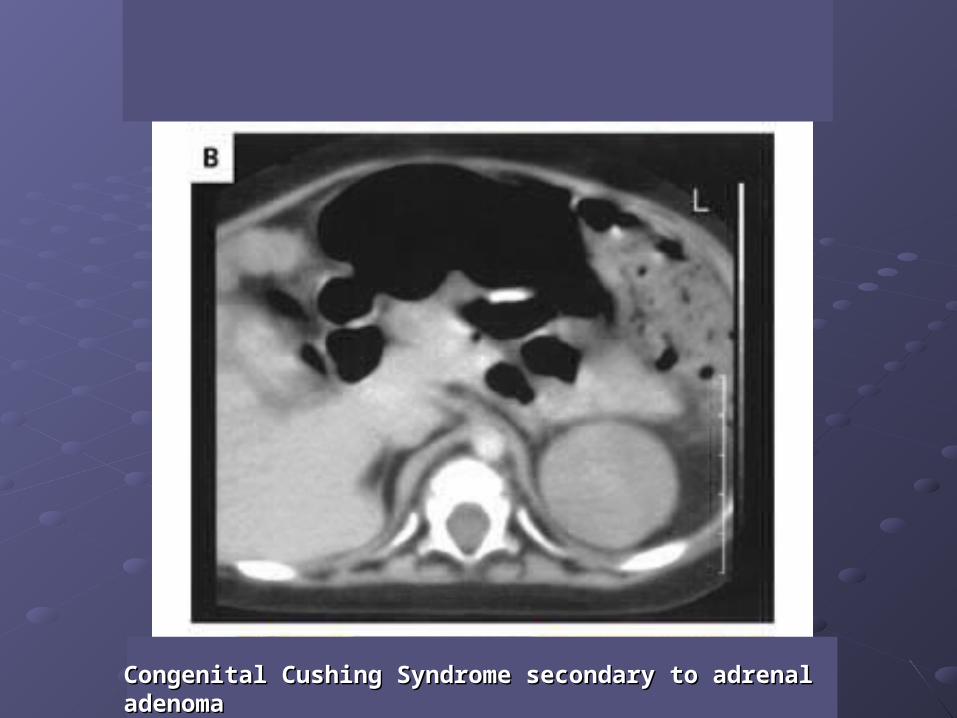
Congenital Cushing Syndrome secondary to adrenal adenomaCongenital Cushing Syndrome secondary to adrenal adenoma
Abdominal “Masses” that fill Abdominal “Masses” that fill the entire abdominal cavitythe entire abdominal cavity
Presentation:
A term male infant is noted to be edematous, tachypneic and to have a gallop with a HR of 160 bpm. Perfusion is sluggish but blood pressures and saturations are normal. The abdomen is distended and tense. Bowel sounds are present. The kidneys are palpable.The liver is large. There is a large subdermal hemangioma on the infant’s nape and smaller one on the left eyelid. The remainder of the exam is deferred because of the need to resuscitate (the infant becomes apneic during the exam).
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 15. LFTs are moderately elevated.

Infantile Hemangioendothelioma
Presentation:
An SGA term male infant is found to be in respiratory distress secondary to an abdomen that is extremely distended and tense. Bowel sounds are absent. The kidneys are not palpable. The remainder of the exam has to be deferred because of the need to resuscitate (the infant becomes apneic during the exam).
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 15. LFTs are moderately elevated.
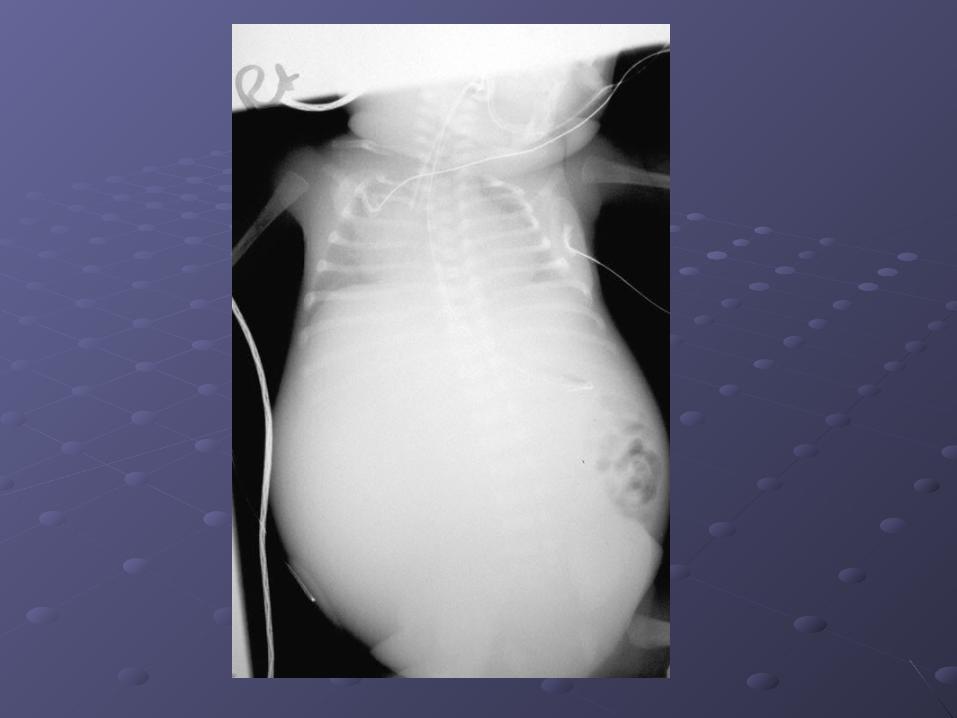
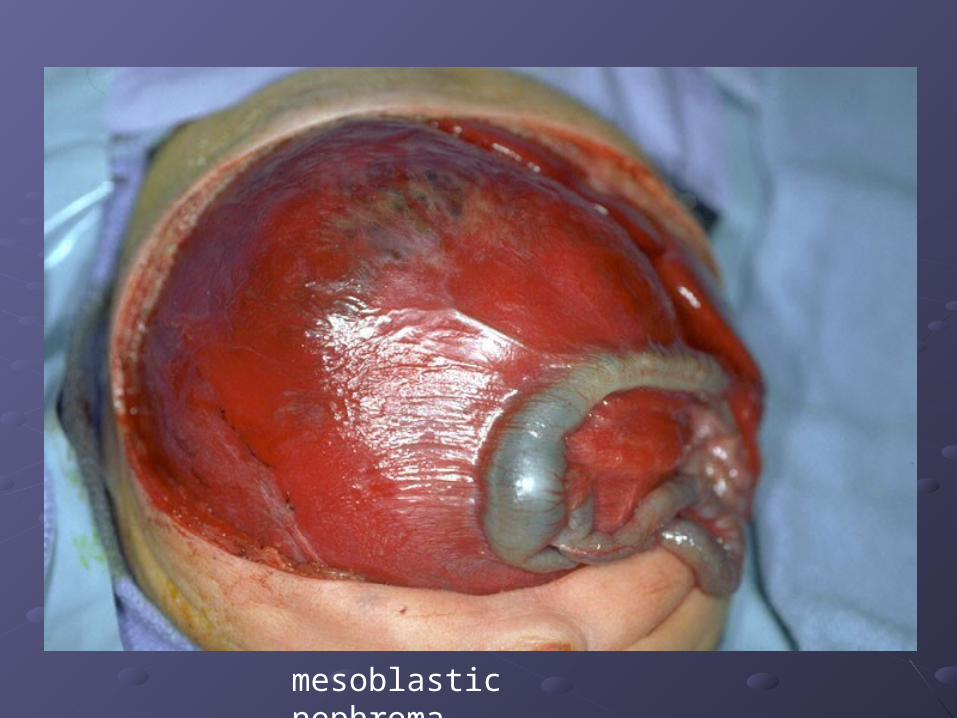
mesoblastic nephroma

Presentation:
An LGA 34 week gestation male infant of a diabetic mother is found to have an abdomen that is distended and tense on the 3rd day of life. Bowel sounds are present. The kidneys are palpable. The infant has been feeding sluggishly. The liver is difficult to palpitate due to the distention. Perfusion is good. Color is good. The child has not stooled.
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 32. LFTs are normal.
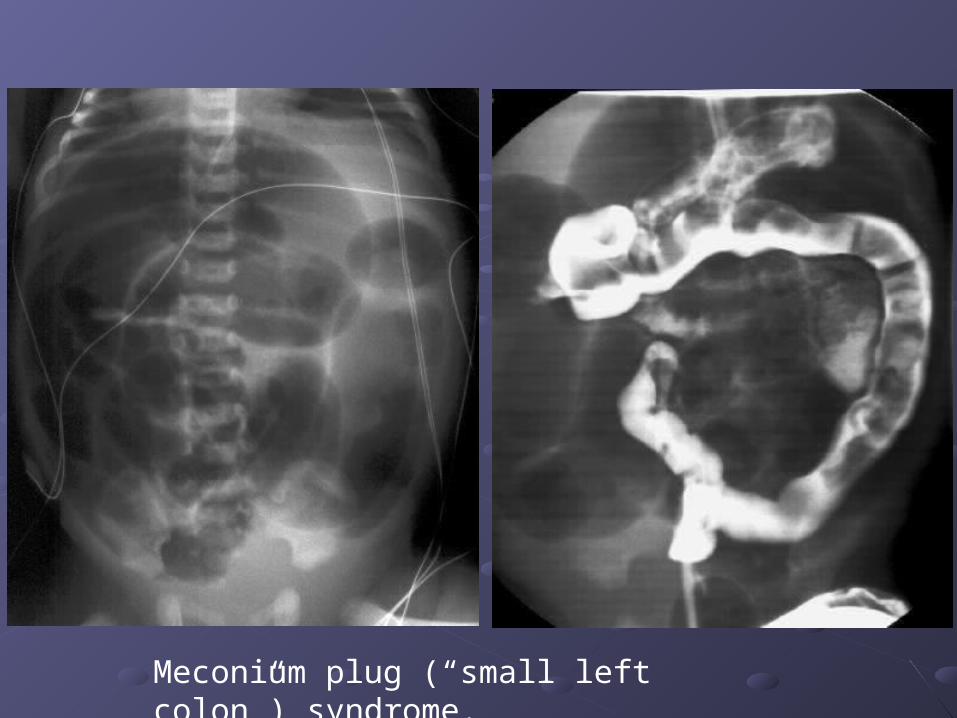
Meconium plug (“small left colon”) syndrome.
Midline Abdominal “Masses” Midline Abdominal “Masses” in the newborn in the newborn
Presentation:
An SGA 36 week gestation female infant of a mother with an anxiety disorder is born at an outside hospital and noted to have a distended abdomen at birth. The infant eats well but has had nothing but black liquid stools over the 1st 3 days of life. A KUB was read by an adult radiologist, who reported a radio-opaque, mid-line mass in the lower abdomen. The transferring doctor reports that, other than the distended abdomen, the child’s exam is normal.
Labs:
An electrolyte panel is notable for a serum creatinine of 0.9 and a BUN of 15. LFTs are normal.


Cloacal Malformation / Caudal Regression Syndrome
Presentation:
A term female infant of a mother with an anxiety disorder is born at an outside hospital and noted to have an intermittently distended abdomen (thought to be related to agitation during unsuccessful attempts at breast feeding). 3 weeks later, the now formula fed infant eats well but has had alternating diarrhea and constipation. The transferring ER doctor reports that, other than the persistently distended abdomen, the child’s exam is normal.
Labs:
An electrolyte panel is notable for a serum creatinine of 0.8 and a BUN of 42. LFTs are normal.

duplication cyst of ileocecal junction
LUQ Abdominal “Masses” in LUQ Abdominal “Masses” in the newborn the newborn
(3 Cases with the same presentation)(3 Cases with the same presentation)
Presentation (for the next 3 cases):
A term female is noted to have a distended abdomen with a large, tender viscous mass in the LUQ at birth. Other pertinent findings include persistent agitation, skin mottling, a cap refill of 2 seconds and “projectile” vomiting during the first feed. The infant has a worried look on its face.
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 18.

Jejunal Web

Malrotation and Midgut Volvulus

Duodenal Atresia

Sacral-coccygeal “Masses” in Sacral-coccygeal “Masses” in the newborn the newborn
Presentation:
A term infant is born by c-section due to evidence of a sacral mass on ultrasound. On initial exam, a lobular, fully epithelialized, doughy protrusion is attached to the sacral-lumbar region of an otherwise normal infant. The infant is tachycardic (200 bpms) but hemodynamically stable. An x-ray reveals no bone or dental elements within the external portions of the mass.
Labs:
An electrolyte panel is notable for a serum creatinine of 1.1 and a BUN of 18.
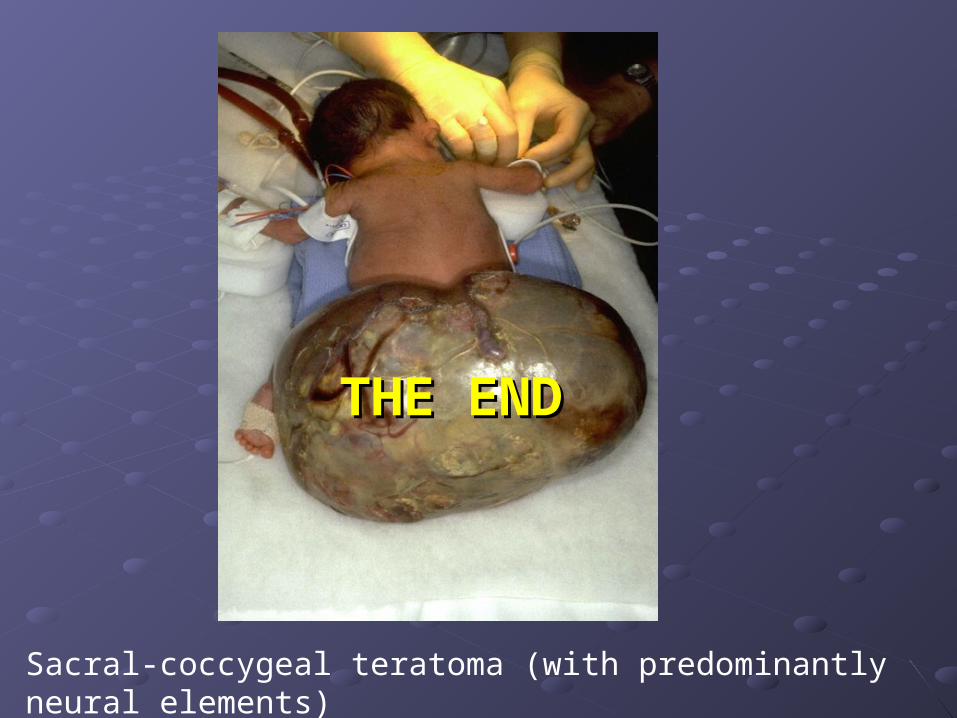
Sacral-coccygeal teratoma (with predominantly neural elements)
THE ENDTHE END