a3 - symptom management
TRANSCRIPT

Click to edit Master title style
• Click to edit Master text stylesImproving bowel management in a
specialist palliative care service
A clinical project
Emilie Clark - Donny Trust Specialist Nurse Trainee 2014

Click to edit Master title style
• Click to edit Master text styles
Background
• Perceived gap in clinical
documentation
• Transition period

Click to edit Master title style
• Click to edit Master text styles
Importance of effective bowel management
Constipation is highly prevalent at the end-
of-life.
• Distressing and uncomfortable. Effective management may alleviate distress
(MacLeod, Vella-Brincat & Macleod, 2012).
• 70% of patients receiving palliative care experience constipation during admission to a specialist inpatient unit. (Clark, Smith & Currow, 2012)

Click to edit Master title style
• Click to edit Master text styles
Constipation
“It was all I thought about, all the time. I never want to experience that again”
Hospice Patient (2013)

Click to edit Master title style
• Click to edit Master text styles
Bowel Care Guidelines
PRINCIPLE Maintenance of palliative
care patient’s own individual bowel
regime and prevention of discomfort
and complications due to
constipation will be achieved by full
assessment, attendance to Bowel Care
Plan and acknowledgement of
the changing condition of the patient.Arohanui Hospice (2013)

Click to edit Master title style
• Click to edit Master text styles
Method
1. Was there a nursing bowel assessment completed on admission?
2. Does the patient have an individualised bowel care plan?
3. Are laxatives prescribed regularly for the patient if they are prescribed
opiates?
4. Was the bowel status of the patient recorded on each shift? Including:
–Frequency
–Number of days since bowels last opened
–Bristol Stool Chart
–Quality
–Quantity
–Abnormalities present (if applicable)
5. If interventions were used, was effectiveness documented?

Click to edit Master title style
• Click to edit Master text styles
Audit 1 - ResultsAdmission - Was there a bowel assessment on admission?
All
Individualised bowel care plan
7/10 had no plan
2/10 on paraplegic bowel regime
1 had a care plan from PNH – new
colostomy
Laxatives - are the prescribed regularly for those patient with opiates All
If interventions were used, was effectiveness documentedYes - 4/10 had interventions
Recording’s
Minimal recordings of quality using Bristol Stool Chart
Often descriptive wording used eg.
Large, soft.
Erratic documentation - no
structure, sometimes recorded very
well but others no recording at all.
? - used frequently.
Click to edit Master title style
• Click to edit Master text styles
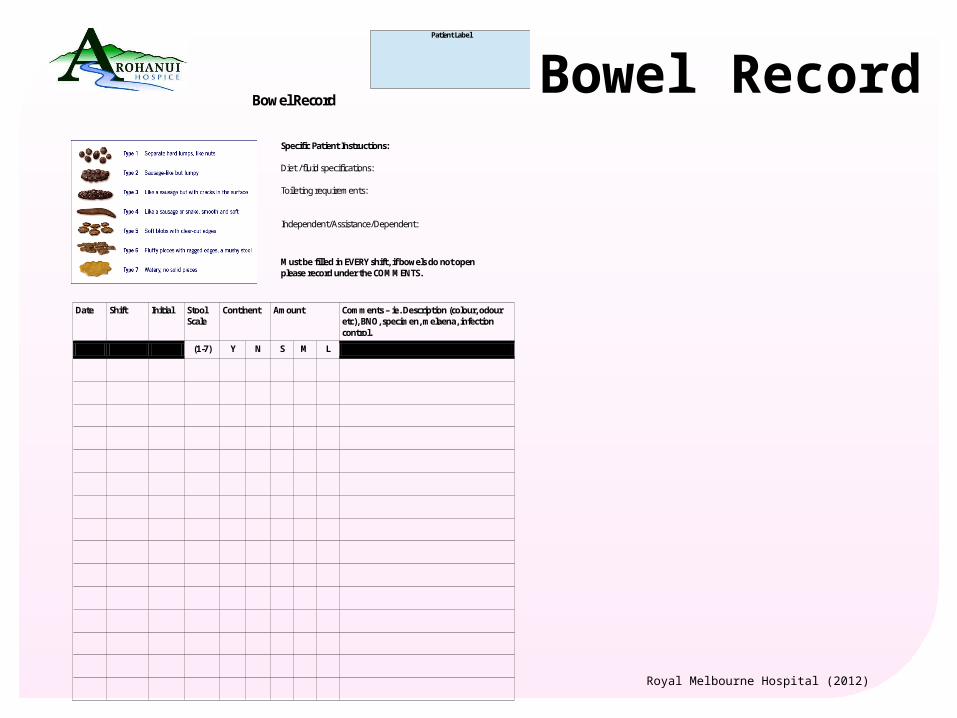
Bowel RecordBowel Record
Date Shift Initial Stool Scale
Continent Amount Comments – ie. Description (colour, odour etc), BNO, specimen, melaena, infection control.
(1-7) Y N S M L
Patient Label
Specific Patient Instructions: Diet /fluid specifications: Toileting requirements: Independent/Assistance/Dependent:
Must be filled in EVERY shift, if bowels do not open please record under the COMMENTS.
Royal Melbourne Hospital (2012)

Click to edit Master title style
• Click to edit Master text styles
Feedback
• Do you use the bowel chart on a
regular basis?
• Do you find it simple and easy to use?
• Do you feel the form adequately captures the patient’s bowel pattern whilst a patient in the IPU?

Click to edit Master title style
• Click to edit Master text styles“The bowel chart is great and a vast improvement on how we were recording bowel routines before.”
“It’s good to have the scale on the chart. At least then we are all reading from the same page.”
“...it’s only as good as the recording and staff need to be responsible.”

Click to edit Master title style
• Click to edit Master text styles
Audit 2 - ResultsAdmission - Was there a bowel assessment on admission? All
Individualised bowel care plan
9/10 had no plan
1 had a care plan from the community
palliative care team
Laxatives - are the prescribed regularly for those patient with opiates Yes
If interventions were used, was effectiveness documented None had interventions
Recording’s
Perfect documentation on patient with a care plan
"Unknown" used frequently in regards to
quality of stool.
Not recorded on all shifts majority of the time
- exception is the patient with
care plan and a patient admitted with a
bowel obstruction.

Click to edit Master title style
• Click to edit Master text styles
Findings
1. Change
2. Care plans
3. Autonomy and self-recording

Click to edit Master title style
• Click to edit Master text styles
Implications for practice
• Further development
• Care plans

Click to edit Master title style
• Click to edit Master text styles
Objective or Subjective?
“Different things to different people.” (Andrews & Morgan, 2013)
“Despite the attention of staff on quantifying the frequency or character of the stools, ultimately constipation is a highly subjective sensation”
(Clark & Currow, 2014).

Click to edit Master title style
• Click to edit Master text styles
Implications for practice
• Education
• Further research

Click to edit Master title style
• Click to edit Master text styles
Any questions?
THANK YOU

Click to edit Master title style
• Click to edit Master text styles
References
Arohanui Hospice. (2013). Guidelines service continuum clinical procedures gastro-intestinal bowel care guidelines. Palmerston North: Arohanui Hospice.
Andrews, A., & Morgan, G. (2013). Constipation in palliative care: Treatment options and considerations for individual patient management. International Journal of Palliative Nursing, 19(6), 266-273. Retrieved from ScienceDirect database.
Clark, K., Smith, J.M., & Currow, D.C. (2012). The prevelance of bowel problems reported in a palliative care population. Journal of Pain and Symptom Management, 43(6), 993-1000. Retrieved from ScienceDirect database.
DeRoo, M.L., Leemans, K., Claessan, S.J.J., Cohen, J., Pasman, R.W., Deliens, L., & Francke, A.L. (2013). Quality indicators for palliative care: Update of a systematic review. Journal of Pain and Symptom Management, In Press. Retrieved from ScienceDirect database.
Dhingra, L., Shuk, E., Grossman, B., Strada, A., Wald, E., Portenoy, A., Knotkova, H. & Portenoy, R. (2012). A qualitative study to explore psychological distress and illness burden associated with opioid-induced constipation in cancer patients with advanced disease. Palliative Medicine, 27(5), 447-456. Retrieved from ProQuest database.
Hospice New Zealand. (2012). Standards for palliative care: Quality review programme and guide 2012. Retrieved from http://www.hospice.org.nz/HNZ_Standards_Book_Online_-_May_2013(1).pdf.
Kyle, G. (2011). End of life: A need for bowel care guidance. Retrieved from http://www.nursingtimes.net/nursing-practice/specialisms/continence/end-of-life-a-need-for-bowel-care-guidance/5029189.article

Click to edit Master title style
• Click to edit Master text styles
References
MacLeod, R., Vella-Brincat, J., & Macleod, A.D. (2012). The palliative care handbook: Guidelines for clinical management and symptom control. (6th ed.). Retrieved from http://www.hospice.org.nz/cms_show_download.php?id=377.
Royal Melbourne Hospital. (2012). Bowel Chart.