a solution that overcomes the challenges of implementing ... · a solution that overcomes the...
TRANSCRIPT
Exa™ Mammo A Solution that Overcomes the Challenges of Implementing Digital Breast Tomosynthesis
A W H I T E P A P E R
Konica Minolta Healthcare Americas, Inc.
E X A M A M M O | A W H I T E P A P E R
Konica Minolta Healthcare Americas • konicaminolta.com/medicalusa • October 2017
Numerous published studies have shown that digital breast
tomosynthesis (DBT), also referred to as 3D mammography, can
overcome limitations of traditional 2D mammography, enhance
lesion conspicuity, and improve sensitivity and specificity.1-4
Other studies report that adding 3D mammography or ultra-
sound to regular screening mammograms can detect more
cancers in dense breasts.5,6 In the US, nearly 50% of women in
their 40s have dense breasts.7
A 2014 study reported a 41% increase in the detection of invasive
breast cancers and a 29% increase in the detection of all breast
cancers with DBT compared to 2D mammography.8 Another study
found that the rate of recalls was nearly 37% lower among women
who had DBT compared to women who only had conventional
mammography (2D). The benefits of DBT were further reported in
a 2016 study, including a 50% increase in invasive cancer detec-
tion in women with heterogeneously dense breasts.9
With evidence supporting the clinical benefits of DBT, new guide-
lines from the National Comprehensive Cancer Network (NCCN)
recommending that physicians consider tomosynthesis as an
option for their patients’ annual breast cancer screenings and
three new CPT codes for screening and diagnostic DBT, along with
Centers for Medicare and Medicaid (CMS) reimbursement of DBT
for screening in conjunction with 2D mammography, the market
for DBT is expected to continue growing. By 2018, DBT units will
exceed 2D mammography systems in the US and by 2020 the DBT
market value will reach $521B.
While DBT delivers clinical advantages over 2D mammography,
there are workflow and infrastructure challenges to implementing
the technology. Exa™ Mammo from Konica Minolta Healthcare
Americas is designed to overcome the
challenges associated with viewing, read-
ing and reporting DBT exams.
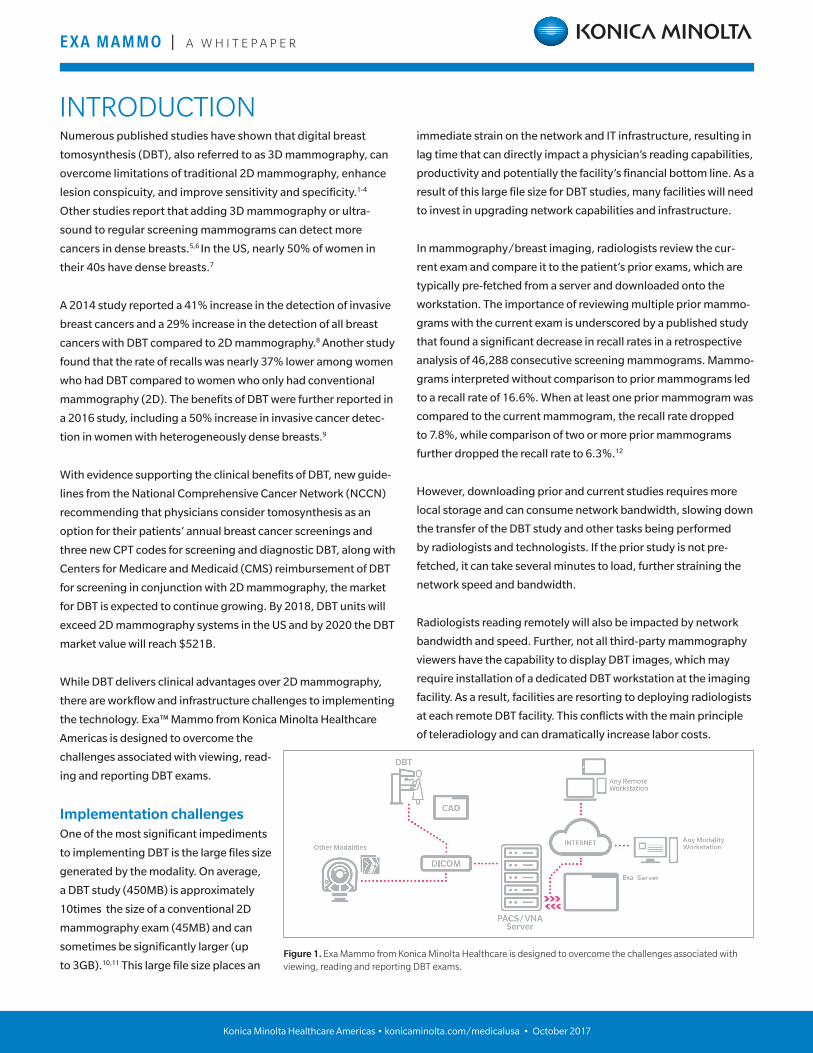
Implementation challenges One of the most significant impediments
to implementing DBT is the large files size
generated by the modality. On average,
a DBT study (450MB) is approximately
10times the size of a conventional 2D
mammography exam (45MB) and can
sometimes be significantly larger (up
to 3GB).10,11 This large file size places an
INTRODUCTION
Figure 1. Exa Mammo from Konica Minolta Healthcare is designed to overcome the challenges associated with viewing, reading and reporting DBT exams.
immediate strain on the network and IT infrastructure, resulting in
lag time that can directly impact a physician’s reading capabilities,
productivity and potentially the facility’s financial bottom line. As a
result of this large file size for DBT studies, many facilities will need
to invest in upgrading network capabilities and infrastructure.
In mammography/breast imaging, radiologists review the cur-
rent exam and compare it to the patient’s prior exams, which are
typically pre-fetched from a server and downloaded onto the
workstation. The importance of reviewing multiple prior mammo-
grams with the current exam is underscored by a published study
that found a significant decrease in recall rates in a retrospective
analysis of 46,288 consecutive screening mammograms. Mammo-
grams interpreted without comparison to prior mammograms led
to a recall rate of 16.6%. When at least one prior mammogram was
compared to the current mammogram, the recall rate dropped
to 7.8%, while comparison of two or more prior mammograms
further dropped the recall rate to 6.3%.12
However, downloading prior and current studies requires more
local storage and can consume network bandwidth, slowing down
the transfer of the DBT study and other tasks being performed
by radiologists and technologists. If the prior study is not pre-
fetched, it can take several minutes to load, further straining the
network speed and bandwidth.
Radiologists reading remotely will also be impacted by network
bandwidth and speed. Further, not all third-party mammography
viewers have the capability to display DBT images, which may
require installation of a dedicated DBT workstation at the imaging
facility. As a result, facilities are resorting to deploying radiologists
at each remote DBT facility. This conflicts with the main principle
of teleradiology and can dramatically increase labor costs.

E X A M A M M O | A W H I T E P A P E R
Konica Minolta Healthcare Americas • konicaminolta.com/medicalusa • October 2017
Cybersecurity Downloading and pre-fetching patient studies onto a workstation
may introduce additional cybersecurity vulnerabilities. A June
2017 report by the US Department of Health and Human Services,
Health Care Industry Cybersecurity Task Force, warned that US
healthcare cybersecurity is in critical condition, citing a “severe
lack of security talent” in the majority of health delivery organiza-
tions. The report also noted that Meaningful Use requirements
may have led to “hyper-connectivity without secure design and
implementation.”13
Twenty-one cybersecurity experts helped compile the report,
which also found that the healthcare industry experienced more
breaches due to cybersecurity than any other industry.11 An
increase in ransomware has only exacerbated this issue, as is
evident by the recent attack on National Health Service (NHS)
hospitals in the United Kingdom that shut down medical care in
16 hospitals and impacted nearly 40 NHS organizations.14,15
Cost and ROI of DBT The cost of a DBT system can vary from just under $400,000 for a
basic system configuration to just over $550,000 for a fully config-
ured solution that may include computer-aided detection (CAD),
a dedicated workstation, contrast-enhanced spectral mammog-
raphy and upright biopsy equipment. By comparison, the average
cost of a FFDM unit is around $275,000.16
Interest in DBT has fueled an increase in the price of digital mam-
mography systems, which can often be upgraded to DBT. Accord-
ing to the latest public data available from the Modern Healthcare/
ECRI Institute Technology Price Index, digital mammography
(likely with a tomosynthesis option) was one of the top 10 most
expensive capital items reported by ECRI Institute members in
November 2016.17 The index also reported a 4.1% increase in the
cost of digital mammography over a 12-month period (November
2015-November 2016).
In 2015, CMS adopted new CPT coding for DBT when used in
conjunction with screening and diagnostic mammography. Coding
changes for DBT were implemented in 2017 to simplify mammog-
raphy codes that were previously separate for FFDM, film mam-
mography, CAD and DBT.18
For both screening and diagnostic DBT, the Medicare reimburse-
ment component is $30.86 for professional (physician) and $25.48
for technical (facility), or $56.34 for both. An imaging site would
recover its initial investment in a basic system configuration
($400,000) after billing for 2,219 DBT exams or in a fully configured
system ($550,000) after billing for 4,881 DBT exams.
DBT with Exa Mammo Considering the cost of DBT and the volume required to recoup
the initial investment before generating income, facilities may
seek solutions that reduce overall expense yet enable remote
reading without requiring extensive upgrades to networks and
infrastructure.
Exa Mammo is a first-of-its-kind Konica Minolta solution that
preserves an existing investment in imaging and information
technology while enhancing radiologists’ efficiency and
productivity. The platform enables the viewing of images from
any modality, including DBT and digital 2D mammograms, from
any workstation* with instant access and zero lag time.
Two key features make Exa Mammo one of a kind. First, with 100%
Diagnostic Zero Footprint (ZFP) technology, the user/facility
never has to install a viewer. It functions on any operating system
or browser, and it is a true diagnostic viewer for any modality,
including DBT. Second, Server-Side Rendering (SSR) allows
immediate access to even the largest file sizes, such as DBT, as well
as priors. SSR eliminates the need to download images or files,
which can reduce radiology-related network traffic by up to 60%.
Further, SSR significantly increases exam opening speed, as all
rendering and processing occurs on the server, not the workstation,
and removes the need to pre-fetch or plan ahead with routing rules.
For cybersecurity, Exa minimizes unwanted exposure to patient
data with no data transferred to or stored on workstations.
By implementing Exa Mammo, facilities can avoid the additional
expense and maintenance of a separate mammography
workstation. It works as a stand-alone solution or supplements an
existing PACS or VNA and enables radiologists to read remotely
from any location. Exa Mammo also offers a customizable
“EXA MAMMO IS A FIRST-OF-ITS-KIND KONICA MINOLTA SOLUTION THAT PRESERVES
AN EXISTING INVESTMENT IN IMAGING AND INFORMATION TECHNOLOGY WHILE ENHANCING RADIOLOGISTS’ EFFICIENCY
AND PRODUCTIVITY.”
E X A M A M M O | A W H I T E P A P E R
Konica Minolta Healthcare Americas • konicaminolta.com/medicalusa • October 2017
mammography workflow engine and
optional voice recognition and report-
creation technologies.
With SSR and ZFP, Exa Mammo is
exceedingly simple to deploy and use
on existing workstations. It integrates
with other interfaces and saves facilities
from expensive IT upgrades when
deploying DBT, while enhancing security
of patient data by never downloading
images or information onto an individual
workstation. For all required (MQSA)
mammography tracking and reporting,
Exa Mammo integrates with third-party
software, such as Penrad, MRS and
Ikonopedia. Through this software,
tracking items such as Bi-Rads assessment
and recommendations, breast density,
calcification and geometry selection, and
biopsy protocol selection are all presented
to the radiologist during reading and
dictation. Each third-party software
meets MQSA standards put forth by the
American College of Radiology.
Conclusion DBT is an evolution in digital
mammography systems, with initial
clinical evidence indicating a higher
cancer detection rate, particularly in
women with dense breasts, and a lower
false-positive recall rate. However, the
large file size of DBT exams presents
implementation challenges and can
place a strain on existing networks and IT
infrastructure. The equipment’s high cost
can further impede a facility’s economic
ability to provide this potentially life-
saving technology to patients.
Exa Mammo from Konica Minolta can
help overcome these limitations with
a cost-effective solution that does not
require any image downloads, dedicated
tomosynthesis workstation or expensive
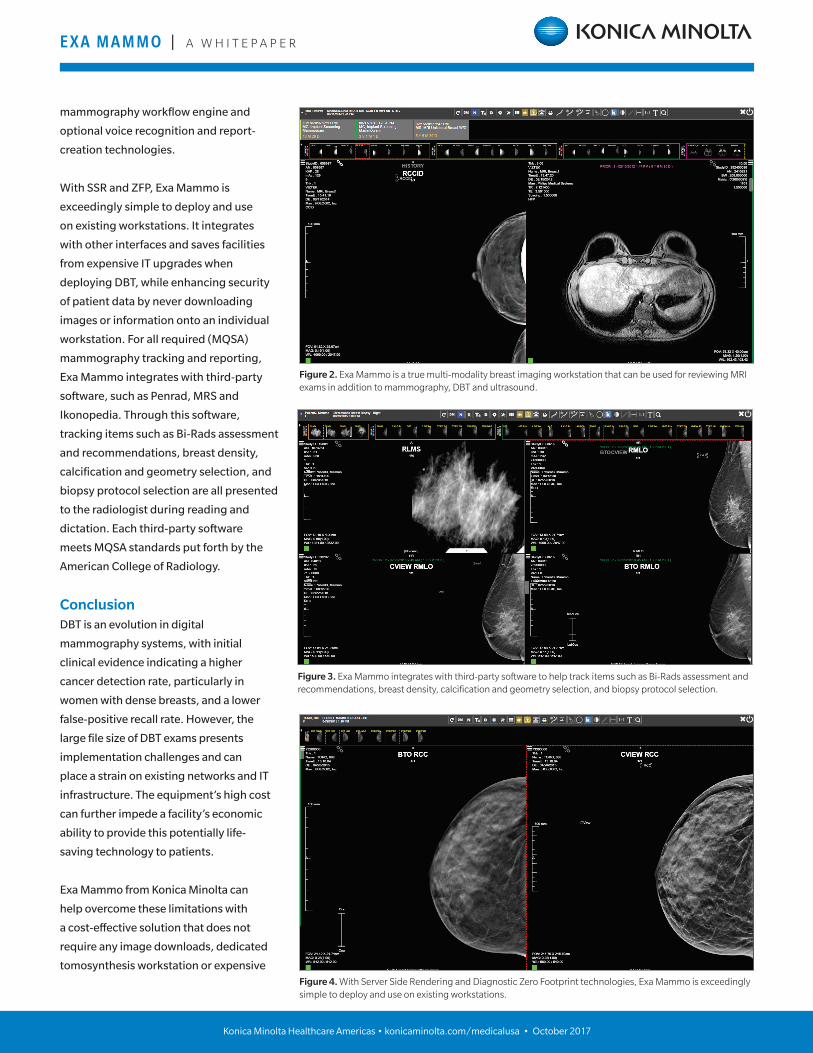
Figure 2. Exa Mammo is a true multi-modality breast imaging workstation that can be used for reviewing MRI exams in addition to mammography, DBT and ultrasound.
Figure 3. Exa Mammo integrates with third-party software to help track items such as Bi-Rads assessment and recommendations, breast density, calcification and geometry selection, and biopsy protocol selection.
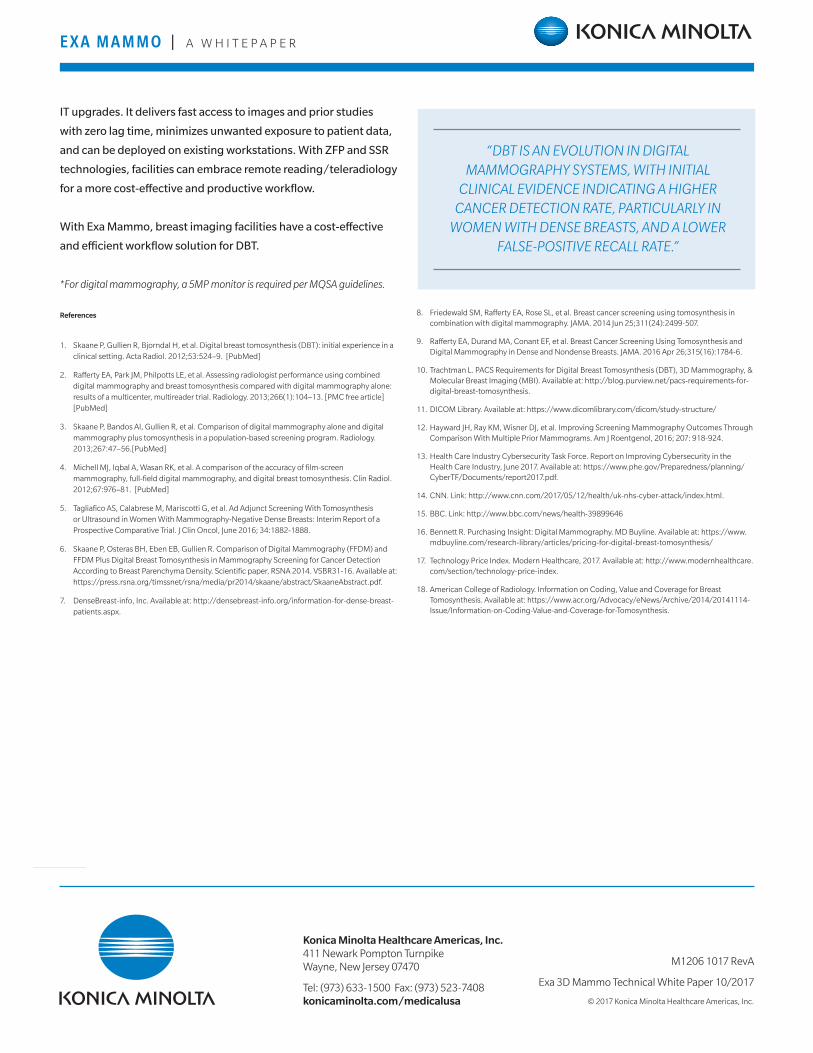
Figure 4. With Server Side Rendering and Diagnostic Zero Footprint technologies, Exa Mammo is exceedingly simple to deploy and use on existing workstations.
E X A M A M M O | A W H I T E P A P E R
IT upgrades. It delivers fast access to images and prior studies
with zero lag time, minimizes unwanted exposure to patient data,
and can be deployed on existing workstations. With ZFP and SSR
technologies, facilities can embrace remote reading/teleradiology
for a more cost-effective and productive workflow.
With Exa Mammo, breast imaging facilities have a cost-effective
and efficient workflow solution for DBT.
*For digital mammography, a 5MP monitor is required per MQSA guidelines.
References
1. Skaane P, Gullien R, Bjorndal H, et al. Digital breast tomosynthesis (DBT): initial experience in a clinical setting. Acta Radiol. 2012;53:524–9. [PubMed]
2. Rafferty EA, Park JM, Philpotts LE, et al. Assessing radiologist performance using combined digital mammography and breast tomosynthesis compared with digital mammography alone: results of a multicenter, multireader trial. Radiology. 2013;266(1):104–13. [PMC free article] [PubMed]
3. Skaane P, Bandos AI, Gullien R, et al. Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population-based screening program. Radiology. 2013;267:47–56.[PubMed]
4. Michell MJ, Iqbal A, Wasan RK, et al. A comparison of the accuracy of film-screen mammography, full-field digital mammography, and digital breast tomosynthesis. Clin Radiol. 2012;67:976–81. [PubMed]
5. Tagliafico AS, Calabrese M, Mariscotti G, et al. Ad Adjunct Screening With Tomosynthesis or Ultrasound in Women With Mammography-Negative Dense Breasts: Interim Report of a Prospective Comparative Trial. J Clin Oncol, June 2016; 34:1882-1888.
6. Skaane P, Osteras BH, Eben EB, Gullien R. Comparison of Digital Mammography (FFDM) and FFDM Plus Digital Breast Tomosynthesis in Mammography Screening for Cancer Detection According to Breast Parenchyma Density. Scientific paper, RSNA 2014. VSBR31-16. Available at: https://press.rsna.org/timssnet/rsna/media/pr2014/skaane/abstract/SkaaneAbstract.pdf.
7. DenseBreast-info, Inc. Available at: http://densebreast-info.org/information-for-dense-breast-patients.aspx.
8. Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014 Jun 25;311(24):2499-507.
9. Rafferty EA, Durand MA, Conant EF, et al. Breast Cancer Screening Using Tomosynthesis and Digital Mammography in Dense and Nondense Breasts. JAMA. 2016 Apr 26;315(16):1784-6.
10. Trachtman L. PACS Requirements for Digital Breast Tomosynthesis (DBT), 3D Mammography, & Molecular Breast Imaging (MBI). Available at: http://blog.purview.net/pacs-requirements-for-digital-breast-tomosynthesis.
11. DICOM Library. Available at: https://www.dicomlibrary.com/dicom/study-structure/
12. Hayward JH, Ray KM, Wisner DJ, et al. Improving Screening Mammography Outcomes Through Comparison With Multiple Prior Mammograms. Am J Roentgenol, 2016; 207: 918-924.
13. Health Care Industry Cybersecurity Task Force. Report on Improving Cybersecurity in the Health Care Industry, June 2017. Available at: https://www.phe.gov/Preparedness/planning/CyberTF/Documents/report2017.pdf.
14. CNN. Link: http://www.cnn.com/2017/05/12/health/uk-nhs-cyber-attack/index.html.
15. BBC. Link: http://www.bbc.com/news/health-39899646
16. Bennett R. Purchasing Insight: Digital Mammography. MD Buyline. Available at: https://www.mdbuyline.com/research-library/articles/pricing-for-digital-breast-tomosynthesis/
17. Technology Price Index. Modern Healthcare, 2017. Available at: http://www.modernhealthcare.com/section/technology-price-index.
18. American College of Radiology. Information on Coding, Value and Coverage for Breast Tomosynthesis. Available at: https://www.acr.org/Advocacy/eNews/Archive/2014/20141114-Issue/Information-on-Coding-Value-and-Coverage-for-Tomosynthesis.
“DBT IS AN EVOLUTION IN DIGITAL MAMMOGRAPHY SYSTEMS, WITH INITIAL
CLINICAL EVIDENCE INDICATING A HIGHER CANCER DETECTION RATE, PARTICULARLY IN
WOMEN WITH DENSE BREASTS, AND A LOWER FALSE-POSITIVE RECALL RATE.”
Konica Minolta Healthcare Americas, Inc. 411 Newark Pompton Turnpike Wayne, New Jersey 07470
Tel: (973) 633-1500 Fax: (973) 523-7408 konicaminolta.com/medicalusa
M1206 1017 RevA
Exa 3D Mammo Technical White Paper 10/2017
© 2017 Konica Minolta Healthcare Americas, Inc.