a novel approach to informing the public about the risks of overdose and nonmedical use of...
TRANSCRIPT

A Novel Approach to Informing the Public aboutthe Risks of Overdose and Nonmedical Use ofPrescription Medications
Suzanne Doyon, MD, FACMT,1,2 Wendy Klein‐Schwartz, PharmD, MPH,1
Bruce A. Anderson, PharmD,1 Christopher Welsh, MD2
1School of Pharmacy, University of Maryland, Baltimore, Maryland2School of Medicine, University of Maryland, Baltimore, Maryland
Background: Poison centers answer telephone calls from personsrequesting identification of tablets. Many of these calls are frompeople for whom the tablets were not prescribed and potentiallyrepresent nonmedical use. Implementation of a telephone‐basedprogram of overdose prevention and screening for nonmedical use ofprescription medications is examined.Methods: Social workers with experience in substance abusedisorders were hired by a poison center to answer telephone callsfrom persons asking for tablet identification. The social workers askedquestions regarding demographics, provided the ingredients, providedoverdose prevention/safety information, and offered referral totreatment to callers who desired it.Results: A total of 17,616 tablet identification calls from the publicwere answered by the social workers during the 20‐month studyperiod. Most callers were Caucasian with median age 33 years (range18–93 years). Overdose prevention/safety information, aimed mostlyat reducing polydrug use, was delivered to 6,635 (37.7%) callers.Conclusions: Treatment resource information was provided to 3,775(21.4%) callers. A telephone‐based service made up of social workersinteracted with several thousand individuals potentially at risk foradverse outcomes from nonmedical use of prescription medicationsand delivered overdose/safety information. Although further study isneeded, this type of service can complement existing state/communityefforts aimed at education regarding the nonmedical use ofprescription medications. (Am J Addict 2013;22:108–112)
INTRODUCTION
In the United States, more people use prescriptionmedications nonmedically than the total number of peoplewho use cocaine, heroin, hallucinogens, ecstasy, and inha-lants.1 In 2008, an estimated 34.8 million persons over the age
of 12 years reported having ever used pain relievers (primarilyopioids) nonmedically. In addition, tranquilizers (primarilybenzodiazepines) had been used nonmedically by approxi-mately 21.5 million, stimulants by 21.2 million, and sedatives(primarily barbiturates) by 8.9 million.1 In 2009, nearly one‐third of persons aged 12 years and over who used drugs for thefirst time began by using prescription medications nonmedi-cally.2 The state of Maryland is not immune to these nationaltrends. The Attorney General for Maryland reported thatprescription drug abuse rose 132% statewide between 1999and 2003.3
In addition, between 1999 and 2006, the number of fatalpoisonings involving prescription opioids more than tripled inthe United States, from 4,000 to 13,800.4 Additionally,approximately 50% of prescription opioid‐related deaths arereported to involve more than one medication, with benzo-diazepines co‐specified most frequently.5 Recognizing theserisks, the federal government (Drug Enforcement Administra-tion, Food and Drug Administration, Substance Abuse andMental Health Services Administration) and Partnership for aDrug‐Free America have launched initiatives targeting the lackof awareness regarding the dangers of prescription medicationabuse.2,6,7
People often turn to poison centers for help in identifyingmedications based on the imprint code. Over one million tabletidentification calls were answered by US poison centers in2009.8 Between 2002 and 2005, the Maryland Poison Centerexperienced a substantial increase in tablet identification callsfrom 7,942 to 20,003 calls per year, and it was felt by the poisonspecialists who answered these calls that most of the increasecame from people who were using the medicationsnonmedically.
Based on the well‐established poison center model ofimmediate telephone‐based delivery of poisoning informationand injury prevention to the public, a tablet identificationservice was implemented. Social workers with specific trainingin substance abuse counseling not only identified the tablets but
Received July 21, 2011; revised August 17, 2011; acceptedNovember 1, 2011.
Address correspondence to Dr. Doyon, Maryland Poison Center,220 Arch Street, Office level 1, Baltimore, MD 21201. E‐mail:[email protected].
The American Journal on Addictions, 22: 108–112, 2013Copyright © American Academy of Addiction PsychiatryISSN: 1055-0496 print / 1521-0391 onlineDOI: 10.1111/j.1521-0391.2013.00305.x
108

also warned callers about potentially risky behaviors involvingthese medications. To our knowledge, no similar service hasbeen described.9,10
MATERIALS AND METHODS
One full‐time and two part‐time masters‐level socialworkers with clinical experience in screening, assessment,and brief interventions around substance use disordersperformed their duties using the telephone and computerworkstations within the poison center call receiving area. Thisservice was available approximately 10 hours per day, 7 daysper week.
Training of the social workers consisted of one 8‐hour shiftlearning the telephone management system and tabletidentification database Thompson Reuters Poisindex® (www.thompson.com). This database can identify 80–85% of tablets.Further training in use of Lexi‐Comp® (www.crlonline.com),Facts and Comparisons® (http://online.factsandcomparisons.com), and IdentaDrug® (www.identadrug.com) occurred overthe following 2 weeks. This additional training was necessary inorder to reach 95–98% tablet identification.
Data were entered in real time and collected prospectivelyadhering to the guidelines provided in a five‐page instructionbinder. Tablet identification for callers under the age of 18 yearswas restricted as per the pre‐existing policy of the MarylandPoison Center. The University of Maryland InstitutionalReview Board waived the requirement for review of thisresearch.
All calls to the poison center were initially triaged bycertified specialists in poison information (nurses andpharmacists) to assess and confirm that an actual exposurehad not occurred. Subsequently, the tablet identification callswere re‐routed to the social workers who proceeded to say: “Iwill give you the information your are requesting but may I askyou a few questions before I do so?” Social workers then askedquestions regarding demographics, identified the contents, andoffered relevant overdose prevention/safety information.
Demographic InformationAge of caller, name, phone number, zip code of the call (not
residence), date and time, reason for the call, and tabletcontents were recorded in the poison center database (VisualDotlab Enterprise®, Version 4.3.8; WBM Software). Race,gender, relationship of caller to user, what the caller thought thetablet contained, offer of overdose prevention/safety informa-tion, and/or treatment resource information were recorded in acustomized web‐based application. Data were analyzed usingdescriptive statistics including frequency of distributions.
Identification of Tablet ContentTablets were defined as solid dosage forms of drugs (eg,
pills or capsules). The unique tablet imprint (letters andnumbers) embossed on the outside of the tablet was used.Social workers were trained to differentiate generic, brand, and
street names of medications, to recognize the differentingredients in combination tablets (eg, hydrocodone combinedwith acetaminophen), to understand the different formulationsand delivery systems and keep current with emergingprescription medication trends (eg, introduction of tapentadol).Poison specialists, nurses, and pharmacists with extensivetraining in toxicology and years of experience with identifica-tion of tablets, provided immediate on‐site back up at all times.
Overdose Prevention/Safety Information and AdviceOverdose prevention/safety information aimed at reducing
risky behaviors such as polydrug use or other behaviorsassociated with drug use were delivered by the social worker.Information was individualized based on the reason for the calland specific tablet contents. Typical information included:(1) “do not mix different sedatives such as benzodiazepines,ethanol, and opioids”; (2) “do not operate machinery includingmotor vehicles after taking the (sedating) medication”; (3) “donot overuse different acetaminophen‐containing products”;(4) “do not mix your tablets in the same container.” The firsttwo messages were delivered when an opioid, benzodiazepine,or muscle relaxant was identified; the third message wasdelivered when an acetaminophen combination product wasidentified; the fourth message was more generic and onlydelivered to certain callers. The relevant messages wereimmediately delivered upon identification of contents. Thereason for termination of the call was recorded (“hung up mid‐conversation,” “conversation finished,” “unknown”).
Treatment Resources InformationAt the discretion of the social worker (largely dependent on
the perceived receptiveness of the caller), certain callers wereasked the following question(s): “do you have a substanceabuse problem?” or “do you think he/she might have a problemwith drugs?”Callers who answered yes to these questions wereimmediately engaged in further discussion and provided withtreatment information, if desired. Relatives/friends of the userwere also advised that additional resources may be available tothe user if he/she called back at a later time. Finally, callerswere asked if they could be contacted by phone for a follow‐up.
RESULTS
Between August 21, 2007 and March 6, 2009 the socialworkers employed by the Maryland Poison Center answered atotal of 29,461 tablet identification calls: 17,616 (59.8%) werefrom the public, 5,513 (18.7%) from law enforcement officersor detention centers, 2,189 (7.4%) from health care providers,and 4,143 (14.1%) other or unknown. Public callers’ medianage was 33 years (range, 18–93 years; Fig. 1). The callersidentified themselves as Caucasian (82.4%), AfricanAmericans (12.7%), Hispanic (1.1%), Asian (.4%), and other(3.3%). Male callers were 42.8%.
Of the 17,616 public calls answered by the social workers,10,985 (62.4%) identified themselves as the users of the tablet
Doyon et al. March–April 2013 109
and 6,631 (37.6%) identified themselves as a relative/friend ofthe user. Of the “self‐callers,” only 5,971 (54.4%) reported thatthe tablet was prescribed to them; 3,978 (36.2%) reported thatthe tablet was not prescribed to them; and 1,036 (9.4%)reported that the source of the tablet was unknown.
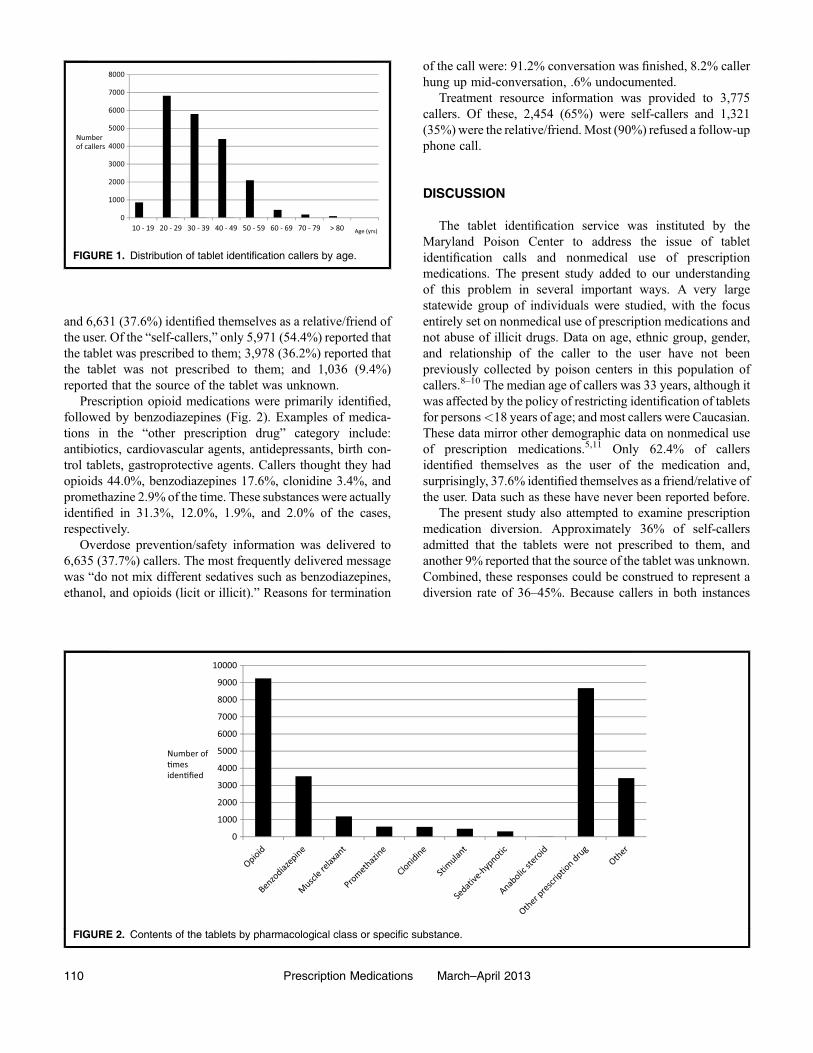
Prescription opioid medications were primarily identified,followed by benzodiazepines (Fig. 2). Examples of medica-tions in the “other prescription drug” category include:antibiotics, cardiovascular agents, antidepressants, birth con-trol tablets, gastroprotective agents. Callers thought they hadopioids 44.0%, benzodiazepines 17.6%, clonidine 3.4%, andpromethazine 2.9% of the time. These substances were actuallyidentified in 31.3%, 12.0%, 1.9%, and 2.0% of the cases,respectively.
Overdose prevention/safety information was delivered to6,635 (37.7%) callers. The most frequently delivered messagewas “do not mix different sedatives such as benzodiazepines,ethanol, and opioids (licit or illicit).” Reasons for termination
of the call were: 91.2% conversation was finished, 8.2% callerhung up mid‐conversation, .6% undocumented.
Treatment resource information was provided to 3,775callers. Of these, 2,454 (65%) were self‐callers and 1,321(35%) were the relative/friend.Most (90%) refused a follow‐upphone call.
DISCUSSION
The tablet identification service was instituted by theMaryland Poison Center to address the issue of tabletidentification calls and nonmedical use of prescriptionmedications. The present study added to our understandingof this problem in several important ways. A very largestatewide group of individuals were studied, with the focusentirely set on nonmedical use of prescription medications andnot abuse of illicit drugs. Data on age, ethnic group, gender,and relationship of the caller to the user have not beenpreviously collected by poison centers in this population ofcallers.8–10 The median age of callers was 33 years, although itwas affected by the policy of restricting identification of tabletsfor persons<18 years of age; and most callers were Caucasian.These data mirror other demographic data on nonmedical useof prescription medications.5,11 Only 62.4% of callersidentified themselves as the user of the medication and,surprisingly, 37.6% identified themselves as a friend/relative ofthe user. Data such as these have never been reported before.
The present study also attempted to examine prescriptionmedication diversion. Approximately 36% of self‐callersadmitted that the tablets were not prescribed to them, andanother 9% reported that the source of the tablet was unknown.Combined, these responses could be construed to represent adiversion rate of 36–45%. Because callers in both instances
0
1000
2000
3000
4000
5000
6000
7000
8000
10 - 19 20 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 > 80
Number of callers
Age (yrs)
FIGURE 1. Distribution of tablet identification callers by age.
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
Number of �mes iden�fied
FIGURE 2. Contents of the tablets by pharmacological class or specific substance.
110 Prescription Medications March–April 2013

could easily misrepresent the source of the tablet(s), these dataneed to be interpreted cautiously. Historical data on diversionare sparse, but in one study, it was thought to be responsible forup to 63.1% of unintentional overdose deaths.12 The NationalSurvey on Drug Use and Health (NSDUH) reported that 70.2%of persons who used pain relievers nonmedically in the past12 months obtained the pain relievers from a friend orrelative.13 It is important to remember that the presentstudy and the NSDUH surveyed two different populations.Nevertheless, these data may complement existing data ondiversion rates and trends.
This study also attempted to examine lay persons’familiarity with tablet ingredients. A surprising number ofcallers misidentified the ingredients in the tablets. Reasons forthis misidentification include: drug seller deception, prescriberdeception, and conviction that the pharmacist dispensed thewrong medication. Misidentification of medications by users israrely discussed in the literature and these findings areimportant for law enforcement, physicians, and other treatmentproviders who rely heavily on self‐reporting of drug use. Inbrief, self‐reporting of nonmedical use of prescriptionmedication may yield false information in up to 30% of cases.
The tablet identification service served two additional corefunctions: (1) to provide targeted and timely overdoseprevention/safety information; (2) to provide treatmentresources information if desired by the caller. The servicewas designed to reach out to individuals who may nototherwise come into contact with traditional medical settingssuch as primary care providers or emergency departments. Theservice delivered at least one overdose prevention/safetyinformation message to 6,635 callers. The service was uniquein that it provided to users and/or relatives information that wasboth immediate and relevant to the tablet ingredients and issue.The overdose prevention/safety information messages werelistened to by most, as >90% of callers waited until the fullmessage was complete before terminating the call. Historically,the majority of overdose prevention efforts were directed ateducation and reduction of risky behaviors. They wereperceived to suffer from delays between issue identificationand introduction of safety messages, and to lack sufficientflexibility in coping with shifts in drug markets.14 The socialworkers operating within the tablet identification service actedwithout delay and attempted to be relevant to the substanceidentified, the caller, and the issue. However, the impact of theoverdose prevention messages on mortality rates or emergencydepartment visits could not be measured. Also, because mostdid not want to be contacted again, the callers were notroutinely asked whether the information was useful to them.Despite these shortcomings, it is likely that there is value inproviding overdose prevention/safety information to callers.Consistent relevant messaging from multiple different sourcesover time may help effect changes in behavior.
Limitations include the fact that these data are from one stateonly and may not be generalizable. The study relied on self‐report and is therefore subject to recall bias, resulting inunderestimates. Consistency of interactions could not be
assured and provider drift could have occurred. The study wasalso limited by the lack of follow‐up and evidence that theoverdose prevention/safety information changed behavior.
The findings of this study raise certain questions regardingpracticability and future practice implications. Implementationof a tablet identification service is within the scope, reach, andcapabilities of many agencies. Further study in this area, couldinclude the use of current communication technology (instantmessaging, texting, Facebook, Twitter) to deliver moreoverdose prevention/safety information and treatment resourceinformation. It could also include measures of efficacy, such assurveying recipients regarding the usefulness of the informa-tion or whether or not they entered treatment, again usingcurrent communication technology. Lastly, further study couldfocus on the use of voice, video calls, and voice chat overthe internet.
CONCLUSIONS
The addition of social workers with clinical experience insubstance use disorders to assist in tablet identification andprovide overdose prevention/safety information was anintervention that was practical, rapidly implemented statewide,and feasible. This telephone‐based service interacted with ascarcely studied population of several thousand individualspotentially at risk for adverse outcomes from nonmedical useof prescription medications. The service offered usefulinformation about this population. Although further study isneeded, this type of service can complement existing state/community efforts aimed at educating the public regarding thenonmedical use of prescription medications.
Declaration of InterestThe authors report no conflicts of interest. The authors alone
are responsible for the content and writing of this paper.
REFERENCES
1. Substance Abuse and Mental Health Services Administration. Resultsfrom the 2008 National Survey on Medications Use and Health: NationalFindings (Office of Applied Studies, NSDUH Series H‐36, HHSPublication No. SMA 09‐4434). Rockville, MD; 2009.
2. Office of the National Drug Control Policy. Prescription drug abuse.http://www.whitehousedrugpolicy.gov/prescriptiondrugs/. AccessedJuly 2011.
3. Curran JJ. Prescription for disaster—The growing problem of prescriptiondrug abuse in Maryland. State of Maryland Office of the Attorney General.http://www.oag.state.md.us/Reports/PrescriptionDrugAbuse.pdf#search.Accessed October 2010.
4. Paulozzi LJ, Yongli X. Recent changes in medications poisoning mortalityin the United States by urban–rural status and medications type.Pharmacoepidemiol Med Saf. 2008;17:997–1005.
5. Warner M, Chen LH, Makuc DM. Increase in fatal poisonings involvingopioid analgesics in the United States, 1999–2006. NCHS Data Brief.Hyattsville, MD: National Center for Health Statistics; 2009; p. 22.
6. Woodcock J. A difficult balance—Pain management, medications safety,and the FDA. New Eng J Med. 2009;361:2105–2107.
Doyon et al. March–April 2013 111

7. The Partnership for Drug‐Free America. Senate bill would require doctortraining to fight prescription drug abuse. http://www.drugfree.org/join‐together/drugs/senate‐bill‐would‐require‐doctor‐training‐to‐fight‐prescription‐drug‐abuse. Accessed July 2011.
8. Bronstein AC, Spyker DA, Cantilena LR, et al. Annual report of theAmerican Association of Poison Control Centers’ National Poison DataSystem (NPDS): 27th Annual report. Clin Toxicol. 2010;48:979–1198.
9. Anderson HG, Jaramillo JE, Jaramillo JP, et al. Medication identification:A survey of poison control centers. J Toxicol Clin Toxicol. 2004;42:371–381.
10. Scharman EJ. Poison centers and medication identification. J Am PharmAssoc. 1997;NS37:373.
11. Coben JH, Davis SM, Furbee PM, et al. Hospitalizations for poisonings byprescription opioids, sedatives, and tranquilizers. Am J Prev Med.2010;38:517–524.
12. Hall AJ, Logan JE, Toblin RL, et al. Patterns of abuse among unintentionalpharmaceutical overdose fatalities. JAMA. 2008;300:2613–2620.
13. Substance Abuse and Mental Health Services Administration. Resultsfrom the 2009 National Survey on Medications Use and Health: Volume I.Summary of National Findings. http://oas.samhsa.gov/NSDUH/2k9NSDUH/2k9Results.htm. Accessed July 2011.
14. Horyniak D, Higgs P, Lewis J, et al. An evaluation of a heroinoverdose prevention and education campaign.Drug Alcohol Rev. 2010;29:5–11.
112 Prescription Medications March–April 2013