a japanese approach to establish an electronic patient record system in an intelligent hospital
TRANSCRIPT

International Journal of Medical Informatics 49 (1998) 45–51
A Japanese approach to establish an electronic patient recordsystem in an intelligent hospital
Hiroshi Takeda a,*, Yasushi Matsumura a, Takeo Okada a, Shigeki Kuwata a,Michitoshi Inoue b
a Department of Medical Information Science, Osaka Uni6ersity Hospital 2-15, Yamada-Oka, Suita 565, Japanb Osaka National Hospital, 2-1-14, Hoen-Zaka, Chao-Ku, Osaka 540, Japan
Keywords: ERR; Electronic Patient Record; Hospital Information System
1. Introduction
In order to respond to the growing needsfor clinical, educational and academic func-tions, the Osaka University Medical Schooland its attached hospital were moved to anew campus in 1993. On this occasion theuniversity hospital has planned to constructan ‘intelligent’ hospital. The new hospitalconsists of 19 clinics for an average of 2200outpatients’ visits per day and 1076 beds in24 nursing units, nine Hospital Service Divi-sions, Pharmacy Department, Nursing De-partment and Department of Administration.
Two aspects must be emphasised in the‘intelligent’ hospital. Firstly, as human re-sources are limited, the hospital is required tointroduce new technologies which will saveman-power and reallocate the power. Simul-taneously, the hospital will provide amenities
which will facilitate the human work. Sec-ondly, integration of various types of hospitalinformation will be much more important. Inorder to support the decision making of thehospital manager and clinical staffs, hospitalmanagement data and patient data must becollected and integrated by means of infor-mation technologies.
One of the final goals in an intelligenthospital is to establish an Electronic PatientRecord (EPR) system which replaces conven-tional paper medical record charts. In thispaper, our approach is described and somebarriers in terms of security and privacy is-sues will be discussed.
2. Conventional medical record chartsmanagement
Before reconstructing the university hospi-tal, medical records of both inpatients and* Corresponding author.
1386-5056/98/$19.00 © 1998 Elsevier Science Ireland Ltd. All rights reserved.
PII S1386-5056(98)00009-4

H. Takeda et al. / International Journal of Medical Informatics 49 (1998) 45–5146
outpatients were stored and retrieved in eachclinical department and the way of manage-ment was so poor that patient records wereutilised to a limited extend. In the new hospi-tal, ‘one patient–one identification number(ID)–one medical record filing’ method hasbeen applied and the active and inactiverecord charts are stored in the central medicalrecord library where an automatic retrievalrobot system and transportation system arewell operated. Only the medical staffs areallowed to enter the reading room of themedical records. The entrance events arerecorded by opening the door by using thestaff ID card reader. The quality of the man-agement and the filing method is dramaticallyimproved. It is also emphasised that thechange in the medical record charts manage-ment system will facilitate the paradigm shiftfrom doctor-centred to patient-oriented medi-cal record and will provide the emotionalbasis for sharing the whole patient clinicalrecord for education, clinical research as wellas clinical practice without boundaries amongclinical departments and types of professions.
3. Hospital information system: HUMANE
3.1. Design goals of the HIS
In our hospital, the Hospital InformationSystem (HIS) has been nicknamed as ‘HU-MANE’ (Human-oriented Universal MedicalAssessment system by Network Environ-ment) [1]. In the development of HUMANE,the initial goals to be achieved were:1. Physicians Order Entry (POE) and good
Man–Machine Interface (MMI);2. short response time at a micro frame and,3. Multi-Media Database (MMD) and Pic-
ture Archiving and Communication Sys-tem (PACS).
3.2. Hardware of the HIS
The Main-Medium-Micro Frame Link(MMML) is our original hardware configura-tion of HIS in Japan [2]. Although the systemis a so-called legacy one, we have chosen thevertical–horizontal–vertical distribution ofthe information processing in order to solvethe problem for ensuring the fast responseand good MMI at minimum cost. The role ofthe mainframe is to manage the database andon-line transactions. The medium frameworks as a server of the microframe and filesbasic patient clinical data and master tables.The microframe has as function to maintaina good MMI and assist POE. In HUMANE,the mainframe is ACOS 3600/10 MP (mainmemory 64 MB, 16 GB hard disk), and fortyworkstations (EWS 4800, OS: UNIX, mainmemory 36 MB, 1.2 GB hard disk) as medi-umframes and about six hundred personalcomputers (PC9821, OS: MS-DOS 5.0, Win-dows 3.1, main memory 11.6 MB, 120 MBhard disk) as microframes. This MMMLconfiguration is rented from NEC (Tokyo,Japan).
3.3. Software and application programs
The organisational approach to build upthe software architecture of a HIS is veryimportant. A strategic goal of HUMANE isto support decision making. In this respect, amultidimensional EPR system must be con-sidered. To realise the strategic level, thetactical level and operational level must beestablished beforehand.
At tactical level HUMANE is to create adigital information environment with intra-and inter-network. The hospital administra-tive database and clinical information data-base [3] are highly interactive and relate toeach other. PACS is already partially in-stalled for test beds [4,5] to clear problems

H. Takeda et al. / International Journal of Medical Informatics 49 (1998) 45–51 47
due to the large amount of information quan-tity. This will facilitate telemedicine [6,7] inthe regional health care and comprehensivehealth care.
At operational level HUMANE is used toreduce the paperwork load, to enhance real-time communication, patient service improve-ment and quality control of patient care. Theoperational level features order entry andreporting system and the mission is almostcompleted in our university hospital exceptfor parental drug ordering.
The software menu of the HIS is dividedinto two categories. The one is Interdepart-mental or Common Application Program(IDAP) and the other is Department-SpecificApplication Program (DSAP). AmongIDAPs of the HUMANE are patient registra-tion, accounting and billing system, orderentry system (prescription, laboratory test,radiological examination admission order,surgical operation and meal service), diseasename registration, reporting system (labora-tory test and radiological examination), reser-vation (re-visit, special examination),admission management and nursing care sys-tem. DSAPs in the HUMANE are developedin the pharmacy department, laboratory de-
partment, radiological examination depart-ment (RIS, Radiology Information Sys-tem), surgical operation department, mealservice department and blood transfusiondepartment.
As almost all orders will be filed in thepatient management database, accountingcalculation will be easily made and the loss ofthe billing will decrease. The reporting systemis the most important part of the operationallevel of the hospital information system inthe intelligent hospital.
4. EPR system of Osaka University Hospital(EPROU)
4.1. Concept
A successful installation of a totally inte-grated hospital information system HU-MANE will be followed by the developmentof a comprehensive EPR system (EPROU)[8]. The concept of EPROU is illustrated inFig. 1. The output of the system will beconverted into Medical Mark-up Language(MML) or SGML format which the Japanesenational EPR project will adopt as data ex-change standard [9].
In an EPR system, data elements in apatient record are simplified as a model. Itwill be recognised that the fact, assessment,action, summary and message will be thecontents of the clinical record and continuouslink among fact, assessment and actionmoves time-serially in accordance with theclinical process. Some of the fact and actiondata such as the results of lab tests andcontents of prescription could be obtainedfrom the HIS database. However, importantdata for the EPR system such as chief com-plaints, physical findings and problem listswould be input by physicians and/or nurses.
Fig. 1. The concept of the EPR system in OsakaUniversity Hospital (EPROU).
H. Takeda et al. / International Journal of Medical Informatics 49 (1998) 45–5148
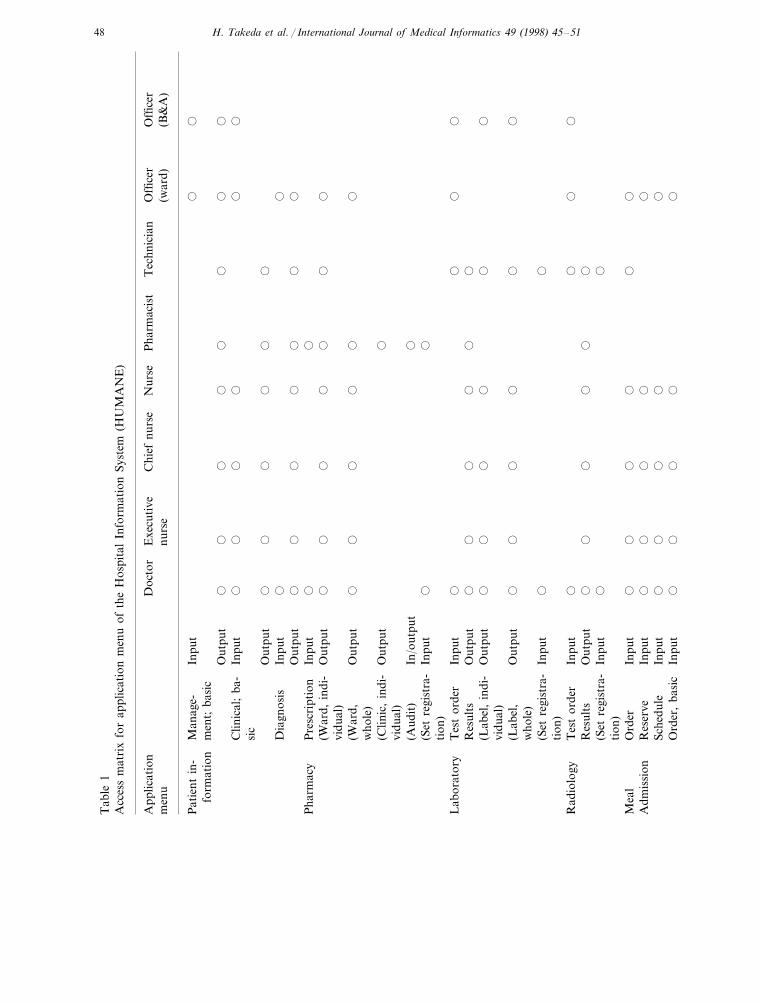
Tab
le1
Acc
ess
mat
rix
for
appl
icat
ion
men
uof
the
Hos
pita
lIn
form
atio
nSy
stem
(HU
MA
NE
)
Doc
tor
Exe
cuti
veT
echn
icia
nC
hief
nurs
eN
urse
Pha
rmac
ist
Offi
cer
App
licat
ion
Offi
cer
nurs
em
enu
(B&
A)
(war
d)
Inpu
t�
�P
atie
ntin
-M
anag
e-fo
rmat
ion
men
t;ba
sic
��
��
��
�O
utpu
t�
��
��
�C
linic
al;
ba-
�In
put
sic
��
��
Out
put
��
Dia
gnos
is�
Inpu
t�
��
��
��
�O
utpu
t�
Pha
rmac
yP
resc
ript
ion
Inpu
t�
��
��
��
�O
utpu
t(W
ard,
indi
-vi
dual
)�
(War
d,�
��
�O
utpu
t�
who
le)
�O
utpu
t(C
linic
,in
di-
vidu
al)
(Aud
it)
�In
/out
put�
�(S
etre
gist
ra-
Inpu
tti
on)
��
��
Lab
orat
ory
Tes
tor
der
Inpu
t�
��
Res
ults
Out
put
��
� ��
��
��
Out
put
(Lab
el,
indi
-vi
dual
)�
(Lab
el,
��
��
Out
put
�w
hole
)�
�In
put
(Set
regi
stra
-ti
on)
Tes
tor
der
��
�In
put
�R
adio
logy
��
��
�O
utpu
t�
Res
ults
�In
put
�(S
etre
gist
ra-
tion
)O
rder
��
��
Inpu
t�
Mea
l�
��
Adm
issi
onR
eser
veIn
put
��
��
��
Sche
dule
��
Inpu
t�
Ord
er,
basi
c�
�In
put
��

H. Takeda et al. / International Journal of Medical Informatics 49 (1998) 45–51 49
Tab
le1
(Con
tinu
ed)
Doc
tor
Exe
cuti
veO
ffice
rC
hief
nurs
eN
urse
Pha
rmac
ist
Tec
hnic
ian
App
licat
ion
Offi
cer
men
u(B
&A
)(w
ard)
nurs
e
Surg
ical
op.
�In
put
Res
erve
Sche
dule
��
�O
utpu
t�
� ��
��
Inpu
tR
eser
vati
on�
Con
sult
atio
n�
��
��
��
Spec
ial
test
Inpu
t�
(Ind
ivid
ual)
��
��
Out
put
��
�(T
est)
��
��
Out
put
��
��
Inpu
tM
anag
emen
t�
Nur
sing
Car
eor
der
Inpu
t�
��
��
��
�O
utpu
t�
�W
orks
heet
Out
put
��
��
��
Inpu
tM
anag
emen
t�
��
Per
sonn
elaf
-In
put
fair
s�
��
Inpu
t�
Clin
ical
man
-P
atie
ntse
-ag
emen
tqu
ence
Clin
ical
sys-
tem
Fin
anci
alsy
s-te
mP
AC
SE
PR
syst
em

H. Takeda et al. / International Journal of Medical Informatics 49 (1998) 45–5150
Since physicians’ direct data entry is socommon in Japan, an EPR system is requiredto enable faster input of necessary clinicaldata. Furthermore, the entered data shouldprovide the basis for synthetic and analyticpurposes in clinical research, education, hos-pital management as well as clinical care. Tomerge and balance the operability and theutility of an EPR system, we have developeda system (DTDES, ‘Dynamic TemplateDriven Data Entry System’) [10] which al-lows users to select the desired data from alist of items by means of a graphical userinterface.
4.2. DTDES
Some data may be simple and others maybe complex. If each entry item were to bedisplayed in the same manner, the user wouldhave to follow the same procedure for inputof detailed information and for simplifieddata. In order to input simplified and detaileddata more effectively, we have decided thatentry items must be displayed in a templatein which the size will be adjusted due to thequantity of the information, and that thesystem will need to be driven by a type ofnavigation system which displays entry itemsbased on the previously entered value or cate-gory. For example, if the chief complaint of apatient is pain, a template appears in theCRT display and the physician will choosesecond keywords among pain related wordsets such as chest, abdomen and so on.
4.3. Display of registered data
There are two modes for displaying theregistered data. One is a progress note wheredata entered from the template are translatedinto a form of natural language and de-scribed on the note of EPROU. The other isa flow sheet which summarises the contents
of the clinical record time-serially in a matrixform. By clicking a cell, the detailed data aredisplayed, and the related progress note willbe shown by clicking on the date.
4.4. Template master and its maintenanceprogram
The contents and navigation method oftemplates and their translation method intonatural language have to be created throughrepeated trial and error. The template mastermust have two parts in which controllingdata for the template navigation and contentsof items are registered. The master file maybe generated and edited by end-users. Rulesfor translation into natural language are reg-istered in another master file. This file mustbe maintained by the system manager.
5. Discussion
Major premises for establishing the EPRsystem are maintainability of medical recordcharts management, quality control of thecontents of the conventional medical recordand the expansion of HIS. After taking thosehurdles, the launching of the EPR system willnot be a futuristic story in the Osaka Univer-sity Hospital. However, the problems of pri-vacy and security issues have not been solvedyet.
The conventional medical charts areconfined to the central medical record library.But for clinical care, only clinical staffs whocarry an authorised ID card are able to ac-cess the paper patient record which will bepresented to the staffs of the medical recordmanagement department. As long as the pa-tient record is described in the medical chart,the security and the protection of the privacywould be very confident. The rule of themanagement is controlled by the committee

H. Takeda et al. / International Journal of Medical Informatics 49 (1998) 45–51 51
on the medical record management. It is im-portant to note that the one patient–one filemanagement system where no segmentationof the patient record among the medical spe-cialisms occurs and time-serial presentationof the whole record is possible, will increasethe utility of the EPR system significantly.
The general policy for accessing the HISHUMANE was defined in the executive com-mittee of the hospital management. The oper-ational rules for accessing the hospitalinformation system were on the responsibilityof the Department of Medical InformationScience. The present rules are summarised inTable 1. Although the rules are now welloperated, it is limited to our HIS. New ruleswill be necessary for the forthcoming EPRsystem and telemedicine environment.
6. Conclusions
The EPR system of our university hospital(EPROU) is now under development and willbe operational in a few years. The qualityand maintainability of both the conventionalmedical charts management and the HIS areclosely connected to each other to establishthe EPR. The EPR development comprisesamongst others the dynamic template drivenentry system which is one of the optimalsolutions for physicians’ direct data entry. Inorder to make the EPR system practical, weare eager to establish the security and privacyprotection rules and to develop related tech-nologies in accordance with global and do-mestic harmonisation and standardisation.
References
[1] H. Takeda, Y. Matsumura, H. Kondo, H. Imai,M. Inoue, Development of a totally integrated
hospital information system: an intelligent hospi-tal in Osaka University, in: K. Lun et al. (Eds.),Proc. MEDINF092, 1992, pp. 241–246.
[2] Y. Matsumura, H. Takeda, M. Inoue, Implemen-tation of the totally integrated hospital informa-tion system (HUMANE) in Osaka UniversityHospital, in: R. Greenes et al. (Eds.), Proc.MEDINF095, 1995, pp. 590–593.
[3] S. Kuwata, Y. Matsumura, H. Takeda, M.Okada, M. Inoue, Development of patient infor-mation database: analysis of population in OsakaUniversity Hospital, in: Proc. Joint Conf. onJapanese Medical Informatics, 1995, pp. 931–934.
[4] C. Kuroda, et al., Planning for PACS at OsakaUniversity Hospital, Comput. Methods Prog.Biomed. 36 (1991) 147.
[5] H. Takeda et al., System design and implementa-tion of HIS, RIS and PC-Based PACS at theOsaka University Hospital, in: R.A. Greenes,H.A. Peterson, D.J. Protti (Eds.), Medinfo95,Proc. Eight World Congr. on Medical Informat-ics, Vancouver, Elsevier, Amsterdam, 1995, pp.430–433.
[6] K. Inamura, H. Kondoh, H. Takeda, Develop-ment and operation of PACS/Teleradiology inJapan. IEEE Commun. Mag. (1996) 46–51.
[7] H. Takeda et al., Development of a medical im-age filing system based on super high definitionimage and its functional evaluation, in: Proc.SPIE, vol. 3013, Bellingham: the Society ofPhoto-Optical Instrumentation Engineering, SanJose, 1997, pp. 149–156.
[8] H. Takeda et al., Development of a cardiovascu-lar disease-oriented electronic patient recordmodel in a Japanese university hospital, in: Proc.Toward An Electronic Patient Record ’96, SanDiego, Broadview, Kelvyn Press, 1996, pp. 520–523.
[9] H. Takeda, Y. Satomura, M. Kimura, Harmo-nization for standardisation: a Japanese ap-proach, in: Proc. Toward An Electronic PatientRecord ’97, Nashville, Broadview, Kelvyn Press,1997, pp. 370–373.
[10] H. Takeda et al., Dynamic template driven dataentry system for an EPR system, in: Proc. To-ward An Electronic Patient Record ’97,Nashville, Broadview, Kelvyn Press, 1997, pp.139–143.
.