a framework for conducting initial medication adherence ... · a framework for conducting initial...
TRANSCRIPT

1
A FRAMEWORK FOR CONDUCTING INITIAL MEDICATION ADHERENCE
RESEARCH
An ISPOR Workshop by the Medication
Adherence Good Research Practices Working
Group of the Medication Adherence and
Persistence Special Interest Group
Medication Adherence Good Research Practices Working Group
Co-Chairs: David Hutchins, MHSA, MBA Executive Advisor, Pharmacy Networks, CVS Caremark (Scottsdale, AZ, USA)
Andrew M. Peterson, PharmD, PhD Dean, Mayes College of Healthcare Business and Policy, University of the Sciences (Philadelphia, PA, USA)
Leadership Group:
Maria Malmenäs, MSc - Director, Health Economic Modeling Unit, HERON (Stockholm, Sweden)
Elizabeth Manias, RN, BPharm, MPharm, PhD - Deakin University, School of Nursing and Midwifery, Victoria; Adjunct Professorial Fellow, Department of Medicine, Royal Melbourne Hospital, the University of Melbourne (Melbourne, Australia)
Craig S. Roberts, PharmD, MBA Senior Director, Global Health & Value, Pfizer Inc (Collegeville, PA, USA)
Allison F. Williams, RN, PhD - School of Nursing and Midwifery, Monash University (Victoria, Australia)
John E Zeber, MHA, PhD - Co-director, Health Outcomes at Scott & White Healthcare, Center for Applied Health Research; Investigator, Central Texas Veterans Health Care System; Associate Professor, Texas A&M College of Medicine (Temple TX, USA)

2
WORKSHOP Presenters
Andrew M. Peterson David Hutchins – Discussion Leader
Craig S. Roberts John E. Zeber
PURPOSE of WORKSHOP:
To provide guidance on measuring initial
medication adherence (IMA), including
developing standard nomenclature and key
components of quality IMA research
Encourage discussion among a diverse
audience of investigators, health system
practitioners, patients and policy makers

3
John E. Zeber Central Texas VA; Scott & White Healthcare;
Texas A&M Health Science Center
Initial Medication Adherence – Study Background
Our first project* delved into complex IMA arena
Observed complexity of topic, definitions
overlap, problematic study design issues
Recognized need to summarize current IMA
research, benefits and limitations
Focused on factors associated with poor IMA
* Zeber JE, Manias EF, Williams AF, Hutchins D, Udezi WA, Roberts CS, Peterson AM. (2013). A systematic literature review of psychosocial and behavioral factors associated with initial medication adherence: a report of the ISPOR medication adherence & persistence special interest group. Value in Health, 16(5):891-900.
4
Background (continued)
Systematic literature review through 2012:
Medline, PsychInfo, CINAHL, others
Started with 865 articles … 63 read in full; 24
were eligible (moderate quality at best)
Variety of terms for very first Rx
Numerous study design approaches with
inconsistent abstract, key words, methods
Most examined patient factors; some covered
role of system and providers
Background (continued)
Key factors => medication class (16), patient
characteristics (14), physical comorbidities
(14), co-payments (11), health beliefs (6)
Strongest predictors = RX cost (ORs up to 7.3),
specific drug, illness severity, SES, lack of
discharge counseling
Similar factors influence IMA as for longer-term
adherence, but …
Discussion led into need for more standardized
Methodological approach, i.e., this study!

5
David Hutchins CVS Caremark
Overview of Current Methodological Study
Background: Second Project Second working subgroup
Purpose: meta-analysis
Findings: similar to those in our first project
Current project Provide guidance to and encourage more studies
Summarize current body of research
different methods
Feedback’s unanticipated stumbling block taxonomy

6
Cramer Taxonomy
Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value in Health. Jan-Feb 2008;11(1):44-47
Vrijens Taxonomy
Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. May 2012;73(5):691-705

7
Taxonomies
Initial Medication Adherence (IMA)
• Initial medication adherence is when a patient presents and receives a medication prescription for the treatment of a disease for the first time
• Nonadherence encompasses both unpresented and unclaimed prescriptions

8
Taxonomy Challenge: AUDIENCE INTERACTION #1
Break into groups (~10”)
Discuss Pros and Cons of “Initial
Medication Adherence” (IMA)
Re-gather and report
Summarize ideas
Initial Medication Adherence (IMA)
• Initial medication adherence is when a patient presents and receives a medication prescription for the treatment of a disease for the first time
• Nonadherence encompasses both unpresented and unclaimed prescriptions
9
State of Current IMA Research
Andrew M. Peterson University of the Sciences
Data Sources for IMA
Surveys of Patients
Prescribers
Pharmacists
Databases Pharmacy
Hospital/Clinic
Prescriber Office
Prescription Tracking Manual
Electronic
10
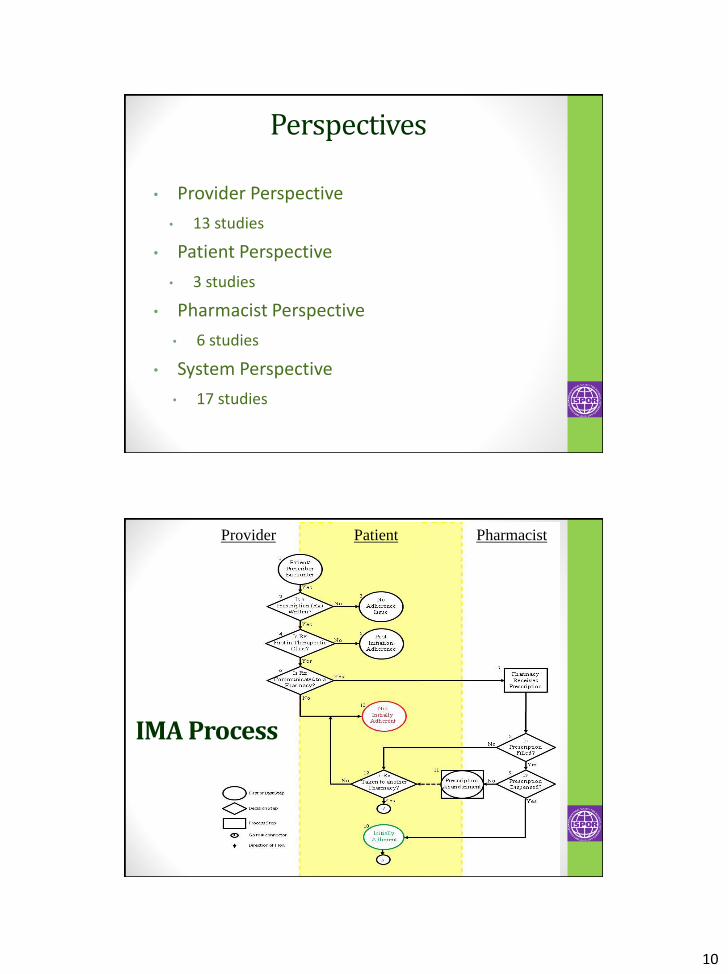
Perspectives
• Provider Perspective
• 13 studies
• Patient Perspective
• 3 studies
• Pharmacist Perspective
• 6 studies
• System Perspective
• 17 studies
IMA Process
Provider Pharmacist Patient

11
Framework for Analysis of IMA
Two key events required for an IMA Prescribing Event
Dispensing Event
Parameters involved in an IMA Core: must be provided to calculate a valid IMA
measurement
Supplemental: refine accuracy of IMA
measurement
Ancillary: influence IMA measurement
Craig S. Roberts Pfizer, Inc.

12
Defining IMA Study Parameters
• Must be provided for valid IMA measurement
• Examples: clear prescribing and dispensing information, specified time window for adherence, etc.
Core
• Refine accuracy of IMA measurement
• Examples: Consideration of substitution at the pharmacy, addressing potential out-of-network fulfillment, etc.
Supplemental
• Influence IMA measurement
• Examples: consider influence of behavioral factors, pharmacy characteristics, prescriber characteristics on adherence outcome.
Ancillary
Core parameters Study parameters that must be defined and
described for IMA research
Parameters include:
Identification and scope of prescribing events
Identification and scope of dispensing events
Means by which prescription may be
transmitted from prescriber to dispensing
Defined time window after which qualifies as
non-adherent

13
Supplemental parameters Parameters that may impact the validity of IMA measurement
Impact may depend on data source, characteristics of
medication
Considerations include:
Process to ensure initial prescription is a new prescription (e.g.
360 days history)
Address potential for substitution (Therapeutic substitution, OTC
self-care)
Address potential for out-of-network prescribing/dispensing
(outside network pharmacy, cash payment) Potential for
alternate instructions to patient (e.g., ‘fill if not feeling better in
3 days’)
Considerations regarding censoring (e.g. hospitalization or death
of patient)
Ancillary parameters
Study parameters that help understand
attributes that influence IMA
Parameters include:
Patient factors: age, sex, race, health beliefs,
income, comorbidities, support network,
stated reasons for adherence/non-adherence
Non-patient factors: health system
characteristics, covered benefits, provider and
pharmacy characteristics

14
AUDIENCE INTERACTION #2: Study parameters
Consider the three classifications of parameters
(core, supplemental, ancillary)
What study parameters may go in each category?
What considerations should researchers have
when addressing these parameters?
Is there a fourth category of study parameters that
is relevant to initial medication adherence?
Recommendations for Conducting Solid IMA Research
Based upon our initial systematic review and the current deeper exploration into Methodological issues, we have developed the following set of recommendations for conducting solid IMA research:
Hutchins D, Zeber JE, Peterson AM, Roberts CS et al. Initial Medication Adherence: A Review and Analysis of Methodology: A report by the ISPOR Medication Adherence Good Research Practices Working Group [manuscript to be submitted soon to Value in Health]

15
IMA Research Recommendations
I. Use the term “initial medication
adherence”
II. State and define the specific perspective
taken (e.g., patient vs. system)
III. Delineate the core, supplemental, and
ancillary parameters that will be covered
General:
Recommendations (continued)
IV. Provide sufficient details on the prescribing
event and the procedures for determining
a new therapeutic class/initial Rx
V. Specify the timeframe between the
prescribing and dispensing event and
justify selection
Core:
16
Recommendations (continued)
Supplemental:
VI. Address perspective bias by ensuring the
comprehensiveness of information
sources
VII. Address substitution bias regardless of the
source
Recommendations (continued)
Ancillary:
VIII. Include patient characteristics information
IX. Include non-patient characteristics

17
Wrap-up and Final Issues
Summary
Final Audience Input, Questions, or Concerns
Recommended next steps and future research directions
Contact Information
David Hutchins, MHSA, MBA Senior Advisor, Pharmacy Networks
CVS Caremark - Scottsdale, AZ [email protected]
** The Working Group expresses our thanks and appreciation
to Theresa Tesoro ([email protected]) for coordinating all of
our activities, and to the two rounds of internal ISPOR
reviewers for their recent comments on the manuscript draft
summarizing this study.