a cytogenetic study of 47, xxy males of known origin and their parents
TRANSCRIPT

Ann. Hum. Genet. (1988), 52, 311)-315
Printed in areal Brifain 319
A cytogenetic study of 47,XXY males of known origin and their parents
P. A. JACOBS,* C. BACINO,? T. HASSOLD,$ N. E. MORTON,$ M. KESTONll AND M. LEE11
* Wessex Regional Cytogenetics Unit, Salisbury General Hospital, Salisbury, Wiltshire, SP2 7SX
f Department of Pediatrics, Cornell University Medical College, 1300 York Avenue, New York, N Y 10021
$ Division of Medical Genetics, Emory University School of Medicine, Atlanta, G A 30322 $ C.R.C. Research Group in Genetic Epidemiology, Department of Community Medicine,
University of Southumpton, Southampton General Hospital, Southampton, SO9 4X Y 11 M .R.C. Clinical and Population Cytogenetics Unit , Western General Hospital, Crewe Road,
Edinburgh, EH4 2XU
SUMMARY
A number of patients with both sex chromosome aneuploidy and the fragile X syndrome have been reported and this has led to the hypothesis that females heterozygous for the fragile X mutation have an increased rate of meiotic nondisjunction. Furthermore the suggestion has frequently been made that a predisposition to meiotic nondisjunction is associated with an increase in mitotic nondisjunction.
We have tested these two hypotheses by examining the chromosomes of a series of 47,XXY males and their parents. I n the majority the parental origin of the additional sex chromosome was known. The cells were cultured under conditions suitable for demonstrating the fragile X and 100 cells were scored ‘blind’ from the patients and both parents. No fragile X individual was seen and there was no difference in the proportion of aneuploid cells between the parents in whom the nondisjunction event occurred and the control parents. Therefore, our results lend no support to the suggestions that the fragile X is associated with an increase in sex chromosome aneuploidy or that individuals in whom meiotic nondisjunction occurs have an increased level of mitotic nondisjunction.
INTRODUCTION
There have been a number of reports of 47,XXY and 47,XXX individuals in families in which the fragile X syndrome is segregating. (Wilmot et al. 1980; Filippi et al. 1983; Froster- Iskenius et al. 1983; Fryns et al. 1983, 1984; Kahkonen, 1983; O’Brien et al. 1983; Schnur et al. 1986; Tommerup et al. 1986; Fuster et al. 1988). However, it is not known whether this is merely the coincidence of two not uncommon events or whether the fra(X) mutation predisposes to nondisjunction of the X chromosome in some way, perhaps by interfering with recombination. Recently there have been two reports that the association of Klinefelter’s syndrome and the fragile (X) syndrome is greater than can be expected by chance (Filippi et al. 1988; Fryns k van den Berghe, 1988).
In addition to the reported association between constitutional sex chromosome abnormalities and the fra(X) syndrome, suggesting an effect of the fra(X) mutation on chromosome
320 P. A. JACOBS AND OTHERS
segregation at meiosis, there have been two reports of an excess of X aneuploid cells in blood cultures of individuals carrying the fra(X) mutation, implying an effect of the fragile (X) gene on the segregation of the X chromosome at mitosis (Kahkonen, 1983; Brondum Nielsen, 1986).
There are also numerous reports in the literature claiming that the proportion of aneuploid cells in blood cultures of parents of individuals with trisomy (or repeated spontaneous abortions presumed to be due to trisomic conceptuses) is greater than that of controls, thus implying that mitotic aneuploidy is correlated with the production of aneuploid gametes at meiosis (Staessen et al. 1983; Hecht et al. 1984; Juberg et al. 1985).
We are studying a series of males with a 47,XXY constitution and their parents using X- linked restriction fragment-length polymorphisms (RFLPs) to determine the parent and cell division of origin of the additional X chromosome (Jacobs et al. 1988). During the course of this study we cultured the cells of the patients and their parents in conditions suitable for demonstrating the fra(X) in order to see whether we could substantiate the claim that there was an excess of fra(X) individuals among patients with Klinefelter’s syndrome. We studied both the patients and their parents because, if the fra(X) is indeed associated with an increased level of X chromosome nondisjunction at meiosis, fra( X) heterozygotes could have an increased frequency of 47,XXY sons both positive and negative for the fra(X). The fra(X) status of the 47,XXY sons will depend on the number of exchange events between the centromere and the fra(X) site at Xq28 and the cell division at which the nondisjunction takes place.
On the same cultured cells we analysed all the aneuploid metaphases in order to compare the proportion of mitotic aneuploid cells in the parent in whom the meiotic nondisjunction occurred with the proportion in the normal control parent in whom the nondisjunction event had not occurred. Thus we could directly test the hypothesis that mitotic nondisjunction dcmonstrablc in blood cultures is related to meiotic nondisjunction.
This paper reports our observations on 41 patients with Klinefelter’s syndrome and their parents. None of the patients or parents was found to carry the fra(X) and the proportion of aneuploid cells in the parents was not correlated with their status with respect to meiotic nondisjunction. However, there was a significant correlation between the proportion of aneuploid cells and the age of the patient at the time that the sample was drawn.
MATERIALS AND METHODS
The Patients
The patients were non-mosaic 47,XXY males originally seen in Edinburgh and followed in the MRC Registry of Abnormal Karyotypes. They were selected because their most recent known address was in Edinburgh or the immediate vicinity and because neither parent was known to be dead. In the event, 41 patients, 30 fathers and 38 mothers have been studied to date. The Klinefelter patients were originally ascertained in the following ways : newborn screening, 18 ; subfertility clinic, 5 ; referred because of the phenotypic features of Klinefelter’s syndrome, 18. Only 2 of the patients were considered to be mentally retarded and in only 1 was there a family history of mental retardation. The results of X-linked RFLP analysis of the parental origin of the additional X chromosome have been published for 33 patients (Jacobs et a,?. 1988) and in the remaining 8 the analyses are currently underway. The parents were

47,XX Y males and their parents 32 1
Table 1. Cytogenetic analysis of 41 males with Khefelter’8 syndrome
Age group
< I 0
10-19 20-29 30-39 40-49
= 262 f I 1.5 > 49
No. of patients
3 9 14 9 5
41
I
Total cells scored
3 1 5
930
905 505
4224
1469
I 0 0
Non-modal cells
-x I
2
14 13
5 45
I 0
+x -Y +Y 0 2 0 0 3 0
0 1
3 11
4 I4 8 4 0
5 0 2
I 17 39
+ A I
2
3 4 3
I3
0
YO
0 8
4 0 5’ I
2.7
1’2
2 1
12’0
classified as ‘yes’, ‘no’, ‘perhaps’, with regard to the nondisjunction event. In the ‘yes’ category were the parents who contributed the additional X to their 47,XXY son, in the ‘no’ category were the parents who did not contribute the additional X chromosome to their 47,XXY son, i.e. the spouses of the ‘yes’ parents, and in the ‘perhaps’ category were the parents of the 47,XXY males in whom the origin of the additional X was not known.
Cytogenetics
A heparinized blood sample was obtained from the 47,XXY males and their parents and cultured using Gibco Media F- 10 (Formula 78-5227 without hypoxanthine, thymidine and folic acid) supplemented with 5 % fetal calf serum and penicillin and streptomycin. This is the medium we use routinely for detecting the fra(X). The cells were cultured for 3 4 days, colcemid being added for the last 30 min of culture, and harvested using standard techniques. The slides were Q- or G-banded and a minimum of 100 cells scored, 50 in Edinburgh and 50 in New York. The slides were scored blind, the observer having no knowledge of the age of the patient or their status with respect to the nondisjunctional event. A minimum of 5 modal and all non-modal cells were fully analysed on every sample. All fragile sites and chromatid aberrations were recorded and any cell in which a definite or possible fragile (X) WBB seen was checked by at least one other observer.
RESULTS
The results of the cytogenetic analyses of the 47,XXY males are shown in Table 1, their fathers in Table 2 and their mothers in Table 3. No patient or parent was found to be fra(X) positive. Among the 11 262 cells scored we saw four with a chromosome that appeared to be a fra(X). One cell was in a 47,XXY male and three cells were in females. In two of the female cells there appeared to be two fra(X) chromosomes. However, as no one individual had more than a single cell with an apparent fra(X), we do not consider any to be fra(X) positive. The observation of four apparent fra(X) positive cells among 11262 scored is a similar proportion to that seen in our control samples cultured under similar conditions.
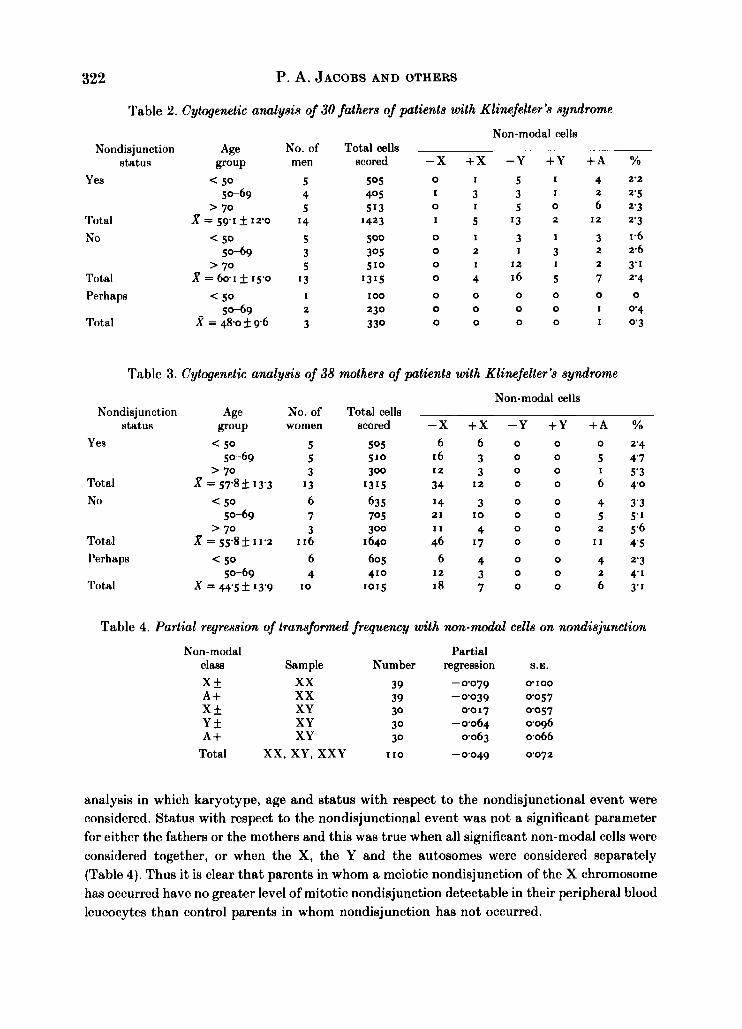
We compared the proportion of significant non-modal cells in the three classes of parents distinguished by their nondisjunctional status. We considered significant non-modal cells to be those with the gain or loss of a sex chromosome or the gain of an autosome. The great majority of cells that are lacking an autosome are technical artifacts resulting from cell breakage and therefore this category of cell was disregarded. The comparison was made using regression
322 P. A. JACOBS AND OTHERS
Table 2. Cytogenetic analysis of 30 fathers of patients with Klinefelter's syndrome Non-modal cells
Nondisjunction Age No. of Total cells status group men scored -X + X -Y +Y + A %
505 0 I 5 I 4 2'2 Yes < 50 5 5-69 4 405 I 3 3 I 2 2.5
> 70 5 513 0 I 5 0 6 2.3 Total X = 591 12.0 14 I423 I 5 '3 2 I 2 2 3
5 500 0 I 3 I 3 1.6 N O < 50 50-69 3 305 0 2 I 3 2 2.6
2 3.1 Total X = 601 f 15.0 13 1315 0 4 16 5 7 2'4
Perhaps < 50 50-69 2 230 0 0 0 0 I 0 4
Total = 48.0 f 9 6 3 330 0 0 0 0 I 0 3
> 70 5 510 0 1 I 2 I
1 I00 0 0 0 0 0 0
Table 3. Cytogenetic analysis of 38 mothers of patients with Klinefelter's syndrome
Nondisjunction status
Yes
Total N O
Total Perhaps
Total
No. of women
5 5 3
I3 6 7 3
I 16 6 4
I 0
Total cells scored
505 510 300
1315 635 705 300
I 640
605 410
1015
Non-modal cells
-X + X -Y +Y + A % o 2.4
16 3 o 0 5 4 7 I 2 3 0 0 1 5'3 34 12 0 0 6 4 0
I4 3 0 0 4 3'3 21 I 0 0 0 5 5'1
0 2 5.6 I1 4 0
6 6 0 0
46 I7 0 0 11 4 5 6 4 0 0 4 2 3
2 4 1 12 3 0 0
18 7 o 0 6 3-1
Table 4. Partial regression of transformed frequency with non-modal cells on nondisjunction
Non-modal class Sample Number X + xx 39 A + xx 39 X f XY 30 Y + XY 30 A + XY 30
Total xx, XY, XXY I I0
Partial
-0079 0100
-0039 0057 0017 0057
-0064 0096 0063 0066
- 0'049 0072
regression S.E.
analysis in which karyotype, age and status with respect to the nondisjunctional event were considered. Status with respect to the nondisjunctional event was not a significant parameter for either the fathers or the mothers and this was true when all significant non-modal cells were considered together, or when the X, the Y and the autosomes were considered separately (Table 4). Thus it is clear that parents in whom a meiotic nondisjunction of the X chromosome has occurred have no greater level of mitotic nondisjunction detectable in their peripheral blood leucocytes than control parents in whom nondisjunction has not occurred.
47,XX Y males and their parents
Table 5. Estimates of the age effect
323
Sample Total XXY XY XXY XY xx XXY XY xx
Non-modal class
A + Y f Y f X f X* X f A + , X f , Y + A + , X f , Yf A + , X f , Yf
Age effect S.E.
0018 0007 0050 0017 0023 0013 0077 0012 0017 0025 0024 0007 0063 0009 0018 0009 0024 0006
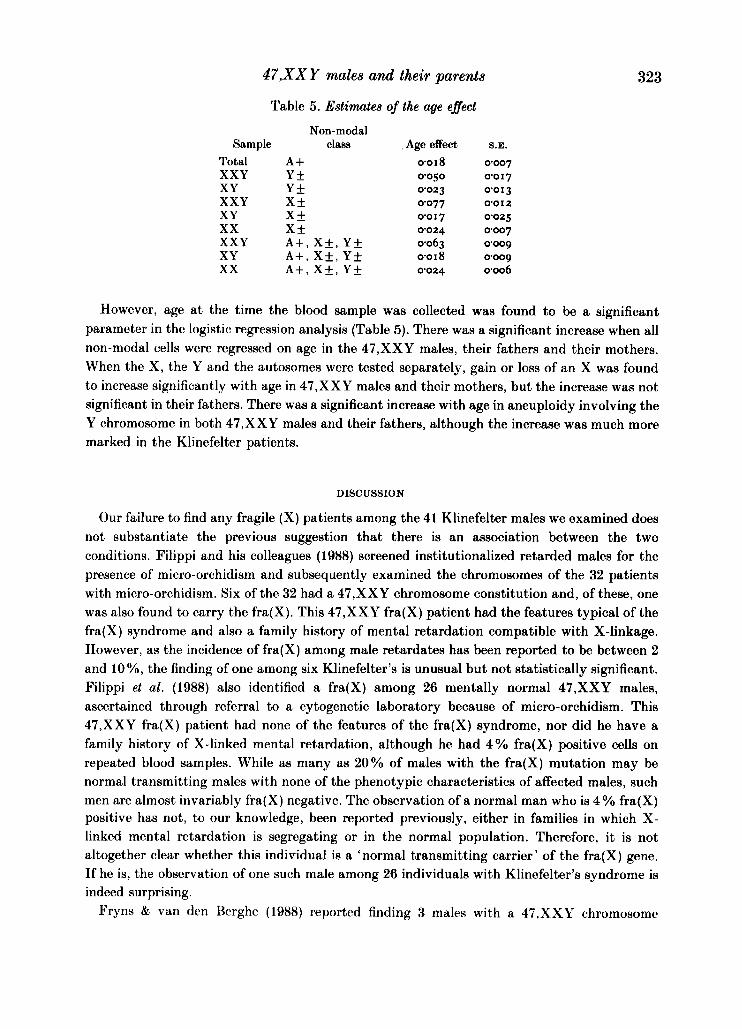
However, age a t the time the blood sample was collected was found to be a significant parameter in thc logistic regression analysis (Table 5) . There was a significant increase when all non-modal cells were regressed on age in the 47,XXY males, their fathers and their mothers. When the X, the Y and the autosomes were tested separately, gain or loss of an X was found to increase significantly with age in 47,XXY males and their mothers, but the increase was not significant in their fathers. There was a significant increase with age in aneuploidy involving the Y chromosome in both 47,XXY males and their fathers, although the increase was much more marked in the Klinefelter patients.
DISCUSSION
Our failure to find any fragile (X) patients among the 41 Klinefelter males we examined does not substantiate the previous suggestion that there is an association between the two conditions. Filippi and his colleagues (1988) screened institutionalized retarded males for the presence of micro-orchidism and subsequently examined the chromosomes of the 32 patients with micro-orchidism. Six of the 32 had a 47,XXY chromosome constitution and, of these, one was also found to carry the fra(X). This 47,XXY fra(X) patient had the features typical of the fra( X) syndrome and also a family history of mental retardation compatible with X-linkage. However, as the incidence of fra(X) among male retardates has been reported to be between 2 and 10 %, the finding of one among six Klinefelter’s is unusual but not statistically significant. Filippi et al. (1988) also identified a fra(X) among 26 mentally normal 47,XXY males, ascertained through referral to a cytogenetic laboratory because of micro-orchidism. This 47,XXY fra(X) patient had none of the features of the fra(X) syndrome, nor did he have a family history of X-linked mental retardation, although he had 4% fra(X) positive cells on repeated blood samples. While as many as 20% of males with the fra(X) mutation may be normal transmitting males with none of the phenotypic characteristics of affected males, such men are almost invariably fra(X) negative. The observation of a normal man who is 4 % fra(X) positive has not, to our knowledge, been reported previously, either in families in which X- linked mental retardation is segregating or in the normal population. Therefore, it is not altogether clear whether this individual is a ‘normal transmitting carrier’ of the fra(X) gene. If he is, the observation of one such male among 26 individuals with Klinefelter’s syndrome is indeed surprising.
Pryns & van den Berghe (1988) reported finding 3 males with a 47.XXY chromosome
324 P. A. JACOBS AND OTHERS
constitution among 465 fra(X) males. While this frequency (06%) is much higher than the general population frequency of approximately 005%, it is not different from the reported frequency of 0.9% of 47,XXY males among the mentally retarded (Court Brown, 1968). As the great majority of the studied fra(X) males were presumably retarded, the observation of 3 in 465 is no greater than expected by chance.
Both XXY and fra(X) predispose to mental retardation, and their cumulative effect is problematical. It would not be surprising if the frequency of males with both abnormalities were higher among institutionalized cases than among retardates in the general population. Therefore, in samples selected in part through retardation, it is difficult to detect or interpret a small excess of fra(X) among XXY and vice versa. When compared with frequencies observed in mentally retarded populations, the reported association of XXY and fra(X) is not significant, and so the hypothesis that fra(X) predisposes to meiotic nondisjunction of the X chromosome is unsubstantiated.
In a blind, controlled study we failed to find any excess of non-modal cells, and specifically cells with the gain or loss of a sex chromosome, in the blood of the parent in whom the nondisjunctional event occurred to produce the Klinefelter offspring. Therefore, our observations lend no support to the suggestion that mitotic nondisjunction demonstrable in blood cultures is related to meiotic nondisjunction leading to aneuploid offspring.
However, we did find a strong correlation between the gain or loss of a sex chromosome and age at the time the blood sample was obtained both in the Klinefelter patients and their parents, thus confirming the well-established association between increasing age and aneuploid cells in blood cultures (Abruzzo et al. 1985).
This work was supported by grant HD21341 from the National Institutes of Health. Dr Bacino is the recipient of a Norman and Rosita Winston Foundation Fellowship in Biomedical Research.
REFERENCES
ABRUZZO, M. A., MAYER, M. & JACOBS, P. A. (1985). Aging and aneuploidy: evidence for the preferential involvement of the inactive X chromosome. Cytogenet. Cell Genet. 39, 275-278.
BRONDUM NIELSEN, K. (1986). Sex chromosome aneuploidy in fragile X carriers. Am. J. Med. Genet. 23, 537-544.
COURT BROWN, W. M. (1968). Sex chromosome aneuploidy in man and its frequency, with special reference to mental subnormality and criminal behaviour. Int. Rev. Exp. Path. 7 , 31-97.
FILIPPI, G., PECILE, V., RINALDI, A. & SINISCALCO, M. (1988). Fragile X mutation and Klinefelter syndrome: a reappraisal. Am. J. Med. Genet. (In the press.)
FILIPPI, G., RINALDI, A., ARCHIDIACONO, N., ROCCHI, M., BALAZS, I. & SINISCALCO, M. (1983). Linkage between G6PD and fragile X syndrome. Am. J. Med. Genet. 15, 113-119.
FROSTER-ISKENIUS, U., FELSCH, G., SCHIRREN, C. & SCHWINQER, E. (1983). Screening for the fra(X)(q) in a population of mentally retarded males. Hum. Genet. 60, 153-157.
FRYNS, J. P., KLECZKOWSKA, A., KUBIEN, E., PETIT, P., HASPESLAQH, M., L ~ D E M A N S , I. & VAN DEN BEROHE, H. (1983). XY/XXY mosaicism and fragile X syndrome. Ann. Ge‘ne’t. 26, 251-253.
FRYNS, J. P., KLECZKOWSKA, A., WOLFS, I. & VAN DEN BERQHE, H. (1984). Klinefelter syndrome and two fragile X chromosomes. Clin. Genet. 26, 445-447.
FRYNS, J. P. & VAN DEN BEROHE, H. (1988). The concurrence of Klinefelter syndrome and fragile X syndrome. Am. J. Med. Genet. (In the Press.)
FUSTER, C., TEMPLADO, C., MIRO, R., BARRIOS, L. & EQOZCIJE, J. (1988). Concurrence of the triple X syndrome and expression of the fragile site Xq27.3. Hum. Genet. 78, 293.
HECHT, F., HECHT, B. K. & BEROER, C. S. (1984). Aneuploidy in recurrent spontaneous aborters the tendency to parental non-disjunction. Clin. Genet. 26, 4346.
JACOBS, P. A., HASSOLD, T. J., WHITTINOTON, E., BUTLER, G., COUYER, S., KESTON, M. & LEE, M. (1988). Klinefelter’s syndrome: an analysis of the origin of the additional sex chromosome using molecular probes. Ann. Hum. Genet. 52, 93-109.
47,XX Y males and their parents 325
JUBERO, R. C., KNOPS, J. & MOWREY, P. N. (1985). Increased frequency of lymphocytic mitotic non-disjunction
KAHKONEN, M. (1983). Marker X associated mental retardation. Observations of the X chromosome. Clin.
O’BRIEN, M. M., PADRE-MENDOZA, T. & PUESCHEL, S. M. (1983). Maternal non-disjunction of fragile X
SCHNUR, R. E., LEDBETTER, D. H. & NUSSBAUM, R. L. (1986). A family with a 47,XXY plus fragile X at
STAESSEN, C., MAES, A. M., KIRSCH-VOLDERS, M. & SUSANNE, C. (1983). Is there a predisposition for meiotic
TOMMERUP, N., TBNNESEN, T. & GUSTAVSON, K.-H. (1986). Paternal non-disjunction in a 46,XY/47,XXY
WILMOT, P. L., SHAPIRO, L. R. & DUNCAN, P. A. (1980). The Xq27 fragile site and 47,XXY. Am. J. Hum. Genet.
in recurrent spontaneous aborters. J. Med. Genet. 22, 32-35.
Genet. 23, 234-235A.
chromosome resulting in Klinefelter syndrome. Am. J. Hum. Genet. 35, 146A.
Xq27.3 due to paternal non-disjunction. Am. J. Hum. Genet. Supplement 39, A100.
non-disjunction that may be detected by mitotic hyperploidy? Clin. Genet. 24, 184-190.
individual with a fragile 1 7 ~ 1 2 in the mother. Clin. Genet. 30, 7&79.
32, 94A.