a comparison of the performance characteristics of classification criteria for the diagnosis of...
TRANSCRIPT
ACAWK
*†‡§�
F
D
A
0d
Comparison of the Performance Characteristics oflassification Criteria for the Diagnosis of Psoriaticrthritisilliam J. Taylor, MBChB, FRACP,* Antonio Marchesoni, MD,† Marco Arreghini, MD,‡
atharina Sokoll, MD,§ and Philip S. Helliwell, DM, PhD�
OBJECTIVE To compare the accuracy of published classification criteria for the diagnosis ofpsoriatic arthritis (PsA) and to see whether data-derived classification criteria would bemore accurate.METHODS Data were abstracted from case-note review and radiographic review of patientsidentified with PsA or rheumatoid arthritis (RA) from 2 clinical disease registers. Eachpatient was classified according to 7 criteria sets. The test performance characteristicswere compared using conditional logistic regression analysis. In an attempt to overcomethe problems of the diagnostic gold standard, latent class analysis also was used tocalculate test-performance characteristics. Classification and regression-tree methodologywas used to derive new criteria and to indicate the diagnostic importance of particular dataitems, especially rheumatoid factor (RF).RESULTS Four hundred ninety-nine patients were identified with RA (n � 156) or PsA (n �343). Excluding the criteria of Fournie, which could not be applied in 24% of subjects, 446cases could be classified by all of the other 6 methods. The most sensitive criteria for thediagnosis of PsA were those of Vasey and Espinoza, McGonagle, and Gladman (99%),whereas the others were significantly less sensitive (between 56% and 94%). The speci-ficity of the criteria was high and statistically similar (between 93% and 99%). The Fourniecriteria were the most difficult to use, whereas the Vasey and Espinoza and Moll and Wrightcriteria were the easiest (98% of subjects were able to be classified). A 2-latent class modelfound very similar test-performance characteristics. Logistic regression and classificationand regression-tree models suggested that negative RF was not necessary for diagnosis inthe presence of other characteristic features of PsA.CONCLUSIONS Apart from the Bennett and European Spondyloarthropathy Study Group crite-ria, which have inadequate sensitivity, the published classification criteria for PsA havesimilar test-performance characteristics. These data suggest that the criteria proposed byVasey and Espinoza, Gladman, or McGonagle are the most accurate and feasible indistinguishing between PsA and RA.
Research Fellow, Rheumatology and Rehabilitation Research Unit, University of Leeds, United Kingdom.Contract Professor in Rheumatology, U.O. Di Reumatologia, Istituto Ortopedico G. Pini, Milano, Italy.Research Fellow, U.O. Di Reumatologia, Istituto Ortopedico G. Pini, Milano, Italy.Senior Registrar in Rheumatology, Department of Rheumatology, St. Luke’s Hospital, Bradford, United Kingdom.Senior Lecturer in Rheumatology, Rheumatology and Rehabilitation Research Unit, University of Leeds, Leeds, United Kingdom and Department of Rheuma-
tology, St. Luke’s Hospital, Bradford, United Kingdom.rom the Rheumatology and Rehabilitation Research Unit, University of Leeds, Leeds, United Kingdom; U.O. Di Reumatologia, Istituto Ortopedico G. Pini,
Milano, Italy; and the Department of Rheumatology, St. Lukes Hospital, Bradford, United Kingdom.r. Taylor was the recipient of the Dorothy Eden Fellowship of the Arthritis Foundation of New Zealand and the Arthritis Research Campaign during this study
(Grant Number T0520).ddress reprint requests to Dr. William Taylor, Department of Medicine, Wellington School of Medicine and Health Sciences, University of Otago, PO Box 7343,
Wellington, New Zealand. E-mail: [email protected].
575049-0172/04/$-see front matter © 2004 Elsevier Inc. All rights reserved.oi:10.1016/j.semarthrit.2004.05.001

Doohctmiocwthtd
rmsttawattPhfBsdswpoespqjvMoWta
576 W.J. Taylor et al.
RELEVANCE International agreement about classification criteria for PsA will assist the inter-pretation of clinical and epidemiologic research. However, further prospective studies onunselected patients with and without PsA, including controls with non–rheumatoid inflam-matory arthritis, are required to confirm these findings.
Semin Arthritis Rheum 34:575-584 © 2004 Elsevier Inc. All rights reserved.
KEYWORDS psoriatic arthritis, classification criteria
menP
drttsscaptm
oeddoantpetaid
Pvpddafls
atdpr
espite the recognition that psoriatic arthritis (PsA) is adistinct disease, clinical and basic research into this dis-
rder often is confounded by the absence of a widely agreedr validated case definition (1). Several classification criteriaave been proposed and used in the literature, but it is un-lear which of these best represents “true” PsA. The opera-ional definitions of these criteria are listed in Table 1. Rheu-atologists in practice appear to exhibit substantial variation
n how PsA is diagnosed (2). This is problematic for a numberf reasons. Clinicians are unable to apply the results fromlinical research to their own patients, when it is unclearhether the subjects of research have the same condition as
heir own patients. Clinical research is muddied by includingeterogeneous study populations and prognostic or interven-ion trials will be difficult to interpret when patients withifferent diseases are included.Moll and Wright (3) made seminal contributions to the
ecognition that PsA is a distinct disease, different from rheu-atoid arthritis (RA) and ankylosing spondylitis, but sharing
imilar features of each. Their case definition of PsA remainshe most widely quoted. Although Moll and Wright’s defini-ion actually specified that rheumatoid factor (RF) be “usuallybsent,” it is unclear how frequent “usually” means and underhich circumstances RF positivity is permitted. We chose to
dopt a conservative interpretation to contrast this approacho other, more permissive approaches to RF. Bennett (4) felthat the Moll and Wright criteria were likely to overdiagnosesA and suggested more rigorous diagnostic criteria. Theseave been used in a single clinical study (5), without evidenceor their discriminant validity. We suggest modifications ofennett’s original criteria, primarily because the inclusion ofynovial biopsy and synovial fluid analysis render the caseefinition impractical for clinical use or epidemiologic re-earch. We also modified the item regarding erosive changeithout periarticular osteopenia, because the recognition oferiarticular osteopenia is known to be subject to excessivebserver error (6). We substituted “joint osteolysis” or “DIProsive arthritis” for this item (7). Vasey and Espinoza (8)implified the Bennett rule, but recognized that there are 2rinciple manifestations of PsA. Thus, only 2 criteria are re-uired: psoriasis and 1 manifestation of either peripheral
oint disease or spinal disease. This rule has neither beenalidated nor used in any published study catalogued byEDLINE. Gladman’s group from Toronto published several
bservational studies on PsA (9-11). They modified Moll andright’s rule principally to allow RF positivity, recognizing
hat RF occurs in about 4% (12) of the general population
nd that there was no known reason why cases with PsAight not have coincidental RF. The definition does, how-ver, specify exclusion criteria so that these alternative diag-oses would appear to take precedence over the diagnosis ofsA. The possibility of coexistent disease is excluded.The European Spondyloarthropathy Study Group (ESSG)
erived classification criteria from consecutive patients withheumatologist-diagnosed spondyloarthropathy and con-rols with other rheumatic diseases (13). Although the inten-ion of the criteria was for the diagnostic classification of thepondyloarthropathy group as a whole, particular types ofpondyloarthropathy can be identified from the publishedlassification criteria, including PsA. For the first time, it islso recognized that PsA actually can occur in the absence ofsoriasis. Cases in which arthritis precedes skin manifesta-ions are well recognized, so that a family history of psoriasisay be the only indication of a psoriasis association at onset.Recently, it was proposed that the pathology of PsA (and
ther spondyloarthropathies) is fundamentally located at thenthesis. Manifestations of enthesitis are thus proposed toistinguish spondyloarthropathies from RA. This model ofisease led McGonagle et al (14) to a definition of PsA basedn enthesopathy. There is a significant problem with evalu-ting the original McGonagle criteria set because of the mag-etic resonance imaging (MRI) requirements. It is unlikelyhat MRI would be practical for epidemiologic research pur-oses. It is also likely that the MRI appearances in well-stablished disease would show features of both enthesiopa-hy and synovitis so that the discriminant value is markedlyttenuated. It has been suggested that plain radiographic ev-dence of enthesitis might be more useful in well-establishedisease (McGonagle, personal communication, March 2000).The only diagnostic rule specifically aimed at diagnosing
sA that has been derived from actual patient data was de-eloped by Fournie et al (15). It has yet to be tested in otheropulations. The items and weighting were selected usingiscriminant function and logistic regression analysis. It waserived from a population of PsA, ankylosing spondylitis,nd RA from a single clinic. A score of 11 points is requiredor the diagnosis of PsA (sensitivity, 95%, specificity, 98%;ikelihood ratio for a positive test result, 47.5). The authorsuggest that validation in other centers is now required.
There are thus 7 different methods of diagnosing PsA. Theim of this study was to determine which classification washe most accurate and most feasible for clinical research. Too this, we analyzed existing data from clinical databases ofatients with PsA and RA, their case records, and availableadiographs from these patients.
In addition, we postulated that a classification rule derived

ftd
MPbGdego
riddsarrpdoe
T
G
M
F
E
B
M
V
*
†
Classification criteria of psoriatic arthritis 577
rom the data themselves and tested against a subsample ofhe data would be more accurate than any of the theoreticallyerived rules.
aterials and Methodsatients with RA or PsA were identified from clinical data-ases at St. Luke’s Hospital, Bradford, United Kingdom, and. Pini Orthopaedic Institute, Milan, Italy. All available ra-iographs and case notes were reviewed and data items werextracted to enable classification by each method. Radio-raphic features were defined using the definitions devel-
able 1 Operational Definitions of Each Classification Criteri
ladman [current psoriasis, history of pssacroiliitis or inflammatory sposteoarthritis, reactive arthriti
cGonagle (modified) [current psoriasis, history of pspain, anterior chest wall pain,erosion, ankylosis, juxta-articuossification, romanus lesion,entheseal insertion; finger DIPsacroiliitis; any of: SAPHO, speriostitis, chronic recurrent minvolved joints is <5]
ournie A score >10 derived from the fAND [onset of psoriasis befornegative] AND {[family history[current psoriasis, history of pscore 3; [inflammatory thoracinvolved joints less than 5], senthesis pain], score 2; [radioarticular new bone formation,negative], score 4.
If a score for any item could noassigned the score. If the sum>10, the case was deemed to
SSG [current psoriasis, history of ps[predominant lower limb arthr
ennett (modified) [current psoriasis or nail diseasfeatures: [1 or more other inv[negative RF], [radiographic josyndesmophytes, or paraverte
If a score (for any of the 8 suppdata, a dummy variable was amissing scores plus actual scmissing, the case was deeme
oll and Wright [current psoriasis, history of pssacroiliitis or inflammatory sp
asey and Espinoza [current psoriasis, history of psasymmetry, [symmetry] ANDosteolysis, tuft erosion, ankyldisease, or radiographic sacro
Asymmetry defined as number of matched involved joint pairs > n(shoulder, elbow, wrist, MCPs, PIPs, DIPs, hip, ankle, MTPs, to
Predominant lower-limb arthritis defined as number of involved loweupper limb joints (shoulder, elbow, wrist, MCPs, PIPs, DIPs).
ped by an earlier observer reliability study (7). Data were l
ecorded onto standardized forms and included demograph-cs (ethnicity, gender, age), psoriasis (whether currently evi-ent or previously observed, nail involvement), onset of skinisease and arthritis, dactylitis, chest wall pain, diffuse enthe-is pain, inflammatory heel pain, clinical sacroiliitis, swollennd tender joint examination findings, family history of pso-iasis, inflammatory spinal pain or stiffness (lumbar, tho-acic, and cervical), clinical enthesopathy, RF, elevated acute-hase reactant, HLA typing (if available), extra-articularisease, rheumatoid nodules, primary clinical diagnosis,ther rheumatic diseases, number of joint surgeries, and dis-ase treatment. The precise definitions of each clinical, radio-
, or nail disease] AND [inflammatory joint disease, clinicalsease] AND NOT [rheumatoid nodules, grade 4eropathic arthritis, gout, or systemic lupus erythmatosus]
or family history of psoriasis] AND [inflammatory heelender enthesis; any of these radiographic features, tuftw bone formation, syndesmophytes, paravertebraln at an entheseal insertion, new bone formation at aninvolvement, inflammatory spinal symptoms, clinical
lodiscitis, arthritis mutilans, onycho-pachydermo-cal recurrent osteomyelitis; dactylitis, or number of
ng: [current psoriasis, history of psoriasis or nail disease]oncomitant with joint symptoms], score 6; [first item isoriasis] or ([onset of psoriasis after joint symptoms] ANDis, or nail disease])}, score 3; [finger DIP involvement],ervical symptoms], score 3; [asymmetry]* AND [number of; [clinical sacroiliitis, heel pain, chest wall pain, or diffusel changes-DIP erosion, joint osteolysis, ankylosis, juxta-t erosion], score 5; [HLA B16 or B17], score 6; [RF
etermined because of missing data, a dummy variable wasmmy variables for missing scores plus actual scores wasinsufficient data to classify., family history of psoriasis, or nail disease] AND
asymmetry, or inflammatory spinal disease]D [at least 1 involved joint] AND 5 of the following 8joint], [dactylitis], [asymmetry], [absence of nodules],teolysis or DIP erosive change], [radiographic sacroiliitis,ssification]features) could not be determined because of missingd the score of 1. If the sum of the dummy variables foras >4, or either of the 2 mandatory features were
ave insufficient data to classify., or nail disease] AND [inflammatory joint disease, clinicalsease] AND NOT [RF positive], or nail disease] AND [finger DIP involvement, dactylitis,gative] AND [absence of nodules], [radiographicr juxta-articular new bone formation], inflammatory spinal
of nonmatched involved joint pairs when 11 joint pairs considered
joints (hip, knee, ankle, tarsus, MTPs, toe IPs) > number of involved
a
oriasisinal dis, entoriasisany tlar ne
erosiojoint
pondyultifo
ollowie or cof ps
soriasic or ccore 1logicaor tuf
t be dof duhave
oriasisitis,†e] ANolvedint osbral oortivessigneores wd to horiasisinal dioriasis[RF neosis, oiliitis]
umbere IPs).r-limb
ogic, and laboratory item are available from the authors. All

ts
wfeCaot
spnfPctwtttfawp
tcytossu
fimttspoctftC
wrrcctstow
RT(iy
(tpsdihcrtpp49avjn0
pltls
snnww(mcmspz
T
AD
SR
578 W.J. Taylor et al.
ogether, information on 50 variables was collected. Table 1hows how each classification method was operationalized.
The overall discriminant validity of each potential featureas assessed using the specificity and sensitivity of each item
or the diagnosis of PsA, and the independent contribution ofach feature was assessed using logistic regression models.ases with missing data items were included in the regressionnalysis by categorizing each variable as “present,” “absent,”r “missing.” The odds ratios presented are with reference tohe “absent” state.
We chose 2 methods of determining the diagnostic “goldtandard,” against which the rules were to be tested. Experthysician diagnosis is the traditional standard when there iso pathognomic feature. All patients had received a diagnosisrom highly experienced rheumatologists with an interest insA. The second method employed the technique of latentlass analysis (LCA) (16). This statistical approach assumeshat each rule classifies patients into the same classes, albeitith different errors. It is also assumed that agreement be-
ween the classes identified by each rule is mediated only byhe underlying true status of the patient. This method is ableo specify a model so that the error rates (false-positive andalse-negative results) or response probabilities (sensitivitynd specificity) of each rule within the model can be derivedithout actually knowing the true classification state of theatient. PANMARK version 3 was used for the LCA.Among the subjects that could be classified by every rule,
he specificity and sensitivity of each classification rule wasompared using forward conditional logistic regression anal-sis. The classification method (rule) was regressed againsthe result of the rule (positive or negative) separately for casesf PsA (comparing sensitivity) and RA controls (comparingpecificity). In this analysis, the definition of case or controltatus was by clinic diagnosis. SPSS software (version 10) wassed for this analysis.Data-derived classification rules were derived using classi-
cation and regression tree (CART) analysis (17). Thisethod of recursive partitioning iteratively selects variables
hat split the sample into progressively purer groups. It has aheoretical advantage to techniques such as logistic regres-ion, in that the structure of the classes in relation to theredictor variables is not assumed, ie, different combinationsf the predictor variables may identify subgroups within eachlass. For instance, axial features are likely to be more impor-ant for PsA with predominant axial disease and peripheraleatures less important. CART is potentially able to uncoverhis structure. Second, when a splitting variable is missing,
able 2 Patient Characteristics
PsA (n � 343) RA (n � 156)
ge, y (SD) 48.0 (14.6) 54.8 (13.0)isease duration,y (SD) 9.9 (7.8) 10.2 (9.0)
ex (% male) 64% 17%F positive (%) 5% 78%
ART is able to specify surrogate predictors at each node, 8
hich minimizes the impact of missing data. Testing of theule uses the technique of v-fold cross-validation whereby vandom samples of the data are used to grow trees that areompared with a tree grown from the entire data set. Typi-ally, a 10-fold cross-validation procedure is used. To assesshe importance of particular features in the diagnosis of PsA,everal models were derived. In particular, trees were grownhat included all variables, without psoriasis items and with-ut RF. CART for Windows (Salford Systems) version 4.0as used for this analysis (18).
esultshere were 499 patients identified from the clinical database343 with PsA, 156 with RA). The disease duration was sim-lar between each disease group, but patients with PsA wereounger and more likely to be male (Table 2).
The discriminant value of laboratory and clinical featuresTable 3) and radiologic features (Table 4) are expressed inerms of sensitivity and specificity. Sensitivity refers to theroportion of patients with PsA who have the feature, andpecificity refers to the proportion of patients with RA whoo not have the feature. The multivariate analysis shown
ncluded all the listed variables, but because the effect ofaving psoriasis was so dominant, models that did not in-lude history of psoriasis or current psoriasis also were de-ived. These showed that when just the clinical and labora-ory features are considered without inclusion of a history ofsoriasis or current psoriasis, the following variables inde-endently contribute to the diagnosis (model chi-square,30; P � .001, R2 � .578): dactylitis (odds ratio [OR], 14;5% confidence interval [CI], 3-69), family history of psori-sis (OR, 13; 3-58), finger distal interphalangeal (DIP) in-olvement (OR, 3; 1-9), �4 metacarpophalangeal (MCP)oints involved (OR, 3; 1-7), lumbar stiffness (OR, 12; 2-75),ail dystrophy (OR, 67; 8-578), RF positive (OR, 0.04;.016-0.089).These 7 features and the 3 radiologic features that inde-
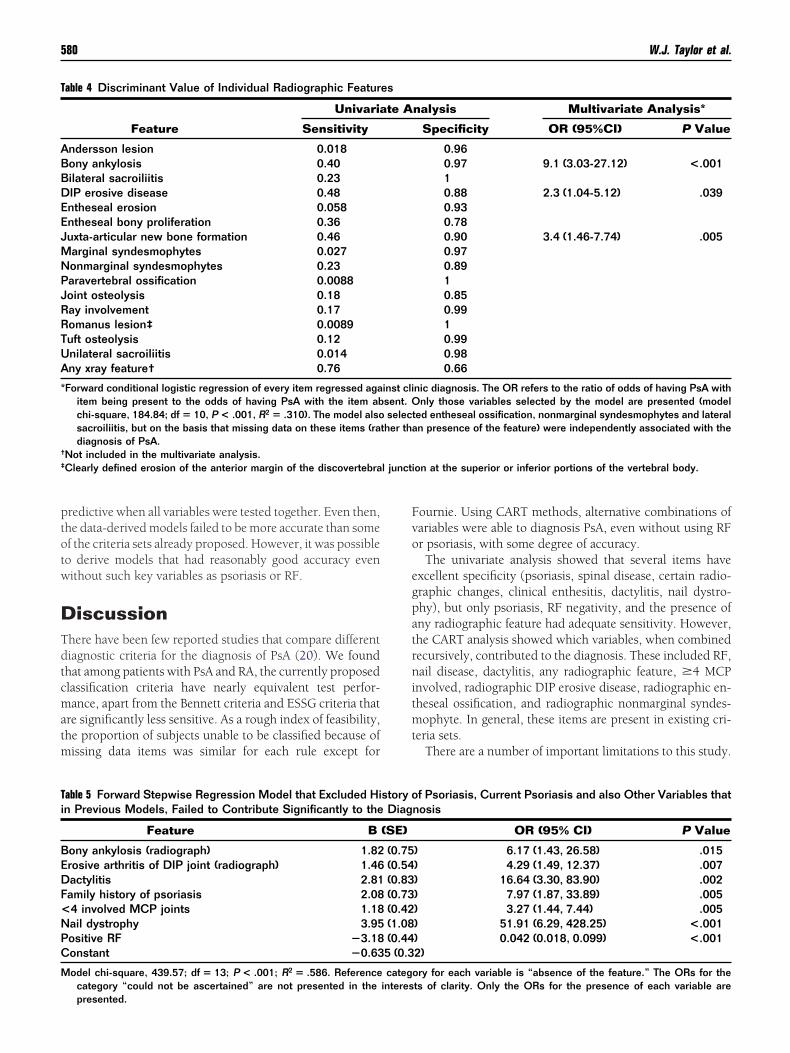
endently contributed to the diagnosis of PsA (bony anky-osis, DIP erosive disease, juxta-articular new bone forma-ion; see Table 4) were entered into another forward stepwiseogistic regression model and the details of this model arehown in Table 5.
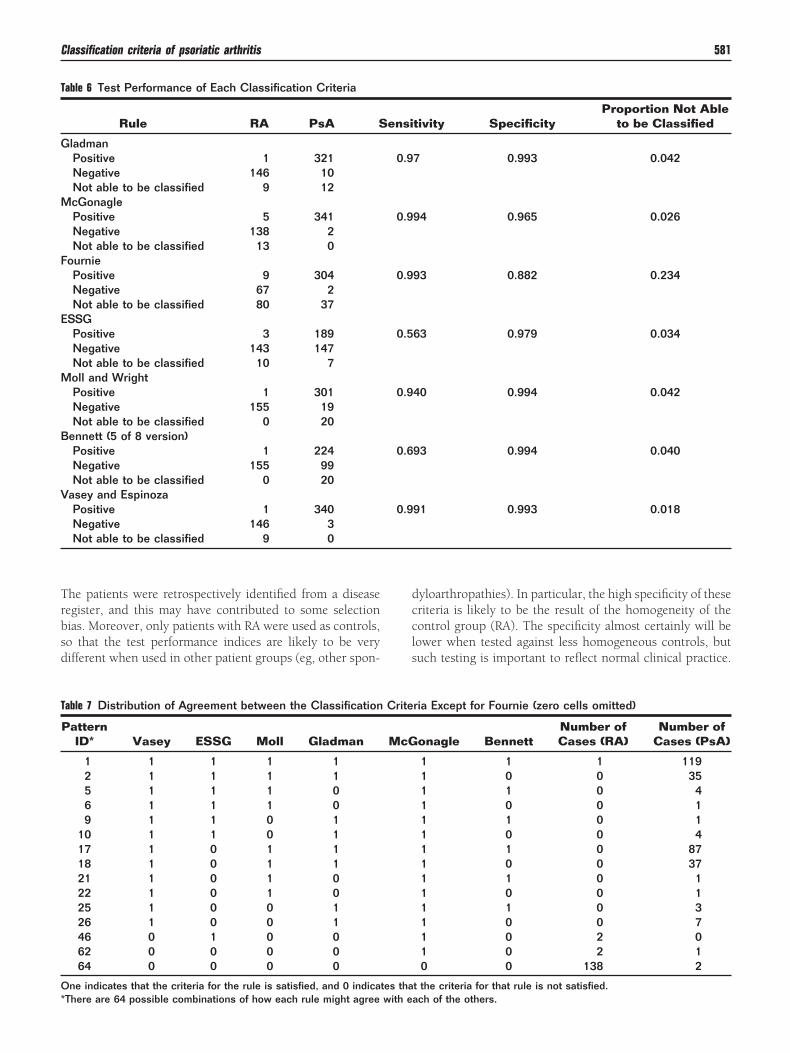
The performance of each rule is shown in Table 6. Becauseome patients could not be classified by every method, theumbers of patients classed as PsA and RA as well as thoseot able to be classified are expressed. The method of Fournieas the most difficult to use, primarily because HLA dataere not retrospectively available from the clinical records
only 77% of subjects could be classified by the Fournieethod). Excluding the Fournie rule, 446 patients (89%)
ould be classified by all of the other 6 methods. The agree-ent pattern between these 6 rules for these patients is
hown in Table 7. With 6 rules, there are 26 � 64 differentossible combinations. Only those combinations with non-ero counts are tabulated.
A 2-latent class model fitted these data adequately (Table
) and found similar performance characteristics of the rules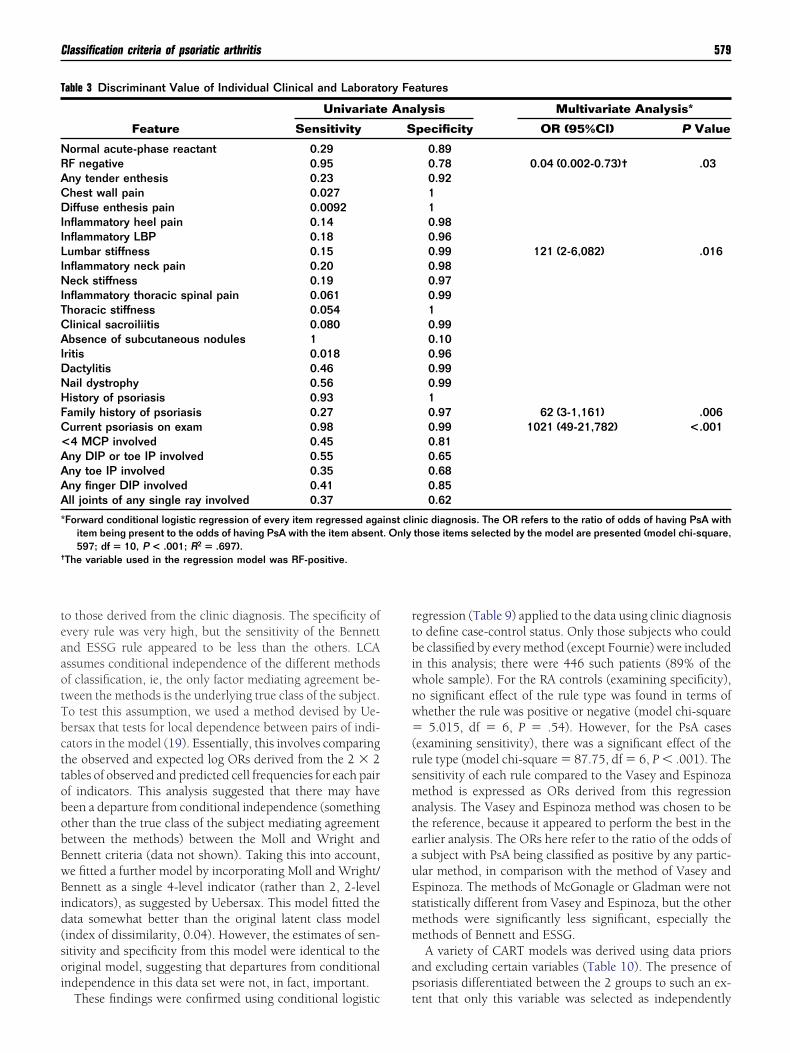
teaaotTbcttobobBwBid(soi
rtbiwnw�(rsmateauEsmm
ap
T
NRACDIILINITCAIDNHFC<AAAA
*
†
Classification criteria of psoriatic arthritis 579
o those derived from the clinic diagnosis. The specificity ofvery rule was very high, but the sensitivity of the Bennettnd ESSG rule appeared to be less than the others. LCAssumes conditional independence of the different methodsf classification, ie, the only factor mediating agreement be-ween the methods is the underlying true class of the subject.o test this assumption, we used a method devised by Ue-ersax that tests for local dependence between pairs of indi-ators in the model (19). Essentially, this involves comparinghe observed and expected log ORs derived from the 2 � 2ables of observed and predicted cell frequencies for each pairf indicators. This analysis suggested that there may haveeen a departure from conditional independence (somethingther than the true class of the subject mediating agreementetween the methods) between the Moll and Wright andennett criteria (data not shown). Taking this into account,e fitted a further model by incorporating Moll and Wright/ennett as a single 4-level indicator (rather than 2, 2-level
ndicators), as suggested by Uebersax. This model fitted theata somewhat better than the original latent class modelindex of dissimilarity, 0.04). However, the estimates of sen-itivity and specificity from this model were identical to theriginal model, suggesting that departures from conditionalndependence in this data set were not, in fact, important.
able 3 Discriminant Value of Individual Clinical and Laborat
Feature
Univariat
Sensitivity
ormal acute-phase reactant 0.29F negative 0.95ny tender enthesis 0.23hest wall pain 0.027iffuse enthesis pain 0.0092
nflammatory heel pain 0.14nflammatory LBP 0.18umbar stiffness 0.15nflammatory neck pain 0.20eck stiffness 0.19
nflammatory thoracic spinal pain 0.061horacic stiffness 0.054linical sacroiliitis 0.080bsence of subcutaneous nodules 1
ritis 0.018actylitis 0.46ail dystrophy 0.56istory of psoriasis 0.93amily history of psoriasis 0.27urrent psoriasis on exam 0.984 MCP involved 0.45ny DIP or toe IP involved 0.55ny toe IP involved 0.35ny finger DIP involved 0.41ll joints of any single ray involved 0.37
Forward conditional logistic regression of every item regressed agaitem being present to the odds of having PsA with the item absent597; df � 10, P < .001; R2 � .697).
The variable used in the regression model was RF-positive.
These findings were confirmed using conditional logistic t
egression (Table 9) applied to the data using clinic diagnosiso define case-control status. Only those subjects who coulde classified by every method (except Fournie) were included
n this analysis; there were 446 such patients (89% of thehole sample). For the RA controls (examining specificity),o significant effect of the rule type was found in terms ofhether the rule was positive or negative (model chi-square
5.015, df � 6, P � .54). However, for the PsA casesexamining sensitivity), there was a significant effect of theule type (model chi-square � 87.75, df � 6, P � .001). Theensitivity of each rule compared to the Vasey and Espinozaethod is expressed as ORs derived from this regression
nalysis. The Vasey and Espinoza method was chosen to behe reference, because it appeared to perform the best in thearlier analysis. The ORs here refer to the ratio of the odds ofsubject with PsA being classified as positive by any partic-lar method, in comparison with the method of Vasey andspinoza. The methods of McGonagle or Gladman were nottatistically different from Vasey and Espinoza, but the otherethods were significantly less significant, especially theethods of Bennett and ESSG.A variety of CART models was derived using data priors
nd excluding certain variables (Table 10). The presence ofsoriasis differentiated between the 2 groups to such an ex-
atures
lysis Multivariate Analysis*
pecificity OR (95%CI) P Value
0.890.78 0.04 (0.002-0.73)† .030.92110.980.960.99 121 (2-6,082) .0160.980.970.9910.990.100.960.990.9910.97 62 (3-1,161) .0060.99 1021 (49-21,782) <.0010.810.650.680.850.62
nic diagnosis. The OR refers to the ratio of odds of having PsA withthose items selected by the model are presented (model chi-square,
ory Fe
e Ana
S
inst cli. Only
ent that only this variable was selected as independently
ptotw
DTdtcmatm
Fvo
egpatrnitmt
T
ABBDEEJMNPJRRTUA
*
†
‡ l juncti
Ti
BEDF<NPC
M
580 W.J. Taylor et al.
redictive when all variables were tested together. Even then,he data-derived models failed to be more accurate than somef the criteria sets already proposed. However, it was possibleo derive models that had reasonably good accuracy evenithout such key variables as psoriasis or RF.
iscussionhere have been few reported studies that compare differentiagnostic criteria for the diagnosis of PsA (20). We foundhat among patients with PsA and RA, the currently proposedlassification criteria have nearly equivalent test perfor-ance, apart from the Bennett criteria and ESSG criteria that
re significantly less sensitive. As a rough index of feasibility,he proportion of subjects unable to be classified because ofissing data items was similar for each rule except for
able 4 Discriminant Value of Individual Radiographic Featur
Feature
Univaria
Sensitivity
ndersson lesion 0.018ony ankylosis 0.40ilateral sacroiliitis 0.23IP erosive disease 0.48ntheseal erosion 0.058ntheseal bony proliferation 0.36uxta-articular new bone formation 0.46arginal syndesmophytes 0.027onmarginal syndesmophytes 0.23aravertebral ossification 0.0088oint osteolysis 0.18ay involvement 0.17omanus lesion‡ 0.0089uft osteolysis 0.12nilateral sacroiliitis 0.014ny xray feature† 0.76
Forward conditional logistic regression of every item regressed agaitem being present to the odds of having PsA with the item abchi-square, 184.84; df � 10, P < .001, R2 � .310). The model alsosacroiliitis, but on the basis that missing data on these items (radiagnosis of PsA.
Not included in the multivariate analysis.Clearly defined erosion of the anterior margin of the discovertebra
able 5 Forward Stepwise Regression Model that Excluded Hin Previous Models, Failed to Contribute Significantly to the
Feature B
ony ankylosis (radiograph) 1.82rosive arthritis of DIP joint (radiograph) 1.46actylitis 2.81amily history of psoriasis 2.084 involved MCP joints 1.18ail dystrophy 3.95ositive RF �3.18onstant �0.63
odel chi-square, 439.57; df � 13; P < .001; R2 � .586. Referencecategory “could not be ascertained” are not presented in the
presented.ournie. Using CART methods, alternative combinations ofariables were able to diagnosis PsA, even without using RFr psoriasis, with some degree of accuracy.The univariate analysis showed that several items have
xcellent specificity (psoriasis, spinal disease, certain radio-raphic changes, clinical enthesitis, dactylitis, nail dystro-hy), but only psoriasis, RF negativity, and the presence ofny radiographic feature had adequate sensitivity. However,he CART analysis showed which variables, when combinedecursively, contributed to the diagnosis. These included RF,ail disease, dactylitis, any radiographic feature, �4 MCP
nvolved, radiographic DIP erosive disease, radiographic en-heseal ossification, and radiographic nonmarginal syndes-ophyte. In general, these items are present in existing cri-
eria sets.There are a number of important limitations to this study.
nalysis Multivariate Analysis*
Specificity OR (95%CI) P Value
0.960.97 9.1 (3.03-27.12) <.00110.88 2.3 (1.04-5.12) .0390.930.780.90 3.4 (1.46-7.74) .0050.970.8910.850.9910.990.980.66
nic diagnosis. The OR refers to the ratio of odds of having PsA withnly those variables selected by the model are presented (model
ed entheseal ossification, nonmarginal syndesmophytes and lateraln presence of the feature) were independently associated with the
on at the superior or inferior portions of the vertebral body.
f Psoriasis, Current Psoriasis and also Other Variables thatnosis
OR (95% CI) P Value
) 6.17 (1.43, 26.58) .015) 4.29 (1.49, 12.37) .007) 16.64 (3.30, 83.90) .002) 7.97 (1.87, 33.89) .005) 3.27 (1.44, 7.44) .005) 51.91 (6.29, 428.25) <.001) 0.042 (0.018, 0.099) <.0012)
ory for each variable is “absence of the feature.” The ORs for thets of clarity. Only the ORs for the presence of each variable are
es
te A
inst clisent. Oselect
ther tha
story oDiag
(SE)
(0.75(0.54(0.83(0.73(0.42(1.08(0.445 (0.3
categinteres
Trbsd
dccls
T
G
M
F
E
M
B
V
T
O*
Classification criteria of psoriatic arthritis 581
he patients were retrospectively identified from a diseaseegister, and this may have contributed to some selectionias. Moreover, only patients with RA were used as controls,o that the test performance indices are likely to be veryifferent when used in other patient groups (eg, other spon-
able 6 Test Performance of Each Classification Criteria
Rule RA PsA S
ladmanPositive 1 321Negative 146 10Not able to be classified 9 12cGonaglePositive 5 341Negative 138 2Not able to be classified 13 0
ourniePositive 9 304Negative 67 2Not able to be classified 80 37
SSGPositive 3 189Negative 143 147Not able to be classified 10 7oll and WrightPositive 1 301Negative 155 19Not able to be classified 0 20
ennett (5 of 8 version)Positive 1 224Negative 155 99Not able to be classified 0 20
asey and EspinozaPositive 1 340Negative 146 3Not able to be classified 9 0
able 7 Distribution of Agreement between the Classification
PatternID* Vasey ESSG Moll Gladman
1 1 1 1 12 1 1 1 15 1 1 1 06 1 1 1 09 1 1 0 1
10 1 1 0 117 1 0 1 118 1 0 1 121 1 0 1 022 1 0 1 025 1 0 0 126 1 0 0 146 0 1 0 062 0 0 0 064 0 0 0 0
ne indicates that the criteria for the rule is satisfied, and 0 indica
There are 64 possible combinations of how each rule might agree with eyloarthropathies). In particular, the high specificity of theseriteria is likely to be the result of the homogeneity of theontrol group (RA). The specificity almost certainly will beower when tested against less homogeneous controls, butuch testing is important to reflect normal clinical practice.
tivity SpecificityProportion Not Able
to be Classified
7 0.993 0.042
94 0.965 0.026
93 0.882 0.234
63 0.979 0.034
40 0.994 0.042
93 0.994 0.040
91 0.993 0.018
ria Except for Fournie (zero cells omitted)
onagle BennettNumber ofCases (RA)
Number ofCases (PsA)
1 1 1 1191 0 0 351 1 0 41 0 0 11 1 0 11 0 0 41 1 0 871 0 0 371 1 0 11 0 0 11 1 0 31 0 0 71 0 2 01 0 2 10 0 138 2
t the criteria for that rule is not satisfied.
ensi
0.9
0.9
0.9
0.5
0.9
0.6
0.9
Crite
McG
tes tha
ach of the others.
Drlrmfoa
Ratbnset
isotrdnitfecend(Pn(gorb(t
sgmdpg
T
VEMGMB
L
*
†
T
G
M
E
M
B
V
S
*†
582 W.J. Taylor et al.
ata were collected from case notes and review of existingadiographs; so that missing data items were a major prob-em. Finally, the small number of patients with RA and pso-iasis, or those with PsA without psoriasis in this sample,ake it very difficult to determine whether other disease
eatures were associated with PsA independently of psoriasis,r whether the association with PsA was the result of anssociation with psoriasis.
Nevertheless, these data suggest that neither psoriasis norF may be critically necessary to the diagnosis of PsA, as longs there are other characteristic features present. Such fea-ures include dactylitis, radiographic juxta-articular newone, �4 MCP involved, radiographic sacroiliitis, absence ofodules, clinical spondylitis, radiographic paravertebral os-ification, radiographic ankylosis, asymmetry, radiographicntheseal ossification, and chest wall pain. The role of RF inhe diagnosis of PsA is of particular interest, given its prom-
able 8 A 2-class Latent Model Fitted to the Data (n � 446)
Criteria Sensitivity (SE) Specificity (SE)
asey 1.00* 1.00*SSG 0.55 (0.03) 0.99 (0.01)oll 0.95 (0.01) 1.00*ladman 0.98 (0.01) 1.00*cGonagle 1.00* 0.97 (0.02)ennett 0.72 (0.03) 1.00*
og likelihood ratio chi-square � 35.35 (df � 50), P � .94.† Index ofdissimilarity � 0.05.
Parameter converged to 1 during estimation. Standard error cannotbe estimated.
P > .05 in a goodness-of-fit test indicates a statistically significantmodel fit.
able 9 Test Performance of the Classification Criteria Using Ca
Rule RA PsA
ladmanPositive 1 293Negative 142 10cGonaglePositive 5 301Negative 138 2
SSGPositive 3 164Negative 140 139oll and WrightPositive 1 285Negative 142 18
ennett (5 of 8 version)Positive 1 215Negative 142 88
asey and EspinozaPositive 1 300Negative 142 3
tatistical comparison of sensitivity and specificity used logistic regfor cases of PsA (sensitivity) and RA (1, specificity), using the V
There were no significant differences in specificity (model chi-squa
Model chi-square, 426.9; df � 5, P < .001, and the effect of rule type wanence in the original Moll and Wright formulation. When RFtatus is included in the CART analysis, the following clustersf features defined 4 subsets of PsA: 1) RF negative or posi-ive, psoriatic nail disease; 2) RF negative, no nail disease, anyadiographic feature, no grade 4 OA; 3) RF negative, no nailisease, no radiographic features, �4 MCP involved; 4) RFegative, no nail disease, no radiographic features, �4 MCP
nvolved, dactylitis. It could be concluded that RF seroposi-ivity should not exclude PsA as long as other characteristiceatures of PsA are present—in particular, psoriatic nail dis-ase. In the absence of nail or skin disease, RF seropositivitylearly associates with RA rather than PsA. However, to prop-rly investigate the relationship of RF with PsA, it would beecessary to study more RF-seropositive patients who wereiagnosed with RA and who also have psoriasis [S � P �RA)] and RF seropositive [S � P � (PsA)] and negative [S �� (PsA)] patients with PsA. In the present study, there wereo subjects with S � P � (RA) and only 16 with S � P �PsA), so that it was impossible to analyze whether theseroups were distinguishable on other grounds. The absencef S � P � (RA) patients from the database from where weecruited subjects may reflect a bias in the way patients areeing diagnosed at these institutions, or may reflect a truebut negative) association between RF and psoriasis in pa-ients with RA.
The problem of diagnostic bias is difficult to resolve intudies looking at test accuracy, when there is no pathologicold standard for the disease. In the rheumatology literature,ost classification criteria are based on the rheumatologistiagnosis as the gold standard. However, in PsA, there ap-ears to be significant disagreement among UK rheumatolo-ists about how PsA should be diagnosed (DPM Symmons,
at Could Be Classified by Every Rule Except Fournie (n � 446)
Sensitivity,OR (95% CI)†
Specificity,OR (95% CI)*
0.97, 0.29 (0.08-1.08)0.99
P � .064
0.99, 1.50 (0.25-9.04)0.97
P � .657
0.54, 0.012 (0.004-0.038)0.98
P < .001
0.94, 0.16 (0.05-0.54)0.99
P � .003
0.71, 0.024 (0.008-0.078)0.99
P < .001
0.99, 1.00 (reference) 0.99
n analysis to determine the ORs for each rule classifying positivelyriteria as the reference variable.5; P � .29), so the OR are not presented.
ses th
ressioasey cre, 6.1
s significant (P < .001).

pspuampsl
ccRsdcTtbptctEatmG
ipumi
AWCt
R
1
1
1
T
AE
E
I
I
N
Classification criteria of psoriatic arthritis 583
ersonal communication, June 2000), and this raises the pos-ibility of considerable heterogeneity among the group ofatients designated as PsA. We approached this problem bysing the technique of LCA, which uses the distribution ofgreement between multiple methods of classification toodel the underlying latent class structure. The model ap-eared meaningful and suggested that the different rules hadimilar accuracy except for Bennett and ESSG, which wereess sensitive than the other rules.
Which classification system should we use? These dataannot definitively answer this question, but it seems that allriteria sets have similar (high) specificity when tested againstA controls, and that the Bennett and ESSG criteria lackensitivity. On theoretical grounds, criteria that permit theiagnosis without the presence of psoriasis as long as otherharacteristic features of psoriasis might seem advantageous.his would favor Fournie, ESSG, and McGonagle. However,
his notion could not be adequately tested in this datasetecause of the absence of clinic-diagnosed PsA cases withoutsoriasis. On the other hand, ease of use is probably impor-ant and judged by the number of patients who have insuffi-ient data to be classified; the methods of Fournie appearedhe most difficult to use. Overall, the criteria of Vasey andspinoza had the best combination of feasibility, sensitivity,nd specificity for distinguishing between PsA and RA, buthere is actually no statistical difference between the perfor-ance of the criteria of Vasey and Espinoza, McGonagle, andladman.To resolve the problem of generalizability to other forms of
nflammatory joint disease, missing data, and selection bias, arospectively designed study that recruits a large number ofnselected (consecutive) patients with PsA and other inflam-atory arthritides (including other spondyloarthropathies)
able 10 Summary of CART Analysis (data priors)
Variables Entered intoAnalysis Splitters Sel
ll data included Current psoriasis onlyxcluding all psoriasis items(current, history, family,or nail disease)
RF, dactylitis
xcluding all psoriasis itemsand RF
Dactylitis, juxta-articular nradiographic sacroiliitis,spondylitis, paravertebraankylosis, symmetry, enwall pain
ncluding nail disease asonly psoriasis feature
RF nail disease, dactylitis>4 MCP involved, DIPossification, nonmargina
ncluding nail disease butexcluding RF
Dactylitis, nail disease, >
disease, entheseal ossifisacroiliitis, radiographicnodules, clinical spondy
ote. “Data priors” indicate that the pretest probability for a diagnothan using a population or clinic prevalence.
s required. 1
cknowledgmentse gratefully acknowledge John Horwood of the
hristchurch School of Medicine, New Zealand, for assis-ance with the statistical analysis.
eferences1. Taylor WJ, Helliwell PS. Case definition of psoriatic arthritis [letter].
Lancet 2000;356:20952. Gorter S. Psoriatic arthritis: performance of rheumatologists in daily
practice. Ann Rheum Dis 2002;61:219-24.3. Moll JMH, Wright V. Psoriatic arthritis. Sem Arthritis Rheum 1973;
3(1):55-78.4. Bennett RM. Psoriatic arthritis. In: McCarty DJ, ed. Arthritis and Re-
lated Conditions. 9th ed. Philadelphia: Lea & Febiger; 1979, p. 6455. Hein G, Schmidt F, Barta U, Muller A. Is there a psoriatic osteopathy?
The activity of bone resorption in psoriatics is related to inflammatoryjoint process. European J Med Res 1999;4:187-92.
6. Sharp JT, Lidsky MD, Collins LC, Moreland J. Methods of scoring theprogression of radiologic changes in rheumatoid arthritis. Correlationof radiologic, clinical and laboratory abnormalities. Arthritis Rheum1971;14:706-20.
7. Taylor WJ, Porter GG, Helliwell PS. Operational definitions and ob-server reliability of the plain radiographic features of psoriatic arthritis.J Rheumatol 2003;30:2645-58.
8. Vasey F, Espinoza LR. Psoriatic arthropathy. In: Calin A, ed. Spondy-loarthropathies. Orlando, Florida: Grune & Stratton; 1984, p. 151-185.
9. Gladman DD, Shuckett R, Russell ML, Thorne JC, Schachter RK. Pso-riatic arthritis—an analysis of 220 patients. Q J Med 1987;238:127-41.
0. Gladman DD, Stafford-Brady F, Chang CH, Lewandowski K, RussellML. Longitudinal study of clinical and radiological progression in pso-riatic arthritis. J Rheumatol 1990;17:809-12.
1. Gladman DD, Farewell VT, Wong K, Husted J. Mortality studies inpsoriatic arthritis: results from a single outpatient center. II. Prognosticindicators for death. Arthritis Rheum 1998;41:1103-10.
2. Ball J, Lawrence JS. Epidemiology of the sheep cell agglutination test.Ann Rheum Dis 1961;20:235-43.
by CARTSensitivity
(%)Specificity
(%)
98 9997 78
ne, >4 MCP involved,les, clinicalfication, radiographical ossification, chest
89 73
adiographic feature,e disease, enthesealesmophyte
94 88
P involved, DIP erosive, radiographicvolvement, symmetry,
90 81
sA used by the CART algorithm is that of the observed data, rather
ected
ew bonodul ossithese
, any rerosivl synd4 MCcationray inlitis
sis of P
3. Dougados M, van der Linden S, Juhlin R, Huitfeldt B, Amor

1
1
1
1
1
1
2
584 W.J. Taylor et al.
B, Calin A, et al. The European Spondyloarthropathy Study Grouppreliminary criteria for the classification of spondyloarthropathy.Arthritis Rheum 1991;34:1218-27.
4. McGonagle D, Conaghan PG, Emery P. Psoriatic arthritis: a unifiedconcept twenty years on. Arthritis Rheum 1999;42:1080-6.
5. Fournie B, Crognier L, Arnaud C, Zabraniecki L, Lascaux-Lefebvre V,Marc V, et al. Proposed classification criteria of psoriatic arthritis. Apreliminary study in 260 patients. Revue Du Rhumatisme, EnglishEdition 1999;66:446-56.
6. Faraone SV, Tsuang MT. Measuring diagnostic accuracy in the absence
of a “gold standard.” Am J Psychiatry 1994;151:650-7.7. Breiman L, Friedman JH, Olshen RA, Stone JS. Classification and Re-gression Trees. Belmont, CA: Wadsworth, 1984.
8. Steinberg D, Colla P. CART—Classification and Regression Trees. In:San Diego, CA: Salford Systems; 1997.
9. Uebersax J. A practical guide to local dependence in latent class models.2000. Available at: http://ourworld.compuserve.com/homepages/jsuebersax/condep.htm. Accessed April 30, 2003.
0. Marques CDL, Navaux F, Constantin A, Maziéres B, Cantagrel A.Comparative study of 4 diagnosis criteria sets for psoriatic arthritisin early inflammatory rheumatisms. Ann Rheum Dis 2000;59(suppl
1):202