a case of hepatocellular carcinoma: spontaneous regression?
TRANSCRIPT
Y
C
Ar
D
msticpdcr
tgcAmVermbtwsdM(m
FP
h1
ARTICLE IN PRESSG ModelDLD-2584; No. of Pages 2
Digestive and Liver Disease xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Digestive and Liver Disease
jou rna l h om epage: www.elsev ier .com/ locate /d ld
herbal medicine (AA), ischaemic and inflammatory processes. No
orrespondence
case of hepatocellular carcinoma: Spontaneousegression?
ear Editor,
Hepatocellular carcinoma (HCC) is one of the most commonalignancies in the world. It is often diagnosed at an advanced
tage, when most potentially curative therapies, such as resection,ransplantation, and percutaneous ablation, are of limited util-ty. Only approximately 30–40% of patients can benefit from suchurative therapies, and up to 70% of patients who undergo theserocedures will have recurrent disease within 5 years. Patientsiagnosed at an intermediate stage can benefit from transarterialhemoembolization while patients in advanced stage of disease areeferred to treatment with sorafenib [1].
We report the case of a 65-year-old Caucasian man with a his-ory of non-alcoholic steatohepatitis (NASH). He was referred to ourastroenterology unit in March 2011 for suspected hepatocellulararcinoma according to computed tomography (CT) scan findings.
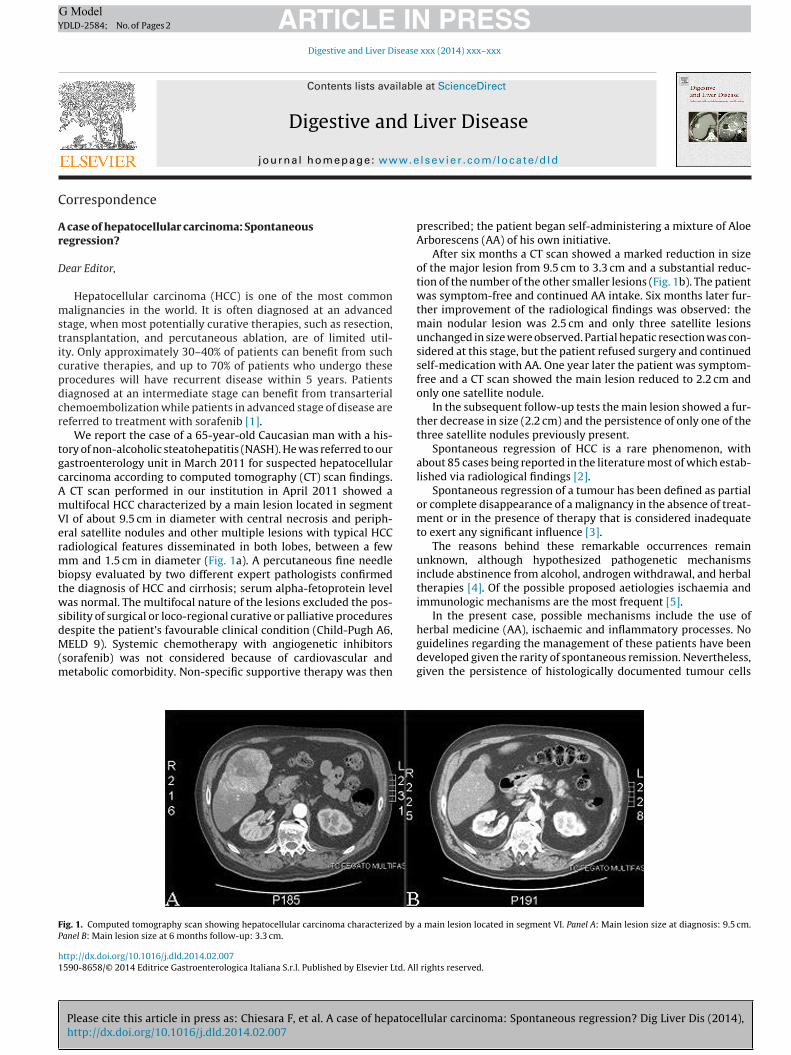
CT scan performed in our institution in April 2011 showed aultifocal HCC characterized by a main lesion located in segmentI of about 9.5 cm in diameter with central necrosis and periph-ral satellite nodules and other multiple lesions with typical HCCadiological features disseminated in both lobes, between a fewm and 1.5 cm in diameter (Fig. 1a). A percutaneous fine needle
iopsy evaluated by two different expert pathologists confirmedhe diagnosis of HCC and cirrhosis; serum alpha-fetoprotein levelas normal. The multifocal nature of the lesions excluded the pos-
ibility of surgical or loco-regional curative or palliative proceduresespite the patient’s favourable clinical condition (Child-Pugh A6,
Please cite this article in press as: Chiesara F, et al. A case of hepatocehttp://dx.doi.org/10.1016/j.dld.2014.02.007
ELD 9). Systemic chemotherapy with angiogenetic inhibitorssorafenib) was not considered because of cardiovascular and
etabolic comorbidity. Non-specific supportive therapy was then
ig. 1. Computed tomography scan showing hepatocellular carcinoma characterized by
anel B: Main lesion size at 6 months follow-up: 3.3 cm.
ttp://dx.doi.org/10.1016/j.dld.2014.02.007590-8658/© 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All
prescribed; the patient began self-administering a mixture of AloeArborescens (AA) of his own initiative.
After six months a CT scan showed a marked reduction in sizeof the major lesion from 9.5 cm to 3.3 cm and a substantial reduc-tion of the number of the other smaller lesions (Fig. 1b). The patientwas symptom-free and continued AA intake. Six months later fur-ther improvement of the radiological findings was observed: themain nodular lesion was 2.5 cm and only three satellite lesionsunchanged in size were observed. Partial hepatic resection was con-sidered at this stage, but the patient refused surgery and continuedself-medication with AA. One year later the patient was symptom-free and a CT scan showed the main lesion reduced to 2.2 cm andonly one satellite nodule.
In the subsequent follow-up tests the main lesion showed a fur-ther decrease in size (2.2 cm) and the persistence of only one of thethree satellite nodules previously present.
Spontaneous regression of HCC is a rare phenomenon, withabout 85 cases being reported in the literature most of which estab-lished via radiological findings [2].
Spontaneous regression of a tumour has been defined as partialor complete disappearance of a malignancy in the absence of treat-ment or in the presence of therapy that is considered inadequateto exert any significant influence [3].
The reasons behind these remarkable occurrences remainunknown, although hypothesized pathogenetic mechanismsinclude abstinence from alcohol, androgen withdrawal, and herbaltherapies [4]. Of the possible proposed aetiologies ischaemia andimmunologic mechanisms are the most frequent [5].
In the present case, possible mechanisms include the use of
llular carcinoma: Spontaneous regression? Dig Liver Dis (2014),
a main lesion located in segment VI. Panel A: Main lesion size at diagnosis: 9.5 cm.
guidelines regarding the management of these patients have beendeveloped given the rarity of spontaneous remission. Nevertheless,given the persistence of histologically documented tumour cells
rights reserved.

ING ModelY
2 d Live
edm
CN
R
[
[
[
[
[
ARTICLEDLD-2584; No. of Pages 2
Correspondence / Digestive an
ven in cases of radiological regression, frequent restaging of theisease in these patients is recommended to identify appropriateanagement.
onflict of interestone declared.
eferences
1] Bruix J, Sherman M. American Association for the Study of Liver Diseases. Man-agement of hepatocellular carcinoma: an update. Hepatology 2011;53:1020–2.
2] Sasaki T, Fukumoria D, Yamamoto K, et al. Management considerations for pur-ported spontaneous regression of hepatocellular carcinoma: a case report. CaseReports in Gastroenterology 2013;7:147–52.
3] Everson TC, Cole WH. Spontaneous regression of malignant disease. Journal of
Please cite this article in press as: Chiesara F, et al. A case of hepatocehttp://dx.doi.org/10.1016/j.dld.2014.02.007
the American Medical Association 1959;169:1758–9.4] Huz JI, Melis M, Sarpel U. Spontaneous regression of hepatocellular carcinoma
is most often associated with tumour hypoxia or a systemic inflammatoryresponse. Official Journal of the International Hepato Pancreato Biliary Asso-ciation 2012;14:500–5.
PRESSr Disease xxx (2014) xxx–xxx
5] Oquinena S, Inarrairaegui M, Vila JJ, et al. Spontaneous regression of hepatocel-lular carcinoma: three case reports and a categorized review of the literature.Digestive Diseases and Sciences 2009;54:1147–53.
Francesca Chiesara ∗
Annalisa SpagnoloMaurizio Koch
Alessandra MorettiGastroenterology and Hepatology Unit, San Filippo
Neri Hospital, Rome, Italy
∗ Corresponding author at: Via Martinotti 20,00135 Rome, Italy. Tel.: +39 06 33063335/339
4957170; fax: +39 06 33062641.
llular carcinoma: Spontaneous regression? Dig Liver Dis (2014),
E-mail address: [email protected] (F.Chiesara)
Available online xxx