2015 neurodegenerative diseases
TRANSCRIPT
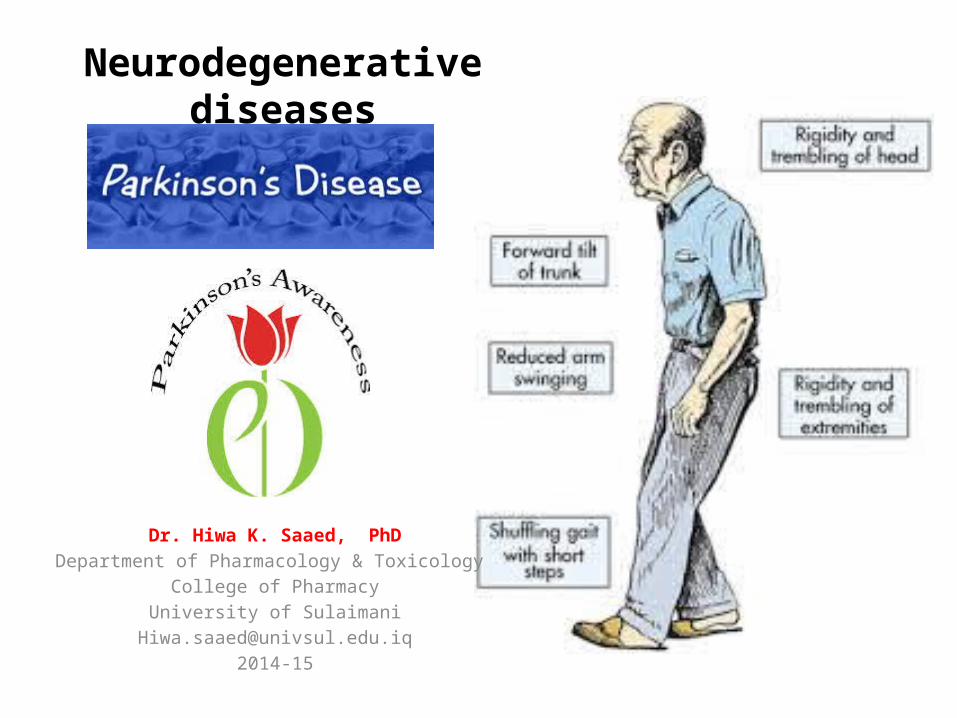
Neurodegenerative diseases
Dr. Hiwa K. Saaed, PhDDepartment of Pharmacology & Toxicology
College of PharmacyUniversity of Sulaimani
Neurodegenerative diseases of the CNS
Progressive loss of selected neurons in discrete brain areas, resulting in characteristic disorder of movement, cognition, or both. Include:
• Alzheimer disease: dementia and disordered cognitive function.
• Parkinson’s disease: a disabling motor impairment disorder.
• Huntington disease: excessive and abnormal movement.• Amyotrophic lateral sclerosis (ALS): progressive weakness
and muscle atrophy.
04/18/2023
2

State of DA/ACH imbalance
04/18/2023 3
PARKINSON’S DISEASE
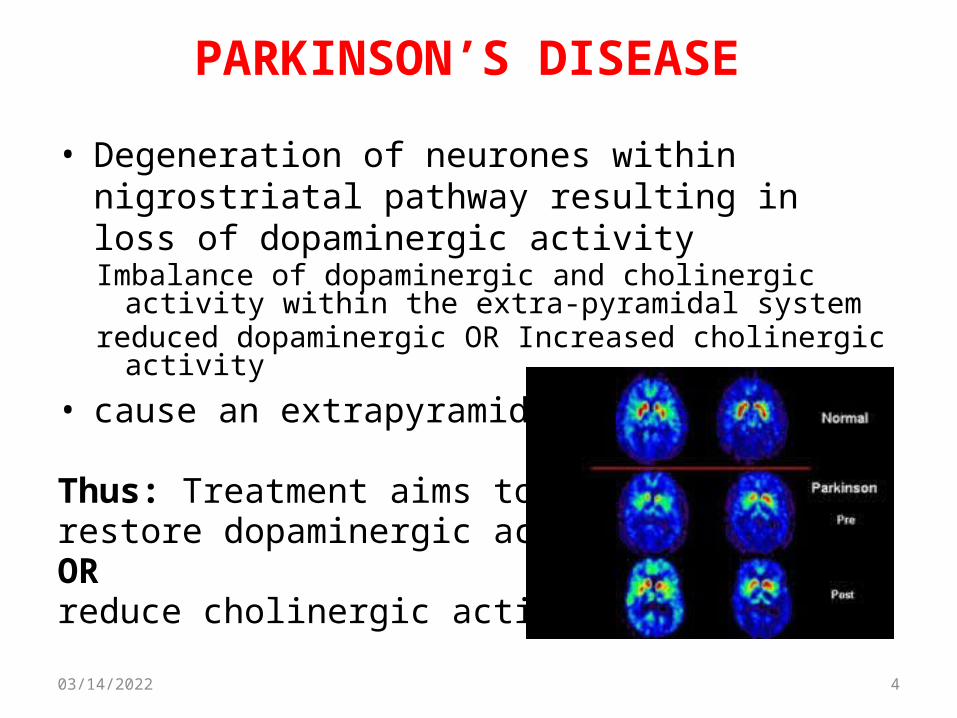
• Degeneration of neurones within nigrostriatal pathway resulting in loss of dopaminergic activity Imbalance of dopaminergic and cholinergic activity within the
extra-pyramidal systemreduced dopaminergic OR Increased cholinergic activity
• cause an extrapyramidal motor disorder
Thus: Treatment aims to restore dopaminergic activity OR reduce cholinergic activity
04/18/2023 4
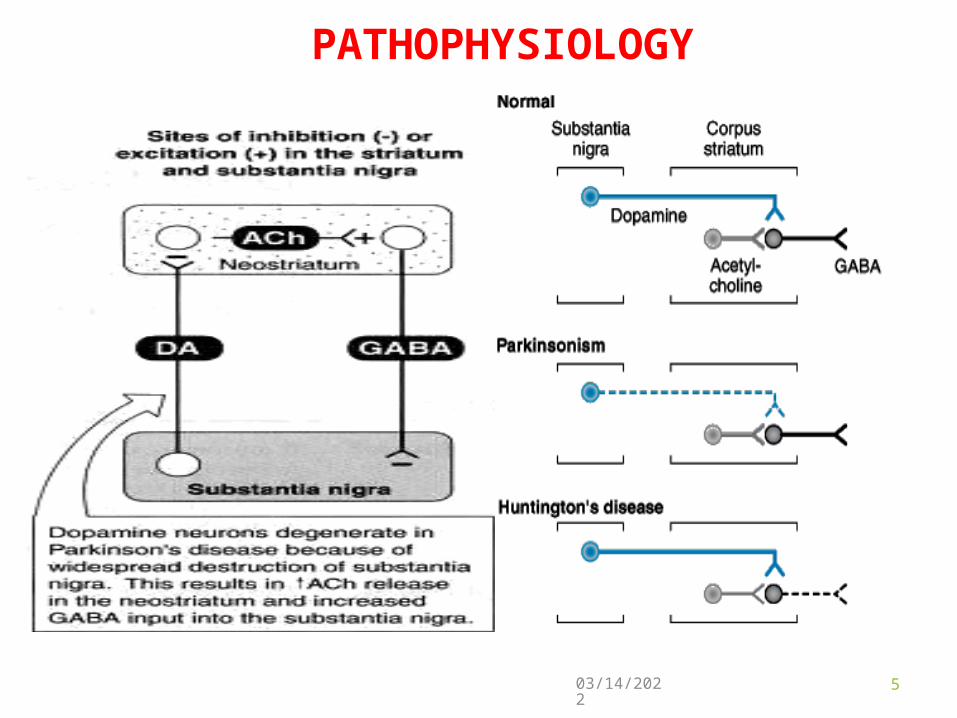
PATHOPHYSIOLOGY
04/18/2023 5

RAFT
Characterized by: RAFT; rigidity, akinesia, flat facies, tremor(1) Rigidity of skeletal muscles,(2) Akinesia (or bradykinesia, or hypokinesia; slowness
in initiating and carrying out voluntary movements, (3) Flat facies (mask like face), (4) Tremor at restWith secondary manifestations like
– postural and gait abnormalities – with a tendency to fall backwards or forwards.
04/18/2023 6
PARKINSON’S DISEASE ETIOLOGY:
04/18/2023 7
Primary; unknown causeSecondary (Drug-induced Parkinsonism):• Reversible:
– butyrophenone, – phenothiazine, – reserpine (at high dose)
• Irreversible: MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine)
Treatment with MAOB Inhibitors protects against MPTP neurotoxicity in animals.
STRATEGY OF TREATMENT
is to re-establish the balance between dopamine and Ach. This can be accomplished by either 1. increasing dopamine activity in the NG, 2. decreasing muscarinic cholinergic activity in the striatum, 3. or both.Through:4. Drug affecting brain dopaminergic system5. Drug affecting brain cholinergic system
04/18/2023 8

PHARMACOLOGIC TREATMENT OPTIONS:
I. Drug affecting brain dopaminergic system1. Dopamine precursor: levodopa2. Peripheral decarboxylase inhibitors:
– carbidopa, benserazide
3. Dopaminergic agonists: – Ergot derivatives: bromocriptine, pergolide, piribedil, – Non ergot derivatives: ropinirole, pramipexole
4. MAO-B inhibitors: selegiline5. COMT inhibitors: entacapone, tolcapone6. Dopamine facilitator: amantadine
04/18/2023 9

1. Central anticholinergics: – trihexyphenidyl (benzhexol), – procyclidine, – benztropine,– biperidine
2. Antihistaminics: – diphenhydramine, – promethazine.
Q. Can these drugs cure? No! Pharmacologic treatments can only offer
temporary relief; they neither reverse nor arrest the disease process
04/18/2023 10
PHARMACOLOGIC TREATMENT OPTIONS:II. Drugs affecting brain cholinergic system
1. LEVODOPA
High therapeutic index-drug of choice for symptom control especially in elderlyMechanism of action• Dopamine itself has low bioavailability and does not
readily cross the BBB, its precursor, Levodopa, is readily transported into the CNS, and is converted to dopamine in the brain by the enzyme DOPA decarboxylase, which is present in many body tissues.
• Levodopa is usually given with carbidopa, a drug that does not cross the BBB but inhibits DOPA decarboxylase in peripheral tissues.
04/18/2023 11
• early phase of treatment (lasts 5-6 years typically) • dopaminergic neurons still present, L-dopa can be stored
in nerve terminals-produces a physiological concentration without much fluctuation “wear off”.
• Unfortunately with time, the number of neurons decreases and fewer cells are capable of taking up exogenously administered levodopa and converting it to dopamine for subsequent storage and release.
• Consequently, motor control fluctuation develops.
04/18/2023 12
“L-DOPA HONEYMOON”
ABSORPTION AND METABOLISM
• The drug is absorbed rapidly from the small intestine. • levodopa should be taken on an empty stomach,
typically 45 minutes before a meal. • Because, Ingestion of large, neutral amino acids
‘leucine and isoleucine’ compete with levodopa for absorption from the gut and for transport across the BBB.
• It has an extremely short half-life (1-2 hrs), which causes fluctuations in plasma concentration. This may produce fluctuations in motor response “on-off” phenomenon.
• Withdrawal from the drug must be gradual.
04/18/2023 13
TOXICITY• GIT (due to stimulation of dopamine receptor): anorexia, nausea, and
emesis. Tolerance to emetic action of levodopa usually occurs after several months.
• CVS: postural hypotension is common, especially in the early stage of treatment.
• CNS: – Dyskinesias choreoathetosis of the face and distal
extremities occurs frequently. – chorea (the ceaseless occurrence of rapid, jerky
involuntary movements), – ballismus (Jerky or shaking movements of the arms or
legs), myoclonus, – tics (an involuntary, compulsive, rapid, repetitive,
stereotyped movement or vocalization. Also called habit spasm.),
– tremor.04/18/2023 14
TOXICITY
• Behavioural effects: – anxiety, – agitation, – confusion, – delusions (false belief) , – hallucinations (false perception), – and depression.
Q. delay L-dopa use especially in younger patients??Answer: Neurotoxicity of L-dopa-DOPA metabolism results in neurotoxic breakdown products results in the progression of Parkinson’s.
04/18/2023 15

CONTRAINDICATION & DRUG INTERACTIONS
• In patient with a history of psychosis, Levodopa exacerbates symptoms, possibly through the build up of central amines.
• In patients with glaucoma, the drug can cause an increase in intraocular pressure.
DRUG INTERACTIONS• Antipsychotic drugs, because these block dopamine
receptors and produce a parkinsonian syndrome themselves.
• The vitamin pyridoxine B6 increases the peripheral breakdown of levodopa and diminishes its effectiveness.
• Non selective MAOI, such as phenelzine, which could lead to a life threatening hypertensive crises caused by enhanced catecholamine production.
04/18/2023 16

2. MAO B INHIBITORS; SELEGILINE
Selegiline, selectively inhibits MAO B (which metabolizes dopamine, but does not inhibit MAO A (which metabolizes norepinephrine and serotonin).
Therefore, it enhances the actions of levodopa, and when these drugs are administered together, selegiline substantially reduces the required dose of levodopa.
Cheese reaction: at recommended doses has little potential for causing hypertensive crisis (Does not cause “cheese reaction”). However, if selegiline is administered at high doses, the selectivity of the drug is lost, and the patient is at risk for severe hypertensive.
04/18/2023 17

3.CATECHOL-O-METHYLTRANSFERASE (COMT) INHIBITORS
• Entacapone and tolcapone are nitrocatechol derivatives that selectively and reversibly inhibit COMT.
• Normally, the methylation of levodopa by COMT to 3-O-methyldopa is a minor pathway for levodopa metabolism.
• However when peripheral DDC activity is inhibited by carbidopa, a significant concentration of 3-O-methyldopa is formed that competes with levodopa for active transport.
04/18/2023 18
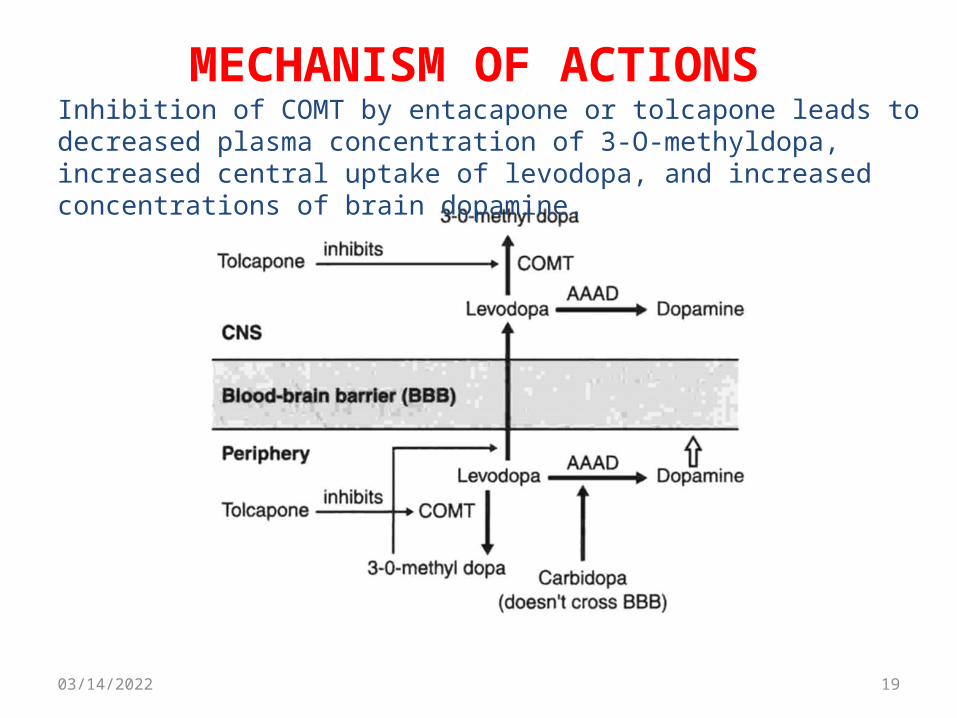
MECHANISM OF ACTIONS
04/18/2023 19
Inhibition of COMT by entacapone or tolcapone leads to decreased plasma concentration of 3-O-methyldopa, increased central uptake of levodopa, and increased concentrations of brain dopamine.
• Both reduce the symptoms of “wearing-off” phenomena seen in patients on levodopa-carbidopa.
• Tolcapone penetrates the BBB and inhibits COMT in the CNS and it has a relatively longer duration of action compared to entacapone.
Adverse effects: • Diarrhoea, postural hypotension, nausea, anorexia, dyskinesia,
hallucinations, and sleep disorders. • Fulminating hepatic necrosis is associated with tolcapone. • Entacapone does not exhibit this toxicity and has largely replaced
tolcapone.
04/18/2023 20
Catechol-O-methyltransferase (COMT) inhibitors
4. DOPAMINE RECEPTOR AGONISTS
• Ergot derivatives– bromocriptine (D2)– pergolide (D1 and D2)
• Nonergolines– pramipexol– Ropinirole
These agents have durations of action longer than that of levodopa, thus have been effective in patients exhibiting fluctuations in their response to levodopa.L-DOPA sparing - useful to delay use of L-DOPA in younger patientsNot neurotoxic ? neuroprotective
04/18/2023 21
BROMOCRIPTINE AND PERGOLIDE
• Pergolide is the more potent of the two. • Side effects severely limit the utility of dopamine agonists.NB. Bromocriptine, in addition to being used to treat Parkinson’s disease,
it is the drug of choice to treat cases of hyperprolactiemia.Adverse Effects; • Hallucinations, confusion, delirium, nausea, and orthostatic
hypotension. Dyskinesia less frequent than with levodopa.• In psychiatric illness, they may cause the mental condition to worsen.• Cardiac problems, particularly in patients with a history of myocardial
infarction. • In patients with peripheral vascular disease, a worsening of the
vasospasm occurs.• In patients with peptic ulcer, there is a worsening of the ulcer. • Because they are ergot derivatives, both have the potential to cause
the pulmonary and retroperitoneal fibrosis.
04/18/2023 22
Pramipexole and ropinirole Advantages
• They alleviate the motor deficits in both: patient who have never been treated with levodopa and patients with advanced Parkinson disease taking levodopa.
• They may delay the need to employ levodopa therapy in early Parkinson, and may decrease the dose of levodopa therapy in advanced Parkinson.
Unlike the ergotamine derivatives, prampixole and ropinirole do not exacerbate peripheral vasospasm, nor do they cause fibrosis.
04/18/2023 23

ADVERSE EFFECTS:
• Nausea, hallucinations, insomnia, dizziness, constipation, and orthostatic hypotension.
• Dyskinesia less frequent than with levodopa.
Drug interaction• Cimetidine, which inhibits renal tubular secretion of
organic bases, increases the half-life of pramipexole by 40%.
• Fluoroquinolone antibiotics inhibit the metabolism of ropinirole, and enhance the AUC by 80%.
04/18/2023 24
AMANTADINE• Increase the release of dopamine• Blockading cholinergic receptors• Act on NMDA receptors• NB: if dopamine release is already at a maximum,
amantadine has no effect.
ADVERSE EFFECTS• Restlessness, • agitation, • confusion, • and hallucinations, • and at high doses, it may induce acute toxic psychosis,
orthostatic hypotension, urinary retention, peripheral edema, and dry mouth.
04/18/2023 25
Amantadine
Compared to L-dopa, Amantadine is:– less efficacious– tolerance develops more rapidly. – has fewer side effects.
Compared to anticholinergic, Amantadine is:– has little effect on tremor, – but is more effective against rigidity and bradykinesia.
04/18/2023 26

Antimuscarinic agents: benztropine, Trihexphenidyl, and biperiden
• They are much less efficacious than levodopa and play only an adjuvant role in Parkinsonism therapy.
• SE: Mood changes, xerostomia and visual problems
04/18/2023 27
DRUGS FOR ALZHEIMER’S
Alzheimer’s disease; progressive loss of memory and disordered cognitive function.
PATHOPHYSIOLOGY: Cholinergic transmission decreased in Alzheimer’s,
TREATMENT STRATIGIES: current therapies are aimed at: 1. either improving cholinergic transmission within the CNS 2. or preventing the excitotoxicity actions of NMDA glutamate
receptors in selected brain areas.
04/18/2023 28

DRUGS FOR ALZHEIMER’S
I. Acetylcholinesterase inhibitors:e.g., donepezil, rivastigmine, galantamine,
tacrineAdverse effects – nausea, diarrhea, abdominal
cramps, bradycardia, urine incontinenceII. NMDA receptor antagonists: Memantine
(dimethyl adamantine derivative related to amantadine) it is an uncompetitive inhibitor of NMDA receptors
04/18/2023 29
HUNTINGTON DISEASE
-An inherited adult onset neurologic disease due to a single defect on chromosome 4.
Characterized by:• shuffling gait, • stooped posture, • resting tremor, • speech impediments, • movement difficulties, • and an eventual slowing of mental processes and
dementia
04/18/2023 30
HUNTINGTON DISEASE
• Pathophysiology: the disease is thought to occur because of excessive dopaminergic activity and diminished GABA functions in the basal ganglia (caudate and putamen).
• Treatment: Dopamine blockers such as haloperidol or tetrabenazine are used to treat this disorder.
04/18/2023 31
• A neurologic disease of unknown cause • Presents with multiple tics associated with snorting,
sniffing, and involuntary vocalizations (often absence)
• Treatment: clonidine, haloperidol
04/18/2023 32
TOURETTE’S SYNDROME
Wilson’s disease
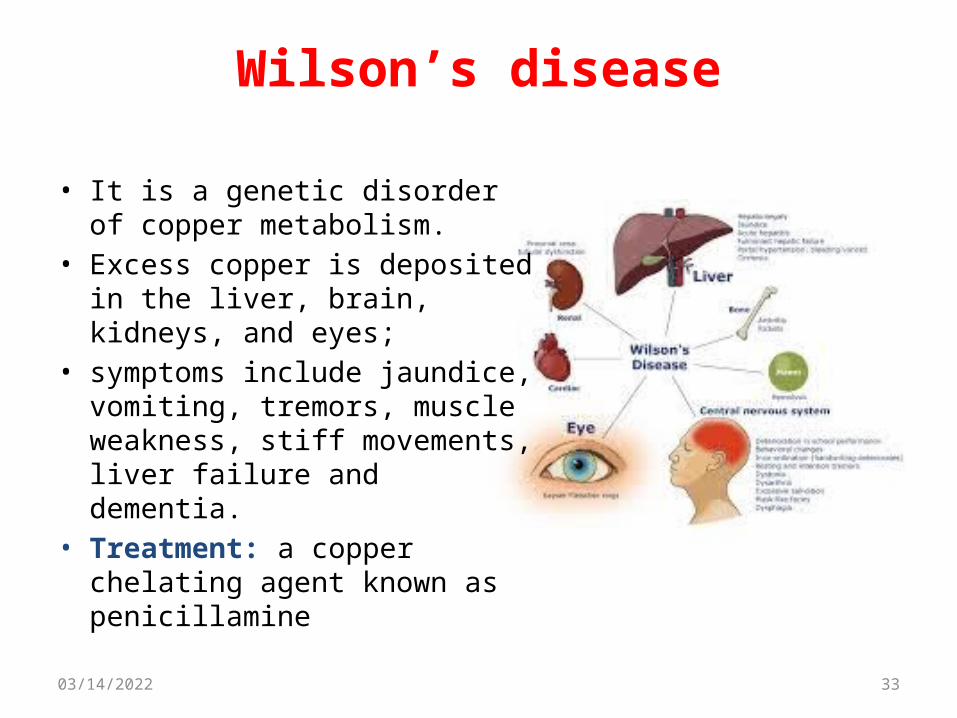
• It is a genetic disorder of copper metabolism.
• Excess copper is deposited in the liver, brain, kidneys, and eyes;
• symptoms include jaundice, vomiting, tremors, muscle weakness, stiff movements, liver failure and dementia.
• Treatment: a copper chelating agent known as penicillamine
04/18/2023 33
QUESTIONS???
04/18/2023 34
https://www.youtube.com/watch?v=3wg9ExKwZy4&list=FLZdUnOFcZY4ENo5Rez_ZHJw&index=1