08 elbow intervention lecture handout.ppt - continuing ed elbow intervention lecture... ·...
TRANSCRIPT

Elbow Interventions
Ed Mulligan, PT, DPT, OCS, SCS, ATCClinical Orthopedic Rehabilitation Education

Age Incidence of Elbow Injuries
Pediatric Adult

overuse injuries of the elbow

Lateral Epicondylitis/osis
tendinosis (collagen degeneration) at common extensor origin (ECRB)
Lateral Tendinopathy
Medial Tendinopathy

Recognition of Pathology PatternLateral Elbow Pain
LESIONORIGIN
LOCAL REMOTEElbow • Cervical Spine Segmental Facilitation or Hypersensitivity
• Adverse Neural Tension• Wrist Dysfunction
TISSUEINVOLVEMENT
CONTRACTILE NON‐CONTRACTILEECRB Tendinopathy
• RHJ/SRUJ Dysfunction• Radial Tunnel SyndromeSynovial PlicaeCapitellar OCDPLRI
ContributingFactors
OveruseErgonomic ViolationsPositional FaultsBiomechanics/Technique Errors5x more common than medial elbow pain
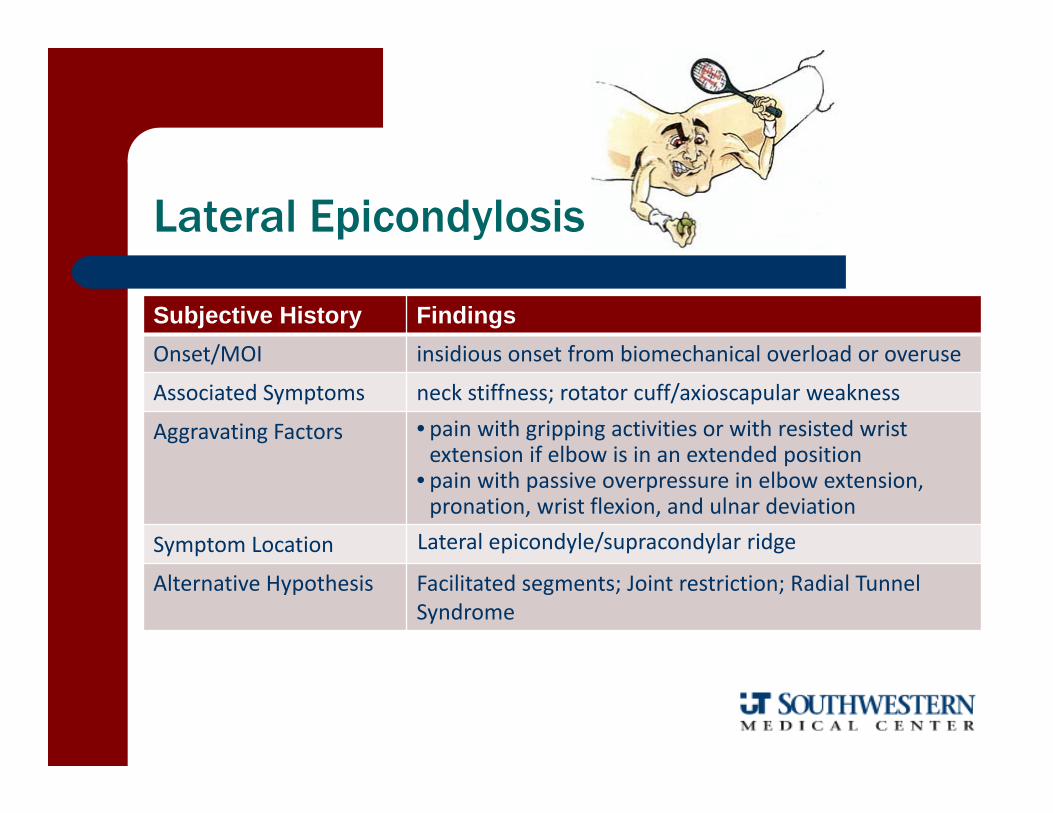
Lateral Epicondylosis
Subjective History FindingsOnset/MOI insidious onset from biomechanical overload or overuse
Associated Symptoms neck stiffness; rotator cuff/axioscapular weakness
Aggravating Factors • pain with gripping activities or with resisted wrist extension if elbow is in an extended position
• pain with passive overpressure in elbow extension, pronation, wrist flexion, and ulnar deviation
Symptom Location Lateral epicondyle/supracondylar ridge
Alternative Hypothesis Facilitated segments; Joint restriction; Radial Tunnel Syndrome

Lateral Epicondylosis
Objective Examination Findings
A/PROM‐End Feel Humeroradial joint restrictions; flexion contracture
Contractile Status Decreased grip strength (particularly in passively insufficient positions)
Palpation Tenderness at insertion of ECRB on supracondylar ridge; radial head (medial displacement) positional fault
Special Tests Cozen and Mills Test
Differential Diagnosis C6 radiculopathy; Radial Tunnel Syndrome (lateral); Pronator Syndrome (medial)
Outcome Tool DASH; Patient‐Rated Forearm Evaluation Questionnaire

Intervention Emphasis
Pain Based– Modalities – Physical Agents ‐Manual Therapy
Impairment Based Local Contractile – ECRB Tendinopathy
– Therapeutic Exercise Local Joint Dysfunction – SRUJ/RHJ
– Manual Therapy (HVLA Thrust, MWM) Local Neural Dysfunction – PIN
– Splinting – Activity Limitations – Neural Flossing Remote Contributions
– Cervicothoracic and Wrist Manual Therapy– Axioscapular Strengthening– Neurodynamic Restoration

Addressing Primary Pain Complaint
Modalities/Physical Agents– Ultrasound or Phonophoreis (B)
When combined with physical interventions
– Iontophoresis (diclofenac) (B)– Acupuncture – (B)
– Cyrotherapy/Ice Massage – (C)– High Volt Galvanic Stimulation (C/D)– Graded mobilization – Education and rest from offending activities
based on systematic reviews by:Trudel D, et al, J Hand Ther, 2004; Biset L, et al, Br J Sports Med, 2005; and Johnson GW, et al, Am Fam Physician, 2007
Low Level (cold) Laser
Level 1 meta‐analysis for effectiveness in short term relief for pain/disability when administered with optimal doses; probably not a good stand alone treatment
Bjordal JM, BMC Musculoskeletal Disorders, 2008
Systematic review suggesting moderate to large effect size for reducing point tenderness and increasing grip force
Chang WD, et al, PhotoMed Laser Surg, 2010

Local Treatment:
ECRB Tendinopathy
Therapeutic Exercise – Value of eccentric emphasis– Prospective, RCT (LOE I) showed
significantly greater function (DASH score), point tenderness, and strength (wrist and middle finger extension) for the eccentric training intervention group as compared to a traditional exercise program
Tyler TF, et al, J Shoulder Elbow Surg, 2010

Local Treatment:
ECRB Tendinopathy
Counterforce Bracing– Non‐elastic circumferential orthoses– No definitive conclusions can be made based
on conflicting or equivocal evidence– Wrist splint provided more pain relief than
forearm strap in a prospective, RCT
Soft Tissue Mobilization – Deep friction or deep tissue massage– no conclusive evidence regarding efficacy

Augmented Soft Tissue Mobilization
Prospective RCT comparing ASTM to medical advice, ergo-nomic counseling, and stretching
While both groups improved in pain, grip strength, and function there was not a significant difference between groups
Authors argue for a larger power sample to detect differences
Blanchette MA, J Manipulative Physiol Ther, 2012

Local Treatment:
Joint Dysfunction
Manual Therapy– Cyriax extension and/or varus
mobilization/manipulations– Short term benefit in regards to
pain to palpation and pain‐free grip
Paungamali, et al, Phys Ther, 2003Vicenzino, et al, Man Ther, 2001
Stretching/Flexibility– studies tend to lump flexibility
training in with other interventions
Joint Mobilization Mobilization with Movement
HVLA Thrust

Remote Interventions
Wrist Manual Therapy– Wrist manipulation more
effective than traditional local treatment
Struijs, et al, Phys Ther, 2003
Neurodynamic Restoration– Neural Glides to address adverse
neural tension and/or peripheral nerve hypersensitivity
Beneciuk JM, J Ortho Sports Phys Ther, 2009Ekstrom RA, et al, Phys Ther, 2002
Cervical Manual Therapy

Global Interventions
Axioscapular and RC training IADL and equipment modifications Job/Sport Specific technique analysis Postural and Ergonomic counseling

Medical Management to enhance physical therapy interventions
Oral NSAIDs Injections
– Corticosteroids vs. PRP Short vs. long term value
– Prolotherapy Topical Nitric Oxide Patches Extracorporeal Shockwave Therapy Surgical Intervention

Latest High Quality Trials Offer Conflicting Conclusions
Supervised Stretching/Eccentric Strengthening (12 visits over 4 wks) superior to friction massage/manipulation in regard to pain and self‐report outcomes
Viswas R, et al, Sci World J, 2012
Friction Massage/manipulation (12 visits over 4 wks) superior to stretch‐ing/eccentric training and phono‐phoresis (diclofenac) in regard to pain and self‐report outcomes
Nagrale AV, et al, J Man Manipul Ther, 2012
• Both groups in both studies improved in a relatively short follow‐up• Both groups had sound methodological design (PEDro) = 6/10)
My interpretation – manual interventions can be utilized in clinic and therapeutic interventions can be emphasized in the HEP

entrapment (compression between the radial head andsupinator muscle) of the posterior interosseous branchof the radial nerve in the radial tunnel
radial tunnel syndrome

Radial Tunnel Syndrome
Subjective History FindingsAggravating Factors Prolonged or repetitive gripping activities;
Sustained positioning in extension‐pronation
Symptom Location Pain at radial head
Symptom Quality Deep burning pain may radiate down the dorsal forearm; possible paresthesias in radial distribution
Alternative Hypothesis C6 radiculopathy; Lateral Epicondylitis

Radial Tunnel Syndrome
Objective Examination FindingsInspection/Observation Atrophy of any muscle
innervated by radial nerve
A/PROM‐End Feel Usually no joint restrictions
Contractile Status Pain with resisted supination or extension of index finger
Palpation Reproduction of symptoms with palpation over radial head (not supracondylar ridge)
Special Tests ULTT 2 (radial bias)
Neuro Screen Radial nerve tension test

InterventionModalities • Low‐intensity Ultrasound (1 MgHz pulsed at 1.0 wtts/cm2)
for pain reduction• Iontophoresis (based on evidence supporting the treatment of CTS)
Manual Therapy Radial nerve glides - no strain or reproduction of symptoms allowed
Therapeutic Exercise Axioscapular and postural exercise
Posture/Ergonomics • Avoidance of elbow extension and pronation positions• Tilted angle and negatively sloped keyboards• Appropriate mouse use (no forearm posting)• Ergonomic evaluation of workstation
Radial Tunnel Syndrome

Intervention
Activity Limitations Prolonged static pinching or squeezing of objects or tools is avoided
Bracing Nocturnal wrist extension splint and during activities of risk as needed to relax extensors and supinators
Regional Concerns Cervical dysfunction
Prognostic FactorsPoor prognosis for non‐operative treatment if notable atrophy of radially innervated muscles and severe pain (>8/10)
Radial Tunnel Syndrome

Cubital Tunnel Syndrome
Ulnar neuropathy secondary topressure, traction, or ischemiain the tunnel between the medial epicondyle and olecranon

Cubital Tunnel Syndrome
Subjective History FindingsOccupational Predisposition Repetitive wrist motions with elbow in flexion –
(baseball/tennis or carpenters/painters/musicians)
Associated Symptoms • Elbow Osteoarthritis• Excessive Cubital Valgus• Subluxing Ulnar Nerve• Elbow instability
Aggravating Factors • Prolonged elbow flexion ‐ increased tunnel pressure and excursion requirement as elbow moves out of extension and into flexion
• Elbow positioned on arm rests or on window when driving
‐ continued on next page

Cubital Tunnel Syndrome
Subjective History FindingsSymptom Location • Pain/paraesthias along medial forearm
• Sensory changes in ulnar distribution
Symptom Quality Intermittent to constant paraesthias in ulnar pattern
Alternative Hypothesis • Thoracic Outlet Syndrome• Cervical Radiculopathy, • Apical Lung Tumor• Handlebar Palsy

Cubital Tunnel Syndrome
Objective Examination FindingsInspection/Observation • + Wartenberg’s sign (abducted 5th digit)
• Motor deficits evidenced by 4th‐5th digit clawing – Bishop’s Hand ‐ usually indicating more advanced stage
Contractile Status Weakness of ulnar innervated muscles; hypothenar muscles
Palpation Tinel’s (careful of false +)
Special Tests • Flexed Posture• Digital Compression• combination of pressure/position most accurate• + Froment’s Sign (FPL substitutes for AP)
Neuro Screen Semmes Weinstein monofilament for sensory impairment or 2 point discrimination for more severe cases
Outcome Tool DASH or Mayo Elbow Function Score

InterventionModalities No proven value for any physical agent or
electrotherapeutic modality
Manual Therapy Careful ulnar nerve glides; normalize joint restrictions
Therapeutic Exercise Restore identified impairments. Promotion of total arm strength and endurance
Posture/Ergonomics No elbow weight bearing or crossing arms when sitting; use of elbow pads
Cubital Tunnel Syndrome

Cubital Tunnel Syndrome
InterventionActivity Limitations REST; Activity modification, ergonomic
recommendations, and rest from offending activities
Bracing Nocturnal splinting in mid range flexion (40‐70°); day time as well for severe cases; towel wrap at night
Regional Concerns Cervical Dysfunction
Prognostic Factors • 75‐90% of patients with mild to moderate cases benefit from conservative care
• Success of non‐op intervention directly related to severity of condition (more on next slide)
• Failed conservative interventions may require subsequent surgical decompression, epicondylectomy, and/or transpositions

Intervention Success
Highly dependent upon presenting severityGrade Motor Deficit Sensory Deficit
I Undetectable weakness Intermittent paresthesias
II Intrinsic weakness
Decreased sensory/vibratory detection
IIIVisible atrophy/Papal Sign
Constant paresthesia; abnormal 2‐point discrimination

Surgical Procedures
Decompression Medial Epicondylectomy Transposition
– Subcutaneous– Submuscular– Intramuscular
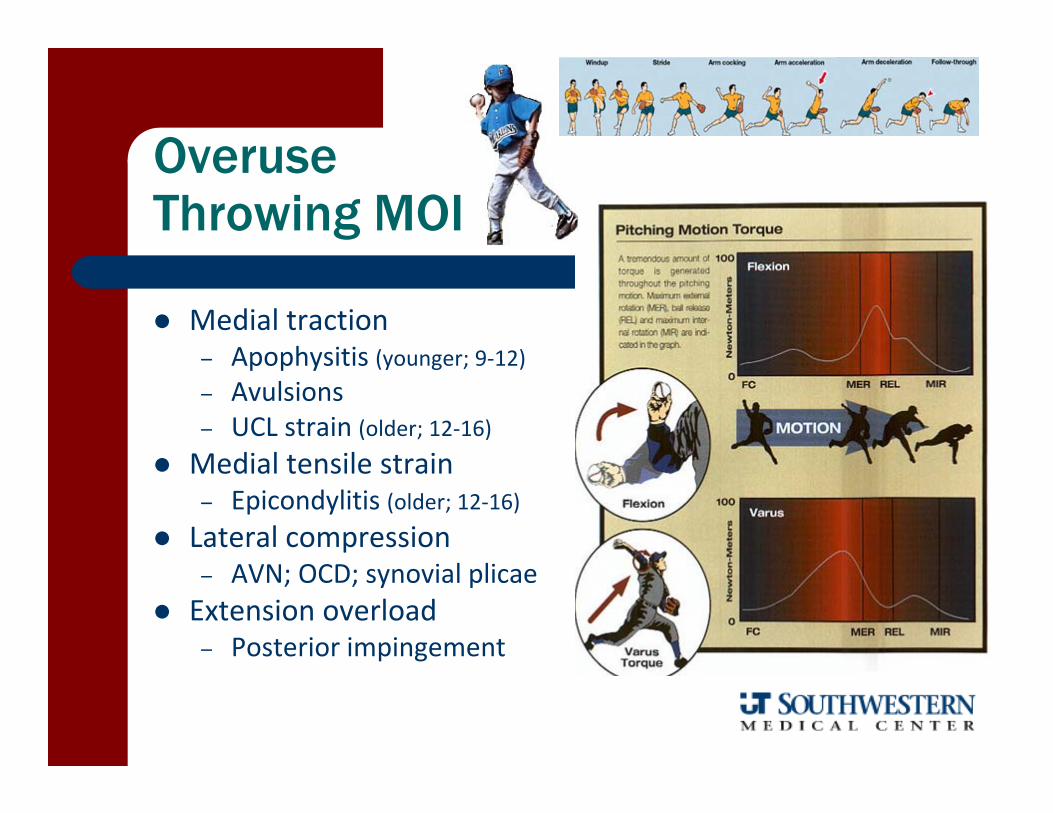
Overuse Throwing MOI
Medial traction– Apophysitis (younger; 9‐12)– Avulsions– UCL strain (older; 12‐16)
Medial tensile strain– Epicondylitis (older; 12‐16)
Lateral compression– AVN; OCD; synovial plicae
Extension overload– Posterior impingement

Throwing Faults
Violation of “Rule of 2s” Biomechanical faults
– Open up to soon (arm behind body)
– Excessive ER– Glove arm low and lateral
• Medial tension• Lateral compression

Spectrum of Injuries
Apophysitis Medial epicondyle avulsion Common flexor strain UCL sprain/tear

Examination
Position(s) played, number of throws/week, and pitch type Palpation for area of tenderness Special Tests
– Valgus Stress Test at 30°– Moving Valgus Test– Milking Sign– Valgus Extension Overload
Elbow Flexor/Pronator Strength Axioscapular/Scapulohumeral Strength

Clinical Presentation
Progressive elbow pain with diminished throwing effectiveness (decreased velocity and control)
Medial epicondylar tenderness
Contractile symptoms – pain with passive stretch or resisted contraction of common flexor insertion muscles
May have mild flexion contracture if chronic

UCL Sprain/Tear
Non‐Op– Rest, NSAIDs, and 2‐3 months throwing avoidance
– Address elbow impairments– Nocturnal valgus protection bracing 90° until symptom free– Throwing progression begins at 3 months with elbow
hyperextension protection
– 40‐50% should be able to return to previous function at about 6 months

UCL ReconstructionPost-Op Protocol
Initially splinted in 70‐90° of flexion with neutral forearm Splint removed at 10 days to initiate active wrist, elbow, and
shoulder ROM exercises (elbow brace limits of 30‐100°) with full ROM expected at 5‐6 weeks
Begin PREs at 6‐8 wks with valgus stress protection
Elbow brace discontinued at 8 wks Throwing progression at 4‐6 months with
expected return to play at 12‐18 months BW reference provided in resource file

Local Exercise TherapyFlexor/Pronator Tendinitis-Strain
Ball flips Tubing pulls Flex bar bends

Elbow Fractures-Dislocations
Supracondylar Fractures Radial Head Fractures Humeroulnar Posterior Dislocations
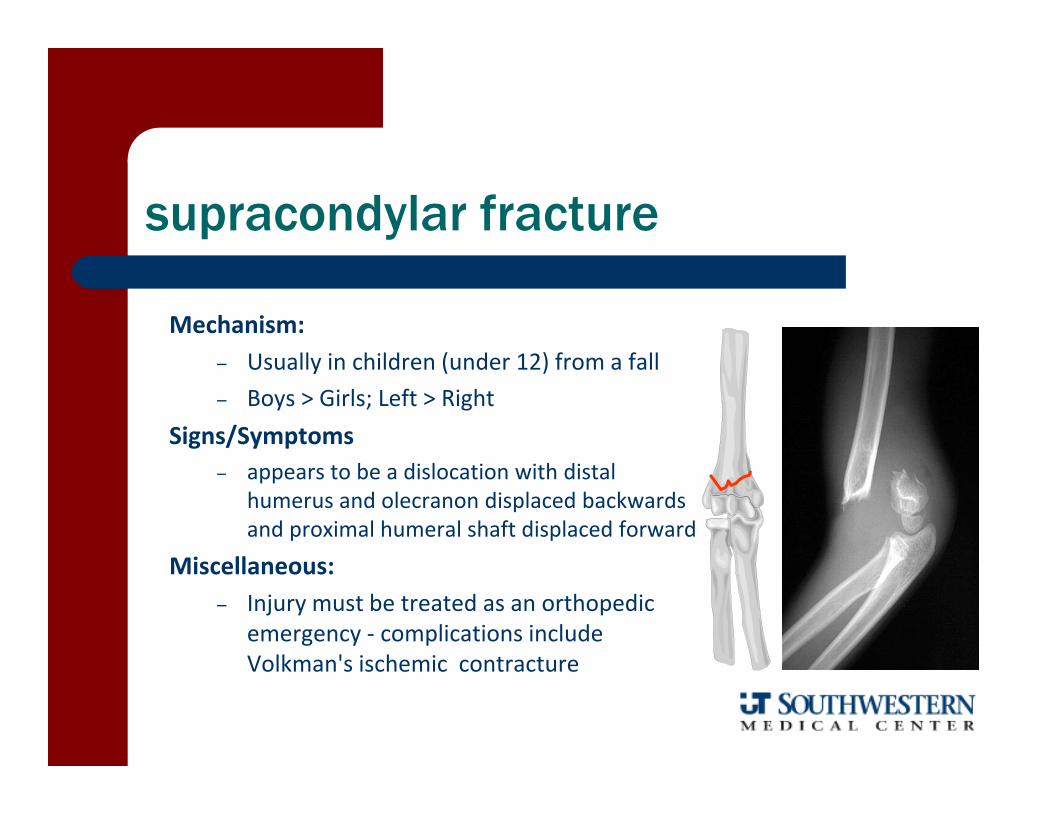
supracondylar fracture
Mechanism:– Usually in children (under 12) from a fall– Boys > Girls; Left > Right
Signs/Symptoms– appears to be a dislocation with distal
humerus and olecranon displaced backwards and proximal humeral shaft displaced forward
Miscellaneous: – Injury must be treated as an orthopedic
emergency ‐ complications include Volkman's ischemic contracture

radial head fractures
Mechanism of Injury: FOOSH
Type I undisplaced fx (< 2mm)
Type II > 2-3 mm displaced and involves more than 30% of radial head
Type III comminuted fx
Type IV elbow dislocation and radial head fx
I
IVIII
II

radial head fractures
Signs/Symptoms– pain and tenderness over radial head– swelling lateral to olecranon– primary limitation is pronation/supination
Prognosis– usually minimally displaced and rapid recovery– aggressive recovery after a short period of sling immobilization

radial head fracture rehabgeneral guidelines
Pain‐free, AA/AROM in stable range after swelling/pain subside in first 10 days
Manual therapy and isometrics at 3‐4 weeks
PREs and progression to functional activities at 4‐6 weeks

Humeroulnar Dislocation
10‐25% of all adult elbow injuries Fall on outstretched hand with elbow extended and
shoulder abducted usually the ulna and radius
dislocate in a posterolateral direction from the ulna
obvious "short" forearm deformity
intense pain and rapid swelling prominent olecranon

• perched vs. complete – perched, not as serious ligament damage– faster rehab and recovery
• complete rupture of UCL – anterior band is essential lesion– probable rupture of RCL and anterior capsule− possible damage to brachialis muscle
• 25‐50% of dislocations have concurrent fractures of radial head
• possible vascular and neurological injury – monitor C6 distribution for median nerve
injury and radial pulse
Complete
pathoanatomy
Perched

perched– 2‐3 days in sling at 90°
complete– 7‐10 days in hinged splint at 90°
post-injury immobilization

general expectations
• 30° flexion contracture at 10 weeks– if less than 45° extension at 3‐4 weeks; employ dynasplint like device
• 10° flexion contracture at average of two years post‐injury
• perched dislocation – normal ROM in 6‐8 wks
• complete dislocation – 80‐90% normal function at 3 months
• recurrent instability is rare

general rehab guidelines
AAROM in extension no PROM strength training begins at 3 weeks unrestricted strength training at 6‐8 wks
rehab with ACTIVE ROM to avoid heterotopic ossification of soft tissues
beware of ulnar nerve entrapment from scar tissue formation
MINIMIZE IMMOBILIZATION
rehabilitation points of emphasis

# of Subjects Immobilization Duration (days) Extension Loss () Time of Disability (wks)
27 < 5 3 613 10‐15 11 197 > 20 21 24
Protzman RR, J Bone J Surg, 1978
Elbow Dislocation importance of early motion
early mobilization is safe, effective, and advantageous after 48 hours
Paschos NK, et al, J Orthop Trauma 2013

specific rehabilitation phases
Phase I ‐ protection phase– reduce swelling, pain, inflammation– ice, electrotherapy, massage– gripping exercises– shoulder ROM

Phase II ‐ motion phase– warm whirlpool– UBE– AAROM‐AROM– isometric strengthening– proprioceptive drills
specific rehabilitation phases
Phase III strengthening phase• isotonic‐isokinetic• PNF• MET• body blade• shadow boxing• bicep eccentrics
specific rehabilitation phases
Phase IV functional training‐ ball dribbling‐ sock toss‐ ball plyometrics‐ inertial ‐ total gym‐ protection from hyperextension with taping or brace
specific rehabilitation phases

Post-Traumatic Stiff Elbow
• Despite high level evidence for early motion following most fracture/ dislocations ‐ high level evidence is sparse in the literature to direct therapeutic care when motion complications develop
• Functional goal is to regain active control 30‐130° of sagittal plane motion and 50‐0‐50° of transverse plane motion

Therapeutic InterventionLoss of Motion Protocol and Treatment Sequencing
Thermal preparation of effected tissue• Passive intervention: heat, diathermy, ultrasound• Active intervention: arm bike or air‐dyne
Manual Therapy followed by facilitated stretching• Joint and soft tissue mobilization• PNF hold or contract relax
Antagonistic muscle training in newly acquired range
Stretching HEP review• Static/Dynamic stretching and/or flexibility training
Cold application concurrent with LLPD stretch

Treatment Pearls
Early motion Heat‐Treat‐Cool Low load prolonged duration philosophy Treat the extra‐articular restriction
– Soft tissue/myofascial techniques– Joint mobilization

Post-Op Protocol References
Total Elbow Replacement Distal Tendon Repair UCL Reconstruction

Questions -Discussion