the process of helping a person to reach the fullest physical, psychological, social, vocational,...
TRANSCRIPT
INTRODUCTION TO REHABILITATION MEDICINE
What is Rehabilitation?
The process of helping a person to reach the fullest physical, psychological, social, vocational, avocational and educational potential consistent with his or her physiologic or anatomic impairment, environmental limitations and desires and life plans
Definitions:
ImpairmentAny loss or abnormality of psychological, physiological or anatomical structure or function
Disability:Any restriction or lack resulting from an impairment of ability to perform an activity in the manner or within the range considered normal for a human being
Handicap:Disadvantage for an individual resulting from an impairment or a disability that limits or prevents the fulfillment of a role that is normal for that individual
Definitions
Impairment Any loss or abnormality of body structure or
of a physiological or psychological function. Activity
The nature and extent of functioning at the level of the person.
Participation The nature and extent of a person’s
involvement in life situations in relationship to impairments, activities, health conditions and contextual factors.

Components of Rehabilitation
Medical Rehabilitation
Social Rehabilitation
Vocational Rehabilitation

What is Rehabilitation Medicine?
Branch of medical science concerned with the comprehensive evaluation and management of patients with impairment and disability arising from neuromuscular, musculoskeletal, cardiovascular and pulmonary disorders; also concerned with the medical, social, vocational and psychological aspects arising from them.
Medical Rehabilitation Team
Composed mainly of:PhysiatristPhysical TherapistOccupational TherapistRehabilitation NursePsychologistSpeech and language therapistOrthotist/prosthetistSocial workerPatient
Physiatrist
Team leaderCoordinates the various members to achieve the goal set.Manages the medical aspects and medical complications that arise during rehabilitation
Occupational Therapist•Evaluate and train patients in ADL’s and IADL’s•Explore vocational and avocational interests•Evaluates the patient’s skill within the community •Train patients in use of modified environment, assistive devices and UE prostheses•Educate the patient’s family to maintain independence
Physical Therapist
Use of physical agents for treatmentAssist patient in functional restoration especially for gross motor functionsTrain use of LE prostheses
Psychologist
Helps the patient and significant others to prepare psychologically for full participationTesting for intelligence, personality, psychological statuscounseling
Rehabilitation Nurse
Direct personal care of patientsAddresses the ADL’sAssist in medication managementEducate families on the related disabilitiesAssist in use of adaptive devices
Speech and Language Therapist
•Evaluates and treats patients with neurogenic disorders such as aphasia, dysarthria, apraxia, cognitive-communication impairments, dysphagia•Educates patients/families on care of tracheostomy tubes, dysphagia, alternative communication.
Social Worker
•Evaluates the patient’s total living condition, including:
–Lifestyle–Finances–Employment history–Community resources
•Assess the impact of disability with the above mentioned factors•Facilitate assistance to cope with such impact.
Orthotist/Prosthetist
•Evaluates, designs and fabricates orthoses and/or prostheses.•Follow up and educate users of care and maintenance of such devices

Other team members
•Vocational Counselor•Recreation therapist•Spiritual counselor•Rehabilitation Engineer
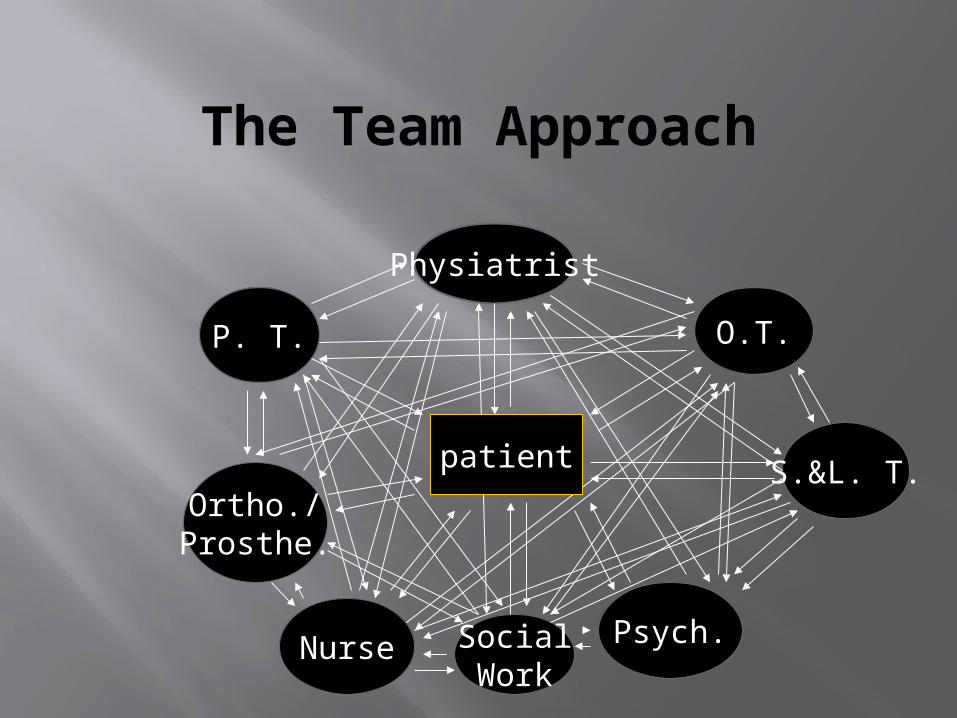
The Team Approach
Physiatrist
P. T. O.T.
Psych.
S.&L. T.Ortho./Prosthe.
Nurse SocialWork
patient
The Physiatric Approach
•Physiatric History–Chief complaint–HPI–Fxnal Hx
•ADL•Community activities•Vocational activities•Functional Goals
–Psychosocial Hx
•The Physiatric Approach
•Past Medical History•Review of Systems•Functional Examination•Musculoskeletal Examination•Neurological Examination
Musculoskeletal examination
0 – no contractions1 – palpable contractions noted2- full range of motion with gravity eliminated3 – full range of motion with gravity4 – full range of motion with gravity and slight resistance5 – full range of motion with gravity and full resistance
Modified Ashworth scale for Spasticity
0 – no increase in tone 1 – slight increase in muscle tone, manifested by a
catch and release or by minimal resistance at the end of the ROM when the affected part is moved in flexion or extension
1+ - slight increase in muscle tone, manifested by a catch followed by minimal resistance throughout the remainder (less than half) of the range of motion
2 - more marked increase in muscle tone through most of the ROM but affected parts easily moved
3 –Considerable increase in muscle tone, passive movement difficult
4 – affected parts rigid in flexion or extension

•Activities of Daily Living
•Mobility–Bed mobility–Wheelchair mobility–Transfers–Ambulation
•Self Care–Dressing–Self feeding–Bathing–grooming
Activities of Daily Living
CommunicationWritingTyping/computer useTelephone useUse of special communication devices
Environmental Hardware
KeysFaucetsLight switchesUse of windows and doors
Instrumental Activities of Daily Living
Home Management
ShoppingMeal planningMeal preparationCleaningLaundryChild carerecycling

Instrumental Activities of Daily Living
Community Living Skills
Money/financial mgtUse of public transportDrivingShoppingAccess to recreational activities
Instrumental Activities of Daily Living
Health Mgt.Handling medicationKnowing health risksMaking medical appointments
Safety MgtFire safety awarenessResponse to dangerous situationsResponse to alarms

Instrumental Activities of Daily Living
Environmental Hardware
Vacuum cleanerStove/ovenRefrigeratorMicrowave ovens
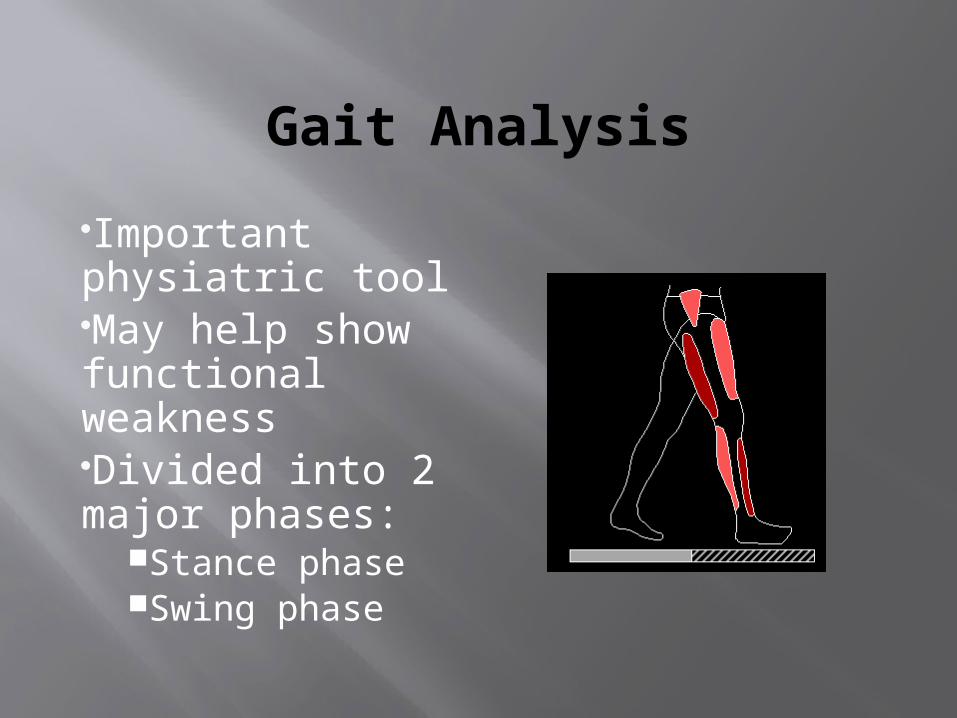
Gait Analysis
Important physiatric toolMay help show functional weaknessDivided into 2 major phases:
Stance phaseSwing phase
Swing Phase
Covers 40 % of the gait cycleInitial swing (acceleration)MidswingTerminal swing (deceleration)
Stance phase
Covers 60 % of the gait cycleLoading response (heel strike)Midstance (foot flat)Terminal stance (heel off)Preswing (toe off)
Six determinants of Gait
Pelvic rotation in the horizontal planePelvic tilt in the frontal plane early Knee flexionWeight transfer from heel to foot flatLate knee flexionPelvic lateral displacement
Considerations in Rehabilitation
•Goal setting•Understanding the functions of the team members•Autonomy of each member•Understanding the needs of the patient